There are two approaches to identifying bacteria associated with a group of symptoms:
UNION — you just join the bacteria associated with each symptom into a single list. This is often done when there is not sufficient data. It’s simple to do.
INTERSECTION — this identifies all people with the same combination of symptoms and then identify what is associated. This requires statistical computations to be done each time.
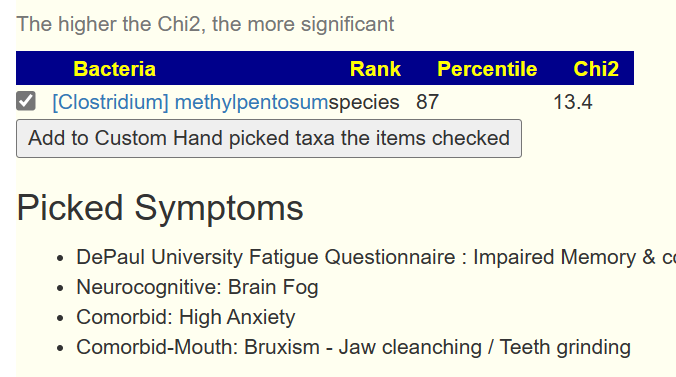
The video below is a quick walkthrough. What is interesting to note is that the number of significant bacteria can increase as more symptoms are added. Why? because you are filtering out noise from the bacteria.
You can also have bacteria appearing that were not in the prior list by adding one more symptom. Example below.
Bottom Line
With a large enough sample and enough characteristics recorded, you can drill down into a lot more data using the appropriate statistical techniques.
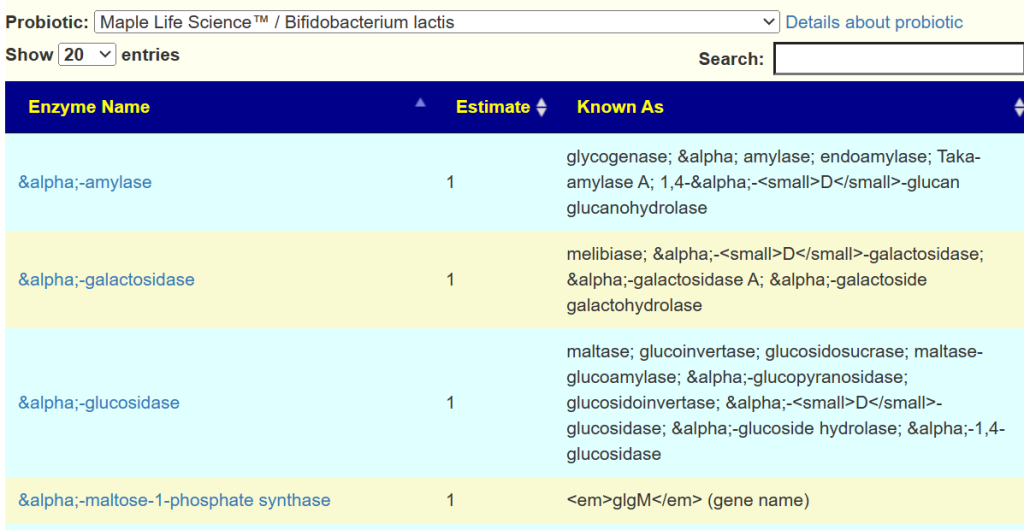
We have the Enzymes produces by a wide variety of strains on the KEGG: Kyoto Encyclopedia of Genes and Genomes. We can aggregate(i.e. average) this data up to the species level and then estimate the enzymes that a probiotic species or retail probiotic mixture may produce.
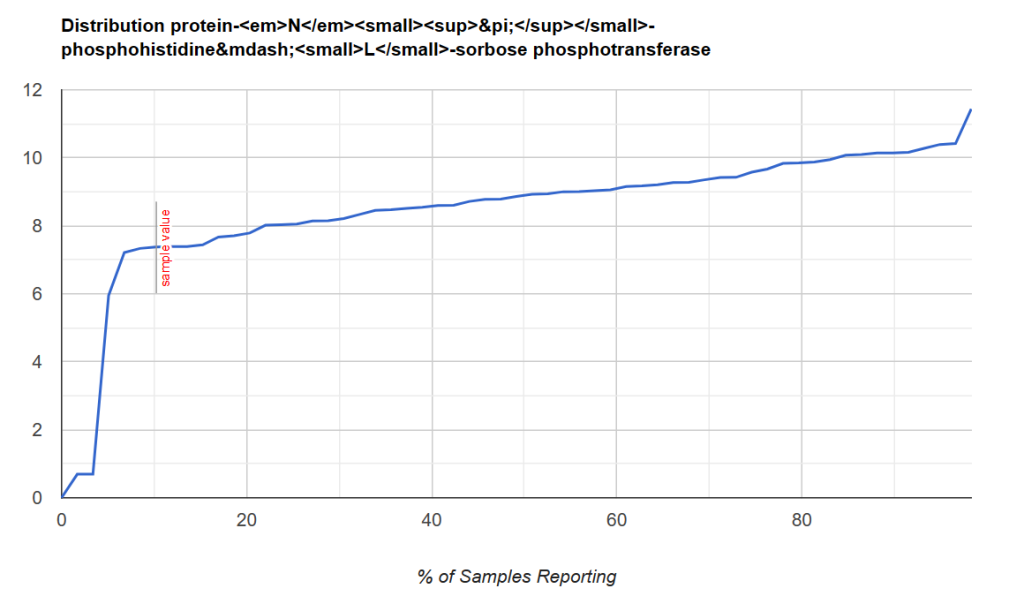
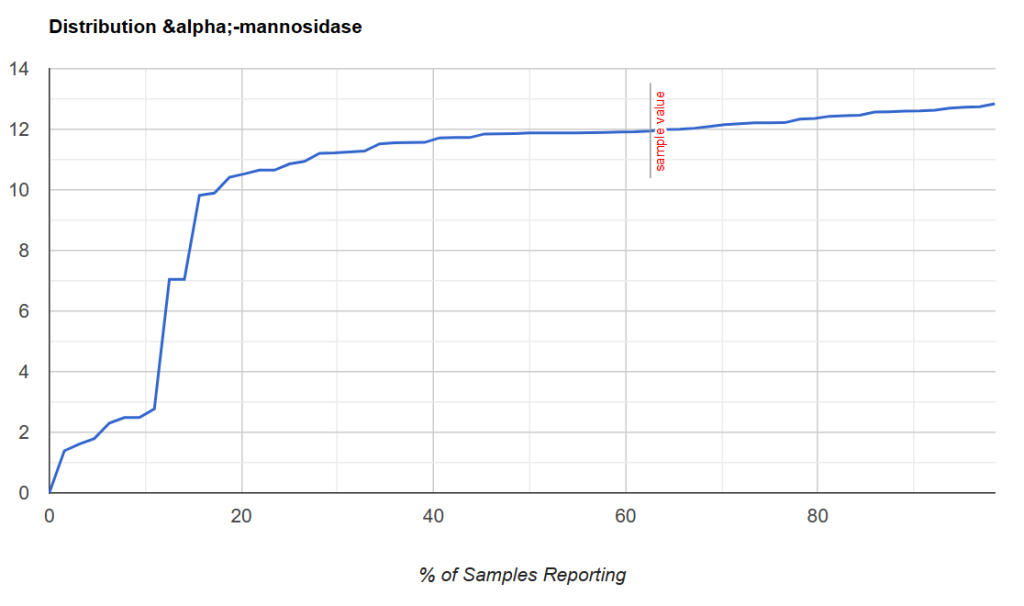
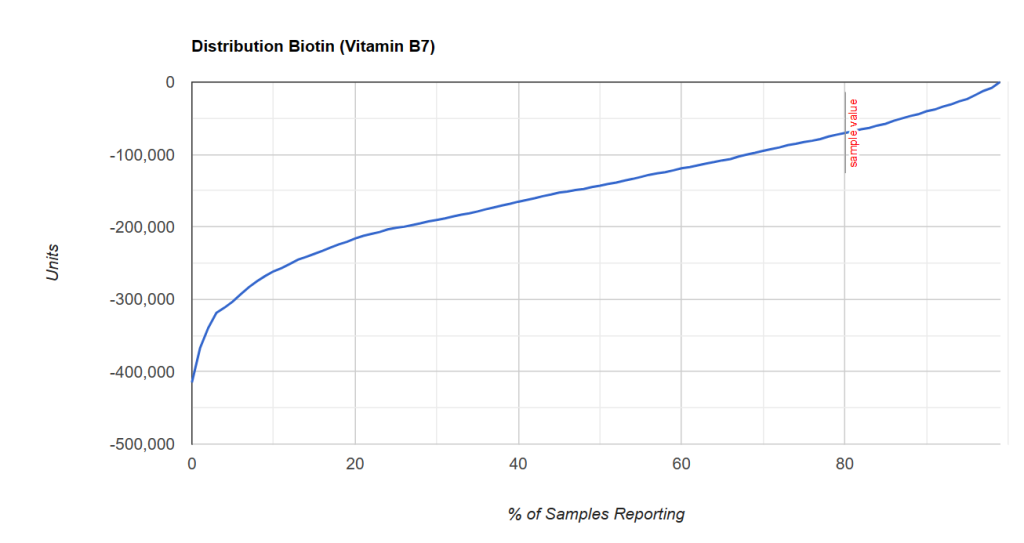
The next step is to identify the enzymes that a person is deficient in. I use the Kaltoft-Moltrup (KM) method to determine the bottom boundaries.
Some visual examples, with this point being around the 8th percentile.
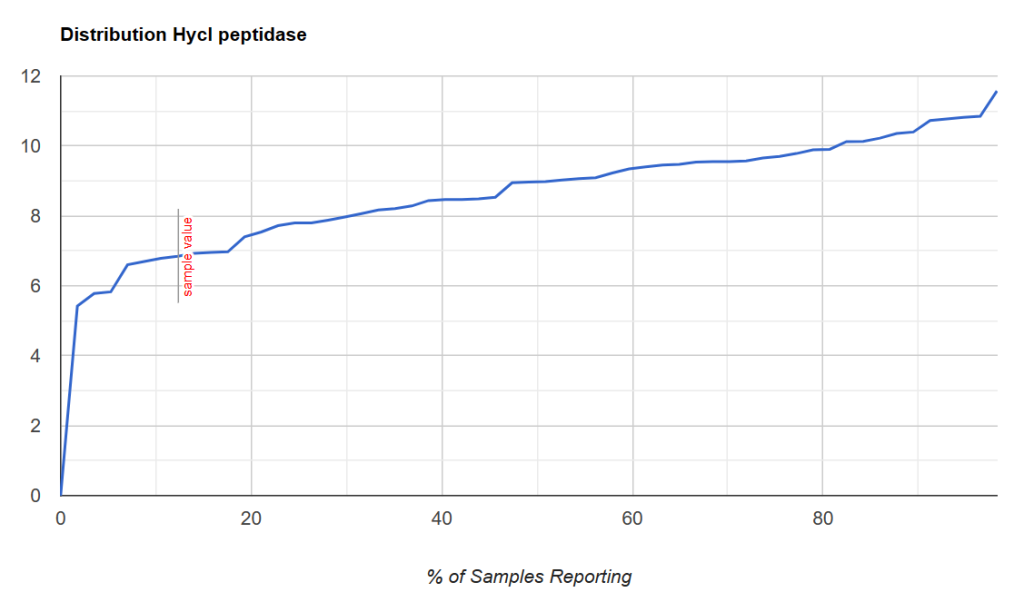
Another example with this point being between 2 and 7%ile
A sample with the cutoff being close to 20%ile.
Thus it is possible to determine:
If a person is likely deficient enough that supplementing enzymes via probiotic may be helpful
We could infer dosages by the distance from the KM cutoff point.
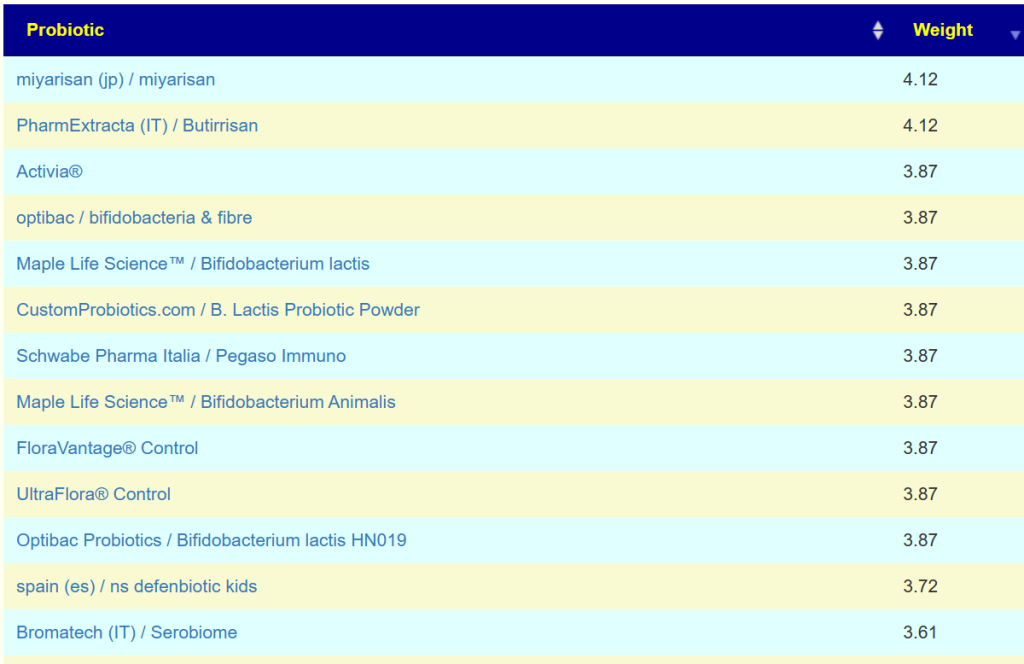
Then we can proceed to apply this to a collection of retail probiotics products
For example, Bifidobacterium Lactis was estimated to produce some 458 different enzymes.
Bottom Line
This approach does not try to “fix bacteria”, rather it tries to make sure that the fuel and oxygen need for the microbiome fire are there. Thus the bacteria issues resolve themselves! A very different way of trying to address microbiome dysfunction.
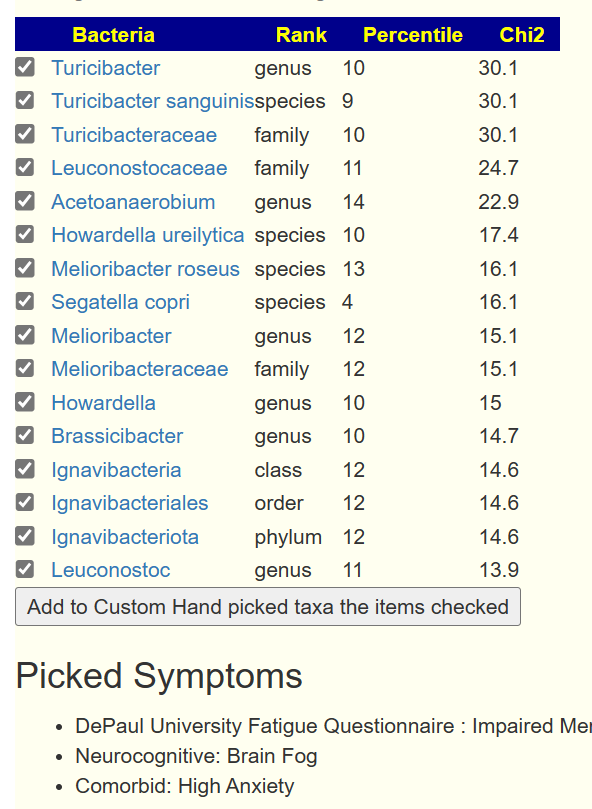
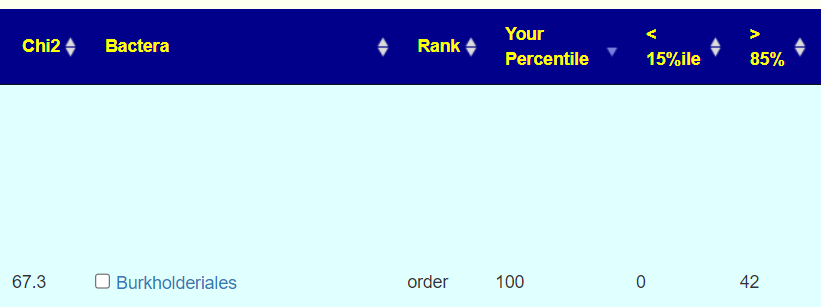
On April 14th, this new/revised feature was released. It determines shifts in these items by looking at the top and bottom 15% of people with these symptoms compared to the annotated sample population. This makes it easy to understand how significance is determined.
The basis is simple:
We count the number of people with symptoms that have a percentile ranking below 15%ile or above 85%ile.
If there is no association, then the numbers should be closed, i.e. 21 for each with the example below.
Rather than get into statistics, we show the common sense counts.
How to get there?
Upon logging with samples you will see this new menu item.
The next screen will matched against annotated symptoms for this sample. If you have no symptoms, this will be shown. You should add your symptoms via the link on this
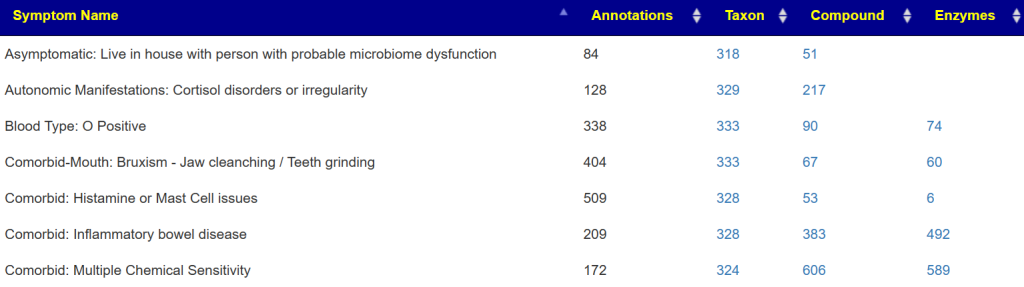
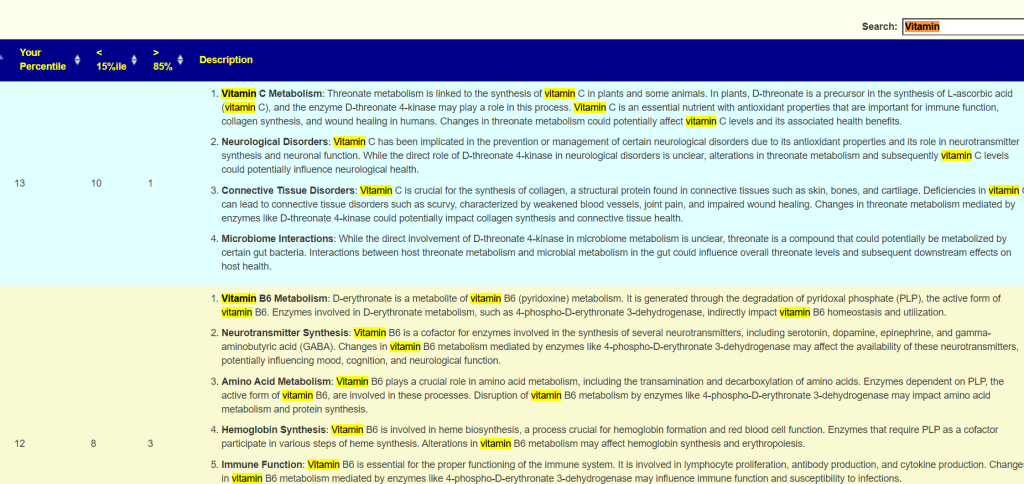
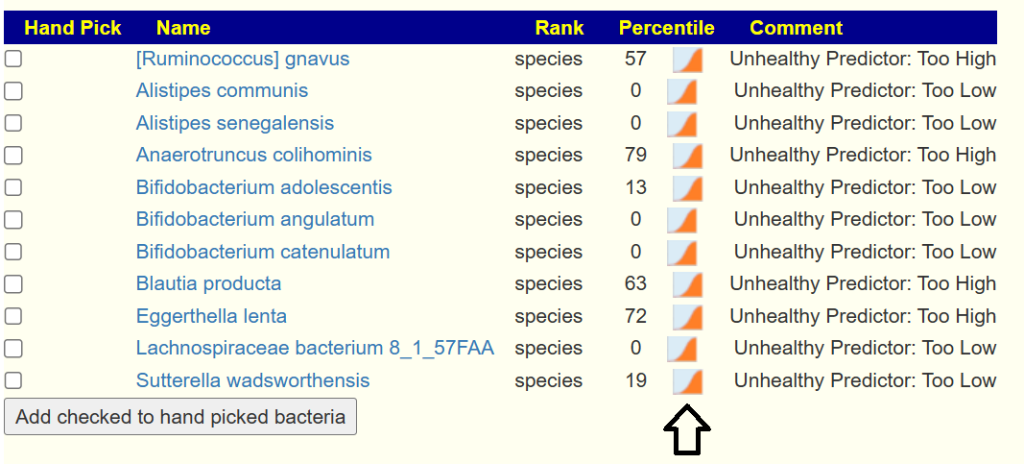
If you have symptoms entered, then you will be shown a summary of what has been associated (according to samples from the lab you used)
The right three columns are hyperlinked. The number of actual matches will be shown when you click the hyperlink. In some cases, many matches in other cases none.
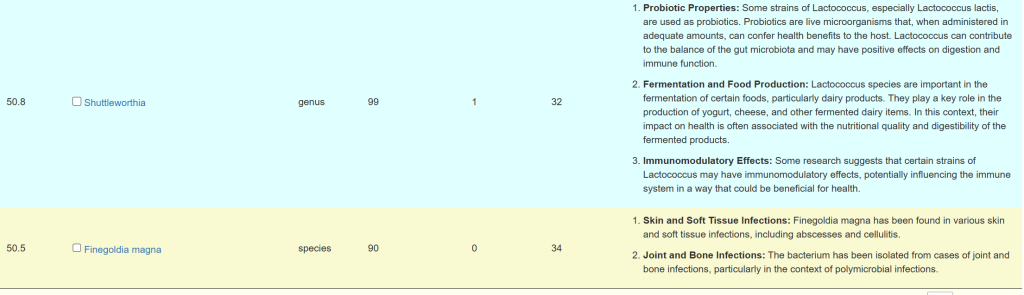
A general description is on the right. For Enzymes, typing “vitamin” in the search box. If the percentile is low, then you should consider supplementing with the vitamins listed. Why? you appears to be deficient in one or more enzymes that produces or uses it (as always, seek an opinion from an expert first)
Video Walk Thru
P.S. all of the bugs identified has been fixed.
Data Availability?
See https://citizenscience.microbiomeprescription.com/ for data. Kegg data on compounds and enzymes needs to be obtained from http://kegg.jp/ (licensing issue).
The notation “3.3e12” is scientific notation, which is a compact way of representing very large numbers. In this notation, the “e” stands for “exponent.” So, “3.3e12” means 3.3×10^12 .
Breaking it down:
3.3 is the coefficient or mantissa.
10 is the base.
12 is the exponent or power of 10.
Therefore, “3.3e12” is equivalent to 3.3 multiplied by 10 raised to the power of 12 , which equals 3.3 followed by 12 zeros:
3.3×1012=3,300,000,000,000.
In other words, “3.3e12” represents 3.3 trillion.
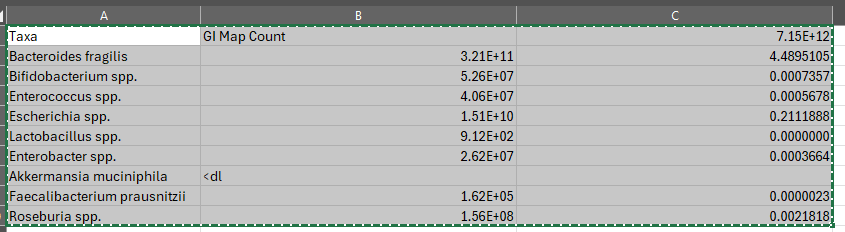
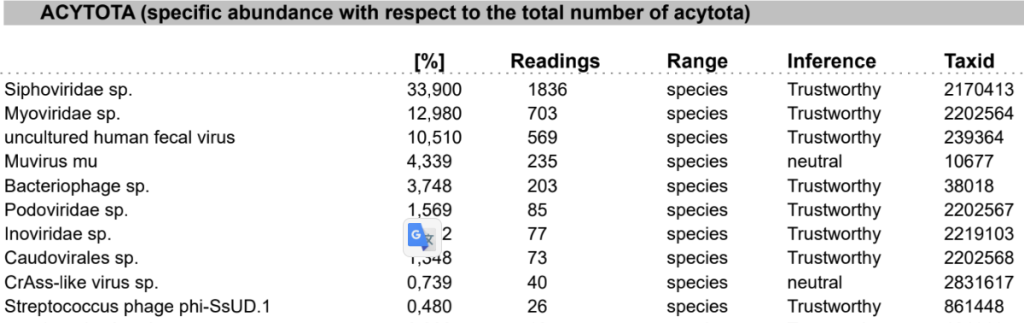
Total Bacteria
Ideally, you would add up all of the phylums; unfortunately GI-MAP only provides two
So the total in this sample is 7.15e12 which is above the reference range max of 3.6e12. So for the purposes of this discussion, we will assume 7.15e12 (with the difference from reference being other phylums).
How does GI-MAP work?
The GI-MAP (Gastrointestinal Microbial Assay Plus) is a diagnostic tool used to assess the composition of bacteria, parasites, and other microorganisms present in the gastrointestinal tract. It utilizes a technique called quantitative polymerase chain reaction (qPCR) to measure the abundance of specific microbial DNA in a stool sample. Here’s how it works:
Stool Sample Collection: A patient provides a stool sample, typically collected at home and sent to a laboratory for analysis.
DNA Extraction: The laboratory extracts microbial DNA from the stool sample. This step involves breaking open the cells of the microorganisms to release their genetic material.
Primer Design: Primers are short DNA sequences designed to bind specifically to the target DNA sequences of interest. For the GI-MAP, these primers target specific regions of the microbial DNA that are unique to certain bacterial species, parasites, or other microorganisms.
qPCR Amplification: The extracted microbial DNA is mixed with the primers and other reagents in a reaction mixture. The qPCR machine then cycles through a series of temperature changes to amplify (copy) the target DNA sequences. Each cycle doubles the amount of DNA present, allowing for the exponential amplification of the target DNA.
Fluorescent Detection: During the qPCR process, fluorescent reporter molecules are incorporated into the DNA as it is amplified. As the amount of amplified DNA increases, so does the fluorescence signal. This allows the qPCR machine to detect and quantify the amount of DNA present in the sample.
Data Analysis: The fluorescence data collected during the qPCR process are analyzed to determine the abundance of specific microbial DNA targets in the stool sample. By comparing the fluorescence signals to standard curves generated from known concentrations of DNA, the laboratory can quantify the relative abundance of different microorganisms present in the sample.
Converting to Percentage
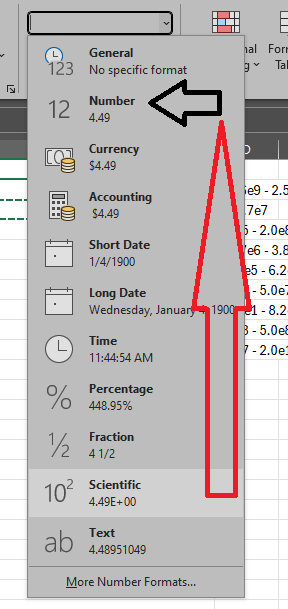
Now, how do we convert. The easy way is to use EXCEL or other spreadsheets. Example of the formula is below.
Then change the display from Scientific to Percentage
Probiotics are a HUGH profit margin. The cost to produce is pretty constant. The difference per BCFU from the cheapest to the most expensive is 650x (i.e. 65,000% difference). You can cut your supplement costs greatly with some careful shopping around and computing the cost per BCFU.
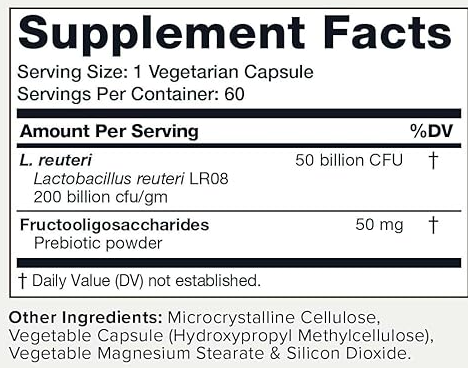
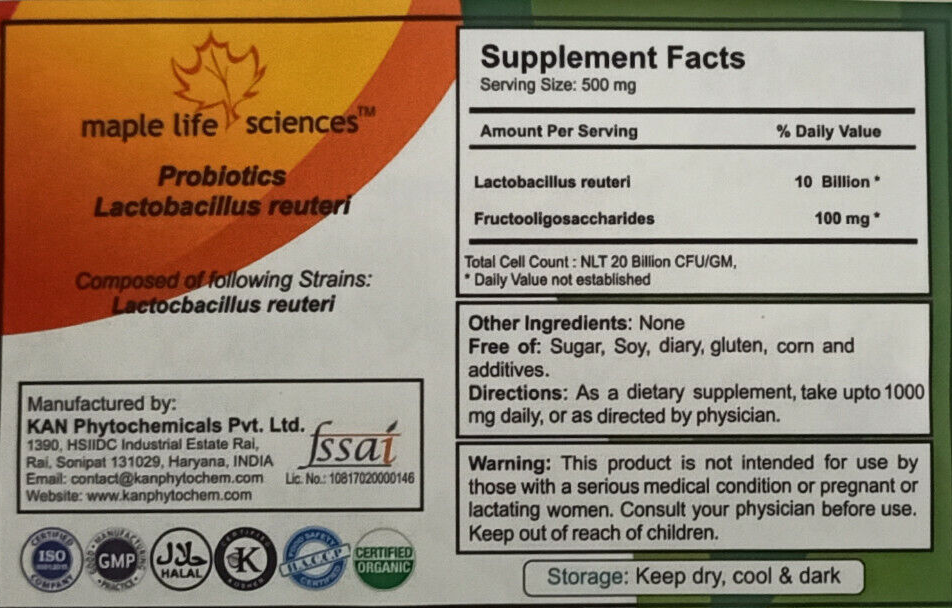
Below are some buying options. I will use Lactobacillus reuteri to illustrate the price issues
50 grams at 20 BCFU/gram = 1000 BFCU for $15.00 = 66 BCFU per dollar They are probiotics with fructooligosaccharides only, no other fillers. Certified Organic
As a reminder, Microbiome Prescription is a “best efforts” site. We do the best that we can with the data that is available.
Request from Reader
Hello Ken,
I would kindly like to ask your opinion on this. I did three BiomeSight tests in three years, then one Xenogene. The Xenogene and last BiomeSight were 10 days apart.
BiomeSight was telling me for three years that my butyrate producers were awesome and my F.Prau was great. Then Xenogene told me the exact opposite. BiomeSight results being so good for so long, I always assumed I have no problem in the microbiome so I kept my diet (15g of fiber at max, lots of meat, veggiest mainly potatoes – no 30-40 different veg/fruit per week). Butyrate producers and F.Prau this high on this diet is a little hard to believe, so I came to the conclusion that BiomeSight is completely off, at least for me.
I remember the Taxonomic nightmare article you wrote and I understand that I cant directly compare two test providers. But when one test tells you that your microbiome is a rockstar and the other tells you its a zombie, its hard to see the usefulness of biomeSight testing. I kindof hope there is some magic that Im forgetting and the biomeSight tests will not prove to be a waste of time and money.
The Xenogene values are percentages of bacteria only (i.e. # F. Prau / # total bacteria), so its “the same thing” as in biomeSight results. Just to be clear that its not # F.Prau / (# bacteria + # protozoa + # archaea + # fungi).
Explanation
Numbers always need to be interpreted against reference ranges.
In other words, both test results were within 1 standard deviation of the mean – that will usually be interpreted as in the normal/reference range. The formula is easy:
(Your Value - Mean) / Standard Deviation
You can do this for each of the bacteria in your report. If the resulting value is between -1.6 and +1.6, you are clearly in the reference ranges.
Lab Provided Ranges
Xenogene provides ranges — this means that over 70% of xenogene files uploaded to MP are below the reference range.
Biomesight reference ranges are below
Every value is within the reference ranges. We have a disagreement.
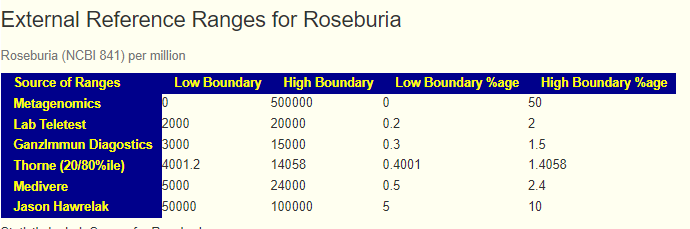
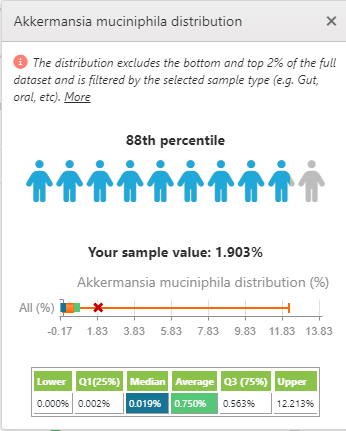
Dr. Jason Hawrelak Recommendations
His ranges are 1-5% for Akkermansia. These are much less than Biomesight and bigger than xenogene. User Feedback: “Dr. Hawrelak’s ranges – how can Dr. Hawrelak have a general range on some bacterium w/o stating which lab he uses for this? Considering all labs report different numbers due to the taxonomy nightmare, I don’t understand how there can be “one range to rule them all”. “
I agree totally, some labs cites him as an authority because they lack the skilled resources to determine their lab specific ranges, Often I have seen ranges from a published studied applied to numbers from a totally different processing pipeline – when challenged they cite “it’s an authority“. Some more readings:
As a FYI: I include his ranges because people have requested it. I provide choices and not judgements.
Microbiome Prescription Ranges
We do not have enough data to independently compute xenogene. Xenogene samples are part of “Other Labs”. The Kaltoft-Møldrup ranges are:
Other Labs: 0 – 7%
Biomesight: 0 -9.6%
Similarly using BoxPlot methodology,
Other Labs: 0 – 3.8%
Biomesight: 0 -1.7%
Note that Zero (0) is in range for many of these.
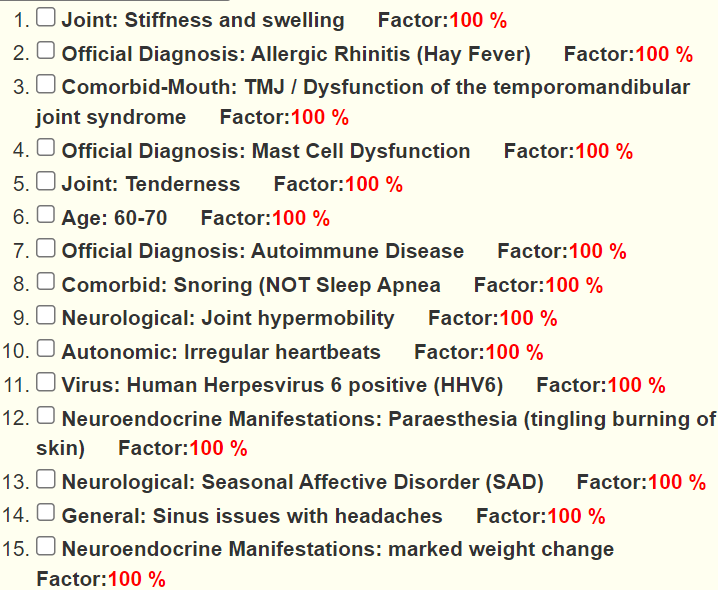
The Symptoms Factor
Identifying bacteria associated with symptoms depends on the number of samples uploaded with annotated symptoms. We do not have sufficient results with Xenogene, we do have sufficient for Biomesight with some 289 associations at present. Note this is pattern matching. “It has the ears of a German Shepard, it has a double coat of a German Shepard, it eyes color matches a German Shepard…etc. ” It may be German Shepard or it may be a Wolf or a Welsh Pembroke Corgi
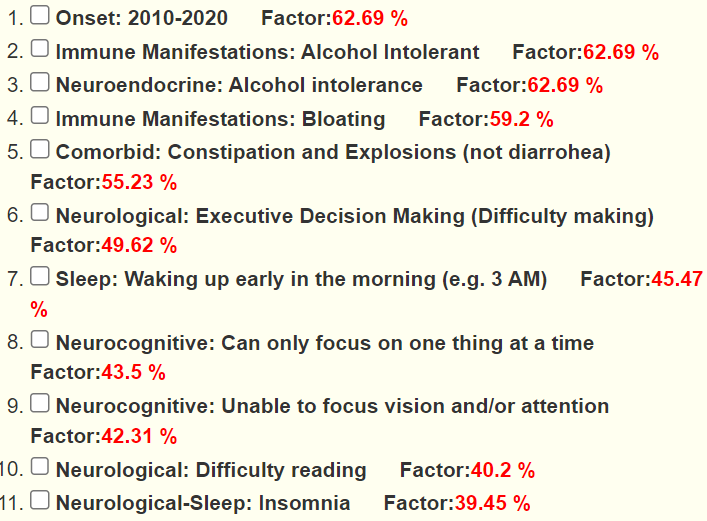
For the latest Biomesight, we see a lot of matches to existing patterns
For Xenogene (which uses “Other Labs”) we have less and weaker matched
If you want to include your symptom in the suggestions report, biomesight is a better choice.
Eubiosis
Eubiosis is not very comparable, because Xenogene is mixed with all of the other odd labs. We have just 19 xenogene, not sufficient to do that much data, We have 61 samples from Thorne – same issue.
Follow up Questions
So my question was how can BiomeSight tell me my butyrate producers are 60% when its highly unlikely, just as with F.Prau being 19%. And the answers that I could imagine getting would be
you having 60% butyrate producers is the result of taxonomic hell, in some cases the positive measurement errors can add up resulting in a hugely overestimated sum – judging the SCFA producers in the biomeSight report is unreliable and should not be taken into consideration at all
OR the only relevant marker for abundance of SCFA producers is stool pH or SCFA measured in stool – use that instead of the SCFA producers % reported by ANY test provider
OR something else if the former two are nonsense
Butyrate evaluation is a good illustration minefield. Some observations:
Labs will usually qualify with “It is important to note that this is not a measure of these metabolites found in the stool sample.“
MP is the only one that appears to include consumers (thus getting a net amount). The choice of genus and species is often based on the depth of research that each lab does. MP is based on the genetics of the bacteria as sequenced and aggregated by KEGG. We do not know if the genetics are activated or not (epigenetics).
What is missing are studies comparing various estimates from bacteria against actual directly determined levels of butyrate and other metabolites…
Second Issue: Percentage of WHAT?
Many labs pull a magical number out of the air, typically if you are over this number you are Satisfactory, below Not Satisfactory. MP gives a percentile ranking against others samples using the same lab. If you are over 30%ile, I would deem it to not need work — but that is a personal judgement call, the numbers are there for you.
Bottom Line
Microbiome reports are full of uncertainty aka fuzzy data. Fuzzy data is not a strong selling point for businesses. Claiming accuracy and correctness is a great marketing ploy. If there are no legal/financial consequences of these dubious claims then they will typically be made by some.
I have seen some labs that started by “just reporting the facts/numbers” and then drift into interpretations because marketing studies found that would increase business.
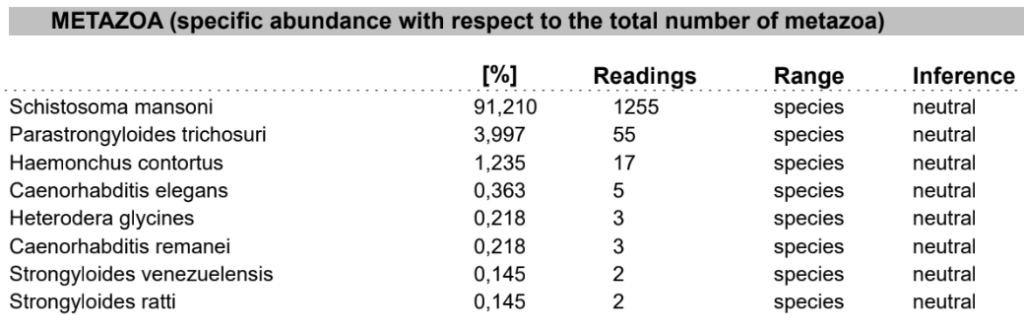
Xenogene (and Thorne) is good because of what else it reports that is not reported on Biomesight which may be part of your health issues. For items that seem very high, you should do some research on them and if any medical conditions are reported/associated with them.
On the other side, we have a lot of samples with annotated symptoms for Biomesight and Ombre. This means that suggestions to modify your microbiome (especially if symptoms are used) are likely better.
My usual advice is simple:
do one of Xenogene or Thorne to check for non bacteria issues (fungi, phages, etx)
use Biomesight or Ombre for regular testing and getting suggestions.
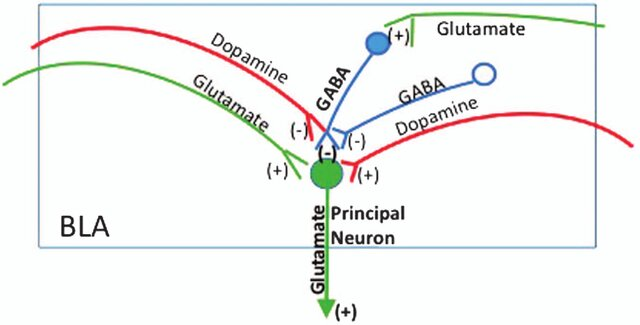
Excessive GABA may be associated with Huntington’s disease, epilepsy, and certain types of encephalopathies. Insufficient GABA may be associated with Anxiety Disorders, Epilepsy, Sleep Disorders, Mood Disorders, Substance Use Disorders, Movement Disorders, Neuropathic Pain and Autism Spectrum Disorders.
Excessive Dopamine may be associated with: Mania or Hypomania, Psychosis, Substance Use Disorders, Hyperactivity and Impulsivity, Tics and Tourette Syndrome, Sleep Disorders, Huntington’s Disease and Excessive Reward Seeking Behavior. Insufficient dopamine may be associated with: Parkinson’s Disease, Depression, Attention-Deficit/Hyperactivity Disorder (ADHD), Drug Addiction and Substance Use Disorders, Restless Legs Syndrome, Schizophrenia and Huntington’s Disease.
Excessive Glutamate may be associated with: Stroke, Traumatic Brain Injury (TBI), Neurodegenerative Diseases, Epilepsy, Migraine, Hypoxic-Ischemic Encephalopathy (HIE), Schizophrenia, Major Depressive Disorder, Bipolar Disorder and Trauma and Neuroinflammation. Insufficient Glutamate may be associated with Cognitive Impairment and Memory Disorders, Depression, Schizophrenia, Pain Disorders, Huntington’s Disease, Epilepsy, Neurodevelopmental Disorders and Sleep Disorders.
Protein-Rich Foods: Glutamate is naturally present in protein-containing foods. Foods high in protein, such as meat, poultry, fish, eggs, dairy products (especially aged cheeses), and legumes, contain significant amounts of glutamate.
Fermented Foods: Fermented foods contain glutamate due to the fermentation process, during which glutamate-producing bacteria break down proteins into amino acids. Examples include soy sauce, miso, tempeh, fermented vegetables (e.g., sauerkraut, kimchi), fermented dairy products (e.g., yogurt), and aged cheeses (e.g., Parmesan, Roquefort).
Seaweed: Certain types of seaweed, such as kombu (kelp), nori, and wakame, are rich sources of glutamate.
Tomatoes: Tomatoes and tomato-based products (e.g., tomato sauce, tomato paste) contain glutamate, contributing to their savory flavor.
Mushrooms: Some varieties of mushrooms, such as shiitake mushrooms, are naturally high in glutamate.
Producers
From Chat-GPT:
Lactobacillus species: Various species within the Lactobacillus genus are known to produce glutamate during fermentation. Examples include Lactobacillus brevis, Lactobacillus plantarum, and Lactobacillus fermentum. These bacteria are commonly used in the fermentation of foods such as sauerkraut, kimchi, pickles, and certain dairy products.
Bacillus subtilis: Bacillus subtilis is a Gram-positive bacterium known for its ability to produce glutamate. It is used in the fermentation of soybeans to produce traditional Japanese seasonings such as miso and soy sauce.
Corynebacterium glutamicum: This bacterium is widely used in industrial fermentation for the large-scale production of glutamate and glutamate-derived compounds. Corynebacterium glutamicum is a key organism in the production of monosodium glutamate (MSG), a food additive used to enhance flavor.
Streptococcus species: Some species of Streptococcus bacteria are capable of producing glutamate during fermentation. Streptococcus thermophilus, for example, is commonly used in the fermentation of yogurt and certain cheeses.
Propionibacterium freudenreichii: This bacterium is involved in the fermentation of Swiss cheese, where it produces various flavor compounds, including glutamate.
A reader asked me to do an update of my 2016 post Psychoactive Probiotics! There has been a lot of recent literature as shown on PubMed. Note that often these are strain specific and not generalized for species cited below. If you cannot find the strains specified in the studies, it may be worthwhile trying different brands of the species (with the most studied species being most probable).
Excessive Dopamine may be associated with: Mania or Hypomania, Psychosis, Substance Use Disorders, Hyperactivity and Impulsivity, Tics and Tourette Syndrome, Sleep Disorders, Huntington’s Disease and Excessive Reward Seeking Behavior. Insufficient dopamine may be associated with: Parkinson’s Disease, Depression, Attention-Deficit/Hyperactivity Disorder (ADHD), Drug Addiction and Substance Use Disorders, Restless Legs Syndrome, Schizophrenia and Huntington’s Disease.
A reader asked me to do an update of my 2016 post Psychoactive Probiotics! There has been a lot of recent literature as shown on PubMed. Note that often these are strain specific and not generalized for species cited below. If you cannot find the strains specified in the studies, it may be worthwhile trying different brands of the species (with the most studied species being most probable).
Excessive GABA may be associated with Huntington’s disease, epilepsy, and certain types of encephalopathies. Insufficient GABA may be associated with Anxiety Disorders, Epilepsy, Sleep Disorders, Mood Disorders, Substance Use Disorders, Movement Disorders, Neuropathic Pain and Autism Spectrum Disorders.
“Metagenomic analyses suggest that the genomes of many gut bacteria encode glutamate decarboxylase (GAD), the enzyme that catalyzes GABA production.” [2023]
“Stress exposure induced a decline in Lactobacillaceae abundance and hence γ-aminobutyric acid (GABA) level in mice.” [2023]
Note: monosodium glutamate (MSG) can increase the production of GABA [2024]
NOTE: The current official name is used below. Most L. species were known as Lactobacillus with older names.
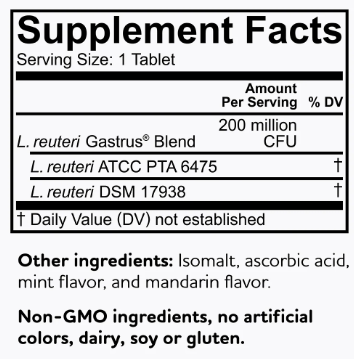
Note: Gamma aminobutyric acid production by commercially available probiotic strains [2023] cites that the best are: Levilactobacillus brevis LB01 [Source], Lactiplantibacillus plantarum 299v [Jarrow Formulas Ideal Bowel Support].
Lactiplantibacillus plantarum 299v is the most available with many suppliers. A dosage of 10-60 BCFU per day is recommended.
“These results suggest that chronic ingestion of Lactobacillus plantarum strain PS128 could ameliorate anxiety- and depression-like behaviors and modulate neurochemicals related to affective disorders.Thus PS128 shows psychotropic properties and has great potential for improving stress-related symptoms.” [2015]
“PS128 is safe and could induce changes in emotional behaviors…These findings suggest that daily intake of the L. plantarum strain PS128 could improve anxiety-like behaviors and may be helpful in ameliorating neuropsychiatric disorders.”[2016]
“We previously have demonstrated that administration of Lactobacillus rhamnosus (JB-1) to healthy male BALB/c mice, promotes consistent changes in GABA-A and -B receptor sub-types in specific brain regions, accompanied by reductions in anxiety and depression-related behaviors.”[2016] [2014] [2014]
“Within minutes of application, JB-1 increased the constitutive single- and multiunit firing rate of the mesenteric nerve bundle, but Lactobacillus salivarius (a negative control) or media alone were ineffective.” [2013]
One study showed improved mood in healthy volunteers following 3-week consumption of a probiotic-containing milk drink that contained Lactobacillus casei Shirota” [2007]
“administration of the probiotic, L. casei Shirota, decreased anxiety in patients with chronic fatigue syndrome.”[2009]








Recent Comments