This is a continuation of Bacteria interacting with Bacteria thread looking at proforma analysis methods and suggesting better processes. My orientation in clinical treatment. When I read a paper such as the one quote below, I roll my eyes. We know Bifidobacterium is less but how much less is needed in an individual sample is unanswered. Similarly which strains or species are shifted is unanswered.
We identified phylum- through genus-wide differences in bacterial abundance including decreased Firmicutes, increased Bacteroidetes, and decreased Bifidobacterium in the microbiome of AD participants.
Gut microbiome alterations in Alzheimer`s disease. Scientific reports (Sci Rep ) Vol: 7 Issue 1 Pages: 13537
Pub: 2017 Oct 19 Epub: 2017 Oct 19
This is the reality for hundreds of papers listed here.
I run a citizen science site where many people(2100+) have uploaded their samples (5200+ – usually 16s) and a significant number(1900+) have annotated their samples with symptoms. Walking down the same Chi2 path as I did with bacteria, we get some potentially interesting insights. I am a statistician by training and work experience.
General Approach
We look at the number of bacteria with low/high bacteria with a specific symptom (say 300 reports) and compare it to others. What others is can be one of the following:
- Those reporting symptoms but not this symptoms (leaving 1600 samples)
- All people without this symptoms (leaving 4900 samples).
My experience is that having significantly more samples results in higher Chi2 values despite the others including some with the symptoms. Conceptually, we may have a lower Chi2 value because of this.
For our example symptoms, Neurological-Audio: Tinnitus (ringing in ear) with 433 samples with this annotation. The table below shows the average percentile ranking.
| Tax Name | Tax rank | Tinnitus Mean | Others Mean |
| unclassified Herbaspirillum | norank | 50.3 | 22.6 |
| Lacrimispora saccharolytica | species | 78.1 | 53.1 |
| unclassified Sutterella | norank | 31.1 | 52.6 |
| Collinsella tanakaei | species | 60.1 | 43.0 |
| Prevotella paludivivens | species | 32.9 | 48.7 |
| Proteus | genus | 61.6 | 46.0 |
| Desulfonatronovibrio | genus | 54.2 | 38.8 |
| Tepidimicrobium xylanilyticum | species | 62.3 | 47.1 |
| Prevotella oralis | species | 37.7 | 52.5 |
| Bifidobacterium gallicum | species | 33.1 | 47.9 |
| Bifidobacterium adolescentis | species | 36.7 | 48.8 |
We are going to use Bifidobacterium gallicum (NCBI 78342) because of the number of samples(1400+) reporting it. What we got is below. From this we can infer odds such as:
- Below 22%ile levels is a double the risk of having Tinnitus
- Below 9%ile levels is four times the risk of having Tinnitus
| Percentile | Expected | Obs | Chi2 |
| 1 | 0.79 | 13 | 190.6 |
| 9 | 7.11 | 29 | 74.1 |
| 10 | 7.9 | 30 | 68.7 |
| 22 | 17.38 | 40 | 37.7 |
| 31 | 24.49 | 45 | 24.9 |
| 36 | 28.44 | 49 | 23.2 |
| 47 | 37.13 | 51 | 9.8 |
| 49 | 38.71 | 52 | 8.9 |
| 50 | 39.5 | 53 | 9.2 |
| 51 | 40.29 | 54 | 9.5 |
| 52 | 41.08 | 55 | 9.8 |
| 53 | 41.87 | 56 | 10.1 |
| 54 | 42.66 | 58 | 12.0 |
| 55 | 43.45 | 60 | 14.0 |
| 56 | 44.24 | 61 | 14.4 |
| 62 | 48.98 | 62 | 9.1 |
| 63 | 49.77 | 63 | 9.5 |
| 64 | 50.56 | 65 | 11.5 |
| 68 | 53.72 | 66 | 8.8 |
| 69 | 54.51 | 66 | 7.8 |
| 71 | 56.09 | 67 | 7.3 |
| 72 | 56.88 | 68 | 7.8 |
| 73 | 57.67 | 69 | 8.2 |
| 75 | 59.25 | 71 | 9.3 |
| 78 | 61.62 | 72 | 7.9 |
| 79 | 62.41 | 74 | 10.2 |
| 86 | 67.94 | 75 | 5.2 |
| 91 | 71.89 | 76 | 2.6 |
| 93 | 73.47 | 77 | 2.4 |
| 96 | 75.84 | 78 | 1.5 |
| 99 | 78.21 | 79 | 0.8 |
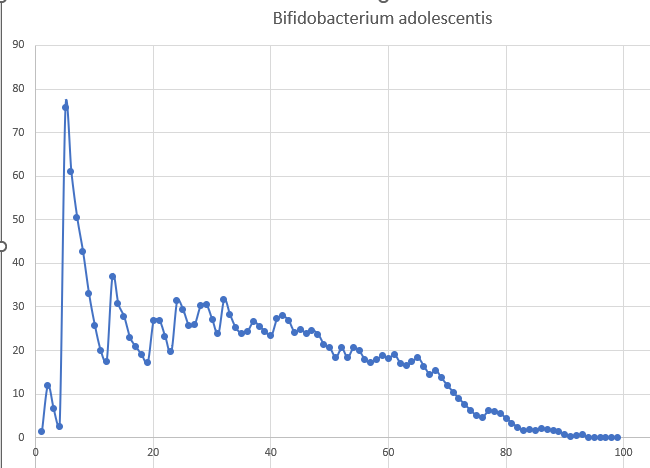
Looking at a bacteria that is available as a probiotics, Bifidobacterium adolescentis (NCBI 1680) and plotting the Chi2 against the percentiles we find that the probability of having Tinnitus has a threshold around 70%ile, or in percentage terms 0.43% of the microbiome. Y axis is Chi2, X axis is the percentile of others.
Each of the above taxa are contributor to the risk of Tinnitus without any being the single cause.
We have 79 of 433 samples annotated with Tinnitus (18.2%) having Bifidobacterium adolescentis. With non Tinnitus we have 2395 out of 4800 samples (49.9%) having Bifidobacterium adolescentis suggesting that not having Bifidobacterium adolescentis is a significant risk factor for developing Tinnitus.
Other Candidate Probiotics
| Tinnitus Mean | Others Mean | Tinnitus Frequency | Other Frequency | |
| Bifidobacterium pseudocatenulatum NCBI 28026 | 53.6 | 45.2 | 8% | 7% |
| Bifidobacterium dentium NCBI 1689 | 55 | 45 | 14% | 20% |
| Bifidobacterium catenulatum NCBI1686 | 24.6 | 43.8 | 12% | 23% |
| Limosilactobacillus fermentum NCBI 1613 | 51.9 | 42.5 | 12% | 10% |
| Bifidobacterium kashiwanohense PV20-2 NCBI 1447716 | 31.4 | 45.1 | 9% | 20% |
| Bifidobacterium catenulatum subsp. kashiwanohense NCBI 630129 | 33 | 45 | 11% | 21% |
| Ligilactobacillus NCBI 2767887 | 37.9 | 49 | 11% | 14% |
Digging Deeper
We have a well studied taxa as a key candidate, Bifidobacterium adolescentis. Let us look at this 2022 article, The Role of Gut Dysbiosis in the Pathophysiology of Tinnitus: A Literature Review (tinnitusjournal.com) which cites “It has been previously described that the presence of tinnitus is related to the decrease in inhibitory neurotransmitters such as GABA and an increase in excitatory neurotransmitters. Besides, the increased GABAergic inhibitory neurons and decreased excitatory responses have been successfully reported to prevent tinnitus, proving the role of neurotransmitter modulation in tinnitus.”
We then find related studies:
- Bifidobacterium adolescentis as a key member of the human gut microbiota in the production of GABA [2020]
- Production of GABA in milk fermented by Bifidobacterium adolescentis strains selected on the bases of their technological and gastrointestinal performance [2023]
- Cell factory for γ-aminobutyric acid (GABA) production using Bifidobacterium adolescentis [2022]
This suggests that an appropriate clinical trail of a Bifidobacterium adolescentis that is both human sourced and a high GABA producer should be done. Ideally with good persistence probability. A further key factor is to determine the pH value for people with tinnitus since studies have shown that the amount of GABA production is deeply influenced by the pH.
We have a lots of other taxa to investigate.
Bottom Line
Using Chi2 and percentiles of samples seem to be different sides of the same coin. The information gleamed from using this approach may often have direct clinical consequences, i.e. for Tinnitus, taking Bifidobacterium adolescentis probiotics and making diet changes to support this bacteria.
The key aspect of this post is not Tinnitus but methodology. From existing data, a lot more items with statistical significance can be extracted.
1 thought on “Symptoms/Diagnosis association to Bacteria”
Comments are closed.