For more information on this project see Health Rising post. Both participants has granted me to do a review with their real names. This is the second of a series of posts on this project, the first one was on The Remission Biome Project: Tess Falor.
Connected with review, you may wish to read Dr. Jadin’s Current Protocol for ME/CFS – Microbiome Prescription Blog, parts are being consider for incorporation into the Remission Biome Projects
The earliest use of antibiotics for treating ME/CFS that I am aware of, dates from the late 1990’s with articles in Journal of Chronic Fatigue Syndrome (and conference reports prior)
- Role of Rickettsiae and Chlamydiae in the Psychopathology of Chronic Fatigue Syndrome (CFS) Patients by Philippe Bottero
- Common Clinical and Biological Windows on CFS and Rickettsial Diseases by C. L. Jadin
- Role of Mycoplasmal Infections in Fatigue Illnesses by G.L. Nicolson
My remission from ME/CFS was done by combining C.L. Jadin protocol with Dave Berg anticoagulant protocol.
A big thanks to BiomeSight.com for donating some testing kits to the project. If interested in using their kits, there is a discount code (“micro”).
Overview of results
First, let us show the numbers and then talk about them. It is clear that there are significant changes. There are a lot of dimensions to consider. Some highlights:
- The number of bacteria with abnormally high representation has gone from 123 down to 29
- The number of bacteria with abnormally low representation has gone from 222, dropping down to as low as 19, before rebounding to 162 (still better than the start)
- Most measure showed great improvement and then some relapse.
| Criteria | 7-Mar | 23-Mar | 15-Apr | 22-Apr | 29-Apr |
| Shannon Diversity Index | 33.8 | 78.0 | 97.1 | 76.5 | 77.1 |
| Simpson Diversity Index | 0.7 | 65.1 | 58.6 | 60.3 | 73.4 |
| Chao1 Index | 91.3 | 61.6 | 72.0 | 89.4 | 14.8 |
| Chi-Square (Lower is better) | 55 | 47 | 46 | 50 | 30 |
| Lab Read Quality | 8.6 | 7.1 | 5.4 | 2.2 | 6.9 |
| Bacteria Reported By Lab | 755 | 638 | 628 | 765 | 461 |
| Bacteria Over 99%ile | 27 | 11 | 13 | 56 | 5 |
| Bacteria Over 95%ile | 72 | 25 | 30 | 105 | 18 |
| Bacteria Over 90%ile | 132 | 46 | 63 | 178 | 29 |
| Bacteria Under 10%ile | 222 | 218 | 62 | 19 | 162 |
| Bacteria Under 5%ile | 191 | 195 | 18 | 12 | 144 |
| Bacteria Under 1%ile | 177 | 179 | 0 | 3 | 112 |
| Lab: BiomeSight | |||||
| Rarely Seen 1% | 8 | 4 | 3 | 66 | 2 |
| Rarely Seen 5% | 22 | 24 | 27 | 128 | 14 |
| Pathogens | 39 | 32 | 33 | 31 | 29 |
| Outside Range from JasonH | 8 | 8 | 8 | 8 | 8 |
| Outside Range from Medivere | 18 | 18 | 16 | 16 | 16 |
| Outside Range from Metagenomics | 9 | 9 | 6 | 6 | 6 |
| Outside Range from MyBioma | 10 | 10 | 6 | 6 | 6 |
| Outside Range from Nirvana/CosmosId | 18 | 18 | 12 | 12 | 12 |
| Outside Range from XenoGene | 52 | 52 | 39 | 39 | 39 |
| Outside Lab Range (+/- 1.96SD) | 43 | 15 | 17 | 36 | 7 |
| Outside Box-Plot-Whiskers | 146 | 51 | 83 | 227 | 43 |
| Outside Kaltoft-Møldrup | 251 | 189 | 105 | 212 | 158 |
| Condition Est. Over 99%ile | 1 | 5 | 0 | 0 | 3 |
| Condition Est. Over 95%ile | 2 | 14 | 0 | 5 | 13 |
| Condition Est. Over 90%ile | 11 | 28 | 2 | 11 | 21 |
| Enzymes Over 99%ile | 7 | 68 | 5 | 19 | 37 |
| Enzymes Over 95%ile | 22 | 281 | 209 | 123 | 250 |
| Enzymes Over 90%ile | 58 | 435 | 361 | 317 | 409 |
| Enzymes Under 10%ile | 219 | 354 | 59 | 48 | 201 |
| Enzymes Under 5%ile | 173 | 265 | 34 | 24 | 144 |
| Enzymes Under 1%ile | 138 | 94 | 13 | 12 | 79 |
| Compounds Over 99%ile | 3 | 44 | 1 | 13 | 16 |
| Compounds Over 95%ile | 15 | 186 | 82 | 68 | 87 |
| Compounds Over 90%ile | 27 | 297 | 154 | 153 | 183 |
| Compounds Under 10%ile | 882 | 889 | 985 | 987 | 875 |
| Compounds Under 5%ile | 862 | 859 | 959 | 963 | 841 |
| Compounds Under 1%ile | 845 | 802 | 935 | 952 | 820 |
As with Tess, the percentages by percentile which I noticed tend to have over representation with ME/CFS and Long COVID in the 0-9 percentile. We see this pattern at the start, with improvement and then a bounce back to high numbers in the last sample
Tamara suggested that I convert the tables below to charts. Both are now available on the site.
Pretty Pictures
Tamara suggested that I convert the tables below to charts. Both are now available on the site.
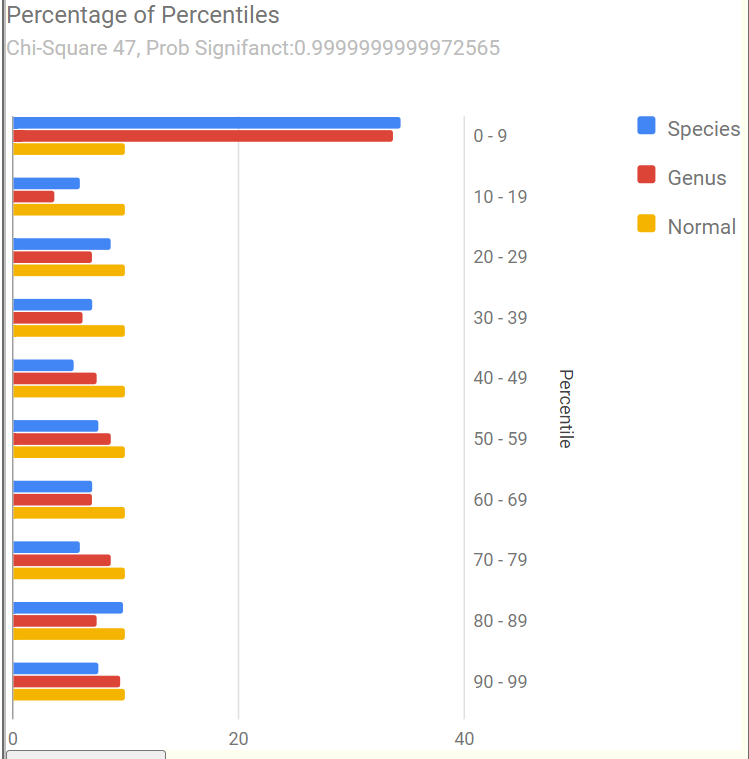
First, an old sample that she happened to have where we see Chi-Square at 6. The first of the recent samples had it jumping to 55, A normal microbiome is expected to have a Chi-square < 13. A higher value indicates a statistically significant, abnormal microbiome.
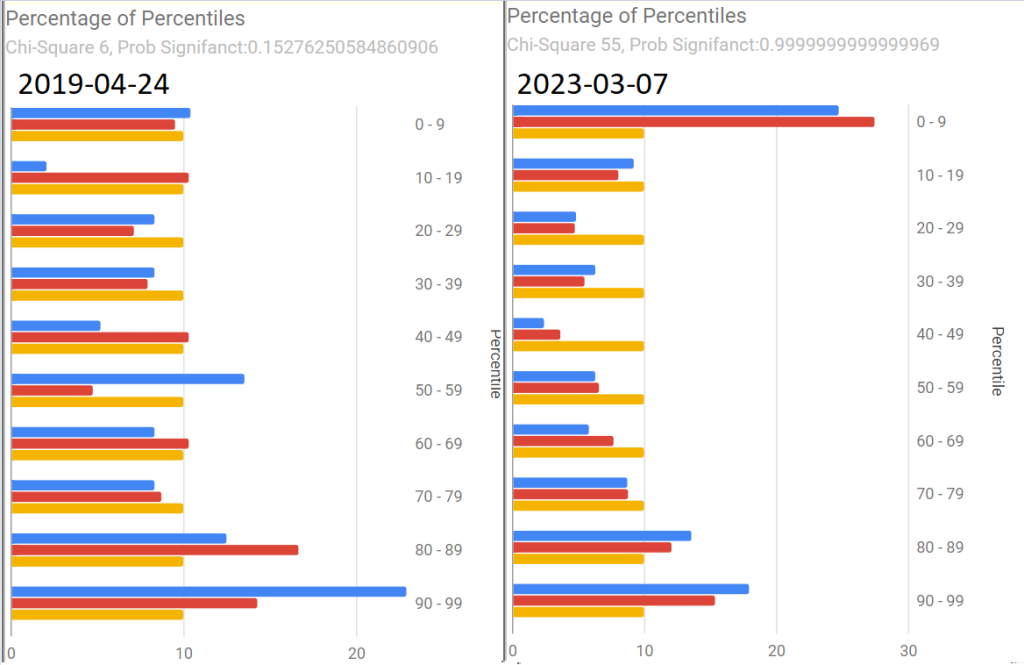
The next three show the changes with antibiotics. Chi-square went from 46 to 50 with a dramatic shift and then drifted down to 30.
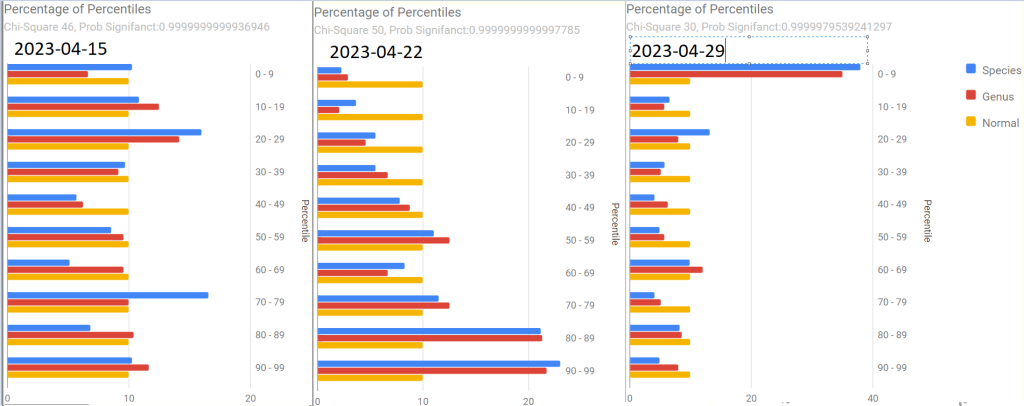
The latest sample increased upward again, with the pronounced spikes that are common with ME/CFS being there.
The raw numbers are also shown. I will spare your eyes by omitting them.
The Events Around the above Samples
- 7 Mar – Before
- 23 Mar – Day 4 AmoxClav
- 15 Apr – More
- 22 Apr – Final Day of AmoxClav (30 days of AC)
- This sample has a low Lab Read Quality, this may account for the number of spikes in its report.
- 29 April – After 3 days of Aprepitant + Erythromycin (this was a BIG difference from Tess and was the intervention that seemed to give me the baseline increase this time).
As with Tess, let us see how these items rank in each sample. As with Tess, imipenem is the most common best suggestion.
| Criteria | 7-Mar | 23-Mar | 15-Apr | 22-Apr | 29-Apr | 22-May |
| Amoxicillin | -104 | 95 | 276 | 296 | 432 | 402 |
| Erythromycin | 59 | 253 | 340 | 236 | 222 | 228 |
| Aprepitant | 393 | 297 | 260 | 320 | 280 | 80 |
| Highest | 632 | 497 | 635 | 610 | 650 | 594 |
| cefaclor hydrate | imipenem | imipenem | imipenem | cefoxitin | cefoxitin |
Going Forward
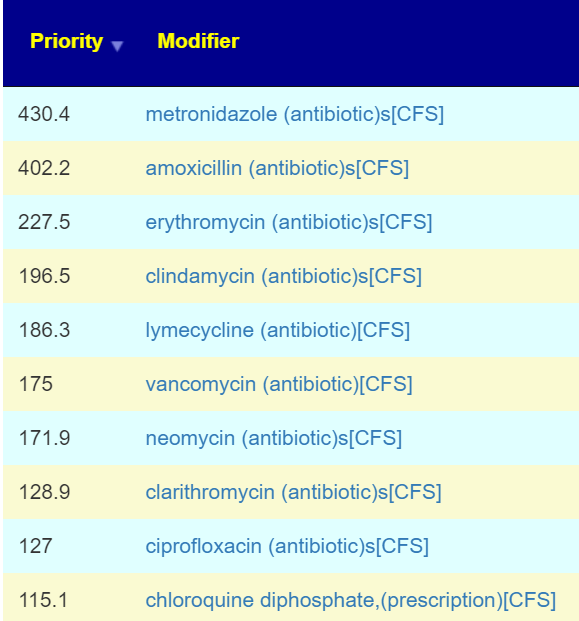
As a result of a conference call with some of the Remission Biome Project, and Dr. Jadin’s Current Protocol for ME/CFS. I annotated all of the antibiotics used in studies for ME/CFS, Lyme, and related conditions with [CFS]. This allows us to quickly see the “consensus” antibiotics (i.e. used in studies and suggested by microbiome prescription algorithms).
The top ones are shown before (Just enter “CFS” in the Search dialog)
Only two of these were negative for her (doxycycline and ampicillin) with docycline sibling, minocycline being just 21).
I would suggest using this list to pick 2 antibiotics to do a one week course and then take a 3 week break. After the course, then do some of these probiotics. I am inclined to omit L.Casei because the strain used in Yakult is a negative. Thus we end up with these three as top suggestions. P.S.
- bacillus subtilis (probiotics) : 342 @ 1 – 10 BCFU/day
- bifidobacterium breve (probiotic) :328 @ 2-15 BCFU/day
- bifidobacterium infantis,(probiotics): 292 @ 1 – 10 BCFU/day
Note the weight of these are above many of the antibiotics above. I usually advocate single species. The Bifido is available from Custom Probiotics with their recommended dosages above the amount listed above.
Part Deux — More Samples!
Her description of subjective changes: generally keep improving in terms of PEM, function etc. (was definitely a dip around the 2nd ‘constipation’ sample)
- 1st, [2023-06-14] in the series just a temporal sample, no additional treatments
- 2nd, [2023-07-15] in the series I had a major episode of constipation – wanted to catch that
- 3rd, [2023-07-20]last one was was post my 2nd treatment of aprepitant+erythromycin
Sample Comparison
We include the prior one above for easy reference). The key change items are:
- The new Anti inflammatory Bacteria Score has seen a dramatic increase from 17%ile to 73%ile. The four prior samples were 7.6%ile, 8.2%ile, 3.9%ile and 6.9%ile
- Outside Kaltoft-Møldrup is dropping. In terms of %age of reported: 32% -> 28% -> 29% ->16%
- The high and low Enzymes also seem to be dropping
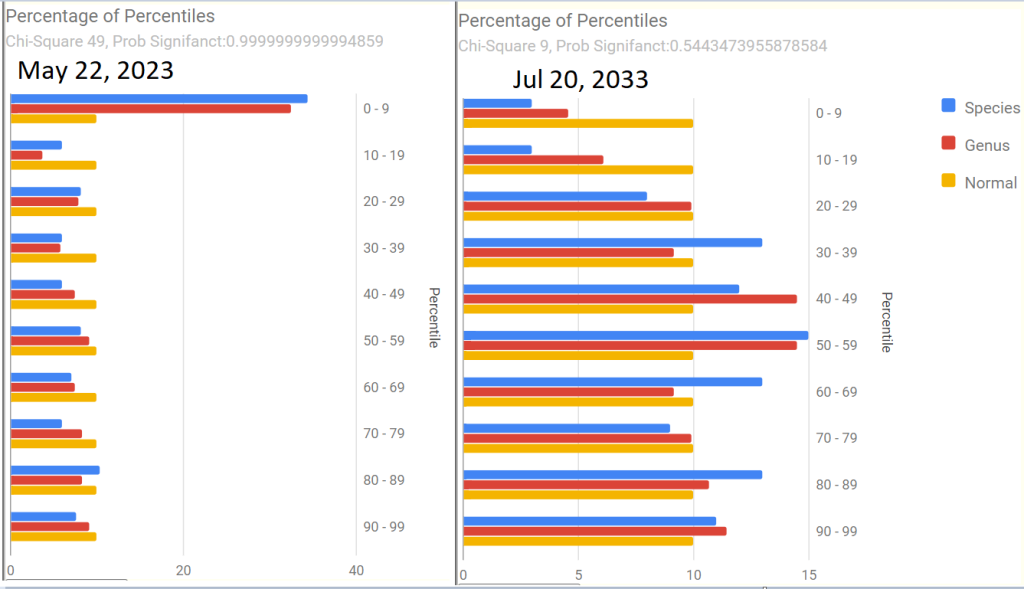
- The last sample had a Chi-Square of 9, that is a probability of 0.54 instead of the .9999999… for all other samples. Unfortunately, the poor read quality makes this fuzzy.
- Note: The last sample has a low read quality (thus less bacteria types are being reported)
| Criteria | 22-May | 14-Jun | 15-Jul | 22-Jul |
| Shannon Diversity Index | 69.4 | 29.20 | 43.00 | 15.00 |
| Simpson Diversity Index | 54.7 | 7.60 | 27.50 | 60.00 |
| Chao1 Index | 72.4 | 0.87 | 21.40 | 8.30 |
| Anti inflammatory Bacteria Score | 17.0 | 30.90 | 43.60 | 73.20 |
| Chi-Square Score | 49 | 51 | 32 | 9 |
| Lab Read Quality | 7.2 | 10.9 | 6.6 | 2.3 |
| Bacteria Reported By Lab | 659 | 752 | 512 | 375 |
| Bacteria Over 99%ile | 10 | 12 | 1 | 4 |
| Bacteria Over 95%ile | 22 | 24 | 2 | 20 |
| Bacteria Over 90%ile | 45 | 41 | 13 | 39 |
| Bacteria Under 10%ile | 199 | 229 | 189 | 19 |
| Bacteria Under 5%ile | 186 | 208 | 184 | 3 |
| Bacteria Under 1%ile | 167 | 165 | 166 | 0 |
| Lab: BiomeSight | ||||
| Rarely Seen 1% | 25 | 13 | 0 | 0 |
| Rarely Seen 5% | 49 | 37 | 7 | 1 |
| Pathogens | 32 | 34 | 36 | 21 |
| Outside Range from JasonH | 4 | 7 | 7 | 4 |
| Outside Range from Medivere | 14 | 19 | 19 | 14 |
| Outside Range from Metagenomics | 6 | 7 | 7 | 6 |
| Outside Range from MyBioma | 4 | 6 | 6 | 4 |
| Outside Range from Nirvana/CosmosId | 18 | 19 | 19 | 18 |
| Outside Range from XenoGene | 33 | 34 | 34 | 33 |
| Outside Lab Range (+/- 1.96SD) | 11 | 12 | 1 | 13 |
| Outside Box-Plot-Whiskers | 56 | 75 | 23 | 50 |
| Outside Kaltoft-Møldrup | 209 | 212 | 150 | 61 |
| Condition Est. Over 99%ile | 0 | 0 | 1 | 0 |
| Condition Est. Over 95%ile | 0 | 0 | 1 | 0 |
| Condition Est. Over 90%ile | 1 | 0 | 3 | 0 |
| Enzymes Over 99%ile | 62 | 1 | 5 | 2 |
| Enzymes Over 95%ile | 130 | 3 | 18 | 11 |
| Enzymes Over 90%ile | 215 | 12 | 99 | 33 |
| Enzymes Under 10%ile | 429 | 211 | 171 | 304 |
| Enzymes Under 5%ile | 310 | 146 | 142 | 211 |
| Enzymes Under 1%ile | 152 | 85 | 73 | 47 |
| Compounds Over 99%ile | 31 | 0 | 3 | 1 |
| Compounds Over 95%ile | 64 | 2 | 9 | 11 |
| Compounds Over 90%ile | 106 | 7 | 48 | 24 |
| Compounds Under 10%ile | 959 | 1096 | 1009 | 1015 |
| Compounds Under 5%ile | 909 | 1041 | 981 | 971 |
| Compounds Under 1%ile | 860 | 1009 | 956 | 922 |
Since we had a symptom of constipation, let us see how well the samples match that reported from Studies on PubMed — there were no matched. When we went to our Special Studies, we see that the microbiome followed the reported symptoms. We then look at the top value from Special Studies — which was Long COVID for all samples. We see the lost of ground around the constipation and then regaining the progress.
| Criteria | 22-May | 14-Jun | 15-Jul | 22-Jul |
| Special Studies | 7%ile | 14%ile | 15%ile | 7%ile |
| Top Item Long COVID | 35 % | 44 % | 41 % | 36 % |
Next we go and look at aprepitant and erythromycin
| Criteria | 22-May | 14-Jun | 15-Jul | 20-Jul |
| Aprepitant | 80.4 | 113.7 | 205.8 | 169.9 |
| Erythromycin | 227.5 | -76.8 | 226.7 | 194 |
| Best CFS antibiotic Priority / Max Priority | metronidazole 430 /549 | lymecycline 176 /307 | amoxicillin 424 / 527 | amoxicillin 351 / 484 |
The Percentage of Percentile show quite a shift — unfortunately, it is unclear if this is a temporary after effect of constipation, poor lab read quality, or the above aprepitant and erythromycin. The next sample may resolve this issue.
Is the Project working — YES
We are seeing both subjective improvement and object improvements.
Personally, I like what appears to be a shift towards Cecile Jadin’s approach — not continuous antibiotics but a course (7-10 days) followed by a break (ideally 3 weeks). Often I find that ME/CFS people tend to be impatient and just want to keep pressing on hard… which I have observed often result in tripping and rolling down the hill to where they were (or worst).
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide information on rotations etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
1 thought on “The Remission Biome Project: Tamara Romanuk”
Comments are closed.