“Things that I have been taking since the last test in February 2023:
Rosemary
Grapefruit seed extract
Turmeric
Natto
Tetracycline
Clove
Anise
Acacia gum
Amoxicillin
Apple peel powder
Thyme
Symbioflor 2
Neem
Jarlsberg cheese
My symptoms:
Still get the red nose (some form of rosacea). But it is better than before.
Still feel fatigued (both physically and mentally). But it is better than before.
Feeling stressed. But it is better than before.
Brain fog.
Bloated.
Lots of gas – I fart and burps a lot. “
This is his fifth sample. Multiple samples are not unusual because fixing the microbiome means a lot of course corrections.
Analysis
First, we will look at measures that were not available for the earlier posts. In the last period, we see a dramatic change of the histamine values!
Sample
Anti-Inflammation Value
Histamine Value
Butyrate Value
2021-08-31
97%ile
98%ile
25%ile
2021-12-03
96%ile
98%ile
57%ile
2022-03-25
18%ile
87%ile
62%ile
2022-08-11
30%ile
90%ile
73%ile
2023-02-22
65%ile
86%ile
82%ile
2023-09-12
87%ile
3.2%ile
80%ile
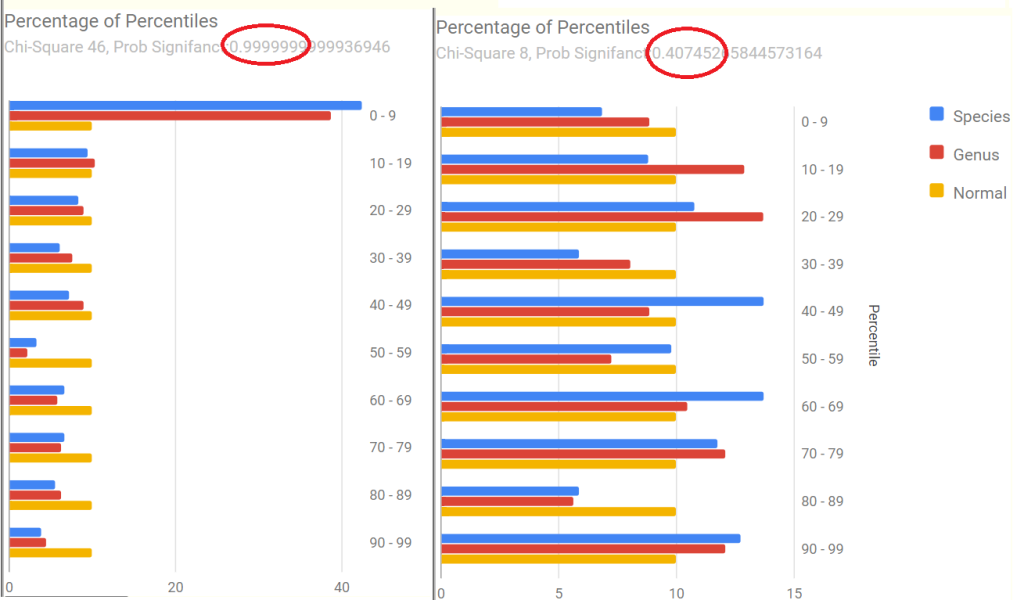
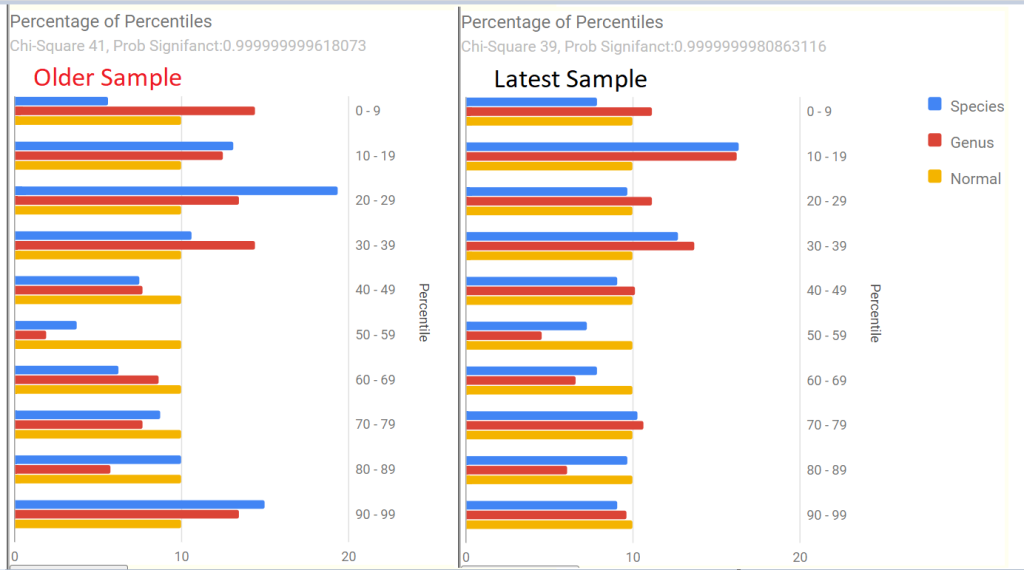
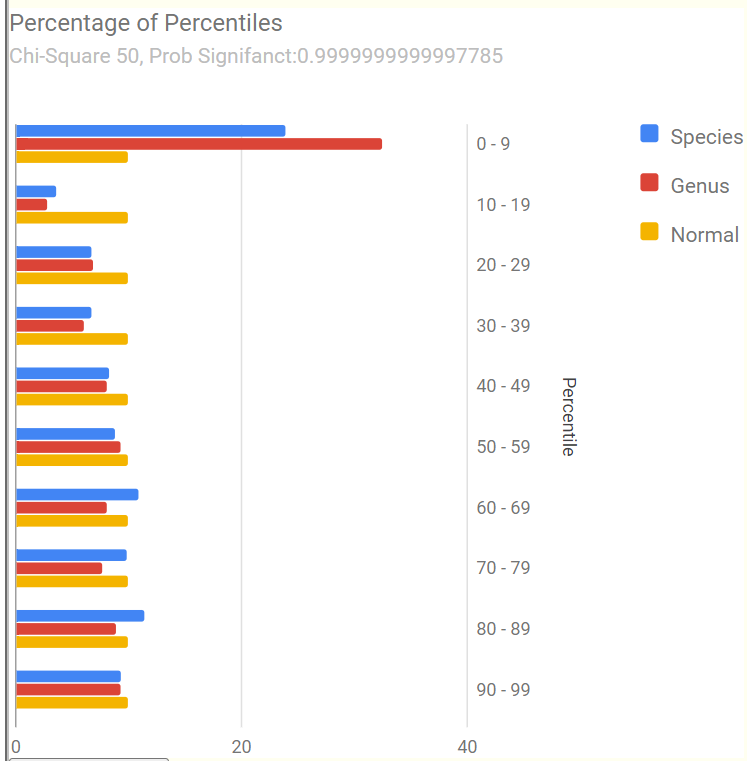
We also see a dramatic change in the Percentages of Percentiles charts that suggests improvement. In fact, there is no longer any statistically significant shifts (going from 0.99999… to .40!). Dropping below 0.95 is an objective target. The pattern went from the common ME/CFS and Long COVID pattern to an normal pattern.
Potential Medical Conditions Detected
We have the following candidates to consider that were not flagged in the prior sample (where nothing stood out):
Allergic Rhinitis (Hay Fever): 100%ile
Stress / posttraumatic stress disorder: 98%ile
Irritable Bowel Syndrome: 97%ile
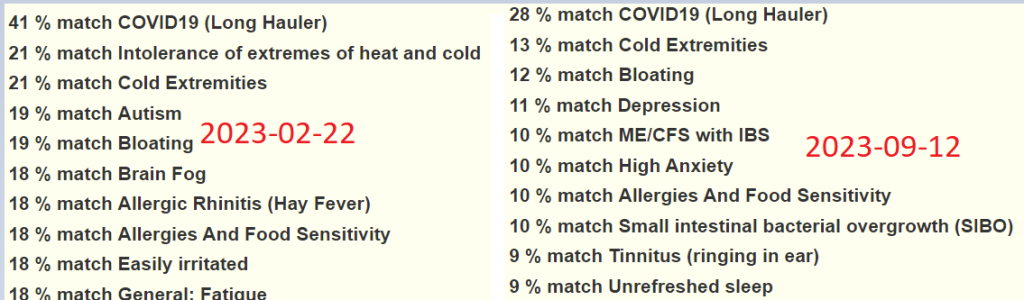
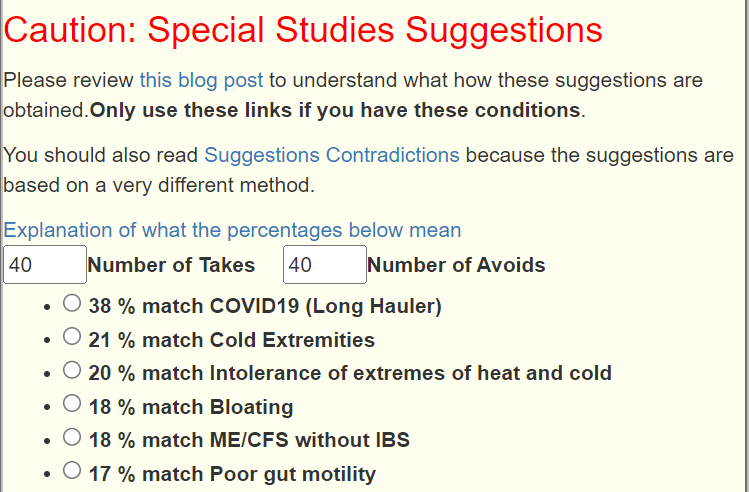
This may be just randomness or because the microbiome is calming down, patterns hidden by noise are showing up. Looking at Special Studies pattern matching, the top one was COVID19 (Long Hauler) at 28% match (prior was 41% match) — a definite improvement. Other items dropped about 8% match each, most were so low, that there may not be significance.
These appear to agree with his personal observations. We have Prevotella copri is at 76%ile, hinting that mycotoxin present (mold) may be in his environment (see this post for more exploration).
Going Forward
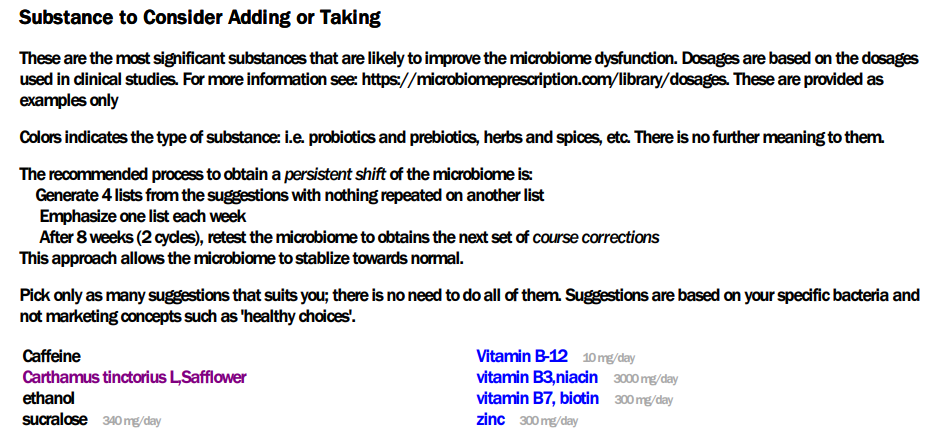
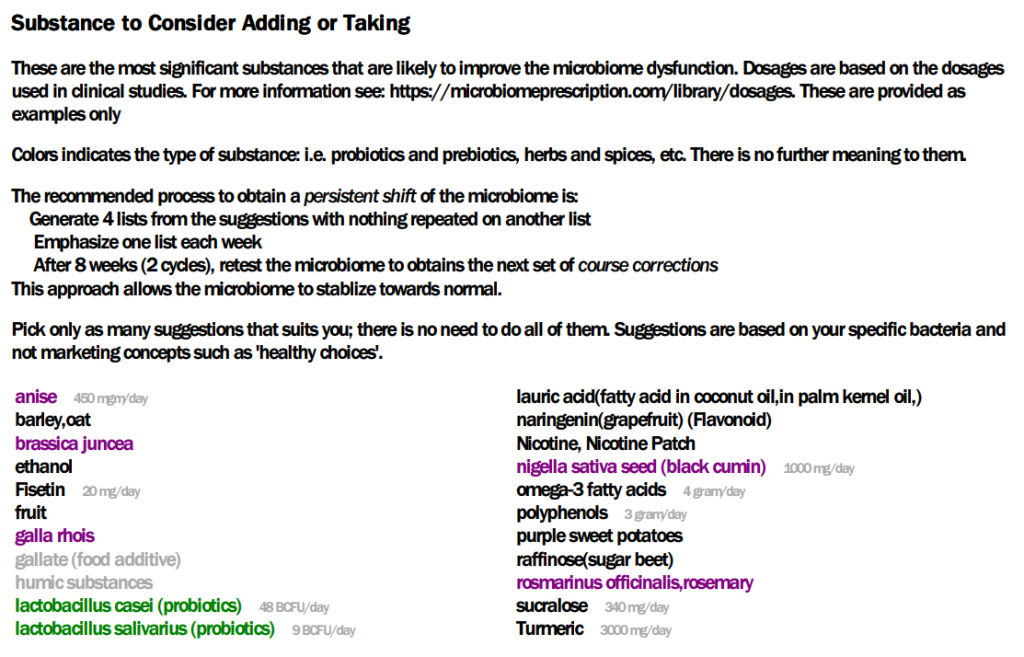
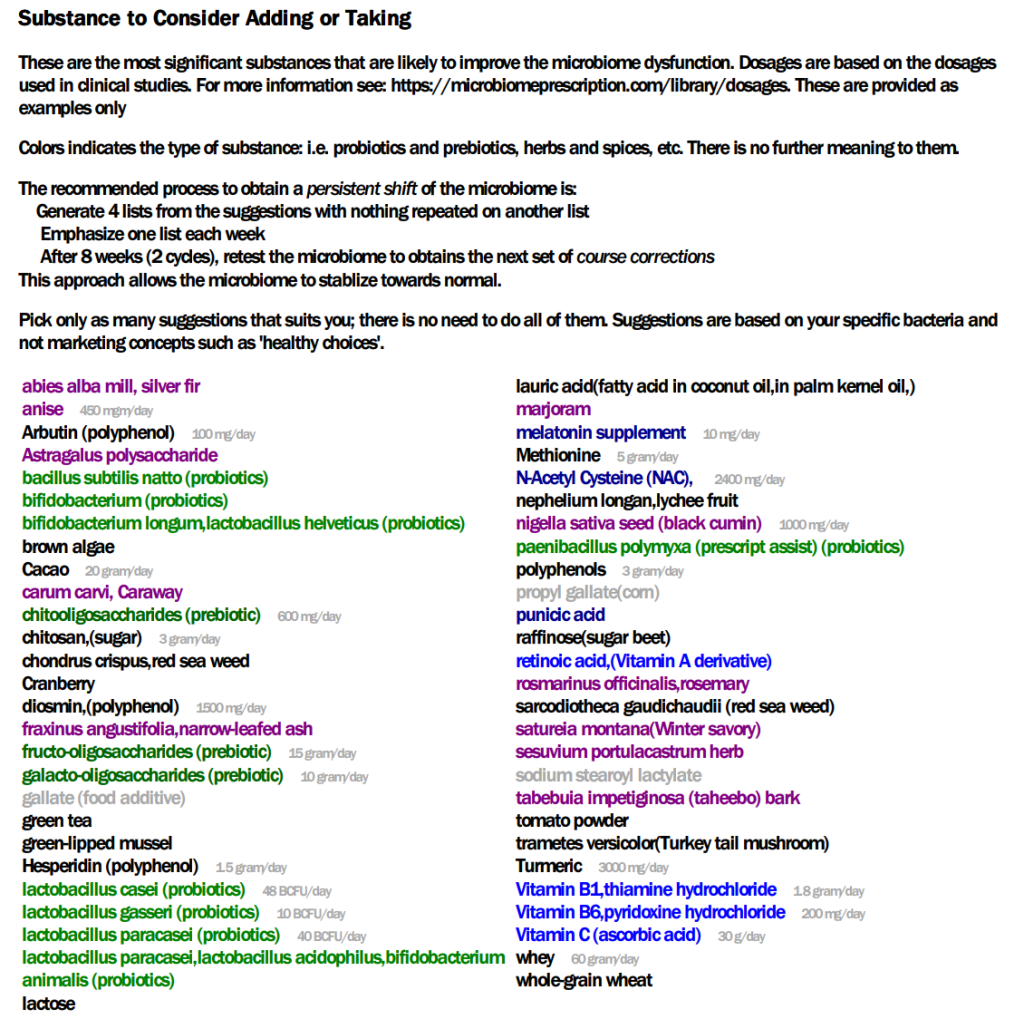
In terms of subjective and objective measurements, this person has improved. So time for the next course correction. I am going to just run with the “just give me suggestions” since nothing really stands out.
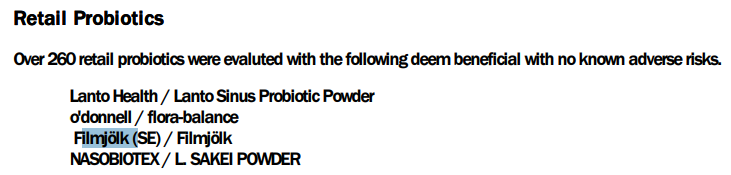
The non-prescription items from the PDF are by far the shortest that I have seen! So the safflower may be difficult because it does not mean safflower oil (an avoid), but the herb.lots of coffee and perhaps a little Aalborg Aquavit.
In terms of probiotics, he lucked out — Filmjölk is likely available to him
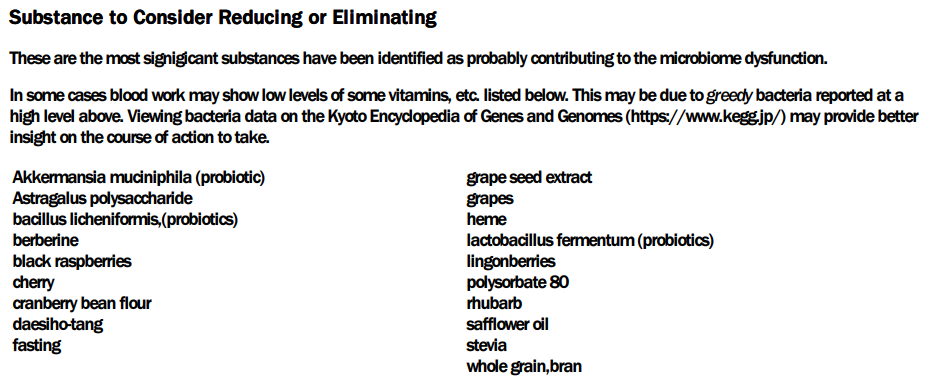
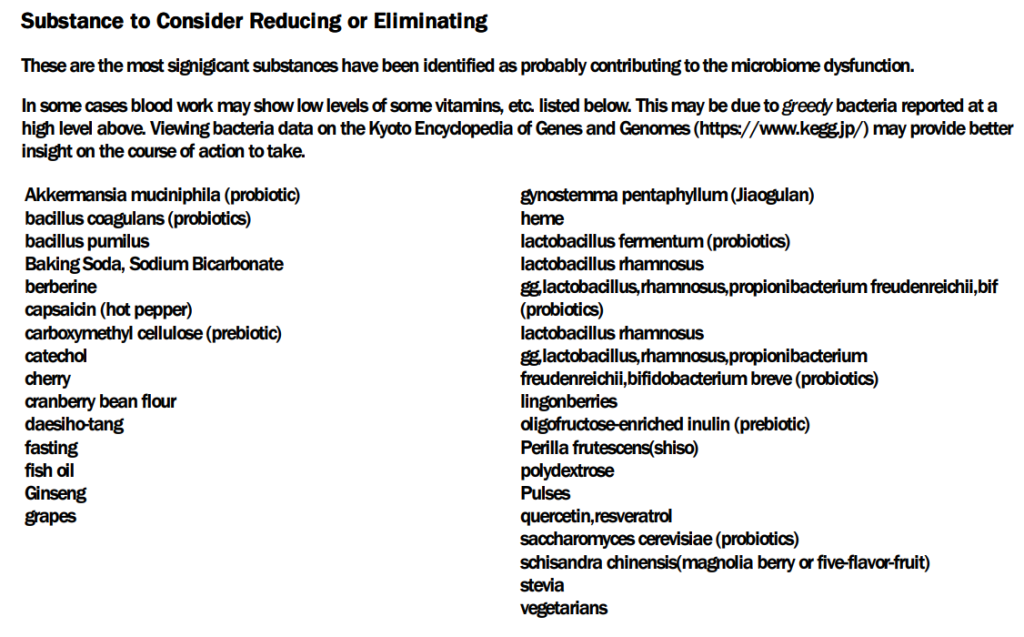
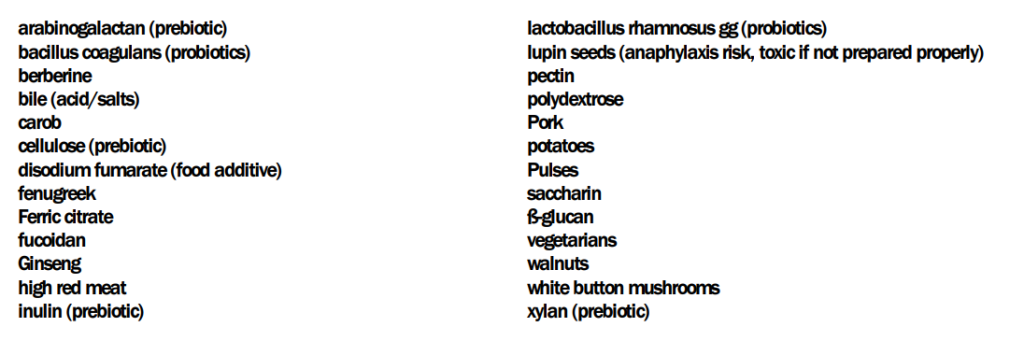
The avoid or reduce list is much longer!!
Going over to items computed from the Kyoto Encyclopedia of Genes and Genomes we have the top item being the typical one for ME/CFS: Escherichia coli (i.e. Mutaflor or Symbioflor-2). In terms of supplements, the two most significant one are: Glutamine, Threonine, Serine.
Since the person has a co-operative MD (i.e. two antibiotics were listed), I reviewed the prescription items. The top item was amoxicillin (antibiotic)s[CFS], which has already been used. We have gatifloxacin, ciprofloxacin (antibiotic)s[CFS], and clinafloxacin (antibiotic) which is a different family (a fluoroquinolones which has a lot of bad press). The next one worth considering is nadifloxacin (antibiotic): Nadifloxacin is a broad-spectrum quinolone antibiotic(in fluoroquinolones family) that has been approved for use in the treatment of acne vulgaris and skin infections. This may impact his rosacea. The next one down the list may be similar: fusidic acid sodium salt (antibiotic).
The following should be read before taking any fluoroquinolones by both the patient and the MD.
One factor to consider is that Cecil Jadin has been using fluoroquinolones for twenty years without seeing any adverse effects. The duration is only 10 days or less. Longer duration of use may be a significant factor. See this post and video for more information.
Questions
“All those antibiotics MUST be taken: after food ( not only water ) and without any dairy products. Patients must avoid sugar intake and some supplements(for example magnesium). Antibiotics should be taken in the morning and the evening. Patients must avoid sugar intake and supplements.”
Q: I’m going to do another round with amoxicillin. — In Jadin’s presentation she says to only take it for 7 days, ain’t ok to take it for 14 days as we talked about before? — Can’t I take other supplements like magnesium when I take antibiotics?
A: The duration range of 7 – 14 days is, IMHO, fine. My main concern is long duration that can result in antibiotic resistance.
Word of warning: If there a herxing, it will get a lot worse!! so start on a Friday night (and consider a few vacation days after the weekend!)
Q: If I want to have a longer list for what to take / avoid, can I use the three that is blue below (as earlier)?
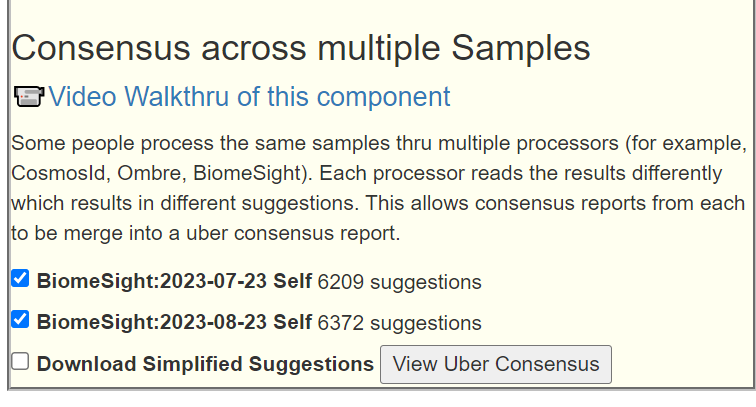
A: What is shown above is from the PDF which I am preferring to use for posts because it keeps things simpler. You can do any combination you wish. You could also consider doing your last sample suggestions and this sample suggestions, an “uber consensus” which should produce suggestions of what has been out of range with both samples.Caution should be done because of how different the two samples are!
This does produce a massive list!!
I would then go thru the list and cross out items that are not shown with at least 7 of the possible 8 in the technical details.
Bottom Line
My own experience with recovery was that it took about a year for many symptoms to wear off. The body is not an electronic device with an on/off switch; think of a meadow that has been damaged by fire, flood, or chemical spill — it takes time for things to come back.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide solid information on rotations, dosages, etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting. Some suggestions may be counterindicated for other medications you are taking and medical conditions.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
Much longer and detailed than usual. Most of the data is “outside of my wheelhouse” of expertise, but readers may have additional insight.
22 Years ago, I had a UTI. It wouldn’t go. I had 5 antibiotics. None of them worked. By the sixth week I was beside myself. A new doctor gave me ciprofloxacin. Finally it went away. Unfortunately, being naïve and a bit dumb back in the day, I started drinking alcohol the following weekend and the UTI came back. I didn’t realize but the bladder lining was weakened and presumably still some residual bacteria there. They got to work again.
I had ciprofloxacin again. 7 day course. My bladder sort of got back to normal but I had to drink more water than usual to stop it from feeling uncomfortable. This lasted four years. I could pee normally, everything was good but I was always conscious things weren’t quite the same as they had been. I stopped drinking alcohol completely.
NB: I developed hay fever pretty immediately after finishing the second course of Cipro. I believe something got knocked out of my microbiome that I’ve never got back.
After a period of huge stress at the age of 30, my bladder suddenly got very hot and tight and uncomfortable. Numerous tests showed no infection. I was offered a urethal stretch. This worked to some extent but I then landed in a pattern that lasted 18 years:
From days 5-14 of my cycle my bladder would feel like I had a UTI. But from days 15 – 28 and then days 1 – 4, I had pretty much no symptoms. My bladder during non-high estrogen days was good. My bladder was like normal. I could eat all foods and drink alcohol somewhat.
However I did have to be careful. I couldn’t drink every night (not that I would anyway) and citrus, black tea, coffee, I had to wary. Too much and it would set things off. Same with stress. High stress periods would see my bladder get very hot and tight and it would take weeks for it to calm back down.
During this 18 year period, I found this pattern that on estrogen-high phases my bladder would go off, feel like a UTI, reduced flow, more frequency, but once progesterone kicked in, everything was fine. During low hormone times, during my period, my bladder was best of all. Worked perfectly.
Two years ago I found out I have osteoporosis. I trialed HRT, using estradiol gel. Within 24 hours, my bladder was very very unhappy. I felt like I needed to pee constantly. Tiny amounts. It was far worse than during my own cycle of estrogen.
I stopped on day 20 because it was so uncomfortable. I really wanted to take the estrogen but I couldn’t. . But I don’t seem to be able to do this. I believe this messing with my hormones sent me straight into much stronger menopause symptoms. I suddenly gained weight around my middle (sign of leaky gut, low estrogen unable to keep the intestinal junctions tight) and my spine and sternum started to ache like they never had before. Brain fog, terrible sleep, frequency of peeing but this time for no reason, just bladder more sensitive overall.
I trialed progesterone only this summer, in the hope that it helps my bladder usually – well my own progesterone seems to. However after a while the familiar burning and uncomfortable feeling came back. It seems like external hormones aren’t for me.
He trialed me on ketotifen but it made things worse. 5% of users can get cystitis type symptoms. Looks like I was one of them.
He now wants me to trial Famotidine (stomach acid suppressant) and Loratadine to switch off H1 and H2 receptors. I’m reluctant to do that. He also thinks I may have a staph epidermis infection but I find this hard to believe because my bladder goes through very good periods for months at a time – it’s only with stress or estrogen that things get bad. It’s true to say though that with every period of stress, my bladder loses function and so now, it’s harder to get all the urine out. It is inflamed at the base, the ultrasound showed.
He’s prescribed Nitrofurantoin twice per day for 2 weeks. I’m really reluctant to take yet more antibiotics.
Additionally I’ve been diagnosed with stage 2 kidney disease just recently, sightly high creatinine and just on the cusp range of too high for calcium too in the blood.
I am low in Vitamin D, just below normal. I am low in ferritin from a recent blood test in August. I am trying to correct these two with supplements the last few weeks but I know it takes time.
I feel overall I’m inflamed. I feel like I don’t absorb things as well as I used to. I don’t sleep very well.
Taking hydroxyzine helps with the aches in my spine and sternum. They have almost gone away. Nice side effect but I know antihistamines are not good long term. I see Fexofenadine seems to do the same thing too https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8421647/
I’d like to get to the stage where maybe I could take the hormones to protect my bones? At least have the choice.
Analysis
We have actually two samples taken a few weeks apart. Technically, there was a little improvement between the samples (one had 9 “9” and the other just 8 “9”).
Both samples had similar profile with Dr. Jason Hawrelak Recommendations. With the following significant items:
Potential Medical Conditions Detected use pattern matching to published studies. We have the following items of note:
hypertension (High Blood Pressure) risk
Hyperlipidemia (High Blood Fats) risk
Prior sample also had: Allergies risk and Colorectal Cancer risk.
Special Studies pattern matching (using other samples uploaded with their declared symptoms) had only one strong match: COVID19 (Long Hauler), with a weaker match for Allergies And Food Sensitivity. The person had COVID but appears to be full required (no symptoms for long hauler).
Going Forward
There are many things happening with this person. There are no really strong microbiome pattern matches for the main symptoms of concern, so I will just work from the standard “just give me suggestions” on each sample and then do an uber-consensus. Every microbiome report has some fuzz factors in measurements, combining two or more (close in time) reduces the noise from the fuzz.
The highest priority was 470 and the lowest was -543. Applying the 50% rule, we will focus on items over 235 or below -272.
Some interpretation notes:
Avoid being a vegetarian does not mean avoid vegetables. It means have some fish or meat.
Fruit is a take with some specific fruits being an avoid (cherry, grapes, lingonberries). Coconuts and Grapefruits
Avoid fish oil is not inconsistent with taking omega-3 fatty acid. See this listing of what is in fish oil. So beware of supplements saying “high in omega-3” that is effectively fish oil. An example of a non fish oil source of Omega-3.
Review of Previous Consumptions
Items between -272 and 235 are unlikely to cause a significant contribution and likely complicates life without a clear benefit. All of the items cited fall in this indifference range.
I also decided to look at the top prescription items as a discussion point with your MD. I have a hypothesis that many prescription items work via their impact on the microbiome. This leads down a speculation path that conditions associated to the top recommended prescription items may be in a pre-significant state — a potential developing risk.
I found what appear to be an association to be aware of. The earlier sample had a pattern matching to a form of cancer.
moxifloxacin (antibiotic): 417 – “Moxifloxacin is an orally administrated fourth‐generation quinolone with broad‐spectrum coverage against tumor‐associated bacteria” [2020]
doxorubicin hydrochloride,(prescription): 327 – “Doxorubicin is an antibiotic derived from the Streptomyces peucetius bacterium. It has had wide use as a chemotherapeutic agent since the 1960s. ” [NIH]
Q: Can I ask – would you consider taking any pre-biotics? Not probiotics but prebiotics? I’m looking at HMOs and PHGG? For increasing bifido? Not sure if this is a good idea…
A: There are no prebiotics that makes it over the threshold for good odds to help. The two that you cite are both negative.
The suggestions are based on considering the impact on all abnormal bacteria. Trying to fix just one bacteria can often result in other bacteria being made worse. I looked at PHGG and found this 2021 study:
You are at 100%ile for both of these…. you do not want to feed them more!
Q: I wasn’t sure from what was written in the article if I should be seeking an antibiotic to reduce down the fragilis and uniformis?
A:
IMHO, we should try non-antibiotic methods first. Often they may require minor diet changes that may become established and keep them away. If after 2 months and a retest show no improvement, then it is time to start negotiating with your MD. This means reaching an agreement on an antibiotic that addresses them BUT does not make your gut worse… To get the first choice list of antibiotics, just click this button. NOTE: Not all are suitable. Some are for vet usage, others may be injected only, etc. Your MD has to evaluate them.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide solid information on rotations, dosages, etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting. Some suggestions may be counterindicated for other medications you are taking and medical conditions.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
I have just updated the site using a refinement of the Kaltoft-Møldrup algorithm that became available to the site this weekend. Before getting into the nerdy details, let us recap the purpose.
In general, studies find associations between higher or lower levels of some bacteria to symptoms or conditions. These are primitive calculations with many deficiencies. In general, they do not establish causality, only association.
The common hypothesis is that being too high increases the risk. A common assumption for many medical conditions (when there is insufficient studies) is that the “top or bottom 5 percentage of patients” may be at risk. This can also be expressed as those in the bottom 5 percentile and top 5 percentile.
In many branches of physical science, this can be computed from the mean and standard deviation. This requires the data to be a normal distribution. This is not the case with microbiome data. Our purpose is to identify the values where we suspect that the risk has become significant.
The tables in this post illustrates the nightmare in my earlier post!
Scope of Investigations
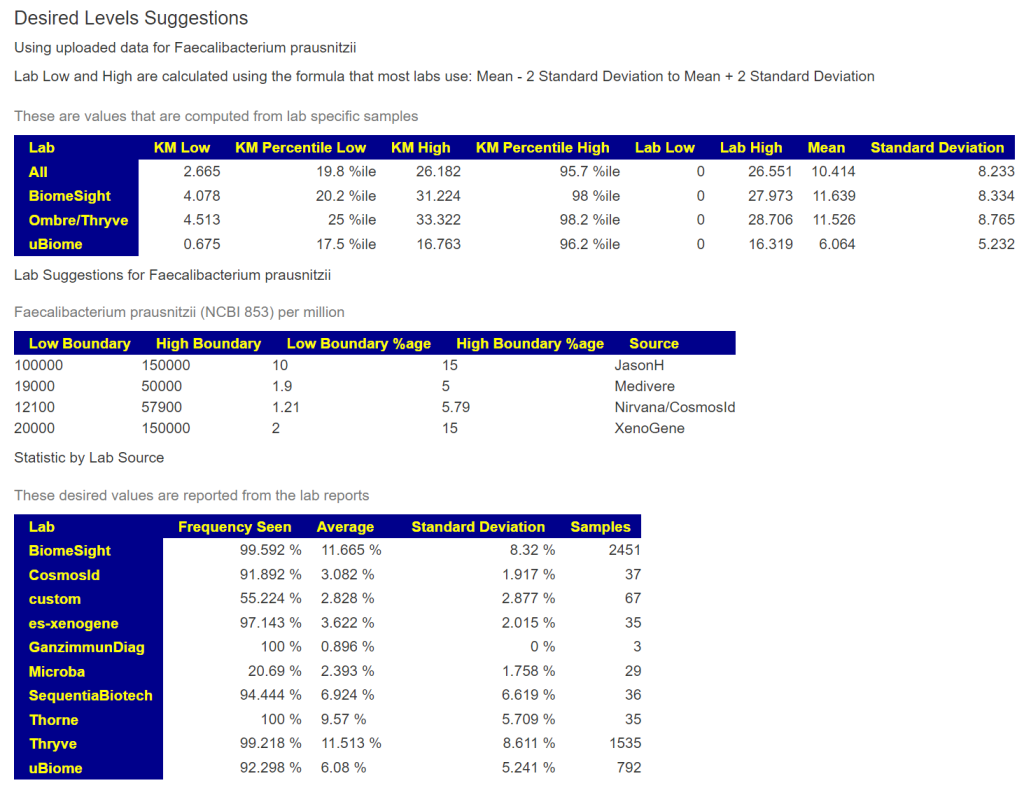
I am going to the bacteria cited in Dr. Jason Hawrelak Recommendations to illustrate the issues. His levels came from published studies, observations and the test results of his patients (which could have been done using labs not covered in this post).
Whether his ranges applies to your sample depends on the lab that did the sample. In some cases, many of the labs have reasonable agreement. In other cases, major differences.
You should ask for full disclosure from any source on how the ranges are calculated. Ignoring or dismissing the differences between different lab results suggests a low bandwidth understanding of the issues involved with the microbiome.
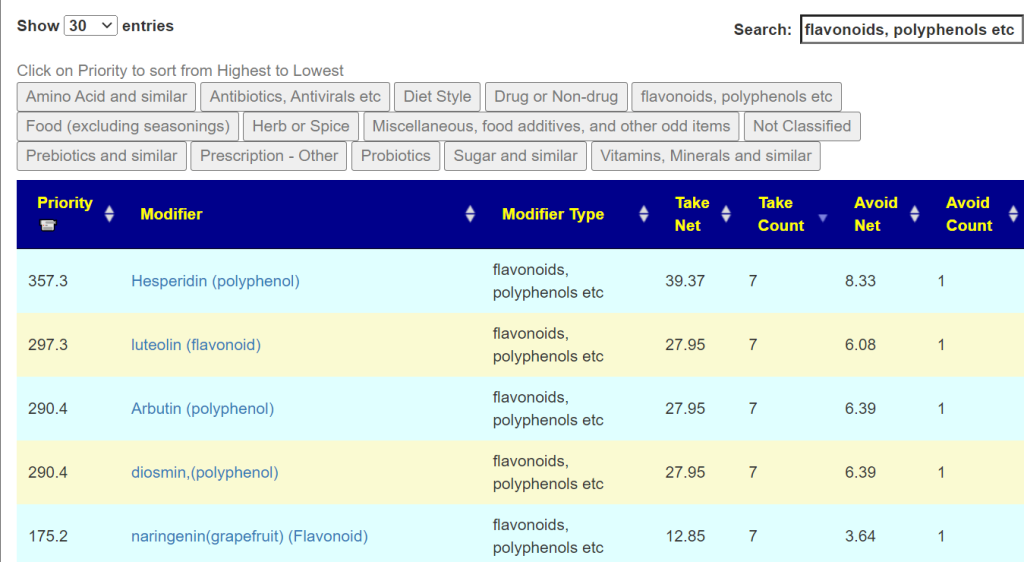
You can see the values when you look up bacteria as shown below
Current Issues: chronic fatigue (not able to exercise or take walks longer than 10-15 min), strong brain fog & reduced cognitive abilities,
History:
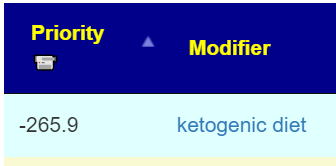
Covid-19 infection in June 2022 followed by intense fatigue, followed by 1.5M of recovery, followed by spontaneous, severe crash (Post-exercise malaise, fatigue, strong brain fog) and continuing since then I tried a ketogenic diet for 6 months (and a carnivore 4:1 ketogenic diet for 1 month) to treat these issues but this actually seemed to make my symptoms worse. Tried a broad spectrum of high dose supplements, vitamins and minerals that did not help at all. Currently slow re-introduction of carbs into my diet again.
Analysis
I can only review the current state since I am microbiome data-bound in reviews. It was interesting that two popular approaches advocated by influencers made him worse. There is no universal solutions / cure. Solutions are specific to the individual.
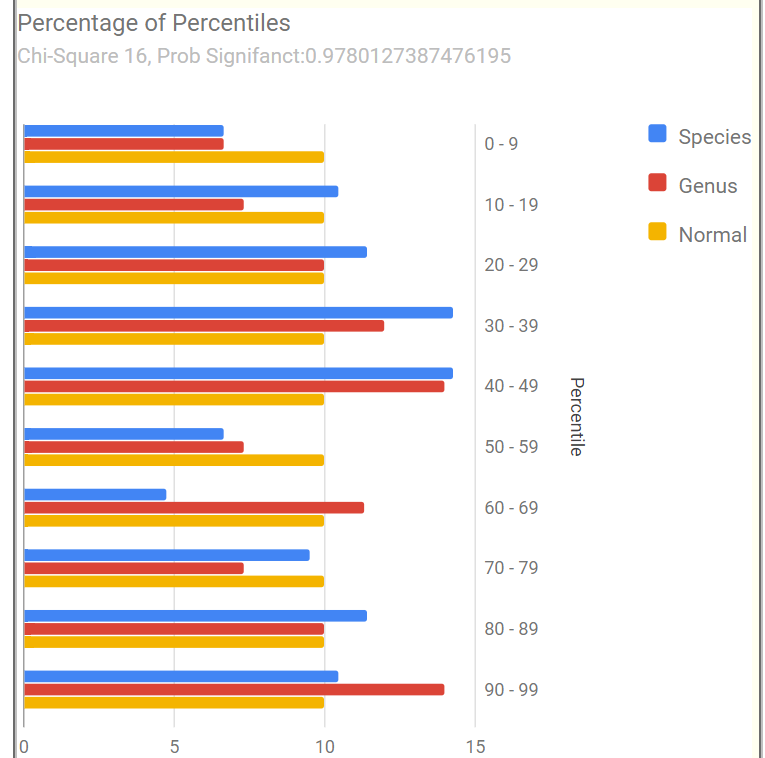
My usual starting point for ME/CFS and post-COVID is the Percentages of Percentiles chart. It is not a match for the usual pattern seen for those conditions, but we see statistically significant abnormalities in the 10-19%ile range. I have not seen this pattern before.
Looking at Potential Medical Conditions Detected, only Mood Disorders stands out. This is consistent with his past history. For Dr. Jason Hawrelak Recommendations, he’s at the 75%ile with the main items of concern being high Bacteroides, Bilophila wadsworthia, and low Bifidobacterium, Roseburia, Akkermansia.
Looking at Special Studies, the top item is likely due to a hybrid ME/CFS with post-COVID:
Where Do We Go From Here?
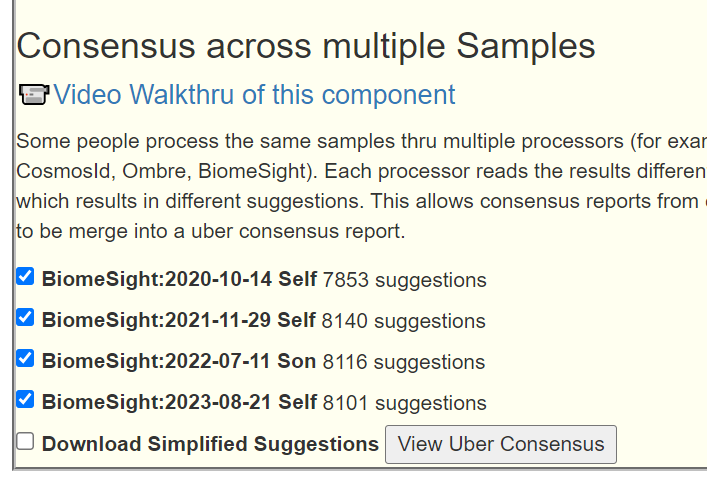
I am going to build a consensus report from the 4 “Just Give Me Suggestions” to which we will add:
Special Studies: COVID19 (Long Hauler)
Potential Medical Conditions Detected: Mood Disorders
There are two ways of looking at suggestions (similar results but minor differences). Using the PDF Download or looking at the details.
In this case (these do not always appear), probiotics too.
Before moving onto the detail view, let us look at KEGG computed probiotics:
#1 was Escherichia coli (which is symbioflor 2 above or Mutaflor). The items below are at 1/6th the estimated contribution.
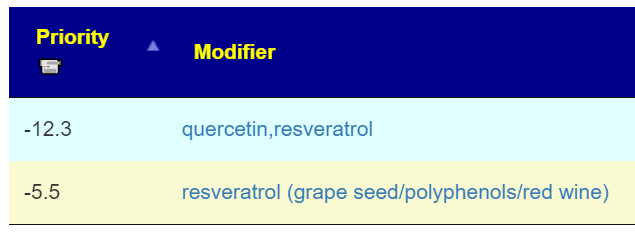
None of the antibiotics or prescription items are above 330; I am disinclined to consider them. During my own recovery, I found that I had a craving for peanut butter (some posts on peanuts: 2013, 2015). There is some evidence that it may improve the ability of the blood to delivery oxygen to the brain in some cases (which may help with cognitive issues). Peanuts do contain Resveratrol [2000] and the question arose below whether just resveratrol alone could be substituted?
Reviewing what he tried…
Ketogenic diet for 6 months… this actually seemed to make my symptoms worse.
I would expect that to make things worse — as shown above.
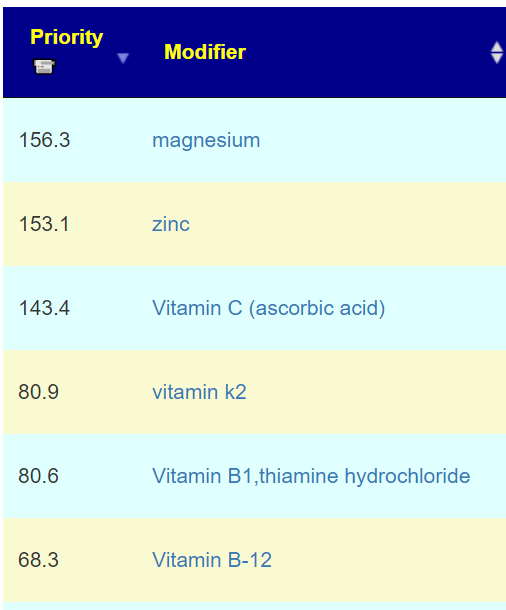
Tried a broad spectrum of high dose supplements, vitamins and minerals that did not help at all.
Remember that 50% of the highest value (540) is my usual demarcation line for suggestions (270). Interesting that not a single vitamin or mineral was even close! About half of them were negatives!
The response from what he tried pre microbiome-sample agrees with the predicted response.
What he should reduce or avoid
This leads us to the next item, items to avoid. They will definitely not sweeten up his life: minimum usage of sugar, saccharin, stevia – but raffinose is fine. Note that nuts are on this list — wait! How can this be? Peanuts is on the to take list. The answer is simple: misnaming. Peanuts are NOT nuts (they look like nuts) but a legume!
Questions and Answers
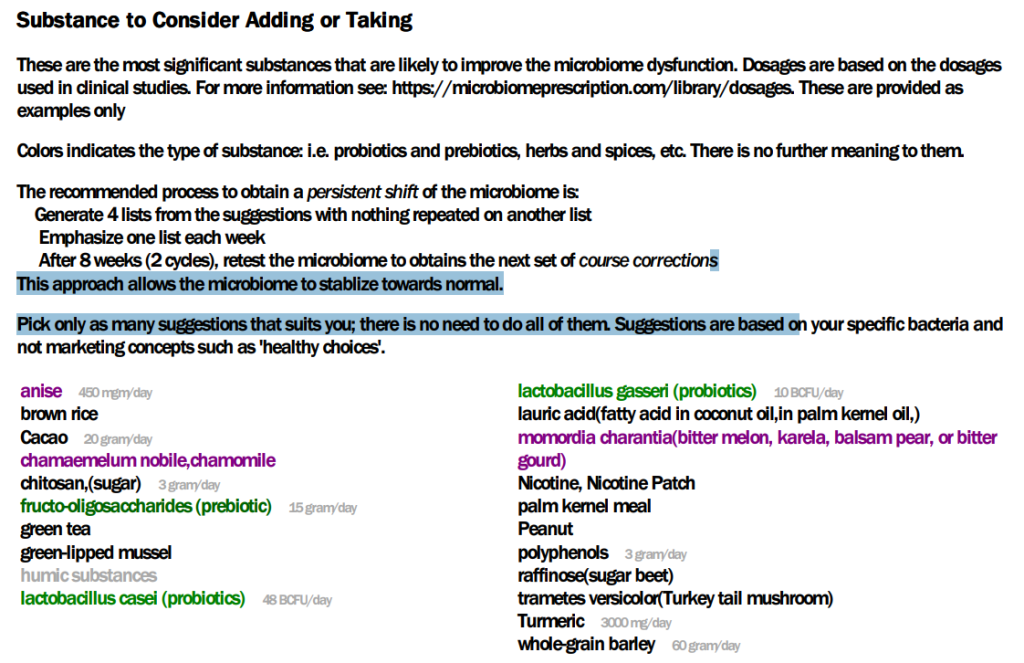
Q: the probiotics dosages stated on the page I was wondering: The page lists the CFUs as X*BCFUs (with the B meaning Billion I suppose?) tho the studies linked to the dosages used mostly dosages in the range of X*10^9 CFUs. Am I missing something? (Because e.g. for lactobacillus casei 48 x10^9 CFUs would seem a lot)
A: I do not know the number needed to insure effective change. The dosages are based on dosages used in Clinical studies and thus dosages that are inferred safe (and someone decided was needed — often the results of earlier studies where only a few responded). See ??️ Dosages for Supplements for links to the studies. There is a difference between maintenance dosages (keep the status quo) and therapeutic dosage (upset the microbiome’s apple cart).
Context for Next Questions
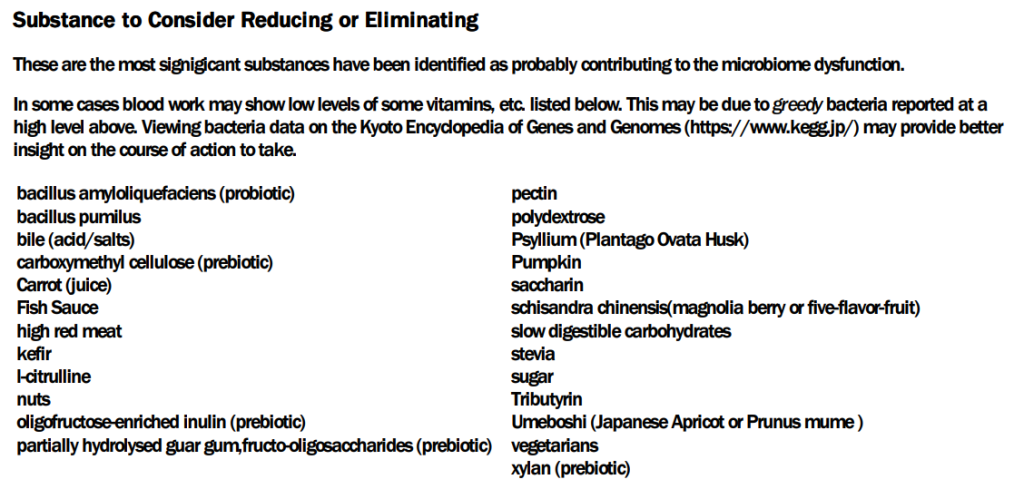
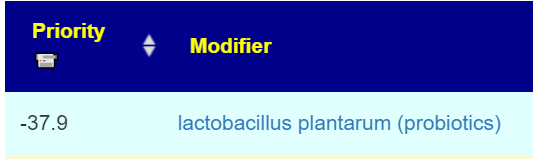
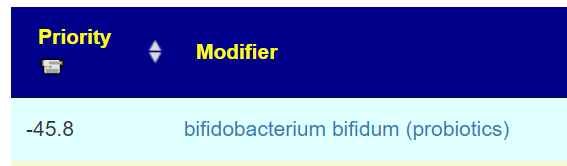
Cookbook Suggestions were created from a list of specific substances provided by a reader supporting Long COVID with some specific directions on how she wanted items evaluated. It is not the preferred list. The preferred methods are looking at the “Technical details” (in horrible complexities — with 1,774 entries for this sample) or using the PDF that filters to keep the number of items low but working off the same numbers.
Q: Cookbook suggestions: Cookbook gave me a clear thumbs down for Bifidobacterium bifidum, and Lactobacillae Rhamnosus and plantarum, tho when I went into detail view or to the consensus suggestions they were ranked well along the other takes. Would you say therefore take or avoid is more recommendable (as I have two probiotics already at home that have these strains in them)
A: As shown above, two are negative (thus avoid), the other one is low positive. (The values range from 539 down to -460). It is unlikely to have any significant impact.
Q: Peanut/ Resveratrol: In addition to eating peanuts, could I also use resveratrol extract to boost the process?
A: This raises the issue of humans wanting to simplify things, sometimes too far. Peanuts contains other things besides resveratrol. This could be it main mechanism of action — but other components may also be acting in isolation or combination. I checked the numbers, and would surmise that the other factors are significant contributors important here. Remember, we are working from very sparse data (despite having 1.9 million facts, we have 20,000 bacteria over 2000 modifiers. i.e. 1.9 million to 40 million combinations is only 5% (or less) hit rate). So, it may help — but not sufficiently to exclude peanuts (or that horrible American food: peanut butter!)
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide solid information on rotations, dosages, etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting. Some suggestions may be counterindicated for other medications you are taking and medical conditions.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
Autism is a variety of conditions caused by DNA mutations, environmental influences and a host of other factors. A significant contributor can be the microbiome. This impact can be further amplified because many children with autism are picky eaters shifting the microbiome further. What is discussed in this post applies to this child and not autistic children in general.
Back Story
A son with autism. He had COVID in April 2021. With autism, it can be challenging to identify long COVID symptoms from autism symptoms. “We have seen marginal improvements in his receptive language and command following. His social skills and emotional understanding is poor . His diet has largely remained the same , vegetables and chicken , lamb, beef or fish and spices. He is verbal but not conversational, does not sleep well at night, does stimming throughout the day, his understanding is minimal He has very good energy levels and is playing till he sleeps on most days. He has very good memory and learn preferred topics quickly but is unable to focus on any task , he is unable to write or hold pencil for long . He cannot always reply to questions and has ecolalia[unsolicited repetition of utterances made by others] . ”
Analysis
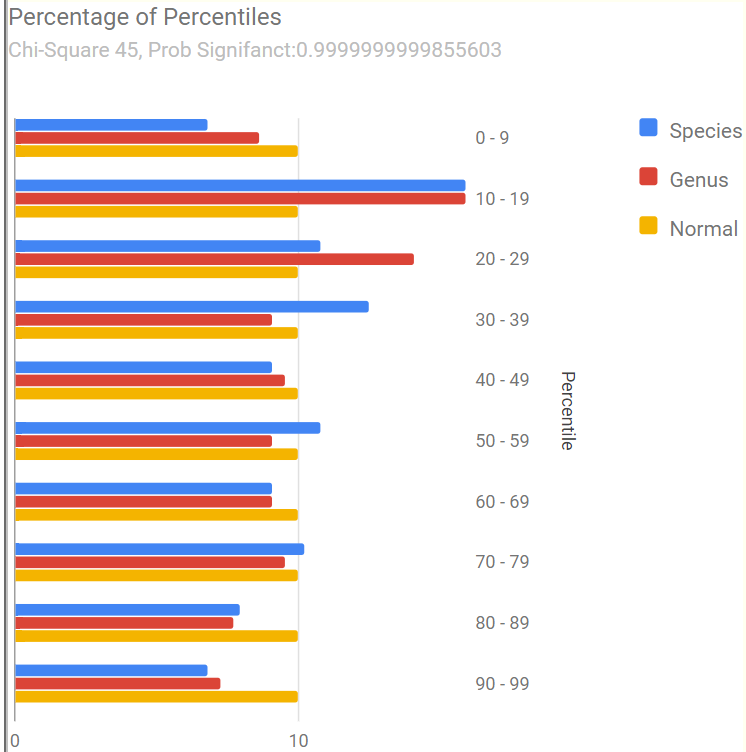
Lookin at Percentages of Percentiles, I see a different pattern than seen with ME/CFS and Long COVID — my most frequent analysis types. He has statistically (between 2 and 5%) significant abnormalities, but far less than people with ME/CFS and Long COVID.
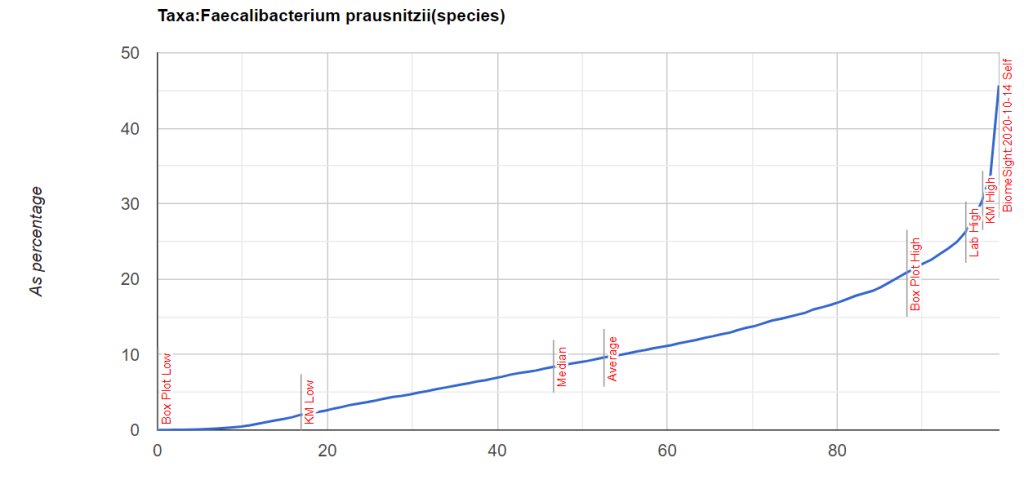
Looking at Potential Medical Conditions Detected we see that ADHD and Mood Disorders patterns are there. Everything is reasonably in range for Dr. Jason Hawrelak Recommendations with two significantly out of range (too low) is Akkermansia (which is available as a probiotic) and Faecalibacterium prausnitzii is too high (27%). This pattern is seen across all of his samples.
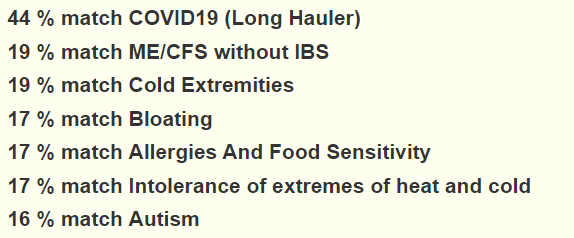
Going over to our Citizen Science Special studies, the top three pattern matches are for:
COVID19 (Long Hauler)
Autism
Brain Fog
These also are seen with an earlier sample from 2020.
Plan for Suggestions
Since this is a persistent state with reasonable continuity across samples, I am going to go the Uber-Consensus route. By this I mean we will do for Each Sample:
“Just Give Me Suggestions” which executes 4 algorithms
Citizen Science using Autism
Then we combine the suggestions from each sample into one, an uber suggestion consensus. The advantage of this approach is to minimize minor fluctuations of the microbiome over time. This means that we have 20 sets of suggestions combined.
I was disappointed with the results — nothing was consistently suggested. I experimented and found that the last two samples gave more consistent results. This implies that there has been significant changes in the microbiome over the last two years.
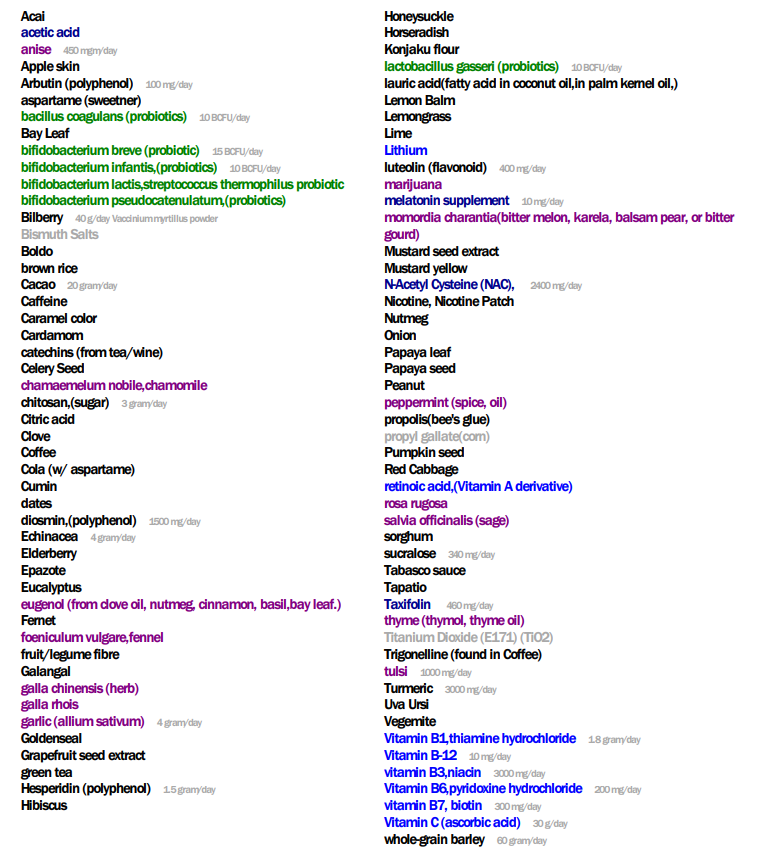
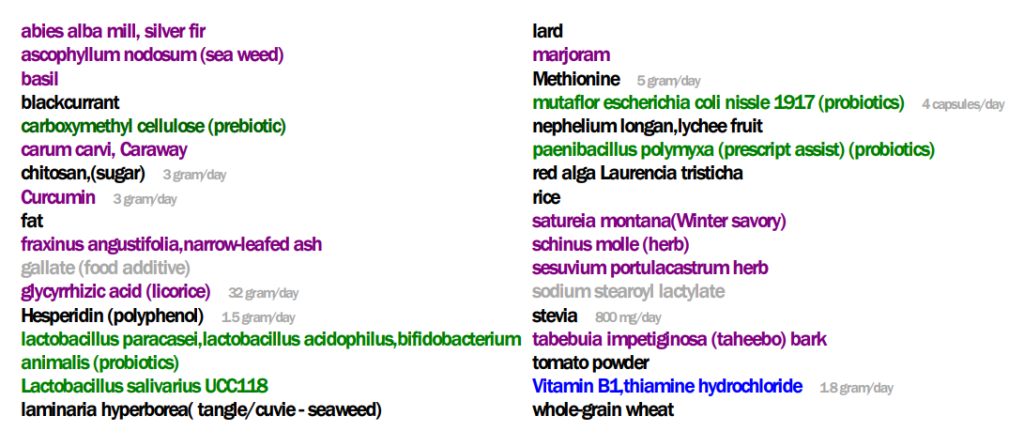
The top suggestions from the PDF are below
As a FYI, in terms of how many times things were suggested:
I should talk a bit about the apparent contradiction with low-fat diets vs lard and fat. These come from the terms that clinical studies used. Low fat diet tends towards fish and poultry, lard is a pork product – I speculate that the type of fat may be significant.
On the flip side, we have these avoids. One item seems to be to suggest gluten free (despite wheat being a to-take):
As an experiment/learning activity — I looked at some of the suggested prescription items and checked if any are used for autism. We are matching these items impact on the microbiome and the shifts that this person has (autism as a diagnosis was not considered).
Since the non-prescription items above should cause similar shifts (and likely with less risk of side effects), it appears that the algorithms are making reasonable suggestions.
The process of checking suggestions derived exclusively from the microbiome against clinical studies for a condition is called cross-validation. When there is a high percentage of agreement, it implies that the mechanism may be via the microbiome and generating candidate substance from the microbiome may produce good results.
KEGG Based Suggestions
These use data from Kyoto Encyclopedia of Genes and Genomes to try to identify substances that the microbiome and the body may be short of which can be obtain via supplements or probiotics.
Probiotics (in decreasing priority)
Escherichia coli – which can be Mutaflor (recommended above) or Symbioflor-2 (which is easier for people in the US to get).
There were several items that are counter-indicated from the suggestions – when there is disagreement, don’t gamble — ignore
Akkermansia muciniphila – low positive score but also identify as low on Dr. Jason Hawrelak Recommendations
Supplements (again double checking across suggestions and keeping only that both agree with)
Q: His gut according to the test is in good condition. I have heard in the past from one of his doctors that his Gut results were one of the best that he has seen in Autistic children, but we have not been able to make a considerable shift in his symptoms in the last few years.
A: My working hypothesis is simple: symptoms are associated to microbiome shifts. He has bacteria shifts that are matches to autism drugs (see above); so I believe further improvement of the gut and behaviors are possible and probable. He may be good; I believe he can be better.
Q: Faecalibacterium prausnitzii is high in my son , I have read it works as anti-inflammatory , but on the contrary I have heard that children with ASD have an inflamed Brian ,I would have thought this would have worked in his favor.
A: Excellent question! Faecalibacterium prausnitzii is anti-inflammatory for Crohn’s disease[2008], colitis [2013]. I was unable to find any clear literature on its effect on the brain. I did found some information that cause me to suspect that it does not impact the brain significantly.
“A 15kDa protein with anti-inflammatory properties is produced by F. prausnitzii, a commensal bacterium involved in CD pathogenesis. This protein is able to inhibit the NF-κB pathway in intestinal epithelial cells and to prevent colitis in an animal model.” [2017] – the size of this is very important.
“Most proteins in the plasma are not able to cross the blood—brain barrier because of their size and hydrophilicity.” [Basic Neurochemistry]
“does not have a barrier against molecules less than 1 kDa.. may form a barrier against molecules larger than 4 kDa” [2020]
Bottom Line — it appears the chemical produced by Faecalibacterium prausnitzii may be too big to reach the brain.
We also find the following reported, suggesting we want to reduce it to a normal range, you should independently research this
“Faecalibacterium predicted social deficit scores in children with ASD” [2018]
“Faecalibacterium prausnitzii … were also found to be highly correlated with Autism Treatment Evaluation Checklist (a measure of Autism severity )”
On the flip side, it reduces abdominal pain and improved bowel movement in ASD [2018].
“Gut microbiome data revealed Akkermansia sp. and Faecalibacterium prausnitzii to be statistically lower in abundance in autistic children than their neurotypical peers with a five and two-fold decrease” [2021] — which may account for the gut issues.
“Compared with healthy controls, Faecalibacterium,..were more abundant in ASD patients” [2021]
Your son’s range is thus very atypical being many, many times higher than expected.
I have caution here, Faecalibacterium and cognitive issues have inconsistent reports [2021, 2023 ], Faecalibacterium is implicated in cognitive issues[2018]. IMHO, encouraging it to the normal ranges may be the wisest course.
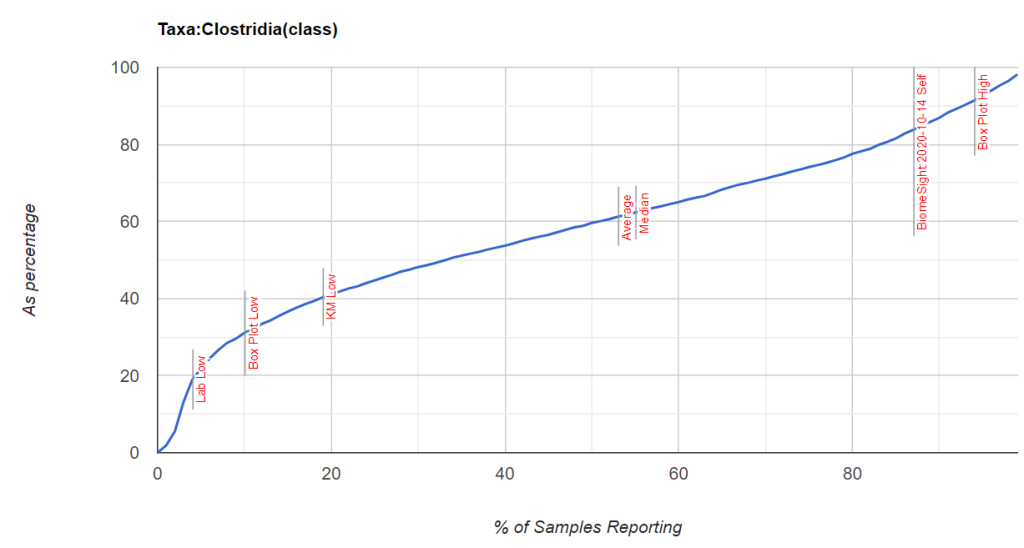
Q: “His results are over all satisfactory ,same as last year about – Gut wellness score – 89.52. I have noticed that Clostridia is about 79.7 % could this be the reason, would appreciate your help.”
A: Clostridia has been high in most samples, I drilled down into it’s main components
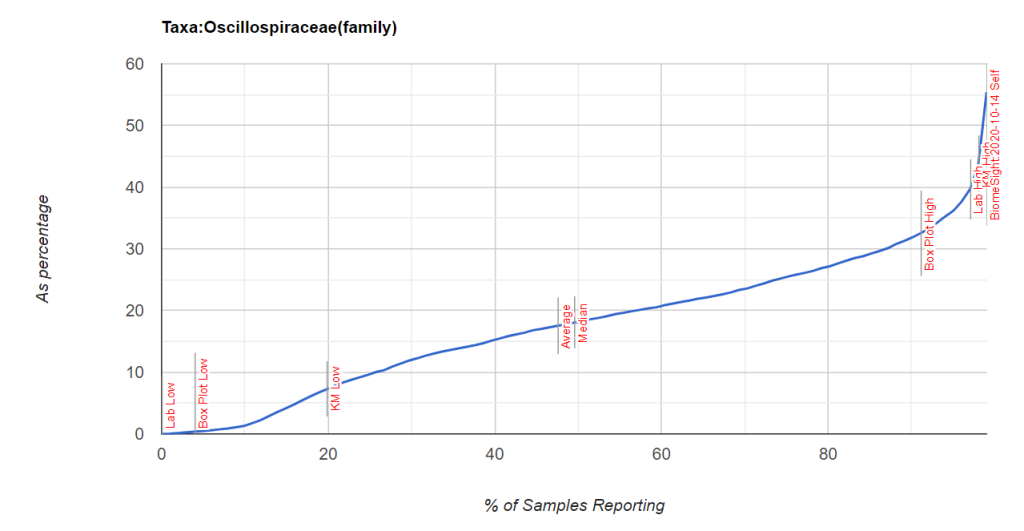
Searching for Faecalibacterium + autism on PubMed resulted in 29+ studies. There was nothing found for Oscillospiraceae + autism. Looking at the latest sample, only 10% of the organisms in Oscillospiraceae could be identified in the sample — no smoking gun for which genus. Doing a Metagenomic Shotgun Sequencingtest would like provide more information (for example, Thorne) — but it is unlikely that will produce more actionable item — just give names.
Looking at what reduces Oscillospiraceae, we see Bumetanide, cycloserine, cefixime and chlorpromazine in that list (as well as many of the above suggestions).
Some visuals: Clostridia is not that extreme, but two of it’s children are.
The question arises, what other conditions are associated with high levels of both of these? Fortunately, this can be obtained from the Microbiome Prescription databases.
Amyotrophic lateral sclerosis (ALS) Motor Neuron
Autism
Crohn’s Disease
Depression
Graves’ disease
Inflammatory Bowel Disease
Irritable Bowel Syndrome
Juvenile idiopathic arthritis
Liver Cirrhosis
Long COVID
Metabolic Syndrome
Mood Disorders
Multiple Sclerosis
Obesity
Parkinson’s Disease
Psoriasis
rheumatoid arthritis (RA),Spondyloarthritis (SpA)
Schizophrenia
Stress / posttraumatic stress disorder
Type 2 Diabetes
Ulcerative colitis
I also pulled the studies where the study specifically cited both are high. The above list were occasionally from taking data from two different studies.
A responsible medical professional would test a patient’s Lactobacillus and Bifidobacterium levels beforesuggesting probiotics to a patient. If your MD makes that recommendation without testing and you have any of the above conditions — it may be time to file a complaint with their supervisors or governing body citing the studies.
A reader forwarded me a study and some of it was interesting hints on this issue.
In vitro experimental results show a potent inhibitory effect (greater than 90%) of chloroquine, a historical antimalarial active ingredient, and clavulanic acid, a β-lactam antibiotic widely used in combination with amoxicillin [80]. A significant inhibition of the enzymatic activity has also been observed with the antihypertensive drug verapamil and the histamine H2 receptor antagonist cimetidine, although the clinical use of the latter is currently anecdotal
My idea is to examine which bacteria these items impact and see if there is a pattern.
The full list is below
Active Ingredient
Indication
Chloroquine
Antimalarial
Clavulanic acid
Antibiotic
Colistimethate
Antibiotic
Cefuroxime
Antibiotic
Verapamil
Antihypertensive
Clonidine
Antihypertensive
Dihydralazine
Antihypertensive
Pentamidine
Antiprotozoal
Isoniazid
Antituberculous
Metamizole
Analgesic
Diclofenac
Analgesic and anti-inflammatory
Acetylcysteine
Mucoactive
Amitriptyline
Antidepressant
Metoclopramide
Antiemetic
Suxamethonium
Muscle relaxant
Cimetidine
Antihistamine (H2 antagonist)
Prometazina
Antihistamine (H1 antagonist)
Ascorbic acid
Vitamin C
Thiamine
Vitamin B1
We have 14 items that we have data on.
At the family level, the following at the commonly impacted — all were decreased.
Bacteroidaceae – 14
Desulfovibrionaceae -14
Enterobacteriaceae -13
Clostridiaceae -13
Peptostreptococcaceae -13
At the genus level we have these all at 14 matches and decreasing
Bacteroides
Bilophila
Lawsonia
Desulfovibrio
Anaerorhabdus
Desulfocurvus
Desulfobaculum
Halodesulfovibrio
Mediterranea
Pseudodesulfovibrio
Desulfohalovibrio
Desulfocurvibacter
There are no clear smoking guns. When we include Special Study: Histamine or Mast Cell Issues we see that histamine issues are associated with lower levels of many bacteria (where as the above are those implicated in higher levels). We also looked at histamines in Exploration: Salicylate Sensitivity And the Microbiome, where we see under detection usually being the characteristic for histamine issues (except for Rothia mucilaginosa.
Doing cross checking, we find that the following are not reported impacted by the above AND are low in the other studies:
Methanobacteriaceae (family) – none
Heliobacteriaceae (family) – none
Anaeroplasmataceae (family) – none
Desulfocella (genus) – none
Spirosomaceae (family) – none
Rhodocyclaceae (family) – none
Cytophagaceae (family) – none
Ezakiella (genus) – none
Halobacteroidaceae (family) – none
Burkholderiaceae – only 1 impacts
Limosilactobacillus – only 10 impacts
All of the “none” are most likely due to this family or genus not be measured in the studies used. This leaves one bacteria of interest: Burkholderiaceae.
Bottom Line
We have no clear pattern. The drugs at the top likely makes room for bacteria that are low in frequency and amount to grow. Our attempt to find the bacteria ignored by the drugs above AND which are seen at low levels only turned up one candidate with a manual review: Burkholderiaceae.
Writing code to drill deeper may find more — stay tune.
I am newly ill from ME/CFS (4-5 months) and wonder if my results look like a “typical ME/CFS” for you, or Long Covid for that matter. I am a bit confused and some of the recommendations are contradictory.
From Reader. He used Biomesight.com (serves the world, discount code “Micro”)
This will be an interesting analysis — the microbiome evolves over time, so a 20 year ME/CFS and a few months of ME/CFS will have differences. I know of no clinical studies looking at “fresh ME/CFS”. There are studies for “fresh Long COVID”.
Percentages of Percentiles
This tend to have a regular pattern for ME/CFS and Long COVID for most people. Over representation of bacteria in the 0-9% percentile range. This matches his pattern. A healthy person would have all of the bars around 10% – they are not.
Going to the Potential Medical Conditions Detected, there was nothing significant. Prevotella copri is 2% (78%ile) which is borderline for mold issues — it would be good to do inspect the home for that risk. Dr. Jason Hawrelak Recommendations comes in at 99.7%ile with high Methanobrevibacter and low Bifidobacterium being the most severe shifts. Anti inflammatory Bacteria Score is 63.1%ile which is a bit better than most people. So, many medical professionals would tell the patient that I cannot see anything wrong.
Special Studies
Special studies are statistical studies that uses samples uploaded and look at the self-reported symptoms. The analysis is done individually for each lab (needed because of differences in how labs process samples). In this case… we see that COVID Long Hauler is by far the strongest match, almost double the next one.
I did the usual Just Give Me Suggestions and then did the Long Hauler suggestions . This gave five (5) packages of suggestions. I then looked at the antibiotics suggestions, focused on those used with ME/CFS. The top ones are:
The list of suggestions to take is actually bigger than usual.
REMEMBER: There is no need to take all of them, just take what works for you (i.e. no adverse effect and acceptable cost).
Probiotics should be rotated (change to a different one) every 7 to 14 days. Probiotics often work by producing natural antibiotics. Continuous taking of the same probiotics may result in it not working because of “natural antibiotic resistance”.
The colors have no meaning except as indicators for category. For example, green is probiotics
Dosages are those that have been used in clinical studies (for other conditions), and thus deemed safe dosages. Often I have see people taking < 1% of these dosages and wondering why nothing happens.
For example, it you are lactose intolerance, then ignore the lactose suggestion. If not, regular cups of good Belgium Cacao would be a good prescription!
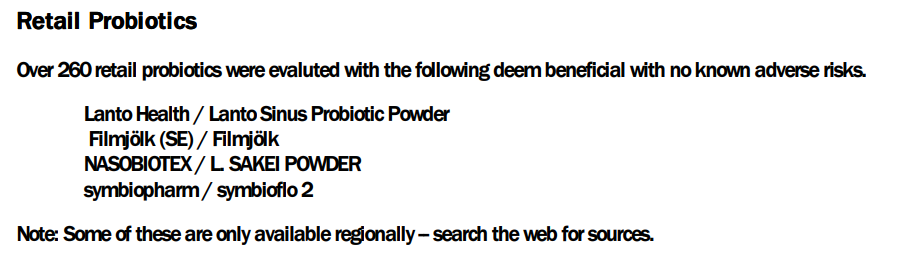
The safe retail probiotics were calculated to be
symbiopharm/ symbioflo2 – an E.Coli probiotic from Germany
Filmjölk (SE) / Filmjölk – a Swedish milk drink
enterogermina – Bacillus Clausii
SunWavePharma / Spor Sun – Bacillus Clausii
Why are these lists not the same? The latter list are ones that will not shift a single one of the bacteria we are focused on in the wrong direction: NOT A SINGLE BACTERIA. This is an extremely safe conservative suggestion. The top list with probiotics in green often contain probiotics that shifts 30 bacteria in the right direction and 3 in the wrong direction. The odds are that they are very likely to help.
We have a third list of probiotics (to make probiotic suggestions even more confusing), the KEGG suggestions. This looks at what enzymes your microbiome are low in, then sees which probiotics can provide those enzymes. Our goal is to reduce enzymes starvation; this cascades in metabolites — chemicals that the body uses — starvation. The key items from this list are:
If you have significant brain fog, I would be careful with taking lactobacillus probiotics. Some retail species can increase brain fog.
The Avoids
Frequently “good suggestions for general health” are bad for some conditions. The avoid list of things to avoid is short
Some quick translation: no iron supplements (ferric citrate), beta-glucans usually means no oats, barley or Reishi mushrooms. The names are those used in clinical studies — so they tend to be “unresolved” often in common speech.
Suggested Cycles
After implementing the above suggestions for 6 weeks, do another test and see what has changed.
Questions and Answers
Q: Is it best to take the antibiotics + the protocol you suggested ? Or is it one or the other?
A: My own choice would be to do both at the same time. If you follow Jadin’s approach, then
First week of antibiotics per month — no probiotics at the same time
Second week do some of the probiotics (I am inclined towards the E.Coli probiotics but that is based on my personal experience — your mileage may vary)
Rotate the other supplements over the weeks. I would suggest 10 days and then change to a different set.
Q: And lastly, in the « Avoids », the « vegetarians » suggestion is a little confusing to me. What does it mean?
Vegetarians mean no animal or fish is being consumed. So, have fish — but some animal proteins are to be reduced: no pork, moderate beef. Duck, chicken and rabbit are fine.
Q: The suggested dosage in the suggestions seems very high. 30g of Vitamin C per day??? Is this correct ?
The actual dosage should be discussed with your medical professional. The dosages are the highest that have been done in clinical studies and thus assumed to be safe dosages. We have no data on what the threshold for an effective dosage should be. I have seen a few studies where 1000 mg of a substance has minor/no effect while 1100 mg has twice the impact and 1200 mg has four times the effect. For many substances there seem to be a threshold that triggers changes.
Usually start at 1/8 of the dosage and double it every second day until there is a response. If very good keep at that dosage. If bad, cut the dosage in half and try a few more days. Give the body time to adapt.
My comment about mold caused him to check his environment carefully…. what he found out of sight!
“Environmental factors – exposure to mold or toxins has been suspected as a trigger for ME/CFS. However, associations of specific environmental factors with ME/CFS have not been established.” [CDC]
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide solid information on rotations, dosages, etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting. Some suggestions may be counterindicated for other medications you are taking and medical conditions.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
This is from a reader that I have been corresponding with since 2017 and known from online groups for decades..
Okay, you don’t want the full saga 😀 (joking ) and so I’ll write the first current impressions of a ME/CFS patient since 1998. I am someone who has tried everything; really everything. First of all, as I had already told you in chat, I use as a criterion of improvement in the disease the increase in cardiovascular tone, which actually happened for a short time as long as I kept a diet that was not exactly ironclad, but very difficult for me: it involved cutting out all refined sugars.
For those interested, I talked about it here : https://www.fable.it/fluorochinoloni-hrv-dieta-e-me-cfs/ (in Italian — use Google translate) . For the first seven days of the diet nothing changed, nothing! After these 7 days suddenly, keeping to this diet , cardiovascular tone started to increase until … well … I kept the rest of the diet but reintroduced sugars (but not alcohol). Then improvement stopped (but maintained existing improvements).
From Reader
Recent significant events are:
fluoroquinolones toxicity in 2020
supplements of akkermansia muciniphila one month before last sample (see below for his experience)
Ancient Test Results
A test result from 23 August 2016 is below. The test is only of a few bacteria without any ranges of normal valid. We will compare the few items reported with the latest Biomesight test. There was little change over 7 years.
Any persistent Fluoroquinolones artifacts?
I did a behind the UI comparison of what Fluoroquinolones changed with his sample. Although it has been 3 years, I am curious. No impact would have 50-50 agreement. We have 64 bacteria showing the effect that that Fluoroquinolones would cause, and 43 showing the opposite effect. This results in a P-Value of 0.0423 from chi-square. A P-value below 0.05 is deemed statistically significant in medical studies. So, this is evidence that the impact of Fluoroquinolones is still there after 3 years.
This is an interesting observation — picking the wrong antibiotic may have effects that persists for years.
The microbiome was been relatively stable over 7 years. In fact, the Biomesight test clarify how extreme the values are (which is not clear from the earlier report).
Where do we go from here?
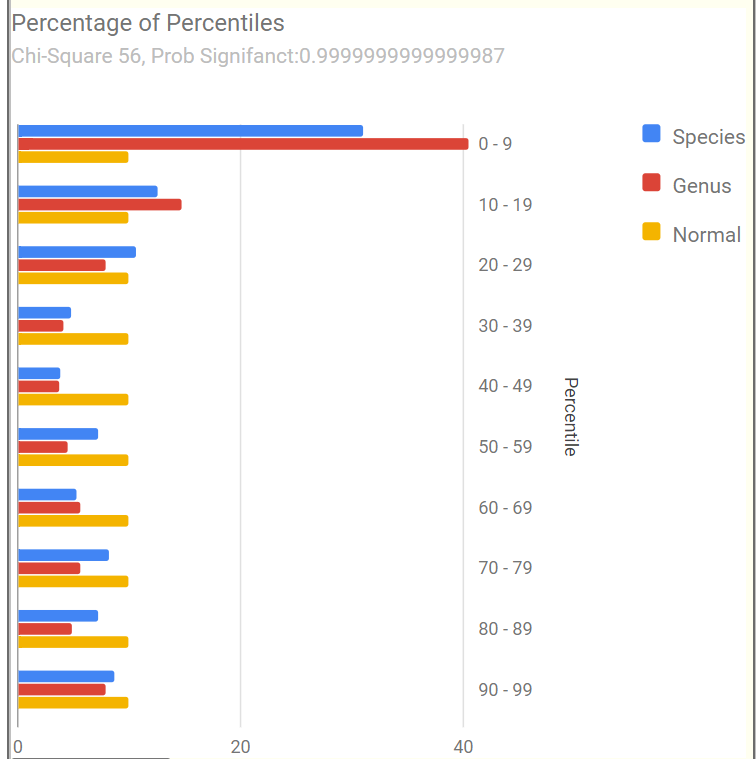
The Percentage of Percentiles pattern shown below is a match for that seen with many ME/CFS or Long COVID microbiome.
Nerdy Explanation: Using percentiles, the data is transformed to an uniform distribution. An unbias sample (a.k.a. normal or healthy), would have the same number in each 10%ile range. We do not. We have the typical spike in the 0-9%ile range (i.e. too many species and genus that have token representation).
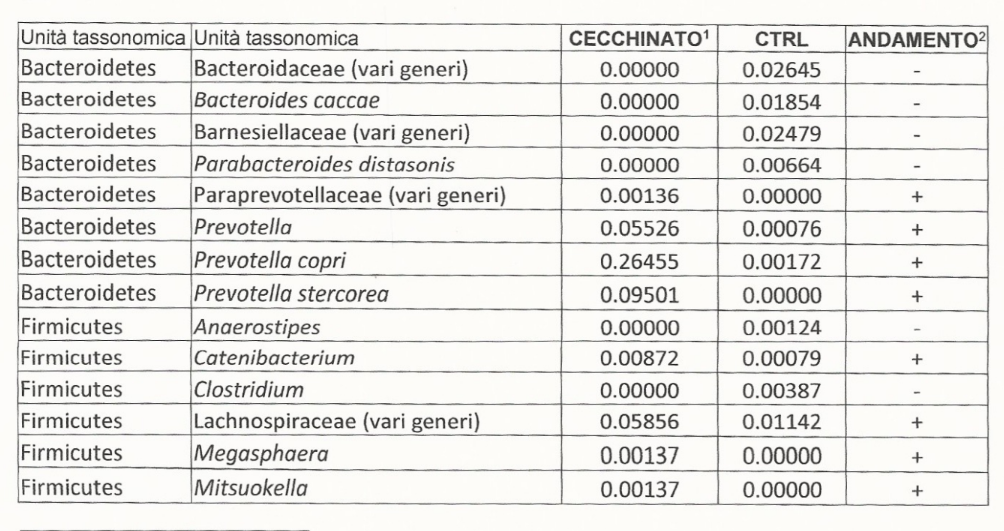
The most important/concerning bacteria identified was Prevotella copri. This bacteria made up 43% of the microbiome!!!! This bacteria is often associated with mycotoxin being present in the environment [2020]. This usually means examining the living space for mold and fungi, as well as avoiding foods likely to have mold (see WHO for more information). His response to this comment was:
Yes, I live in a north-oriented flat where never there is sun on walls. Only in a bedroom not used anymore as bedroom I have visible mold (picture attached). I have tried treating with chlorine bleach. In February 2023, I called a painter. He treated with anti mold solution and thermal painting (which can ben dangerous. I would never lived in that bedroom till the smell went away. And yes, sun recharge me and I don’t know if it also affects mycotoxins. However in my block / area where I live, we never have less than 60% humidity, but in summer usually we have 70-75% so… humidity is a concern.
From Reader
There are many sites providing suggestions on this issue, a few are: [Aircare Hawaii] and this
Is mold related to humidity? European and Italian homes are typically built with reinforced concrete frames and brick walls. Walls and ceiling surfaces are finished with mortar/plaster and water base paint. As water base paint is not waterproof, plaster finishing tends to absorb and retain humidity. These areas can become damp or wet as a result of a water leak or condensation of vapors produced by appliances and normal household activities.
The use of a waterproof paint after cleaning (and running a dehumidifier) in the bedroom is one possible approach. Reader responded (to his delight) that water proof paint was used!
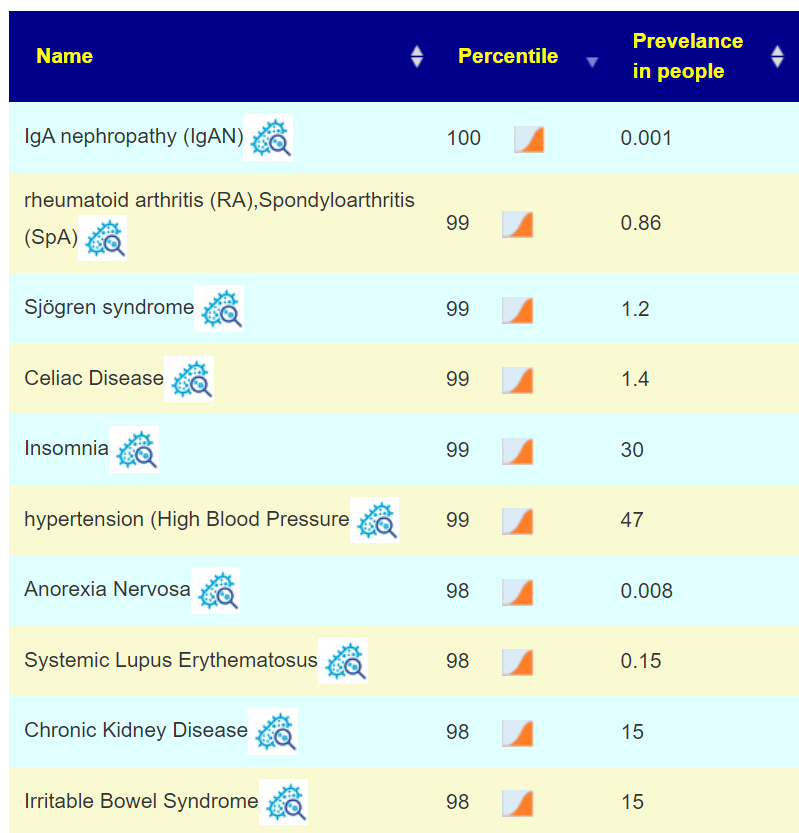
This plus other shifts, matches to a host of conditions shown below. Many are co-morbid with ME/CFS.
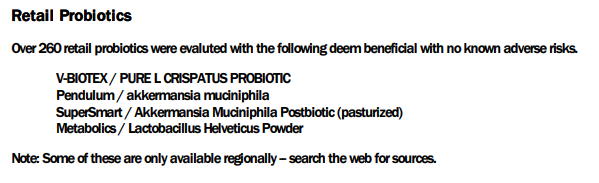
The Computed Probiotics from KEGG Enzymes had some very high numbers (over 600!). High numbers mean that there count of many enzymes is very low. Some of these are available in probiotics, with the top feasible suggestions being:
I will defer the rest of the suggestions to the PDF, attached below. It is interesting to note that akkermansia muciniphila probiotics is well recommended (see experience below).
In this case, we have good positive reader experience happening before the suggestion was made! It should encourage the reader to trust the other suggestions (after all, “one suggestion worked before he got it!” 🙂 )
None of these are typically used for ME/CFS (but other tetracyclines are). We have one big target: P.Copri. I am hoping that you have a cooperative MD. I checked around for information on antibiotics that often have little effect on P.Copri, these studies have extensive lists.
I am inclined to metronidazole, which is often used in treating ME/CFS (also in this 2010 study), and 98% effectiveness reported in this 2019 study.
Akkermansia Muciniphila Experience
Another thing Ken, is the sensational discovery this year of Akkermnasia Probiotics (in my case from Metagenics). In my first two days I went from going to the bathroom once a day to going three four times. How many times have we read that a normal bowel transit involves 1 evacuation a day to one every 2-3 days ? No ! The ideal transit is to go to the bathroom about half an hour after eating ! Well, this happened to me while supplementing Akkermansia once a day. And it is only one strain !!! Not only that ! I felt less “Fight or Flight” but more serene, even when I woke up from my night sleep. Even with scabs on my eyes that who knows how many years I haven’t found (how many of us have perpetually dry eyes ?). I stopped the supplementation after a month and am now resuming it.
Why am I writing you this Ken ? To waste your time !!! No, I am writing this to you because I had first read about this Akkermansia three years ago on the label of an Austrian product, Omni Logic Plus, which contains a lot of good stuff (FOS, GOS , etc.) to feed this specific bacteria, Akkermansia . Three years of supplementation every day has not improved anything. After just a few days of Akkermansia , that is, the strain that that Omni Logic Plus was supposed to feed, did the miracle ! What do I mean by all this ? That , my thought is that rather than acting on the food, if they are available as supplements, little bacterial strains should be introduced, for a far better effect.
From Reader
Questions:
Q: When the “nutrients” of the supernumerary bacteria present they grow. If you cut off their nutrients, the effect on microbiota diversity is extremely “reactive” !!! Whether this happened when I removed the sugars ?? Do you agree with my reasoning ?
A: Yes — consider a human population that is well fed (obese even). If you suddenly impose strict rationing on them, their behavior changes greatly (often with criminal actions).
Q: Is it more effective to remove the food that feeds the overrepresented bacteria and simultaneously supplement the underrepresented strains not so much with diet and food, but with probiotics ? An example of my personal case ? When in the report generated by your site I see among the recommendations clostridium butyricum , which I never tried in my life.
A: The algorithms effectively does that — identify the material that inhibits the overrepresented which do not impact the underrepresented. Also the reverse, feed the the underrepresented without feeding the overrepresented. You can try to calculate these manually — but its a massive amount of reading and searching. Microbiome Prescription uses some 1.8 million facts pulled from almost 12,000 studies.
Q: Who knows if it can give me the same benefits as Akkermansia? After years where weeks on end , I have tried various products. Like everyone else, I have been spending hundreds of Euros. For example:
probactiol duo ( billions of Saccharomyces boulardii)
A: The purpose of Microbiome Prescription is to compute the most likely ones based on your microbiome and what studies reports the effects of various probiotics are. This means greatly increased odds of positive effects! Much better (and cheaper in the long run) than trying things suggested by influencers or which worked for someone with a very different microbiome.
Your list is very short — 50% is what you recently discovered works!!
For probiotics, do one at a time for 10 days then rotate to another. Why? Their effect is often due to natural antibiotics that they produce. Keeping on them continuously allows “natural antibiotic resistance” to develop.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide solid information on rotations, dosages, etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting. Some suggestions may be counterindicated for other medications you are taking and medical conditions.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.





Recent Comments