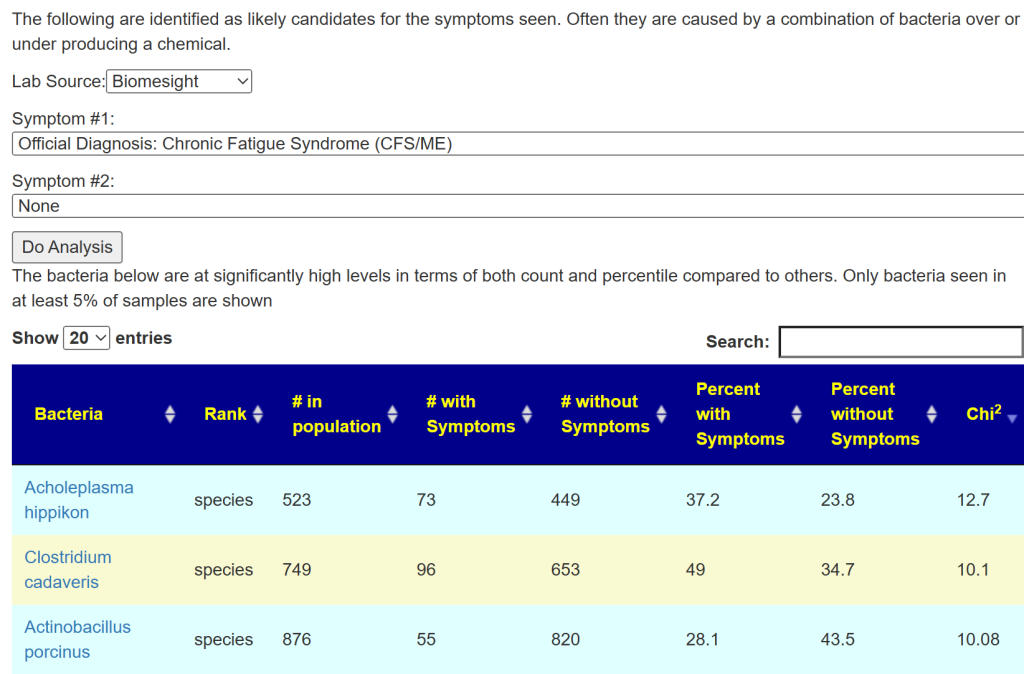
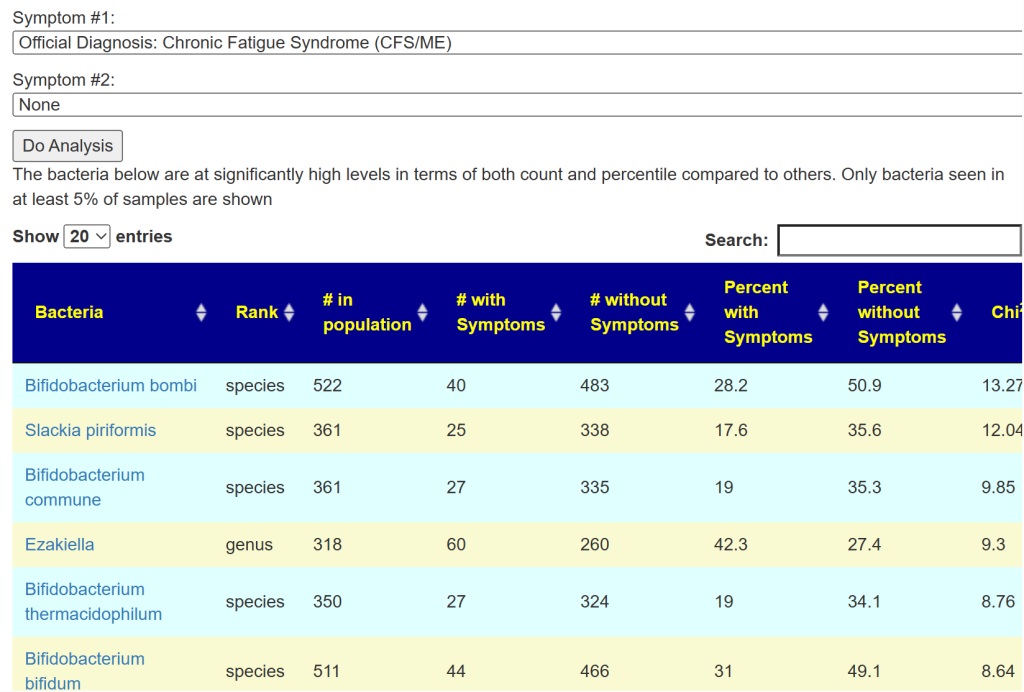
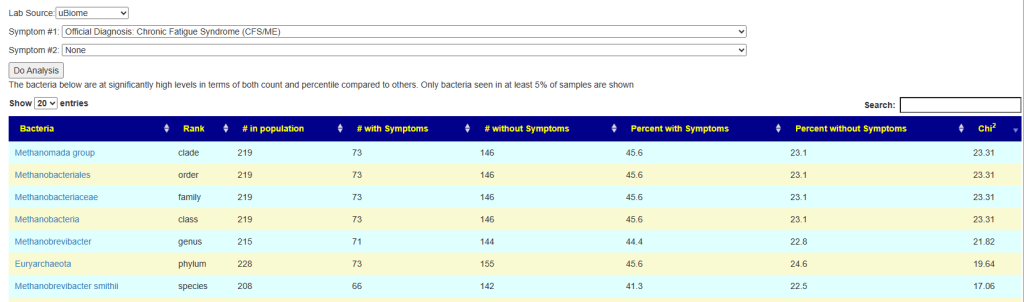
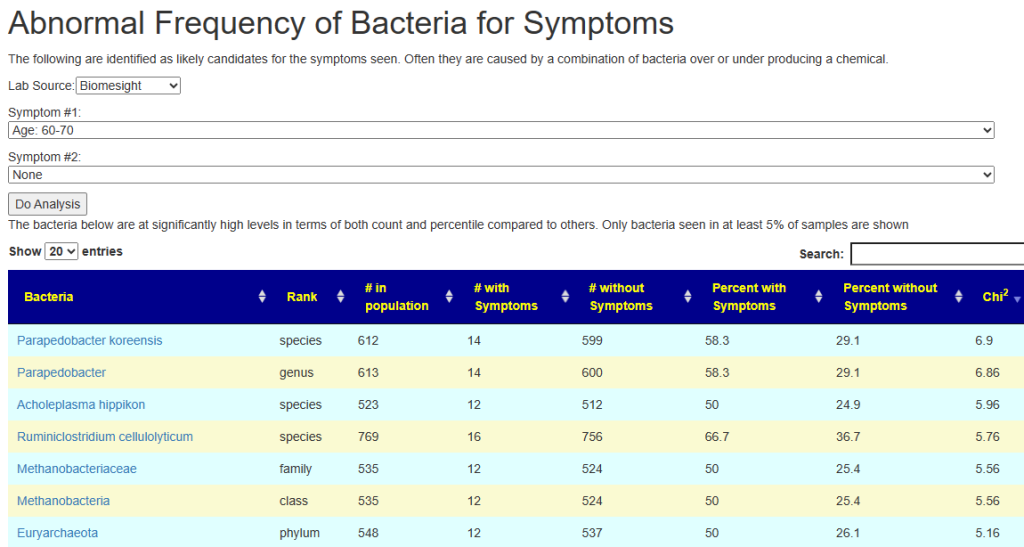
The question arises, what other conditions are associated with high levels of both of these? Fortunately, this can be obtained from the Microbiome Prescription databases.
Amyotrophic lateral sclerosis (ALS) Motor Neuron
Autism
Crohn’s Disease
Depression
Graves’ disease
Inflammatory Bowel Disease
Irritable Bowel Syndrome
Juvenile idiopathic arthritis
Liver Cirrhosis
Long COVID
Metabolic Syndrome
Mood Disorders
Multiple Sclerosis
Obesity
Parkinson’s Disease
Psoriasis
rheumatoid arthritis (RA),Spondyloarthritis (SpA)
Schizophrenia
Stress / posttraumatic stress disorder
Type 2 Diabetes
Ulcerative colitis
I also pulled the studies where the study specifically cited both are high. The above list were occasionally from taking data from two different studies.
A responsible medical professional would test a patient’s Lactobacillus and Bifidobacterium levels beforesuggesting probiotics to a patient. If your MD makes that recommendation without testing and you have any of the above conditions — it may be time to file a complaint with their supervisors or governing body citing the studies.
A reader forwarded me a study and some of it was interesting hints on this issue.
In vitro experimental results show a potent inhibitory effect (greater than 90%) of chloroquine, a historical antimalarial active ingredient, and clavulanic acid, a β-lactam antibiotic widely used in combination with amoxicillin [80]. A significant inhibition of the enzymatic activity has also been observed with the antihypertensive drug verapamil and the histamine H2 receptor antagonist cimetidine, although the clinical use of the latter is currently anecdotal
My idea is to examine which bacteria these items impact and see if there is a pattern.
The full list is below
Active Ingredient
Indication
Chloroquine
Antimalarial
Clavulanic acid
Antibiotic
Colistimethate
Antibiotic
Cefuroxime
Antibiotic
Verapamil
Antihypertensive
Clonidine
Antihypertensive
Dihydralazine
Antihypertensive
Pentamidine
Antiprotozoal
Isoniazid
Antituberculous
Metamizole
Analgesic
Diclofenac
Analgesic and anti-inflammatory
Acetylcysteine
Mucoactive
Amitriptyline
Antidepressant
Metoclopramide
Antiemetic
Suxamethonium
Muscle relaxant
Cimetidine
Antihistamine (H2 antagonist)
Prometazina
Antihistamine (H1 antagonist)
Ascorbic acid
Vitamin C
Thiamine
Vitamin B1
We have 14 items that we have data on.
At the family level, the following at the commonly impacted — all were decreased.
Bacteroidaceae – 14
Desulfovibrionaceae -14
Enterobacteriaceae -13
Clostridiaceae -13
Peptostreptococcaceae -13
At the genus level we have these all at 14 matches and decreasing
Bacteroides
Bilophila
Lawsonia
Desulfovibrio
Anaerorhabdus
Desulfocurvus
Desulfobaculum
Halodesulfovibrio
Mediterranea
Pseudodesulfovibrio
Desulfohalovibrio
Desulfocurvibacter
There are no clear smoking guns. When we include Special Study: Histamine or Mast Cell Issues we see that histamine issues are associated with lower levels of many bacteria (where as the above are those implicated in higher levels). We also looked at histamines in Exploration: Salicylate Sensitivity And the Microbiome, where we see under detection usually being the characteristic for histamine issues (except for Rothia mucilaginosa.
Doing cross checking, we find that the following are not reported impacted by the above AND are low in the other studies:
Methanobacteriaceae (family) – none
Heliobacteriaceae (family) – none
Anaeroplasmataceae (family) – none
Desulfocella (genus) – none
Spirosomaceae (family) – none
Rhodocyclaceae (family) – none
Cytophagaceae (family) – none
Ezakiella (genus) – none
Halobacteroidaceae (family) – none
Burkholderiaceae – only 1 impacts
Limosilactobacillus – only 10 impacts
All of the “none” are most likely due to this family or genus not be measured in the studies used. This leaves one bacteria of interest: Burkholderiaceae.
Bottom Line
We have no clear pattern. The drugs at the top likely makes room for bacteria that are low in frequency and amount to grow. Our attempt to find the bacteria ignored by the drugs above AND which are seen at low levels only turned up one candidate with a manual review: Burkholderiaceae.
Writing code to drill deeper may find more — stay tune.
I am newly ill from ME/CFS (4-5 months) and wonder if my results look like a “typical ME/CFS” for you, or Long Covid for that matter. I am a bit confused and some of the recommendations are contradictory.
From Reader. He used Biomesight.com (serves the world, discount code “Micro”)
This will be an interesting analysis — the microbiome evolves over time, so a 20 year ME/CFS and a few months of ME/CFS will have differences. I know of no clinical studies looking at “fresh ME/CFS”. There are studies for “fresh Long COVID”.
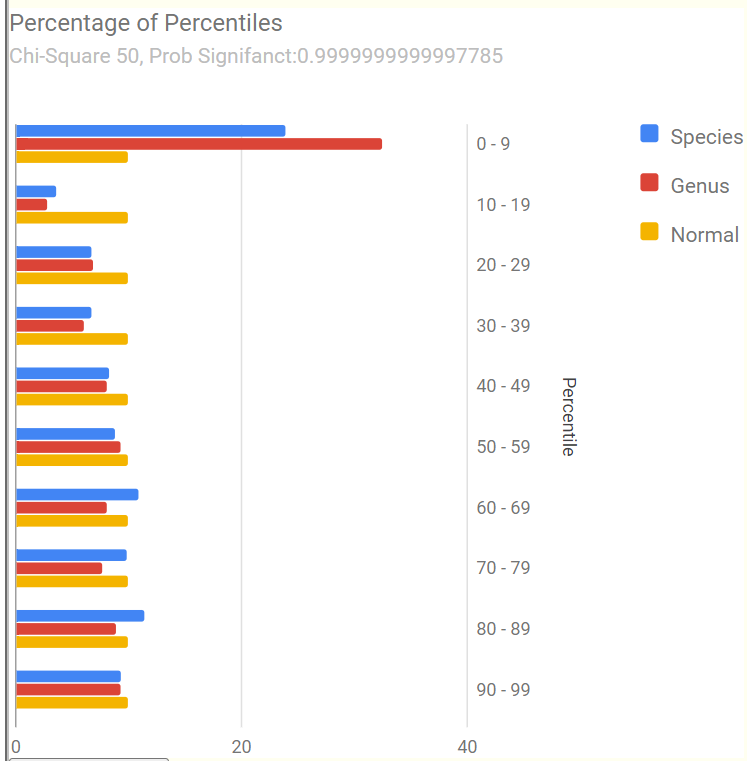
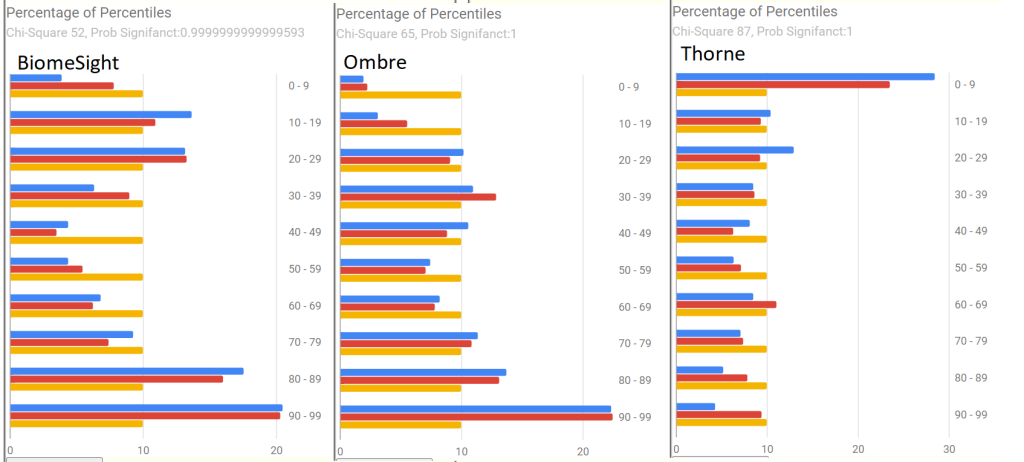
Percentages of Percentiles
This tend to have a regular pattern for ME/CFS and Long COVID for most people. Over representation of bacteria in the 0-9% percentile range. This matches his pattern. A healthy person would have all of the bars around 10% – they are not.
Going to the Potential Medical Conditions Detected, there was nothing significant. Prevotella copri is 2% (78%ile) which is borderline for mold issues — it would be good to do inspect the home for that risk. Dr. Jason Hawrelak Recommendations comes in at 99.7%ile with high Methanobrevibacter and low Bifidobacterium being the most severe shifts. Anti inflammatory Bacteria Score is 63.1%ile which is a bit better than most people. So, many medical professionals would tell the patient that I cannot see anything wrong.
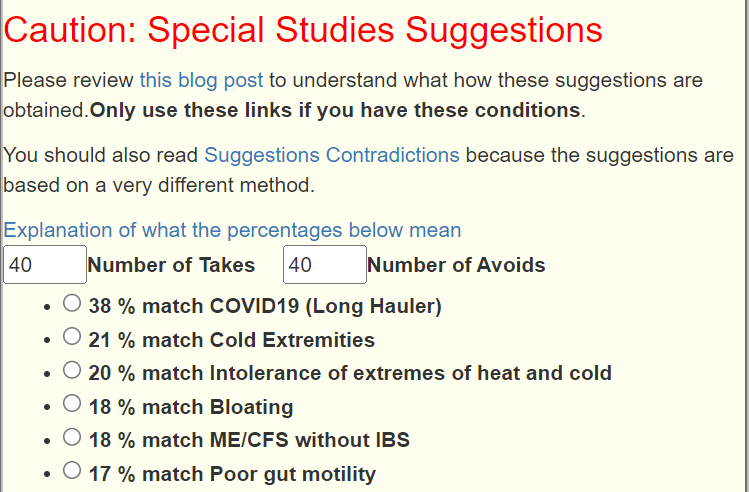
Special Studies
Special studies are statistical studies that uses samples uploaded and look at the self-reported symptoms. The analysis is done individually for each lab (needed because of differences in how labs process samples). In this case… we see that COVID Long Hauler is by far the strongest match, almost double the next one.
I did the usual Just Give Me Suggestions and then did the Long Hauler suggestions . This gave five (5) packages of suggestions. I then looked at the antibiotics suggestions, focused on those used with ME/CFS. The top ones are:
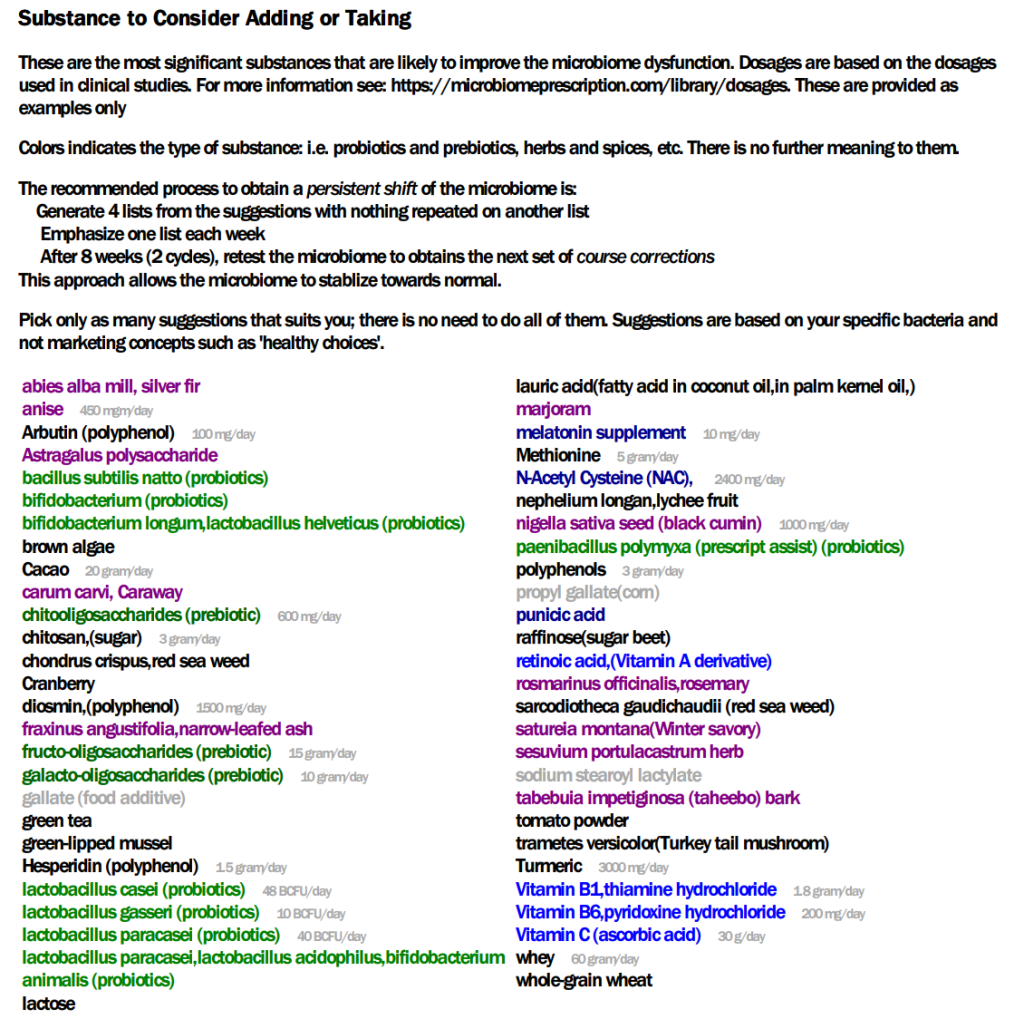
The list of suggestions to take is actually bigger than usual.
REMEMBER: There is no need to take all of them, just take what works for you (i.e. no adverse effect and acceptable cost).
Probiotics should be rotated (change to a different one) every 7 to 14 days. Probiotics often work by producing natural antibiotics. Continuous taking of the same probiotics may result in it not working because of “natural antibiotic resistance”.
The colors have no meaning except as indicators for category. For example, green is probiotics
Dosages are those that have been used in clinical studies (for other conditions), and thus deemed safe dosages. Often I have see people taking < 1% of these dosages and wondering why nothing happens.
For example, it you are lactose intolerance, then ignore the lactose suggestion. If not, regular cups of good Belgium Cacao would be a good prescription!
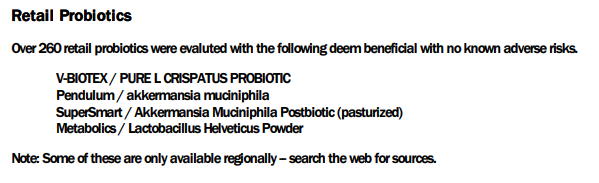
The safe retail probiotics were calculated to be
symbiopharm/ symbioflo2 – an E.Coli probiotic from Germany
Filmjölk (SE) / Filmjölk – a Swedish milk drink
enterogermina – Bacillus Clausii
SunWavePharma / Spor Sun – Bacillus Clausii
Why are these lists not the same? The latter list are ones that will not shift a single one of the bacteria we are focused on in the wrong direction: NOT A SINGLE BACTERIA. This is an extremely safe conservative suggestion. The top list with probiotics in green often contain probiotics that shifts 30 bacteria in the right direction and 3 in the wrong direction. The odds are that they are very likely to help.
We have a third list of probiotics (to make probiotic suggestions even more confusing), the KEGG suggestions. This looks at what enzymes your microbiome are low in, then sees which probiotics can provide those enzymes. Our goal is to reduce enzymes starvation; this cascades in metabolites — chemicals that the body uses — starvation. The key items from this list are:
If you have significant brain fog, I would be careful with taking lactobacillus probiotics. Some retail species can increase brain fog.
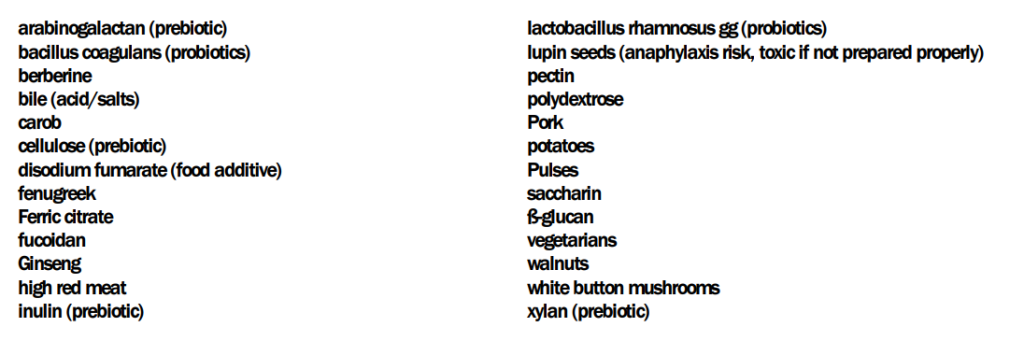
The Avoids
Frequently “good suggestions for general health” are bad for some conditions. The avoid list of things to avoid is short
Some quick translation: no iron supplements (ferric citrate), beta-glucans usually means no oats, barley or Reishi mushrooms. The names are those used in clinical studies — so they tend to be “unresolved” often in common speech.
Suggested Cycles
After implementing the above suggestions for 6 weeks, do another test and see what has changed.
Questions and Answers
Q: Is it best to take the antibiotics + the protocol you suggested ? Or is it one or the other?
A: My own choice would be to do both at the same time. If you follow Jadin’s approach, then
First week of antibiotics per month — no probiotics at the same time
Second week do some of the probiotics (I am inclined towards the E.Coli probiotics but that is based on my personal experience — your mileage may vary)
Rotate the other supplements over the weeks. I would suggest 10 days and then change to a different set.
Q: And lastly, in the « Avoids », the « vegetarians » suggestion is a little confusing to me. What does it mean?
Vegetarians mean no animal or fish is being consumed. So, have fish — but some animal proteins are to be reduced: no pork, moderate beef. Duck, chicken and rabbit are fine.
Q: The suggested dosage in the suggestions seems very high. 30g of Vitamin C per day??? Is this correct ?
The actual dosage should be discussed with your medical professional. The dosages are the highest that have been done in clinical studies and thus assumed to be safe dosages. We have no data on what the threshold for an effective dosage should be. I have seen a few studies where 1000 mg of a substance has minor/no effect while 1100 mg has twice the impact and 1200 mg has four times the effect. For many substances there seem to be a threshold that triggers changes.
Usually start at 1/8 of the dosage and double it every second day until there is a response. If very good keep at that dosage. If bad, cut the dosage in half and try a few more days. Give the body time to adapt.
My comment about mold caused him to check his environment carefully…. what he found out of sight!
“Environmental factors – exposure to mold or toxins has been suspected as a trigger for ME/CFS. However, associations of specific environmental factors with ME/CFS have not been established.” [CDC]
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide solid information on rotations, dosages, etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting. Some suggestions may be counterindicated for other medications you are taking and medical conditions.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
This is from a reader that I have been corresponding with since 2017 and known from online groups for decades..
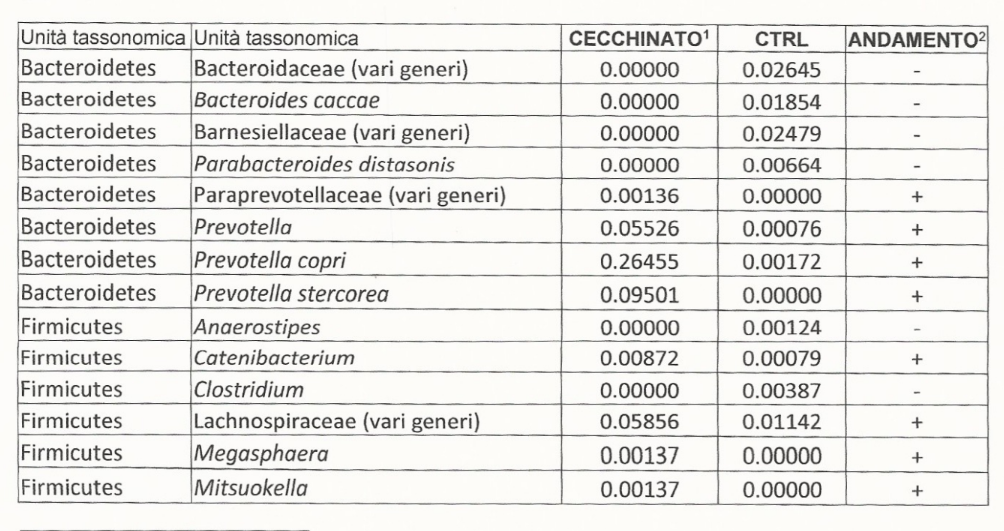
Okay, you don’t want the full saga 😀 (joking ) and so I’ll write the first current impressions of a ME/CFS patient since 1998. I am someone who has tried everything; really everything. First of all, as I had already told you in chat, I use as a criterion of improvement in the disease the increase in cardiovascular tone, which actually happened for a short time as long as I kept a diet that was not exactly ironclad, but very difficult for me: it involved cutting out all refined sugars.
For those interested, I talked about it here : https://www.fable.it/fluorochinoloni-hrv-dieta-e-me-cfs/ (in Italian — use Google translate) . For the first seven days of the diet nothing changed, nothing! After these 7 days suddenly, keeping to this diet , cardiovascular tone started to increase until … well … I kept the rest of the diet but reintroduced sugars (but not alcohol). Then improvement stopped (but maintained existing improvements).
From Reader
Recent significant events are:
fluoroquinolones toxicity in 2020
supplements of akkermansia muciniphila one month before last sample (see below for his experience)
Ancient Test Results
A test result from 23 August 2016 is below. The test is only of a few bacteria without any ranges of normal valid. We will compare the few items reported with the latest Biomesight test. There was little change over 7 years.
Any persistent Fluoroquinolones artifacts?
I did a behind the UI comparison of what Fluoroquinolones changed with his sample. Although it has been 3 years, I am curious. No impact would have 50-50 agreement. We have 64 bacteria showing the effect that that Fluoroquinolones would cause, and 43 showing the opposite effect. This results in a P-Value of 0.0423 from chi-square. A P-value below 0.05 is deemed statistically significant in medical studies. So, this is evidence that the impact of Fluoroquinolones is still there after 3 years.
This is an interesting observation — picking the wrong antibiotic may have effects that persists for years.
The microbiome was been relatively stable over 7 years. In fact, the Biomesight test clarify how extreme the values are (which is not clear from the earlier report).
Where do we go from here?
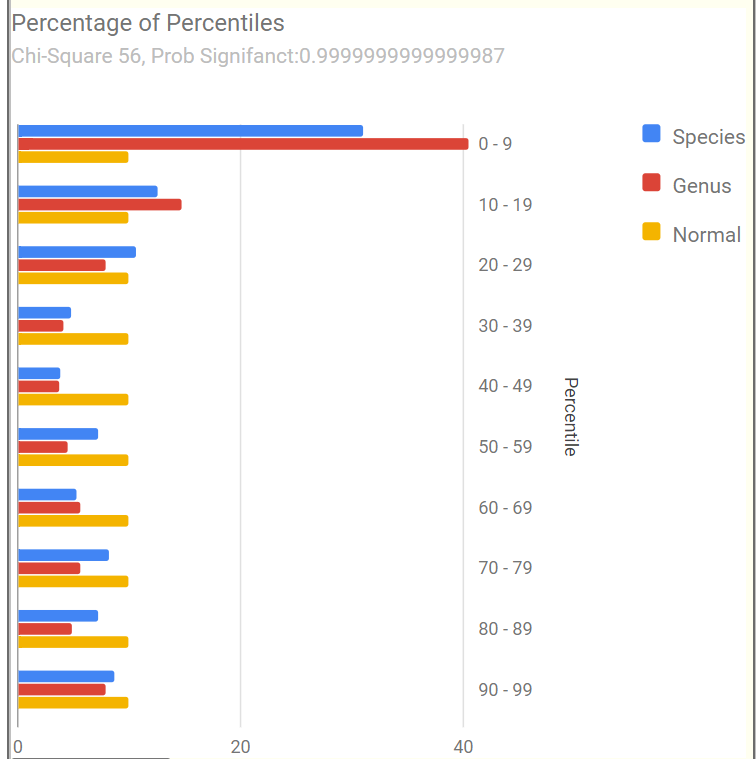
The Percentage of Percentiles pattern shown below is a match for that seen with many ME/CFS or Long COVID microbiome.
Nerdy Explanation: Using percentiles, the data is transformed to an uniform distribution. An unbias sample (a.k.a. normal or healthy), would have the same number in each 10%ile range. We do not. We have the typical spike in the 0-9%ile range (i.e. too many species and genus that have token representation).
The most important/concerning bacteria identified was Prevotella copri. This bacteria made up 43% of the microbiome!!!! This bacteria is often associated with mycotoxin being present in the environment [2020]. This usually means examining the living space for mold and fungi, as well as avoiding foods likely to have mold (see WHO for more information). His response to this comment was:
Yes, I live in a north-oriented flat where never there is sun on walls. Only in a bedroom not used anymore as bedroom I have visible mold (picture attached). I have tried treating with chlorine bleach. In February 2023, I called a painter. He treated with anti mold solution and thermal painting (which can ben dangerous. I would never lived in that bedroom till the smell went away. And yes, sun recharge me and I don’t know if it also affects mycotoxins. However in my block / area where I live, we never have less than 60% humidity, but in summer usually we have 70-75% so… humidity is a concern.
From Reader
There are many sites providing suggestions on this issue, a few are: [Aircare Hawaii] and this
Is mold related to humidity? European and Italian homes are typically built with reinforced concrete frames and brick walls. Walls and ceiling surfaces are finished with mortar/plaster and water base paint. As water base paint is not waterproof, plaster finishing tends to absorb and retain humidity. These areas can become damp or wet as a result of a water leak or condensation of vapors produced by appliances and normal household activities.
The use of a waterproof paint after cleaning (and running a dehumidifier) in the bedroom is one possible approach. Reader responded (to his delight) that water proof paint was used!
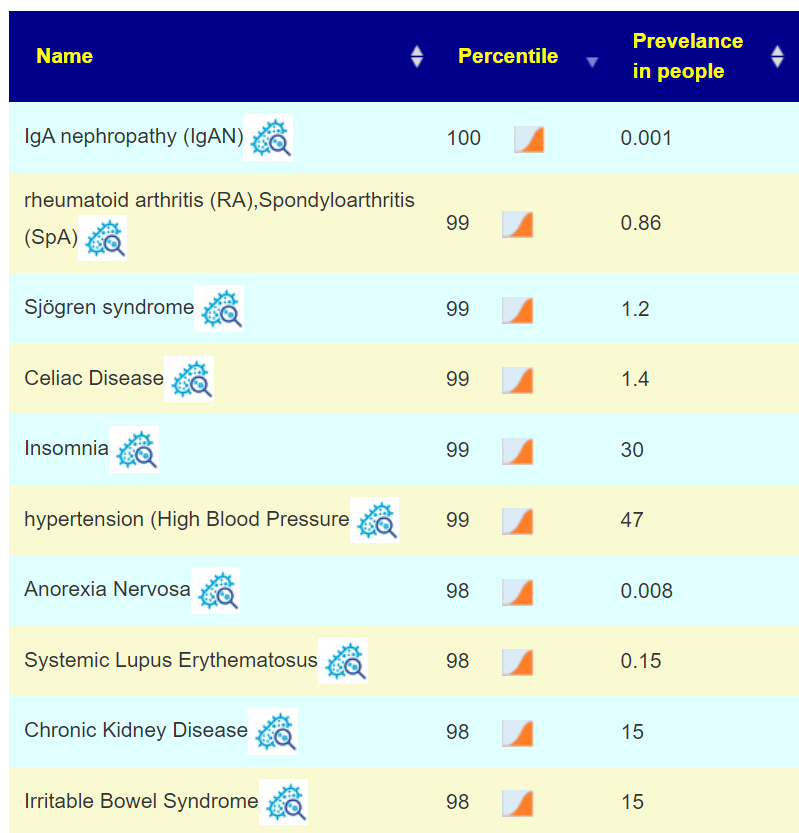
This plus other shifts, matches to a host of conditions shown below. Many are co-morbid with ME/CFS.
The Computed Probiotics from KEGG Enzymes had some very high numbers (over 600!). High numbers mean that there count of many enzymes is very low. Some of these are available in probiotics, with the top feasible suggestions being:
I will defer the rest of the suggestions to the PDF, attached below. It is interesting to note that akkermansia muciniphila probiotics is well recommended (see experience below).
In this case, we have good positive reader experience happening before the suggestion was made! It should encourage the reader to trust the other suggestions (after all, “one suggestion worked before he got it!” 🙂 )
None of these are typically used for ME/CFS (but other tetracyclines are). We have one big target: P.Copri. I am hoping that you have a cooperative MD. I checked around for information on antibiotics that often have little effect on P.Copri, these studies have extensive lists.
I am inclined to metronidazole, which is often used in treating ME/CFS (also in this 2010 study), and 98% effectiveness reported in this 2019 study.
Akkermansia Muciniphila Experience
Another thing Ken, is the sensational discovery this year of Akkermnasia Probiotics (in my case from Metagenics). In my first two days I went from going to the bathroom once a day to going three four times. How many times have we read that a normal bowel transit involves 1 evacuation a day to one every 2-3 days ? No ! The ideal transit is to go to the bathroom about half an hour after eating ! Well, this happened to me while supplementing Akkermansia once a day. And it is only one strain !!! Not only that ! I felt less “Fight or Flight” but more serene, even when I woke up from my night sleep. Even with scabs on my eyes that who knows how many years I haven’t found (how many of us have perpetually dry eyes ?). I stopped the supplementation after a month and am now resuming it.
Why am I writing you this Ken ? To waste your time !!! No, I am writing this to you because I had first read about this Akkermansia three years ago on the label of an Austrian product, Omni Logic Plus, which contains a lot of good stuff (FOS, GOS , etc.) to feed this specific bacteria, Akkermansia . Three years of supplementation every day has not improved anything. After just a few days of Akkermansia , that is, the strain that that Omni Logic Plus was supposed to feed, did the miracle ! What do I mean by all this ? That , my thought is that rather than acting on the food, if they are available as supplements, little bacterial strains should be introduced, for a far better effect.
From Reader
Questions:
Q: When the “nutrients” of the supernumerary bacteria present they grow. If you cut off their nutrients, the effect on microbiota diversity is extremely “reactive” !!! Whether this happened when I removed the sugars ?? Do you agree with my reasoning ?
A: Yes — consider a human population that is well fed (obese even). If you suddenly impose strict rationing on them, their behavior changes greatly (often with criminal actions).
Q: Is it more effective to remove the food that feeds the overrepresented bacteria and simultaneously supplement the underrepresented strains not so much with diet and food, but with probiotics ? An example of my personal case ? When in the report generated by your site I see among the recommendations clostridium butyricum , which I never tried in my life.
A: The algorithms effectively does that — identify the material that inhibits the overrepresented which do not impact the underrepresented. Also the reverse, feed the the underrepresented without feeding the overrepresented. You can try to calculate these manually — but its a massive amount of reading and searching. Microbiome Prescription uses some 1.8 million facts pulled from almost 12,000 studies.
Q: Who knows if it can give me the same benefits as Akkermansia? After years where weeks on end , I have tried various products. Like everyone else, I have been spending hundreds of Euros. For example:
probactiol duo ( billions of Saccharomyces boulardii)
A: The purpose of Microbiome Prescription is to compute the most likely ones based on your microbiome and what studies reports the effects of various probiotics are. This means greatly increased odds of positive effects! Much better (and cheaper in the long run) than trying things suggested by influencers or which worked for someone with a very different microbiome.
Your list is very short — 50% is what you recently discovered works!!
For probiotics, do one at a time for 10 days then rotate to another. Why? Their effect is often due to natural antibiotics that they produce. Keeping on them continuously allows “natural antibiotic resistance” to develop.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide solid information on rotations, dosages, etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting. Some suggestions may be counterindicated for other medications you are taking and medical conditions.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
Ken, I read so much of your stuff, I have ZME 39 years. My granddaughter has POTS and now she was diagnosed with SIBO and fructose Intolerance. Could you point us to a diet for SIBO; She has not been given one nor can find it. I thought of you right away, Please help. Have a great weekend, holiday.
What has been actually studied
First, the reality of SIBO diagnosis. IMHO, it tends to be a little “hit and miss“.
Although abdominal bloating, gas, distension, and diarrhea are common symptoms, they do not predict positive diagnosis. Predisposing factors include proton-pump inhibitors, opioids, gastric bypass, colectomy, and dysmotility. Small bowel aspirate/culture with growth of 10-10 cfu/mL is generally accepted as the “best diagnostic method,” but it is invasive. Glucose or lactulose breath testing is noninvasive but an indirect method that requires further standardization and validation for SIBO. Treatment, usually with antibiotics, aims to provide symptom relief through eradication of bacteria in the small intestine. Limited numbers of controlled studies have shown systemic antibiotics (norfloxacin and metronidazole) to be efficacious. However, 15 studies have shown rifaximin, a nonsystemic antibiotic, to be effective against SIBO and well tolerated. Through improved awareness and scientific rigor, the SIBO landscape is poised for transformation.
There are dozen of diets pushed by influencers for diverse reasons. I tend to be a “show me the clinical studies or reviews” type. What do we find is…
This narrative review suggested that there is a favorable association with monoprobiotics, fiber supplementation and mindful eating, and negative effects associated with low-FODMAP diets on the gut microbiome, especially in IBS patients. Applying these recommendations to the treatment of SIBO was inconclusive due to a lack of research including SIBO patients in the studies.
Our findings suggest preliminary evidence for a role of alternative therapies in the treatment of SIBO. However, robust clinical trials are generally lacking. Existing studies tend to be small and lack standardized formulations of treatment. Breath testing protocols and clinical symptom measurement greatly varied between studies. Large-scale, randomized, placebo-controlled trials are needed to further evaluate the best way to utilize alternative therapies in the treatment of SIBO.
My inclination is to encourage a suitable microbiome test (OmbreLabs, Thorne or Biomesight.com [discount code: Micro] and use the Microbiome Prescription site. There is an apriori set of suggestions based on the bacteria reported from studies. It is interesting to note that rifampicin antibiotic is suggested which is closely related to rifaximin which is cited in the study above, suggesting that working from the microbiome data is a reasonable approach. Other diet related items computed are:
Do just the items that you tolerate (physically, philosophically), there is not a need to do all.
Items to AVOID include:
cinnamon (oil.spice)
foeniculumvulgare,fennel
lactobacillus plantarum(probiotics)
oregano(origanum vulgare, oil) |
syzygiumaromaticum(clove)
thyme(thymol, thyme oil)
triphala
I would extend it to all lactobacillus probiotics because there are hostile to E.Coli probiotics.
Bottom Line
Working from an individual microbiome is the best way to proceed (IMHO). There are massive issues with both being sure of the SIBO diagnosis being correct AND no clinical evidence (except for antibiotics use) of any specific diet being useful.
The basis is that we look for bacteria that are seen more or less often than expected. Bacteria distribution is not a bell curve/normal distribution which makes the use of averages very suspect. Checking against frequency side-steps this answer.
I would be interested to see how the three separate consensus suggestions compare (i.e. not doing the uber consensus). Do the top takes & avoids match across the different labs, or are they different? Because if they are different then the algorithm is not robust to changes in lab.
Using the same data, the process that I will use is where items suggested in both are the same (i.e. take or avoid) or different recommendations. In pseudo sql:
Select Percent(A.Take=B.Take) from Suggestions1 A Join Suggestions2 B on A.substance=B.substance
The results actually surprised me!
Lab Comparison
Items
Agreement
Avg Difference
Ombre vs Biomesight
1705
100%
52
Ombre vs Thorne
1706
100%
100
Biomesight vs Thorne
1694
100%
54
My expectation was somewhere between 80-90%, the same range that I got doing cross validation. The Priority and weight are different, but the take or avoid decision are the same. The difference between these pseudo values was also calculated and added to the table above. Magic Soy on Ombre may be 430, on Thorne 330, on Biomesight 530.
Conclusion, the algorithm is more robust than I expected!
Caveat: This was done using “Just give me suggestions” collection of algorithm on each lab’s data. Disagreements are definitely expected when bacteria selection are “over-focused” and not including the holistic picture of the microbiome.
Comparing standalone suggestions – 2E, a reader wanted to know how similar Microbiome Prescription suggestions were using different data
In this post we are going to combine all of the consensus from the above 3 different sample reports and see what is shared by all of the suggestions. The goal is to see whether there is come convergence of suggestions.
Uber Consensus
We select the Multiple Samples tab and then check the three consensus reports. We should note the number of modifiers in each sample suggestions (over 6000 items were consider). This on the surface appears to be at least one, if not two magnitudes more than the suggestions from the labs,
The following are selecting the highest positive or negative entries where there is good agreement.
There were no probiotics in the above to take, only those to avoid. Interesting that the labs whose business model includes selling probiotics actually suggested these probiotics (ones to be avoided above)!!This have a strong aroma of conflict of interests.
Many of the above items were not suggested by any lab despite a few being typical — i.e. melatonin.
Other Observations
Percentages of Percentiles
For BiomeSight and Ombre, we compute percentiles based on samples uploaded. Thorne provides their own percentiles. We see a major contrast below.
Measure
BiomeSight
Ombre
Thorne
Jason Hawrelak
8 ideal (96%ile)
6 ideal (75%ile)
5 ideal (56%ile)
Bacteria Reported
748
886
3349
Shannon Diversity Index:
1.93 (89%ile)
3.34 (93%ile)
2.85 (70%ile)
Simpson Diversity Index:
0.2 (8%ile)
0.2 (5%ile)
0.3 (9%ile)
Chao1 Index :
17785 (89%ile)
33700 (89%ile)
341848 (70%ile)
The numbers are using based on the lab population
Bottom Line
The purpose of this series of post was to do a non-judgmental evaluation of the three lab reports and suggestions to help people make better choices. All of the steps that I did is very repeatable by anyone who wish to replicate this experiment. (P.S. If you do, I am not opposed to do a repeat set of posts with different data).
Key findings:
Only Biomesight provided AVOID lists (too short IMHO) — i.e. they are happy for you to keep feeding ‘bad’ bacteria
Only Biomesight provide studies links connected to their suggestions
The report from each lab are significantly different, howeverwhen that report is used with Microbiome Prescription algorithms, we get agreement. This is likely due to the nature of the algorithms used.
My impression is to use whichever lab is available to you (two sell in the US only, one world wide); ignore their suggestions and use the free suggestion engine on Microbiome Prescription.
Microbiome Prescription does provide detail evidence trail on every single suggestion it makes. Some of the evidence is less than ideal, but it is at least reasonable (and less than ideal data is diminished in weight).
I gave this an Excellent because it matched the criteria that I use:
Avoid lists are given
Evidence trail to studies for every suggestion
A large number of substances are evaluated
Weights are given for Take lists.
(And I acknowledge there is a conflict of interests here — but no financial gain).
The following videos illustrate the process to see the evidence trail.
Comparing standalone suggestions – 2E, a reader wanted to know how similar Microbiome Prescription suggestions were using different data
Process
It is very simple, look at their suggestions, look at any references they provided. Then look at Microbiome Prescription evidence trail for the same substances.
Suggestions
The number of suggestions were very few. They are listed below. None of the suggestions had links to studies supporting them.
Follow a ketogenic or low-carbohydrate diet
Avoid eating habits that interfere with sleep
Product Recommendations
Dipan-9®: Pancreatin
Effusio® Prebiotic+
Blueberry
Green Tea
Pomegranate
Xylitol
Stevia
FloraMend Prime Probiotic®
L. Gasseri KS-13
B. Longum MM-2
B. Bifidum G9-1
Undecylenic Acid – 10-Undecenoic Acid
Vitamins were:
Red: Vitamin B3, B12
Orange: Vitamin B6,B9
All probiotics were GREEN.
There was no scientific literature links provided to support these choices.
How do suggestions compare?
Analysis against Microbiome Prescription using the data they reported.
Vitamin B3: take 3, avoid 1
Vitamin B6: take 3, avoid 1
Vitamin B9: take 3, avoid 1
Vitamin B12, take 3, avoid 1
L. Gasseri: take 1, avoid 3
B. Longum: take 0, avoid 3
B. Bifidum: take 0, avoid 4
Blueberry: take 3, avoid 1
Green Tea: take 2, avoid 2
Pomegranate: take 1, avoid 3
Xylitol: take 2, avoid 1
Stevia: take 0, avoid 4
Pancreatin: take 1, avoid 0
ketogenic: take 1, avoid 3
low-carbohydrate diet: take 2, avoid 1
Undecylenic are in Microbiome Prescription database. Undecylenic has nothing on PubMed dealing with the microbiome that I could locate.
My Impression are:
For the 4 B-vitamins we have agreement.
For everything else, we have so-so agreement. In fact, the agreement is the same that you would expect with flipping a coin (random)
We have very few suggestions of what to take
We have no clear suggestions on what to avoid (beyond “other diet” types).
Bottom Line
Thorne gives almost no suggestions. There is no links to study supporting their suggestion. The suggestions seem to be ultra-safe suggestions that should work for most people. It if very questionable if the bacteria results were used for the suggestions.
As an ex-teacher, I would not give a grade, I would give an INCOMPLETE-FAILED, nothing of significance submitted. No real effort made.
The videos below shows how you can see the evidence for the suggestions on Microbiome Prescription.

Recent Comments