Fungi and the microbiome finally got on my radar. Apologies to some, but there is a lot of different items on the microbiome radar screen.
“Small intestinal fungal overgrowth (SIFO)… Two recent studies showed that 26 % (24/94) and 25.3 % (38/150) of a series of patients with unexplained GI symptoms had SIFO. …. but evidence for eradication is lacking.”Small intestinal fungal overgrowth [2015]
As I did with taxa years ago, I will be writing a blog on each one reviewing the literature. If there is sufficient data at the end, I may add it as a feature to Microbiome Prescription.
- CDC provides a list of known fungal diseases: Types of Fungal Diseases.
- For the current list of Fungi reviewed on this list, click Information of Different Types Of Fungi
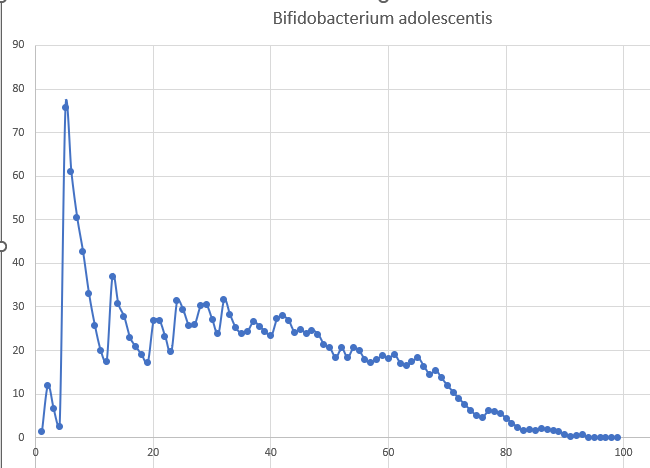
One of my reader’s results motivated this choice. The data from a Thorne Microbiome Test. About 8 out of 10 people have less of it. The person also has a Crohn’s diagnosis (with SIBO and IBS earlier).

Preventive for Fungi
The following are suggestions:
- Reduce and keep your living space humidity at 50% or lower (typically done by dehumidifiers). EPA recommends 30-50% [EPA]; we set our dehumidifiers for 35%.
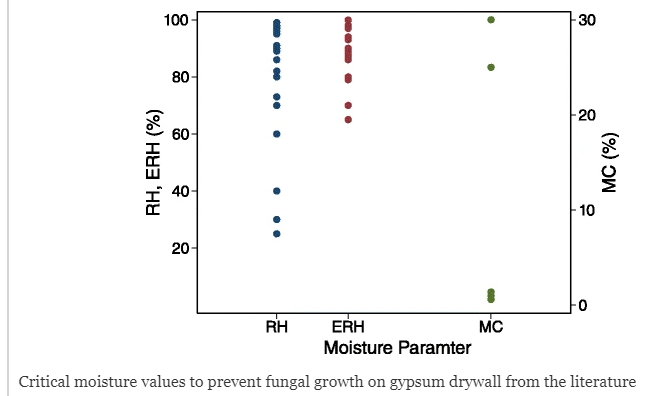
Moisture parameters and fungal communities associated with gypsum drywall in buildings [2015]
- Use a HEPA filter appropriate to your space.
Effectiveness of Airborne Fungi Removal by using a HEPA Air Purifier Fan in Houses [2018]
Typically they are described as “Room Size: Up to 1500 sq.ft. maximum”. We are more aggressive and divide that by 4. For example we use 3 Austin Air HealthMate HEPA Air Purifier for our 900 sq.ft. living space. - Check the north side of your building for mold. If found pressure wash it off and if possible, apply substances to inhibit them coming back.
- Check for mushrooms in lawns etc. If found, remove them and treat where you found them.
Remember, all fungi are not the same. Antibacterial and Antifungal Activities of Spices [2017] does not mention all fungi that I am reviewing. Additionally, some spices are known to have Fungal Contamination of some Common Spices [2022] and Fungi and aflatoxins associated with spices in the Sultanate of Oman [2002] which included cloves (often deem an antifungal).
Basic Information
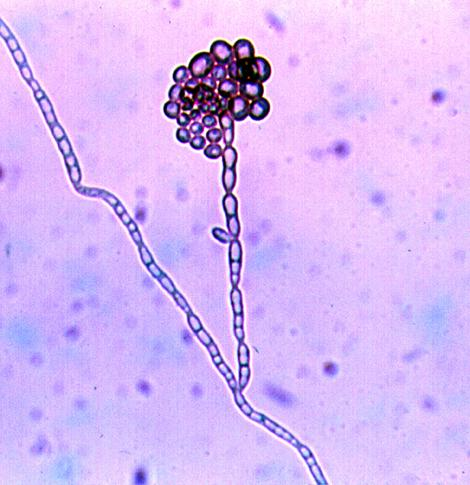
It’s a family with the lineage below: Fungi; Dikarya; Ascomycota; saccharomyceta; Saccharomycotina; Saccharomycetes; Saccharomycetales; CUG-Ser1 clade; Debaryomycetaceae
- There are only 24 studies on PubMed. It was first identified around 2010.
- “The fungal component of the intestinal microbiota of eight healthy subjects was studied over 12 months using metagenome survey and culture-based approaches. …Other families of Ascomycota that reached remarkably high amounts in few samples were Debaryomycetaceae (mostly Debaryomyces)” Longitudinal Survey of Fungi in the Human Gut: ITS Profiling, Phenotyping, and Colonization [2019]
- Antifungal Susceptibility Profiles and Resistance Mechanisms of Clinical Diutina catenulata Isolates With High MIC Values [2021] reports sensitivity to:
- itraconazole (0.06–0.12 μg/ml),
- posaconazole (0.06–0.12 μg/ml),
- amphotericin B (0.25–1 μg/ml),
- 5-flucytosine (<0.06–0.12 μg/ml)
Bottom Line
Our ability to drill down further is limited because the results only report at the family level and sparse literature. Itraconazole, an antifungal that is the top choice for other fungi reviewed appears to work.




Recent Comments