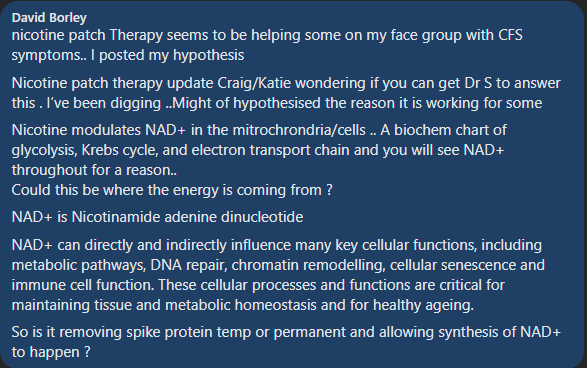
Nicotine often shows up in suggestions. On some people, quite high. It was included because we include everything we find studies for (including Round-Up!). Then I got a reader with ME/CFS who found that nicotine patches caused a major improvement. Then I saw someone mention that 30 years ago, smoking/nicotine was suggested by some MDs to stop UC’s Flares.
nicotine modulates the immune system, inhibits innate and acquired immunity and is used in treating many autoimmune diseases. It often stimulates the α7 receptor and causes an anti-inflammatory state in the body. This study is designed to evaluate the role of nicotine treatment on immune system. The results showed that nicotine affects many cells in immune system, alters the downstream intracellular mechanisms and changes lymphocytes polarization.
Smoking tobacco is associated with a number of gastrointestinal disorders. In some, such as Crohn’s disease and peptic ulcer disease, it increases the risk of disease and has a detrimental effect on their course. In others, such as ulcerative colitis, it decreases the risk of disease and can have a favorable effect on disease course and severity.
Ulcerative colitis (UC) is predominantly a disease of non-smokers and treatment with transdermal nicotine improves symptoms in UC patients, whereas smoking seems to have a deleterious effect in patients with Crohn’s disease (CD).
Anecdotal reports suggest that smoking may be beneficial for patients with inflammatory bowel disease (IBD) as nicotine may act through inflammatory mediators within the colonic mucosa….Moreover, concentrations of IL-1beta and IL-8 were significantly reduced in smokers with UC compared with nonsmokers with UC.
In this relatively small study of patients with active Crohn’s colitis, 6 mg nicotine enemas appeared to be of clinical benefit in most patients. They were well tolerated and safe.
It appears that smoking is bad for Crohn’s, but nicotine may be beneficial. Most studies are on smoking and not nicotine in isolation. IMHO, the suggestion of nicotine is probably a valid (and unusual) one.
Microbiome Prescription computes items that are likely to cause positive shifts in the microbiome. These positive shifts are expected to reduce symptoms and symptom severity. This is only part of a treatment plan. How much to take? When to take it? Interactions between suggestions are clinical issues that are usually based on clinical experience. We do not have that wisdom.
We can provide some guidance from the literature:
List of dosages used in clinical studies for many items are available here ??️ Dosages for Supplements. Our general suggestion is to use the highest dosage by starting at a low dosages and slowly increasing.
We provide information about interactions of various items with probiotics. Our general suggestion is not to take items together that conflicts. For example, taking an antibiotics or herbal oil/extract that reduces a type of probiotic with that probiotic. Wait until the course of antibiotics or herbal oil/extract ends, then take it (to help restore the lost population).
Our thinking has been greatly influenced by the work of Cécile Jadin, MD – who is a surgeon. She applied models from her father’s time at Pasteur Institute of Tropical Medicine when he worked with a Nobel Prize Winner. She has had over 25+ years treating difficult conditions: ME/CFS, Chronic Lyme Disease, Chronic Q-Fever and Rickettsia infections. See Dr. Jadin’s Current Protocol for ME/CFS
Our general interpretation of her model gives us some general rules to follow are:
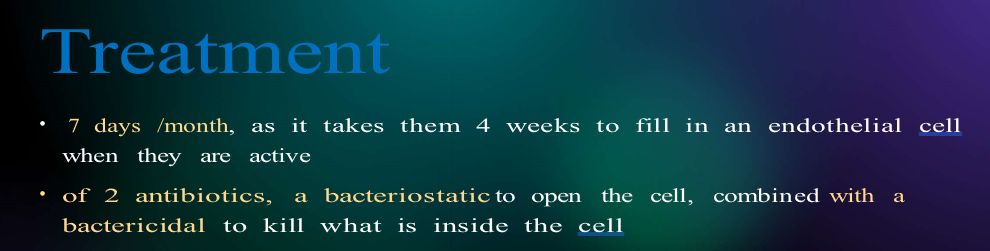
Pairs of antibiotics for 7 days and then 21 days off and then different ones for the next month
Antibiotic means prescription antibiotics AND Herbal antibiotics.
Typically two dosages a day, 12 hours apart
See Jadin’s notes for her suggestions of things not to do with certain antibiotics
Probiotics should be viewed as antibiotics (many produce natural antibiotics)
There are good and bad probiotics. You do not want to play Russian roulette with a mixture of both good and bad.
Caution: for me, some probiotics at bed time will cause deep sleep (with night sweats on some) while others will make getting to sleep hard. Adjust the time to your response.
A 4 week cycle may look like this:
1st week on a pair of antibiotics,
2nd week on a herbal oil or extract
3rd week on a probiotic — ideally a single species probiotics at desired dosage
4th week rest
At the end of the 4th week, take another microbiome sample. We want to have some natural stabilization of the microbiome before the next course correction.
If no antibiotics are involved, then do a different herb or spice instead. My personal preferences are two from the following list (make sure they are positive for you):
Wormwood
Olive Leaf Extract
Neem
Triphala
Tulsi
Amino acids and vitamins can usually be taken continuously.
Pre- and post- biotics should be started with the probiotic AFTER verifying that it increases the probiotics selected (see tool above). Example for Human milk oligosaccharides is shown below.
Picking items on Suggestions
We are walking thru a vast desert devoid of good studies with a few oasis. We compensate by using fuzzy logic. In keeping with increasing odds, my usual advice is to look at the highest priority item number and divide by two. Those over half (50%) of this should be your main focus. Similarly, look at the most negative item and those more negative than half of that are items to reduce or eliminate. For example:
Highest Priority: 800, look at items between 400 and 800
Lowest Priority: -450, look at reducing items between -225 and -450.
Review with your Medical Professional
At least, inform them of what you are going to do (by email, message or letter) and ask “Do you see any problems?”. 99% of the time the response will be silence, or a “I don’t see an issue”. If something goes wrong, you have a defense against a blame game….
Finding a knowledgably experienced medical professional is a challenge. Often the reality is that you have to educate your medical professional which is a slow process. My usual strategy is to bring in 1-2 summaries or papers printed from the US National Library of Medicine each time after finding a medical professional that is interested in learning more (i.e. no burn out, patient exhaustion, etc.).
Cécile Jadin, MD, has very graciously put together a power point on the state of her protocol and allowed me to share it. This protocol has been in use for over 25 years by her with a high success rate (90%). The protocol actually dates back around 50+ years (for a condition with a different name).
For earlier notes from her, see C.Jadin Resources which links to some of her earlier presentations.
My Experience
The basics of this protocol put me into remission around 2000 and has put me into remission for flares. Far more important, it resulted in my understanding the complexity of this condition’s treatment. Even today, I view many MDs keeping to a naïve one-shot magic-bullet approach: “we need to find the virus (i.e. EBV, HHV6, etc) or bacteria that triggered it; find a drug to treat it and the patient is cured!” I have read so many accounts of people being “cured by X, but it stopped working after N months and X does not work anymore”.
Dr. Jadin has many decades of clinical experience treating ME/CFS and related conditions. She built upon clinical experience treating this type of condition. I have decades of doing software development.
Jadin and I are two sides of a Treatment Coin
Cécile Jadin is a MD with decades of clinical experience treating ME/CFS applying and evolving a protocol that she inherited from her father’s time at the Pasteur Institute of Tropical Medicine. I am a high functioning autism person well trained in Artificial Intelligence and Statistics who has applied it to the microbiome. My AI algorithm very very often suggests the same set of antibiotics and supplements that she uses. The algorithm works off bacteria only (and thus ignores many other co-factors). We walk different paths and end up in the same treatment approach.
She talks about Obligated Intracellular Organism or OIO. This term may be unfamiliar to many, for some background readings see this Research Topic on Frontiers. I talk about the bacteria in the gut.
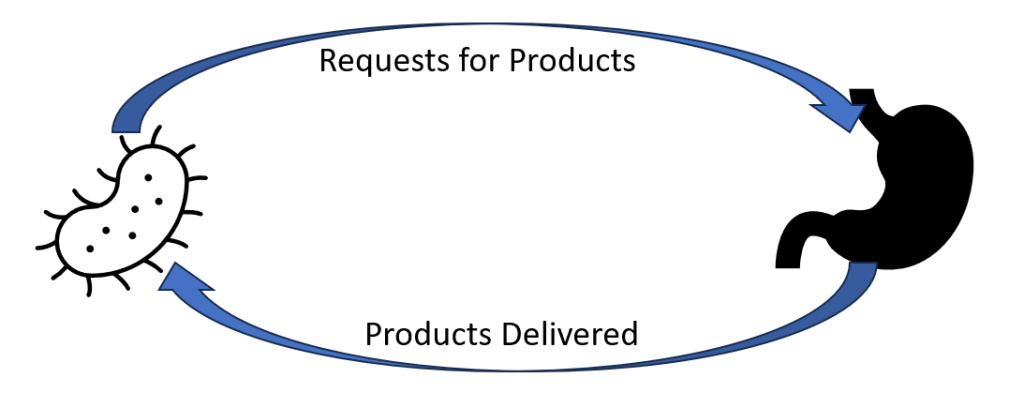
They are very interconnected with a lot of information exchanged between them. OIO sends mis-information messages to the gut to produce more of this or that enzyme, metabolites, compounds [Products]. There are over 26,000 different products potentially involved. The gut receives this information and fill these bogus orders. The OIO gets its supplies and proceed to prosper. A side effect of these bogus production orders are symptoms – they could be view as pollution from the production. The symptoms often depends on a person’s DNA.
This cycle needs to be broken. This may be done by attacking the command center (the OIO) or attacking the factories (the microbiome) or both.
Original Motivation
One of the goal of building my AI was to try to identify the factors for non-responders. To me, it appears to be due to variations in the microbiome. Recently there has been many studies reporting that the difference between responders and non-responders for both cancer treatment and the severity of COVID has been the patients microbiome. The AI can suggest what to take; Jadin’s clinical experience provides information on how to take it.
Remission is the Target, not who is right
Patients and their MDs can go down two path, the paths actually run besides each other.
Follow Cécile Jadin process and protocol precisely
Follow Cécile Jadin process but use iterative sets of suggestions from Microbiome Prescription. By that, pick 1-2 of the top CFS tagged antibiotics, then at the end of first month, take a new microbiome sample and start with the secondary CFS tagged antibiotics (while waiting for the results).
The latter approach can be tried without prescription antibiotics because it identifies probiotics (that often produces natural antibiotics) and herbs (with antibiotic characteristics) and thus allows self-treatment for those without a cooperative medical professional. This no-antibiotics approach will likely work slower for most people. I discourage self-treatment, but often there is no alternative. My first choice is keeping strictly to clinical experience using the microbiome suggestions to select between clinical alternatives.
The Cécile Jadin’s process of alternating substances with breaks is a critical factor. In terms of modelling effectiveness (my expertise) — there is no question, it is the rational approach that treats everything as living entities and not mechanical nuts and bolts.
Video Presentation by Cécile Jadin
Short Version (35 minutes)
The bare presentation.
Long Version (65 minutes)
This version includes questions and answers from participants(and chit-chat). Her presentation starts at 5 minutes into it. At the end a patient shares her experience after the first 3 months.
Power Point as a PDF
You may download her presentation below as a PDF file. Or listen to it on YouTube which is intended for people having difficulty reading (common symptom with ME/CFS).
“All those antibiotics MUST be taken: after food ( not only water ) and without any dairy products. Patients must avoid sugar intake and some supplements(for example magnesium, glutamate, vitamin D). Antibiotics should be taken in the morning and the evening”
“Duration of treatment: 1 – 3 years.” Symptom remission may occur sooner, but that is usually just a tactical victory and not a strategic victory. You won one battle, but the war is not over.
Probiotics:
“Taken at noon only. No specific ones, but they must also be rotated (like the antibiotics)”
Many of these conditions can be transferred from human to human with someone who has never been to Africa having an OIO and those can be unknown in your country (without lab test facilities being available) but they are well known in Africa or South America. You may be told: “So, we have run tests for everything and everything came back negative — you have an atypical condition with no known treatment”.
Bottom Line
Medical treatment suffers from one dimensional linear thinking that often uses a “nuts and bolts” mechanical model. The model and understanding of Dr. Jadin assumes a living organization that changes and adapt. The problem bacteria (be it OIO or microbiome) will literally play hide and seek with treatments. I share this perspective.
Some Possible Paths Forward
Depending on the cooperation of your MD, availability of detailed microbiome tests, etc.
Follow Dr. Jadin protocol
Follow the path being discussed in the Remission Biome Project:
Using Microbiome Prescription to generate a list of candidate antibiotics and then take the highest ranked on that which is on Dr. Jadin’s list – following Dr. Jadin’s pattern of alternating and pulsing
Implement the non-prescription suggestions of to avoid or to take. That targets the factory side (that is the gut microbiome), not the OIO side of the cycle show above. It simply improves the odds.
Do not use antibiotics (either by choice or by lack of cooperating MD) and use the advanced suggestions based on your microbiome sample with a new microbiome test every 6-8 weeks. Each new test will alter suggestions (especially probiotics). All suggestions should be reviewed by your medical professional. See this post: We can suggest what to take, but not how to take! for a more explicit description.
Whilst a quick apparent remission may occur, Dr. Jadin’s opinion is that you need to keep to it for at least a year, in some cases up to 3 years. Having a remission that lasts 3 months and then relapses makes the next remission much harder to obtain.
A current project using antibiotics has two analysis done showing significant subjective and objective improvement.
Q: “this doesn’t address the causes of ME/CFS. Also no mention of any nutrient deficiencies typically seen in every case of ME/CFS I’ve seen, or genetic factors, or anaemia, or thyroid dysfunctions, or other causes and factors.”
Read this again, OIO is a valid cause for many ME/CFS cases and this has been reported in many studies. and there are many more. A microbiome shift is well documented in studies for ME/CFS and that by itself may be the cause of ongoing ME/CFS. Explicitly treating nutrient deficiencies is treating symptoms and not causes. Correcting the microbiome will likely resolve most, if not all, nutrient deficiencies. Microbiome dysfunction is well documented with anemia and thyroid dysfunction. A side effect taking the relevant antibiotic is microbiome correction. See Tess Falor’s experience above where remission came with concurrent normalization of the microbiome (corrected by the antibiotics — either directly or indirectly)
Q: Are you not aware of the black box warning of floxing [fluoroquinolone] with some of those antibiotics? Is this protocol target only for those who have lyme associated with the ME/ CFS. Cause most people in my medical community( not all have lyme)who took them have had horrible consequences from being floxed.
Jadin was asked this question (see long video). She has never encountered this issue. It is critical to note HOW she uses it. Never more than 7 days followed by 3 weeks without antibiotics. For safety, she advises not to exercise while using it. Note that the warning also cites INJECTIONS as well as being seen after weeks on fluoroquinolone
More Questions
Where do prebiotics fit into this 4 week cycle?
This was not asked, and my impression is “however you want” provided they do not impact the antibiotics used.
After one 4 week cycle, I take another microbiome test. Then I start another 4 week course (with the next antibiotic from Dr. Jadin’s list in my case? You wrote you would only take metronidazole in my case.) It will take a month until I have the results. Will the results still reflect my current microbiome after the second 4 week course? Or maybe it is still “good enough”!?
“Good enough” and “Sufficient” are the reality of the world we live it. Ideally, you can test and get results back on the same day. That is not the current reality. It is a maze of what-if choices. My evaluation is that round 2 of antibiotics will likely get more progress [it is unlikely that all of the desired shifts will have been done by the first round]. Testing right after the antibiotics will be a bias sample causing some issues to be underreported. It’s a matter of balancing risks and benefits.
My earlier comments were working off her publications from 2000 and before her presentation.
After I have the results, it will take a few days until I get the antibiotic, the probiotic might not get to me on time (especially CustomProbiotics takes like 2 months, so I would have to look for sth. else!), etc. If one item does not get to me on time, should I take the current one a little longer or make a pause for a few days?
Yes IMHO, look for any local products that have only items in the top 50% of the suggestions is a viable alternative. The exception is if you know that you react to the fillers, etc.
You gave me four probiotics recommendations in your suggestions. With the Jadin approach, I would only do two of them in total right (one in the first and one in the second 4 week cycle)? After that I would already have the new results.
There is no clear guidance for probiotics. My own preference is doing one at a time, but there is no clear concern about doing more than one. In keeping with the pattern for antibiotics, I deem the same pattern for probiotics (because they produce natural antibiotics) is reasonable (just one week per month).
“Patients must avoid sugar intake and some supplements, e.g. magnesium”. Are those general recommendations or only when following the “strictly Dr. Jadin protocol”?
Those are Dr. Jadin’s recommendations from clinical observations. Microbiome prescription reports on specific types of sugars and sweeteners — some to be avoided and some to take. Jadin mentioned explicitly that sugar-craving are a warning sign [i.e. the bad bacteria is sending signals to get more sugar in your system].
Does sugar intake only mean added sugar or also fruit, sweet potatoes etc.?
See above, craving for sweets, i.e. added sugar foods and drinks seems to be her critical concerns.
Herbs also after food?
That I have no information on. My common sense suggestion is if taking them away from food have a negative impact, take them with food.
What is your general dosage recommendation for herbs/herb extracts/herb oils?
I avoid giving explicit recommendation (that is a question for someone with clinical experience). What I have done is found dosages used in clinical studies (and if they were effective). These are dosages that someone with clinical experience found safe. I would advocate starting low and working up. The list is here, ??️ Dosages for Supplements
Can this approach also heal my IBS and food intolerances? Or are there additional things to do for that?
The model that I am using says it is very likely to help significantly with both. I avoid the “heal” and “cure” words. Again this is a model, and not clinical experience.
Regarding that I quickly develop food intolerances, you wrote that taking the herbs every 3 days would be ok. But with the Dr. Jadin protocol I would take the herbs for only one week, so only twice in total!? (These conflicting things make it hard for me to understand what to do, so I am asking this.)
Very food question! See We can suggest what to take, but not how to take! My standing advice is to do just what you are comfortable with, what you can tolerate without concerns. I am not clinical (people dealing). Try your suggestion of twice in a week. Sorry that I cannot provide more advice — but I am trying hard to keep to my expertise only.
Last time I did all the antibiotics in a row, then all herbs, then all prebiotics, then probiotics, each item for 2 weeks. This wouldn’t be a current recommendation of yours anymore right? (Or maybe it was not right in the first place..)
My recommendation is simple, for clinical guidance I feel Jadin’s approach is the best when it comes to antibiotics. That has been her main focus. I take her advice/pattern with antibiotics to other things with antibiotics characteristics: probiotics and some herbs. For other things, we are likely wandering the dark (i.e. in the desert lacking studies for guidance).
I try to avoid giving explicit recommendations (not qualified, lack of clinical experience). When there is significant brain fog with a person, I may cross a line that I prefer not to cross, but cross out of compassion. My recommendation is to base your approach on Jadin’s experience and adapt from there. There are a hundred questions that could be asked… 90% of them will likely be answered with “We just do not know for sure” because there are no studies published.
In the “Dr. Jadins current protocol…” article, the recommendation is that probiotics should be taken at noon only. In the “We can suggest what to take, but not how to take it” article, you talk about probiotics at bedtime. What to do?
Jadin’s advice was for probiotics taken when taking antibiotics, that is midway between antibiotics. If antibiotics are not being taken, then shift the probiotics to when your response to them is best.
For the three Possible Paths forward described in the end of the article, is it possible to say which one is the “best/worst” if all antibiotics would be available?
No. Wanting the best is a common concern; we do not have hard data to answer that. The priority on microbiome prescription is based on the number of studies and the number of bacteria influence in the desired manner.
Or maybe a little less. So the thing is, I am not sure whether I will always get all the antibiotics I want from my source. The approach without the antibiotics (which is probably the one of most MicrobiomePrescription users) should still follow the 4 week cycle from the other article, but does a microbiome test less often, only every 6-8 weeks!? What if I sometimes I get the antibiotic and sometimes have to do without?
Key words are “What you are comfortable with and your medical professional is comfortable with”. The goal is to shift the microbiome, every item is a push.
A reader sent me this note which caused me to do some reflection and an experiment.
Maybe you can help me here. I have two samples from February 2023 (where my function was 90% for the first time in years – I did not use antibiotics to achieve this event it just seemed to gradually happen over several weeks since starting valtrex (MicrobiomePrescription : valacyclovir hydrochloride is an antiviral)).
But then I crashed in March after taking, neem, tulsi and Lauricidin which wiped out my microbiome (at least the one I had before!). Then on May 23rd sample my microbiome looked almost the same as February but I was only experiencing about 75% function. There were some outliers like firmicutes to bac ratio being different and prausnitzii being lower than before – but other than that it looked ok.
Second, what I did was compute a number based on the bacteria alleged to be Anti inflammatory and added it to Health Indicators page based on his observations and some research.
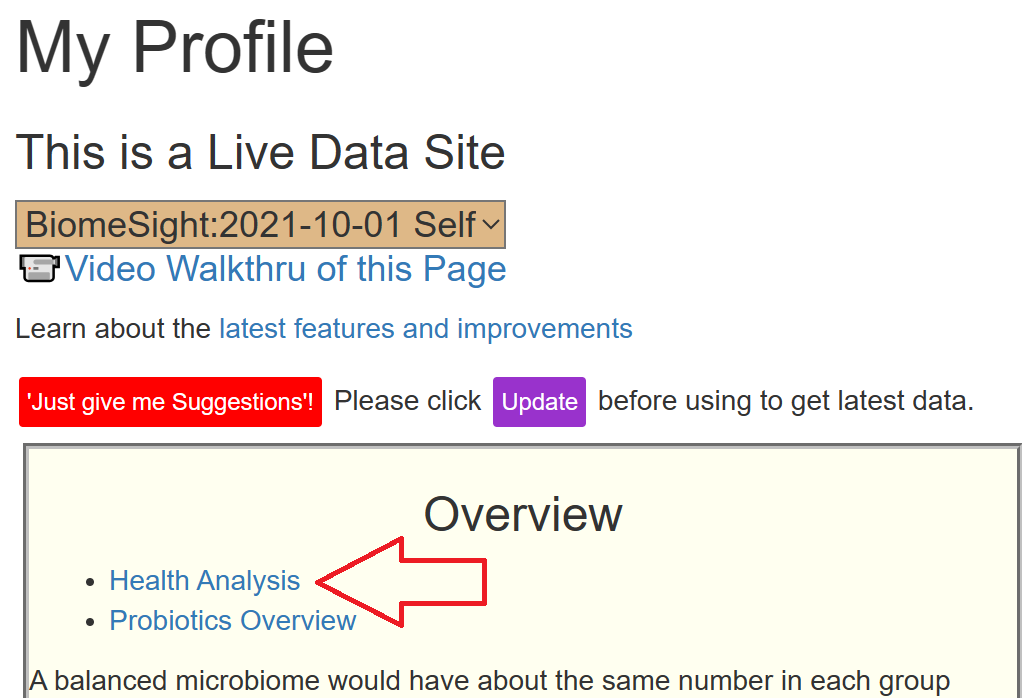
Where is it on the site?
These are computed on a per-processing-lab basis so the percentile will be appropriate.
This has limited value on a single sample (apart from screaming problems).
For this person we see (Biomesight):
2022-8-17: Score: 11.9 2.5 %ile
2023-2-24: Score: 13.51 93.2 %ile
2023-5-23: Score: 13.15 68.4 %ile
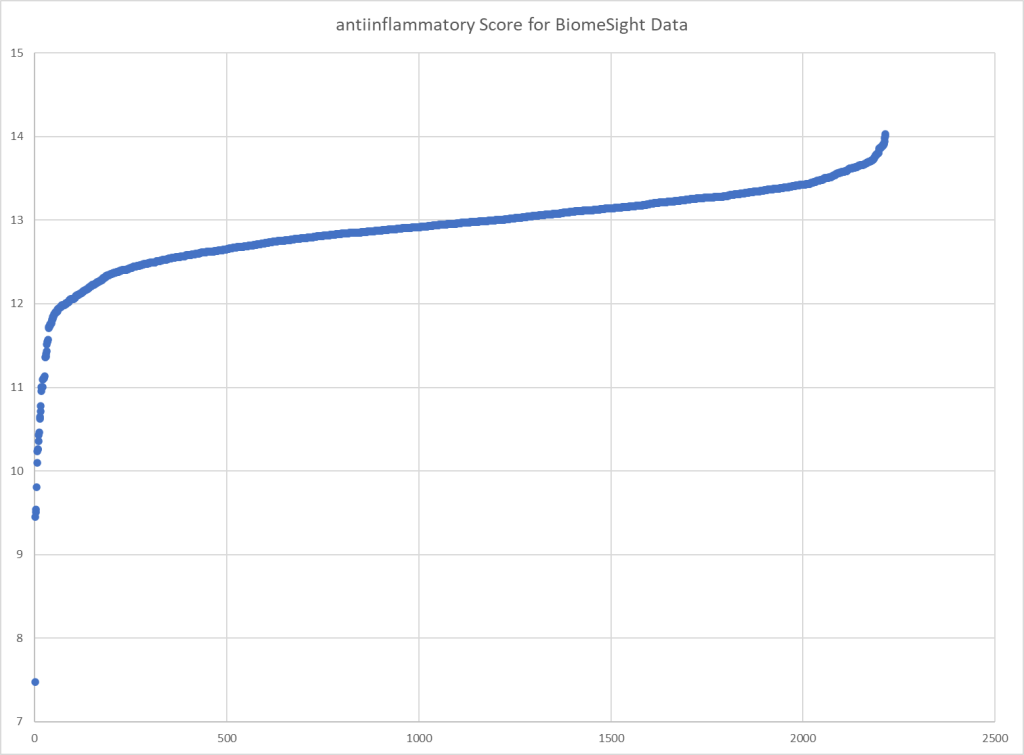
And this follows his subjective experience. Plotting the scores over all of the Biomesight samples, we get our typical score pattern.
User feedback after reviewing “I’ll look into these percentiles I’ve never thought they were useful before! Think I stand corrected.” There is no magic measure that does everything, there are many measures. Some useful for one person and just noise for someone else.
This is different than the body’s Circadian Rhythms. My experience is that it depends on the probiotic — some probiotics taken at bed time will drop me into deep sleep within 10 minutes; other probiotics taken at the same time will keep me wide wake until 3am in the morning — bummer. Why, the probiotic produces enzymes which interacts with the body and the mind. The enzymes vary between probiotics.
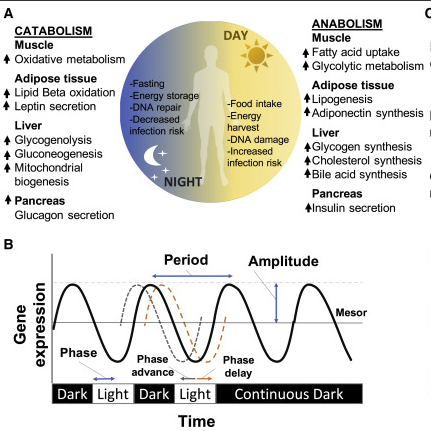
This posts reviews some of the literature and attempts to improve mine, and hopefully yours, understanding of the Circadian Rhythm of bacteria with it’s impact on when certain supplements and probiotics should be taken during the day.
There exists a bidirectional circadian interaction between the host and its gut microbiota, and potential circadian orchestration of both host and gut microbiota in response to invading pathogens. In this review, we summarize what is known about these intestinal microbial oscillations and the relationships between host circadian clocks and various infectious agents (bacteria, fungi, parasites, and viruses), and discuss how host circadian clocks prime the immune system to fight pathogen infections as well as the direct effects of circadian clocks on viral activity
This may account for items like night-sweats, for example, my sleeping body temperature is much higher than my usual daytime temperature.
The Literature
“Conditions of dysbiosis have been linked to circadian rhythm disruption, metabolic alterations, and release of neurotoxic products, all contributing to neurodegeneration.” [2023]
“the gut microbiota can influence the host circadian rhythm by a variety of mechanisms including through interacting with the host immune system. The intricate and complex relationship between the microbiota and their host makes it challenging to disentangle host behaviors from bacterial circadian rhythms and clock mechanisms that might govern the daily oscillations observed in these microbial populations.” [2023]
“Misalignment of the clock can cause obesity, which is accompanied by reduced levels of the clock-controlled, rhythmic metabolite NAD+. Increasing NAD+ is becoming a therapy for metabolic dysfunction; however, the impact of daily NAD+ fluctuations remains unknown.” [2023]
Unconjugated bile acids regulate the amplitude and periodicity of circadian gene expression in the ileum, colon, and liver
High-fat diet
Impaired central and hepatic circadian clock gene expression Dampened circadian oscillations of gut microbiota Altered microbial diversity
Time-restricted feeding
Increased gut microbial diversity Reduced total cholesterol and triglyceride levels
Altered light-dark cycle and mutation of the Clock gene [Bmal1]
Microbiota dysbiosis: increase in proinflammatory bacteria and decrease in anti-inflammatory bacteria Causes dysbiosis
Germ-free mice receiving stool from jet-lagged humans
Enhanced weight gain -Higher blood glucose levels after oral glucose challenge
Some Basic Visuals
The following illustrate the difference between day time and night time. “The endogenous clock anticipates the daily fluctuation in the risk of infection inducing a stronger immune response at the beginning of the active phase of the light/dark cycle“. One common immune response is histamine / mast cells. This is seen in this study The Circadian Clock Drives Mast Cell Functions in Allergic Reactions [2018] which states: Allergic conditions such as asthma or allergic rhinitis have historically shown circadian bias as the severity of symptoms is exacerbated between midnight and morning time and exhibits prominent 24-h variation.
Needless to day (I hope needless), microbiome samples should be taken at the same time of day and preferable on the same day of the week (since shifts between a work day and a day of rest could be significant).
The earliest use of antibiotics for treating ME/CFS that I am aware of, dates from the late 1990’s with articles in Journal of Chronic Fatigue Syndrome (and conference reports prior)
My remission from ME/CFS was done by combining C.L. Jadin protocol with Dave Berg anticoagulant protocol.
Overview of results
First, let us show the numbers and then talk about them. It is clear that there are significant changes. There are a lot of dimensions to consider.
Criteria
2-Mar
9-Mar
21-Mar
3-Apr
16-Jun
Shannon Diversity Index (Percentile)
85.2
79.0
99.8
72.4
16.0
Simpson Diversity Index (Percentile)
72.6
63.4
64.4
77.0
91.4
Chao1 Index (Percentile)
65.7
31.2
77.2
62.9
7.9
Lab Read Quality
8.9
8.7
6
4.5
4.4
Bacteria Reported By Lab
654
533
725
585
389
Bacteria Over 99%ile
2
4
30
11
24
Bacteria Over 95%ile
13
10
70
33
38
Bacteria Over 90%ile
25
23
103
63
55
Bacteria Under 10%ile
287
213
123
113
140
Bacteria Under 5%ile
253
173
66
48
96
Bacteria Under 1%ile
219
135
17
8
46
Lab: BiomeSight
Rarely Seen 1%
13
1
38
5
6
Rarely Seen 5%
28
9
107
17
29
Pathogens
36
31
50
40
36
Outside Range from JasonH
6
6
9
9
8
Outside Range from Medivere
15
15
22
22
22
Outside Range from Metagenomics
7
7
9
9
9
Outside Range from MyBioma
5
5
6
6
6
Outside Range from Nirvana/CosmosId
26
26
18
18
15
Outside Range from XenoGene
28
28
46
46
42
Outside Lab Range (+/- 1.96SD)
6
8
56
17
27
Outside Box-Plot-Whiskers
44
36
124
70
67
Outside Kaltoft-Møldrup
233
169
207
137
170
Condition Est. Over 99%ile
0
0
13
10
48
Condition Est. Over 95%ile
1
0
24
35
75
Condition Est. Over 90%ile
2
2
34
55
84
Enzymes Over 99%ile
0
0
347
606
957
Enzymes Over 95%ile
7
0
635
970
1145
Enzymes Over 90%ile
24
28
746
1159
1228
Enzymes Under 10%ile
506
515
561
237
245
Enzymes Under 5%ile
378
360
422
143
174
Enzymes Under 1%ile
194
166
120
52
94
Compounds Over 99%ile
0
0
225
215
617
Compounds Over 95%ile
2
0
355
410
732
Compounds Over 90%ile
8
11
441
520
778
Compounds Under 10%ile
1243
986
1105
902
822
Compounds Under 5%ile
1156
926
1032
856
796
Compounds Under 1%ile
1115
875
936
828
767
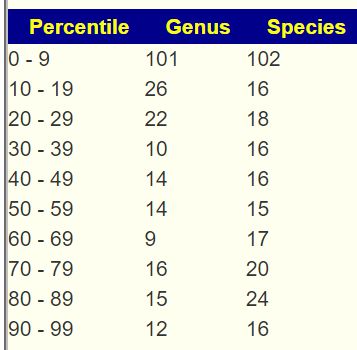
Next are the percentages by percentile which I noticed tend to have over representation with ME/CFS and Long COVID in the 0-9 percentile. We see this pattern at the start, with improvement and then a bounce back to high numbers.
2-Mar
2-Mar
9-Mar
9-Mar
21-Mar
21-Mar
3-Apr
3-Apr
16-Jun
16-Jun
Percentile
Genus
%
Genus
%
Genus
%
Genus
%
Genus
%
0 – 9
65
40%
51
36%
28
15%
29
19%
35
36%
10-19
13
8%
16
11%
36
19%
23
15%
9
9%
20 – 29
11
7%
16
11%
20
11%
23
15%
14
14%
30 – 39
5
3%
9
6%
17
9%
17
11%
4
4%
40 – 49
13
8%
10
7%
14
8%
11
7%
5
5%
50 – 59
12
7%
8
6%
10
5%
8
5%
3
3%
60 – 69
12
7%
9
6%
6
3%
14
9%
1
1%
70 – 79
12
7%
3
2%
10
5%
6
4%
5
5%
80 – 89
10
6%
10
7%
15
8%
9
6%
7
7%
90 – 99
11
7%
8
6%
30
16%
15
10%
15
15%
Total
164
140
186
155
98
2-Mar
2-Mar
9-Mar
9-Mar
21-Mar
21-Mar
3-Apr
3-Apr
16-Jun
16-Jun
Percentile
%
Species
%
Species
%
Species
%
Species
%
Species
0 – 9
41%
94
43%
79
13%
40
17%
36
21%
31
10-19
6%
14
9%
16
15%
44
13%
28
9%
13
20 – 29
8%
18
9%
16
13%
39
12%
27
15%
22
30 – 39
3%
7
5%
10
10%
29
10%
22
8%
11
40 – 49
7%
17
4%
7
7%
20
8%
17
6%
9
50 – 59
9%
21
5%
9
7%
22
6%
12
5%
7
60 – 69
6%
14
8%
14
3%
10
6%
14
6%
9
70 – 79
8%
18
4%
7
6%
19
7%
15
6%
9
80 – 89
6%
13
8%
15
8%
23
8%
17
10%
14
90 – 99
5%
12
6%
11
19%
57
13%
29
14%
21
Total
228
184
303
217
146
The Events Around the above Samples
2023-03-02 (baseline)
2023-03-09 (during a stomach bug)
2023-03-21 (during a “Level 1” remission while taking Amoxiclav. Level 1 = all symptoms gone. Felt great. Had started Amoxiclav on the morning of 3/20, this sample was taken after 3 doses around 3pm)
2023-04-03 (4 days after stopping Amoxiclav, was on Doxycycline)
2023-06-16 (During 2nd round of Amoxiclav when I felt really bad)
The microbiome results definitely reflected the Level 1 remission on 3-21. The low percentile genus and species percentage almost made it to the target level of 10% from the prior 40%! The Shannon Diversity Index was awesome (the higher the better!).
I have often described correcting the microbiome as being similar to sailing a sailboat along a coast line. Depending on wind and tide, there may be a lot of course changes required. I am curious on the ranking of Amoxiclav[amoxicillin] and Doxycycline with these samples. The numbers below suggests that going on to Doxycycline may have been a poor choice. On the 2nd round of Amoxiclav, it was at just 35% of the highest value recommendation versus 70% on the 1st round.
Note that rifaximin and rifampicin are in the same family and used by some ME/CFS specialists. Imipenem shows up often with ME/CFS samples — but since it is intravenous, not the easiest to get on an ongoing basis.
Take Away and Reflections
This project main purpose was to show that remission can be triggered by antibiotics to another generation of people suffering from ME/CFS. The remission on 21-Mar demonstrates this to be correct both subjectively and objectively (Microbiome data — specifically Shannon Diversity Index and Percentages in different percentiles for Species and Genus). I should emphasis that both of these measures are multi-bacteria measures and do not support the common myth that ME/CFS is caused by a single bacteria.
The critical issue is maintaining remission. How do keep the microbiome where it should be. I often use analogies of cities because we are talking about a city of bacteria. To stop riots and looting in the streets you send in the National Guard (antibiotic). The city is back to normal. The causes of the the riots are still there. Typically lack of opportunities, neglect, etc. in these same ghettos. You must address these other issues. A repeat of sending in the National Guard may have the same effect as the first time OR very different effects – the same can be said for using the same antibiotics.
With bacteria we have two “radical organizations in the ghetto” — The Antibiotic resistant and the Resistors. For example, the bacteria that survive learnt how to avoid the National Guard and proceed to share that skill to other bacteria. Instead of a wall of shields pushing the rioters back, Molotov cocktails rain down on the troops from above.
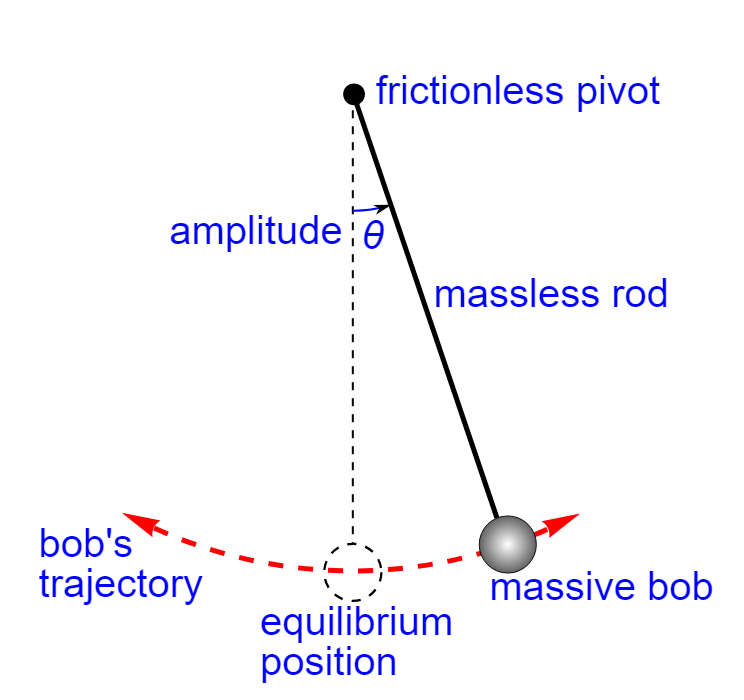
Another analogy is that the gut is a pendulum. The antibiotics, probiotics and other items pushes the gut towards the equilibrium position! There is great joy! The gut is centered… At this point, many people go down the wrong reasoning path — “Keep doing more of the same to stay in remission!“. Remission is lost and the momentum pushes the guts out to the other side!!! You pushed out one devil and seven more devils return! (Math 12:43-45)
The key is to dampen down the swing so there is less and less swing. My personal opinion is that Cecile Jadin’s protocol using antibiotics for only 7 days each month is a very effective way of dampening the pendulum gained from decades of experience.
My approach with Microbiome Prescription is to try to address the whole city. Before taking action, we get intelligence on the nature of the city and decide on the appropriate action for a period of time (typically 4-10 weeks). We then update our intelligence (i.e. microbiome test) and pick the next course of action. Actions may include “food kitchens”, “safe injection sites”, “training programs”, “home repairs”, “on the beat policing”, etc.
There are many people who will state that antibiotics gave me ME/CFS. I do not disagree. Antibiotics can also trigger remission — the problem is WHICH antibiotics. Since every person’s microbiome is unique, there can be no universal “best antibiotic” for ME/CFS. Antibiotics must be selected based on the individuals microbiome (which is the path that Microbiome Prescription took) for the best odds of making the right choice.
My Suggestions Going Forward
I am working with C.L. Jadin, M.D., on documenting her current protocol from almost 30 years of experience using antibiotics for ME/CFS. It will be out soon. I am hoping to have that available within a month. One key aspect of her protocol has been pulsing antibiotics using two at a time. There are a few studies showing that pulsing is more effective. Pulsing often means 7 days on and 21 days off.
Looking at Tess’s last sample, I would propose the following to be considered (items that I picked from the consensus suggestions):
Take a 3 week break from antibiotics (Ideally at the end take another sample)
A common pattern of people is “Just give me a pill to fix me, I want to keep my current life style and I am not prepared to make significant life style and diet changes”. My impression is that making those changes is often required. Inertia is a real maintainer of ME/CFS, especially the pendulum inertia when trying to heal.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide information on rotations etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
In 1994, after two years of a high stress job managing and motivating direct sales groups in my own sales company I quit and I spent 6 months very fatigued, without moving my body very much and staring at the void sitting on my sofa. I could barely lift a glass of water. After the six months I regained strength and I commenced in a new job. Doctor said I had the yuppie flu, gave some vitamins and tests showed I had had epstein-barr viruses.
In 2008 I recall being very fatigued again. And again 6 months secluded at home sleeping 14 hours a day (I have no family in Spain). I could work but I was uneasy and the job was stressful at times,. In 2009 I started to undergo tests in a private clinic, cause the public hospital who was cutting edge at CFS has a a waiting list of years. I wanted to know what I had. Blood samples, screening, mutaflor, some other immune system boosters, etc. Diagnosis 2010: CFS (not Fibromyalgia yet). I started also to attend to conferences and read a lot about my illness (which I don’t do anymore).
In 2016, after years working with fatigue and pain I decided I couldn’t stand it anymore and thought I should care about myself so I went on sick leave for one year. Afterwards I solicited voluntarily leave of absence.
CFS/EM slowly shifted more to Fibromyalgia. I was diagnosed in one of the best public Hospitals in Barcelona (the renowned Hospital Clínic). They gave me advice on doing exercise, not much more.
Now I say I have moderate EM and moderate to severe Fibromyalgia. Depends on the day. I stay at home mainly. IBS, Psoriasis, Costocondritis sometimes, eye problems, dizziness. muscular problems and stiffness, etc. I am going to a Quiropractic for many years. With an electric bike I can do some miles.
I see there are a lot of supplements in Biomesight, It would be highly appreciated if you could give some insight of my Biomesight results and how to get started changing my gut’s microbiome (food, supplements, etc).
Clarity on Suggestions from Biomesight
I do not know how Biomesight derive their suggested supplements. Many microbiome providers use nutritionists who often suggest generic “healthy” supplements. In other cases, they have found a study for a supplement that impacts one bacteria and if you are high or low for that bacteria, suggest that (ignoring what that same supplement will do to other bacteria!). I would love to see a detailed blog from Biomesight on how they determine appropriate supplements to suggest.
Microbiome Prescription uses almost 1.9 million facts(i.e. X substance modify Y bacteria) and then consider all interactions that a supplement has on all bacteria of concern.
Analysis
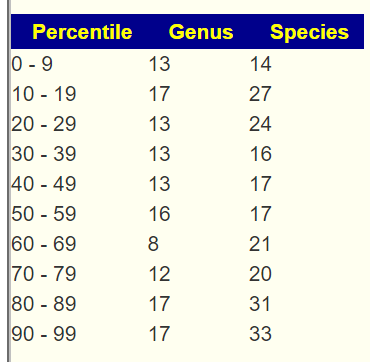
First, we will look for a common fingerprint for ME/CFS and Long COVID: Over representation of bacteria in the 0-9%ile. We have a very strong match shown below. The numbers in each range should be about the same number for a healthy microbiome.
Looking at Dr. Jason Hawrelak Recommendations we find it at 75.3%ile, indicating issues with the following being most concerning:
Faecalibacterium prausnitzii well below his low limit. This bacteria is deemed anti-inflammatory [2008] and thus a contributor
The Potential Medical Conditions Detected using the US Library of Medicine studies show what you reported and a few other items of concern (Asthma, Colorectal Cancer [possible false positive], etc)
Fibromyalgia 96%ile
Chronic Fatigue Syndrome 96%ile
Inflammatory Bowel Disease 94%ile
Gastroesophageal reflux disease (Gerd) including Barrett’s esophagus – 97%ile
Going Forward
First a quick video on the process
I did the “Just give me suggestions” followed by individual sets of suggestions for the four above item resulting in 8 sets of suggestions done with different criteria to select critical bacteria (See video). We then use consensus to identify the items most likely to help. This is a way to improve results in the face of many unknowns.
Probiotics (usually I suggest take 1 probiotic for 2 weeks at sufficient dosage (see this supplement dosages link) and then rotate to the next one on the short list, then repeat.
Antibiotics (if you have a willing MD) — one course then 3 weeks off, then a course of a different one. All of the ones below has been used by specialists for ME/CFS or FM
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
This is a follow up to the January 2022 post, IBS + BioNTech COVID Vaccine -> ME/CFS? For discussion on vaccination changing the microbiome see that post (ANY thing that changes the microbiome has a risk of cascading into ME/CFS — an innocent kiss could result in result in the kissing disease( Infectious mononucleosis) which is usually Epstein-Barr virus and well associated with ME/CFS!).
[Revised: Jul 27th,2023 There was a mix up on the sample for some analysis]
The Request
One biomesight test failed and then I got Covid again, so I had to wait.
There are some improvements since last time: I can listen to music again. I can play cards with my brother a little bit in the night when it’s quiet. I was also able to breathe freely again while doing most things, but in January I had an exhausting doctors appointment and some improvements were lost.
A few specific questions:
Are the “mold bacteria” you mentioned last time still a problem?
Have there been any important/significant new treatments or scientific findings recently that you are aware of that would help me with my issue (CFS from biontech vaccination)?
Things I am taking continuously right now: Magnesium malate, Coenzyme Q10, Acetyl-L-carnitine, Vit. D+K2, Piracetam.
Analysis
“In one study researchers were able to classify 83% of the ME/CFS patients correctly based on their dysbiosis in gut and increased inflammatory markers in blood as a consequence of microbial translocation”
We have three samples, the first one was at the start (and used in the above post). I mentioned in the earlier post that he had not had the symptoms long enough to be deemed ME/CFS. The table below seems to show that the typical ME/CFS and Long COVID pattern is not an immediate result but is cascaded into over time. The pattern of over representation of the percentage in the 0-9 percentile showed up in subsequent samples. We see agreement with his subjective opinion of improvement and then loss of progress in the numbers below.
Nov 2021
Nov 2021
May 2022
May 2022
Jun 2023
Jun 2023
Percentile
Genus
Species
Genus
Species
Genus
Species
0 – 9
11
10
56
81
43
54
10-19
12
16
15
14
13
16
20 – 29
12
13
15
21
17
11
30 – 39
16
19
12
11
8
18
40 – 49
9
13
21
17
9
13
50 – 59
19
24
15
26
14
14
60 – 69
13
19
15
17
17
19
70 – 79
23
20
12
21
11
11
80 – 89
14
18
14
16
12
12
90 – 99
12
12
9
12
5
14
Shannon Diversity Index
79%ile
83%ile
42%ile
Jason Hawrelak
96%ile
95%ile
56%ile
COVID %ile
83%ile
71%ile
83%ile
The “mold bacteria” is a reference to Prevotella. This often grows excessively when there is mold or fungi. His latest sample had a low percentile, so unlikely to be an issue.
Going Forward
Doing “Just Give Me Suggestions” executes the following four individual approaches:
On the simplified summary (intended for those with severe cognitive impairment) there is a button that takes you to the full details (the consensus report)
This gives a list of 1800+ different items that were evaluated. I am not a medical professional and do not have clinical experience. My choices from this tend to arbitrary but with the following guidance:
To take items should be at least 50% of the highest value (in this case, 553 /2 =277)
To Avoid items should be below 50% of the lowest value (in this case, -541/2 = – 270)
If the person has ME/CFS or Long COVID, and I know from reading the literature that studies found that it helps people, I will tend to pick those items
In general, I will not suggest prescription items because most patients will be stonewalled by their MDs on doing prescription items off label. If I do (because the patient reported having a cooperative MD), I will tend to keep to items documented to help ME/CFS patients.
I then checked what is he taking against the results:
Because the reader is in the “Land of Mutaflor” (Germany), I checked that explicitly in two ways:
Using KEGG Data — it was the top probiotic (but the value was lower than usual)
Using Consensus Data — it was very slightly positive (0.3).
So it does no apparent harm (except on pocket book), and I would consider trying it after the above bifidobacterium because low E.Coli has been reported in studies (16s does not provide data).
Checking KEGG suggested supplements against the consensus, we have the following in agreement:
Remember we are dealing “fuzzy data on sparse data” and use the consensus approach to improve odds of picking things that will actually do positive changes. By comparing KEGG identification of metabolites that appear to be at low level (and thus starving some bacteria) with the same items that will improve the bacteria balance, we add another layer to consensus building for suggestions. One more layer is taking substances shown to help ME/CFS which are not in our database. He appears to be making use of my CfsRemission site for that purpose. Consensus and layered is the most likely to produce good results.
Antibiotics
This person reports a friendly medical professional. So:
There are many antibiotics commonly used with ME/CFS that are over 270, which would be my personal preference.
I would do the first one only. I have a pending post with a video with Cecile Jadin which may be helpful.
To Avoid
This is usually selecting items that are likely to be taken by some. If it is below -270, it should be consider to reduce of eliminate. We have a long list, my arbitrary selections are:
vitamin d – -263, close enough and with feedback on current levels, likely a stop
Q: “Vit D is negative”: My vitamin D is in fact over 150 nmol/l already should I stop?
A: Yes. If a value is negative it is likely that taking it will be shifting things in the wrong direction.
Q: “Grapefruit daily”: I quickly develop food intolerances. Would every 3 days be reasonable?
A: Start with every 3 days, if issues arise, try the supplements. Remember these are just suggestions to be considered and may need to be filtered by your tolerance and costs. This applies to your next question too “The same problem for the herbs: Would every 3 days be enough? Also can I just add multiple herbs to my food or are these also “One thing at a time, no juggling”?“
Q: This might be a dumb question: Is the suggestion all three bifidobacterium in a row, or just pick one of them and then Mutaflor?
A: There are never dumb questions. The sequence is arbitrary. Proceed as you feel comfortable. Bifidobacteria is likely to have a greater effect.
Q: B Vitamins and Amino acids: Also one thing at a time? I know I’m asking this question again, but I am really unsure because if I do all the suggestions in a row it seems it might take like a year..
A: Do them all at once or in groups. The reason for doing things in rotation are for items that bacteria are likely to adapt to (i.e. bacteria resistance). These items are typically probiotics (which produce natural antibiotics), antibiotics and a herbs/spices with significant antibiotic like effects. These are not such items.
Q: My mom suggested me N-Acetyl-L-Cysteine which helped her a lot, and I want to look that up.
Feel free to inspect that list and create your own set of suggestions. These are suggestions only based on your microbiome and computation. For ME/CFS, I try to highlight items seen to have positive effects in studied. You may wish to search CFSRemission for literature on items you decide to try.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide information on rotations etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
This person gave an extensive history – the microbiome reflects recent events in general so I have skipped most of it because of that.
An analogy may help, bacteria can be viewed as a city, say London or New York. An “event” happens, for example the Irish Potato Famine, or a shortage of labor causing the import of people from the colonies. The culture of the city is challenged. People are displaced and will often push back; fight back. Eventually a new status quo is established — it does not happen overnight, but over years; over decades. Returning to the old ways (London full of Saxons; New York full of tribal Indians) may be dreamt of, but never happens. An infection is a new wave of immigrants into the city. The impact does not always reflect the numbers. A small number of drug traffickers can have a huge impact on a city. This is how I think about the microbiome — a dynamic living city of bacteria that keeps changes over time. Ghettos develop where once stately manors of well-to-do people were.
Recent Back Story
In September of 2022, I had a COVID infection and fever, which caused a significant “crash”. I have been mainly bedridden ever since. Though the severity of symptoms I experience has waxed and waned from then until now, there has not been any significant differences in ability since. My symptoms are varied, and I’ve noted the ones experienced the week I took my sample on Microbiome Prescription. Positively, I have recently experienced a lowering of resting heart rate with regular electrolyte consumption, HR based pacing, NSDR, and diaphragmatic breathing. Starting Low Dose Naltrexone has helped with pain management, and I’ve needed to take less naproxen as a result.
I’ve tried oxaloacetate and pregabalin to no effect, had some significant side effects with duloxetine, and had a severe reaction with no benefits when I tried CBD/THC oil.
An interesting point is that my microbiome seems more similar to those Covid19 “Longhaulers” than to those with ME/CFS. I wonder why that may be, given that I had ME/CFS before my Covid infection?
I view both Long COVID and ME/CFS to be the same condition with one key difference. Long COVID is a recent major disruption of the microbiome. ME/CFS is often an ancient disruption that has evolved into a more stable state. Long COVID is typically an unstable microbiome that has a high rate of change. See this post on ME/CFS outbreak traced to a specific community infection. Some microbiome return to a stable normal state over time (a.k.a. remission). Going back to the cities examples above, Long COVID is akin to the mass migration of African Americans to Chicago after the civil war. ME/CFS is the state of Chicago today.
This person’s back history included:
“Chronically anxious child with perfectionism tendencies” this pattern has been associated with ME/CFS by many. In terms of the microbiome, the stress would have significant impact on the microbiome.
Severe constipation that required hospitalization, again know microbiome shifts. She has taken Polyethylene Glycol regularly. This is known to cause microbiome shifts.
Taking fludrocortisone (fludrocortisone) and duloxetine for several years.
Crohn’s disease, though the biopsies from the digestive tract were inconclusive. Again known microbiome shifts.
What does this mean? There is a massive amount of “microbiome noise” from these medical conditions and significant drugs. This could be classified as a hodge-podge of a microbiome.
Other questions I have regarding my sample:
Based on my sample, is it possible to tell the likelihood I have (or eliminate the possibility I have)…
poor gut motility
MCAS/Histamine issues
Specific intolerances such as gluten or dairy
SIBO
Leaky Gut
Celiac
Basically, can I extrapolate from the data if I may have issues to fix regarding one of the above or if I can say with some certainty that these don’t affect my gut health?
No, it is not really possible to tell the likelihood. The best that you can do is whether you have bacteriaassociated with those conditions. Association main purpose is to augment or suggest additional medical tests. Some examples:
Special Studies:
12 % matchPoor gut motility (your highest was 30% for Long COVID)
Postural orthostatic tachycardia syndrome (0 %ile) 0 of 6
The PubMed one that you are highest in is Colorectal Cancer (with 9 of 38 matches). This some some resemblance to her recent medical history.
Around August 2020, I started experiencing rectal bleeding, abdominal cramping, mouth sores, and rectal prolapse. I had a colonoscopy and endoscopy in Dec. 2020 with general anaesthetic, and it was as if I had been “hit by a truck”. I could barely get out of bed for the next 5 months. I was diagnosed with Crohn’s disease, though the biopsies from my digestive tract were inconclusive…. Some other anomalies found include a potential cyst on my right ovary and a tender and enlarged lymph node near my right armpit. The cyst and fluid sac may just be “the more you look, the more you find”.
I seem to be intolerant to (or not digest very well) dairy products (with or without lactose), processed foods, acidic fruits (such as raspberries, oranges, lemon or pineapple), starchier foods, oils and fats, lentils, onion, garlic, asparagus, almonds, cucumbers, broccoli, tomatoes, chai, rice crackers, etc. With some foods, such as gluten or eggs, it seems to vary as to whether I tolerate it well.
My medications at the time of the sample were:
Low Dose Naltrexone 3mg
Nadolol 40mg
Multivitamin
Vitamin D 2000iu
Vitamin C 500g
Naproxen as needed for menstrual and joint pain
Since then, I’ve added these supplements:
Magnesium Glycinate 90mg TID (total 270mg)
Inulin 1tsp
Align Probiotic 1 capsule
Probiotic 3 1 capsule TID (total 3 capsules)
Tributyrin-x 3 capsules
D-Ribose 5mg
Analysis
Unlike most Long COVID and ME/CFS microbiomes, the percentage in each percentile is well balanced in the percentages in each percentile. This may be due to items like Low Dose Naltrexone and other medication, or her complex medical history. In terms of Shannon Diversity Index, it was high 2.07 / 97.1%ile.
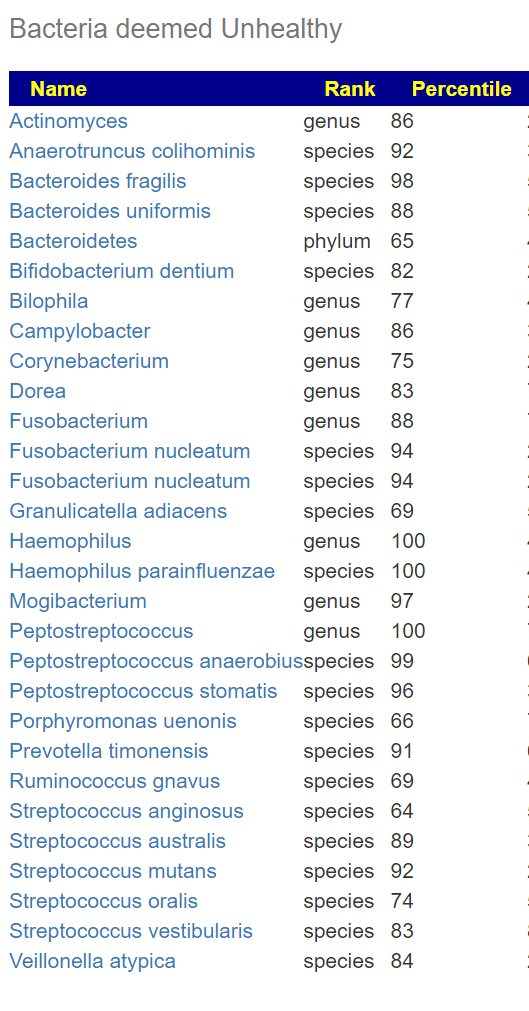
Switching over to Bacteria Deemed Unhealthy, we see a very long list. Some of these are associated with MCAS and allergies. This is a much better signature than the above ones.
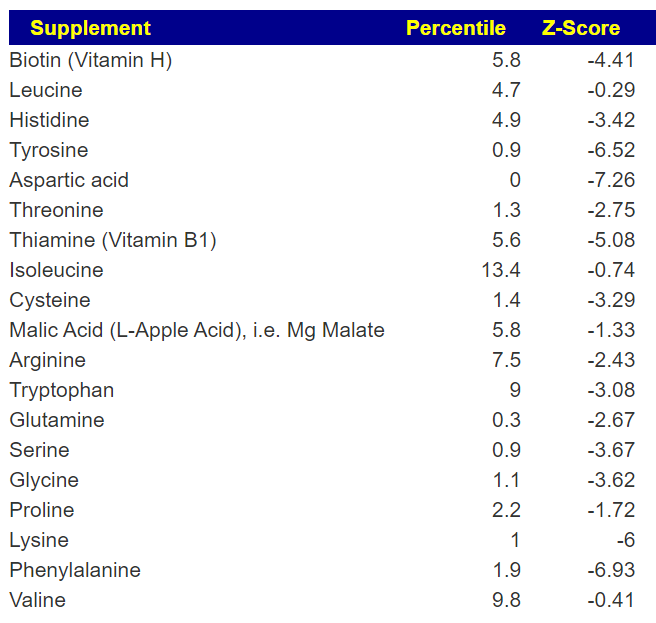
Going over to KEGG AI Computed Supplements, we see a long list, much longer than typical. Items over a Z-Score of 2 are strong candidates for taking as supplements. These are chemicals consumed by bacteria or the body and thus suggests starvation of bacteria (with misbehavior likely).
Looking at AI computer probiotics, nothing stood out strongly. Enterogermina (Bacillus Clausii) is the strongest suggestion.
Analysis of What Is Currently Being Taken
The following times were listed above, I did the “just give me suggestions” and the looked at the full detail via the consensus report. Usually the consensus report highest value is around 400; her report went up to 753 and down to -1064. This is far more variation than I usually see!
Low Dose Naltrexone 3mg – GOOD, 496.4 (max was 753.
Nadolol 40mg – GOOD, 496.4
Multivitamin
Vitamin D 2000iu – so so, -15
Vitamin C 500g – positive: 400
Naproxen as needed for menstrual and joint pain — Good 496.4
Magnesium Glycinate 90mg TID (total 270mg) – negative -355
AOR Probiotic 3 – 1 capsule TID (total 3 capsules)
Enterococcus Faecium – so so (-22, -172), to negative
Clostridium Butyricum – negative – 306
Bacillus Subtilis – so so (-19,-48, -315) to negative
Tributyrin-x 3 capsules – so so -12
D-Ribose 5mg – negative -200
Remember: these are fuzzy logic computation based on fragmentary data available from existing studies. In general, readers have reported improvement from the suggestions – but the suggestions are plotting courses in a fog bank… so do not become dogmatic about doing or not doing.
So what is suggested instead?
Well, all of the prescription items above are big thumbs up! 🙂
496 – Acetaminophen, Paracetamol in UK one with each meal for a week and then one a day? Discuss with your MD. The purpose is altering the microbiome, not headache (i.e. off label use)
584 – sucralose – most other sugars are low or negative value
Questions and Answers
Q: It seems that my microbiome is very well balanced, but has many unhealthy bacteria and a much more varied consensus report than usual. With other similar results from others, do you see a common reason or cause for this being the case?
A: I would not call it well balanced. Several measuring sticks show no strong pattern, but given the large number of microbiome affecting things that have happened to you, those events have likely added a lot of noise. The abnormally large number of bacteria deemed unhealthy is the signature thru this noise. This is not a common situation. Most people have just one microbiome affecting thing.
Q: Being in the 0% percentile for POTS seems interesting for me, given that my POTS is still not quite stable. What are the usual reasons for a microbiome not matching the symptoms and diagnosis of a particular condition (especially that I’m only a 12% match for MECFS with/out IBS)?
A: Similar to above, compounding conditions and treatments that alters the microbiome is a multitude of ways. Ideally, we want to see patterns but patterns usually arise from “pure cases”, you are not a pure case, but a highly compounded case.
Q:Given I have the highest association to Colorectal Cancer, how important is this? Is this something I should be looking to screen for or is it of low enough significance to ignore somewhat?
A: In the abundance of caution, I would ask for screening, you have one recognized risk factor with a hint also from your microbiome. Per CDC guidelines (helps persuade MDs) “However, you may need to be tested earlier than 45, or more often than other people, if you have— Inflammatory bowel disease such as Crohn’s disease or ulcerative colitis.” [CDC]
Q.I’m currently taking magnesium mainly as a tool to manage muscle spasms and twitches. Is there a supplement with similar effects that has a better consensus value?
Lactobacillus paracasei is cited [2004] “Lactobacillus paracasei, but not Lactobacillus johnsonii, Bifidobacterium lactis, or Bifidobacterium longum, attenuated muscle hypercontractility.” Unfortunately a negative.
Streptococcus thermophilus and Lactococcus lactis [2022] “Spasm reductions were accompanied by specific gut microbial alterations, including increases in Streptococcus thermophilus and Lactococcus lactis. Mimicking the fecal microbial alterations in a targeted probiotic, we administered these species in a 5:1 ratio. Targeted probiotic administration reduced seizures and improved locomotor activities in control diet-fed animal” – No information, so these two would be my first preference.
From other articles, there appear to be associations of spasm and twitches with mineral imbalances. For example, hypokalemia(low potassium) [2023] – I would suggest explicit testing for mineral balances
If you have a willing MD, I would ask for amoxicillin which is a common antibiotics and has the second highest confidence of having an impact. The top one, Imipenem, is an intravenous β-lactam antibiotic and it’s impact on the microbiome is less certain. Remember, most MDs will only prescribe for acute active infection and a microbiome dysfunction/issues may not be sufficient for them. My next choice would be thyme oil and hesperidin supplements. With the thyme oil — definitely start with a low dosage and expect bacteria to be protesting strongly (often they protest by massive dumping of toxins into the body… they do not go out quietly).
If you try these suggestions and notice changes, I would suggest another test in 8-10 weeks to see what changed and what your next course correction will be.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
Microbiome Prescription uses over a million rules to generate suggestions on improving the microbiome and hopefully reduce or moderate autism behavior. All of the sources of the rules are studies on the US National Library of Medicine. Microbiome Prescription also can provide the complete evidence trail for every suggestion! That is, where — precisely– is all of the information coming from — none of it is private personal opinion or speculation.
Cross validation is the process of taking one set of information to generate forecasts or suggestions and then look at a totally independent source of information to see if the forecasts and suggestions are valid, reasonable, and appear to help individuals with the condition. I have done that for several conditions with very good results. NOTE: Everything is generated by code — code that I prefer to improve or correct. I have no personal stake in the suggestion, nothing to defend.
The process is simple: some items may have been tests in trials for autism, some have not. If it has been tried, we see what the result in and provide a link to the study (open data!! no “trust me, I am an expert” hype)
“Binding studies show that both the B. subtilis and human ASLs bind up to 4 mol of APBADP per mole of enzyme tetramer and that both enzymes exhibit cooperativity: negative for B. subtilis ASL and positive for human ASL.” [2008]
Randomized controlled trial of sulforaphane and metabolite discovery in children with Autism Spectrum Disorder [2021] “Sulforaphane (SF), an isothiocyanate from broccoli, is a multifunctional phytochemical that has several demonstrated benefits on cellular processes relevant to ASD, including cytoprotective, antioxidant and anti-inflammatory responses, mitochondrial and synaptic function, neuroinflammation and neuroprotective mechanisms, as previously reviewed”
One item that is complex/questionable – depends on the child’s DNA
The goal / objective of Microbiome Prescription is to make suggestions that are more likely to help than to hurt. That goal seems to be accompanied. A secondary goal is to suggest items that have not been studied but modelling suggests that it may be of benefit to try. We have 5 such items above.
Remember these are GENERIC Suggestions for GENERIC Autism
The results of an individuals microbiome will be different — there are many variants and subsets for Autism. Each variant will tend towards their own set of variations for the microbiome. Using an individual’s microbiome sample will get suggestions unique for them.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
Recent Comments