Over the last two weeks, there has been a couple of email pointing out possible errors in some citations. I am not surprised. I expect 90-95% correctness (i.e. 1 in 10 or 1 in 20) may be incorrectly entered. To improve the quality, we need independent review of the data. In one amusing case, I quoted my source correctly but that review study incorrectly cited it’s source. The data entry was right, the source document was wrong.
The articles are technical studies which often require advance reading skills and knowledge of this topic. Some of the sources are available in full on the web for free, others are behind a paywall. If you are connected with a university or college, you may have access thru your institution.
If you cannot access the full text of the source, then skip it. Extracts and summaries can contain errors.
Process
Just email me from the email account that you logged in with and I will add auditor or QA permissions to your account.
Doing it
When you logged in, you should see:
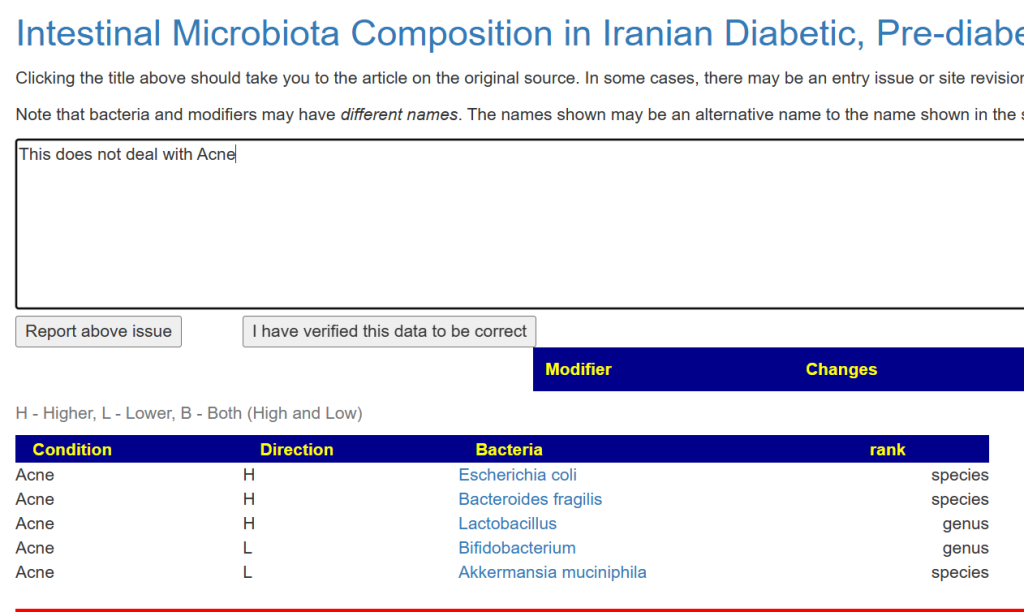
When you look at citations, you will see the ⚖️ icon (or a ✅ if someone has already checked) beside the citation.
Example for a list of citations
Note that there may be more in the study then what the titles implies. Often data is from Appendix and tables.
Clicking ⚖️ will take you to a page showing what was extracted and gives you an opportunity to correct it,
Click [Report above Issue] will send emails to me and to your self. If all of the information is correct, then click [I have verified..] and the next time you see the citation, there will be a ✅ beside it. Your email is stored beside the citation as the reviewer.
You will get an email confirming stuff
If there is information that was missed (more likely) please include the TAXON numbers of the bacteria. This speeds up the process. Often information was missed because of alternative spelling.
That’s the process. Short, simple and with the ability for me to quickly make corrections.
Bacteroides/Bifidobacterium (Ba/Bi) ratios “with Low Ratio showing a significant increase in propionic acid and being enriched in glycolysis functions, whereas High was enriched in amino acids and aminoglycolysis functions”
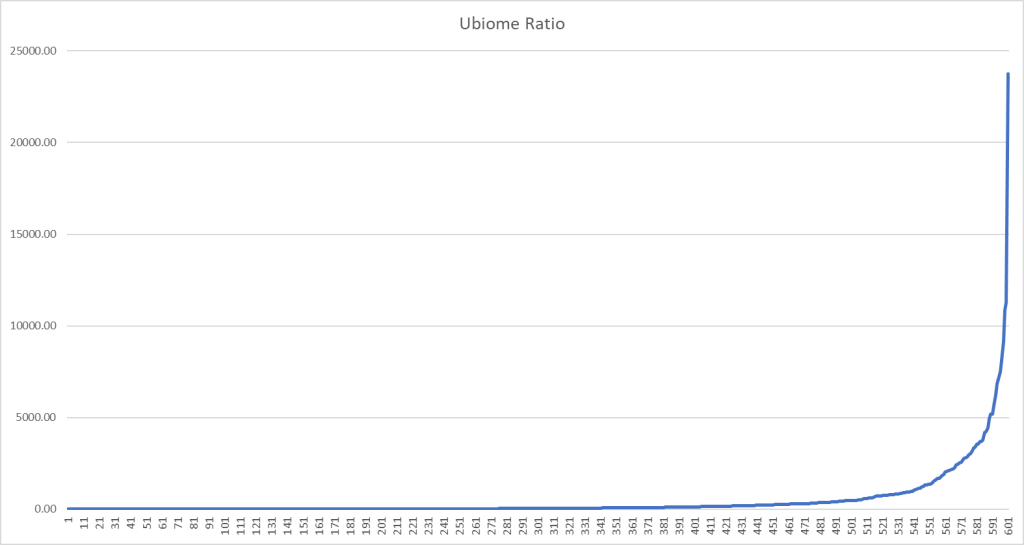
Of course, the question becomes what are low and high ratio? To answer that question, I pulled some data by lab
Ubiome Ratios
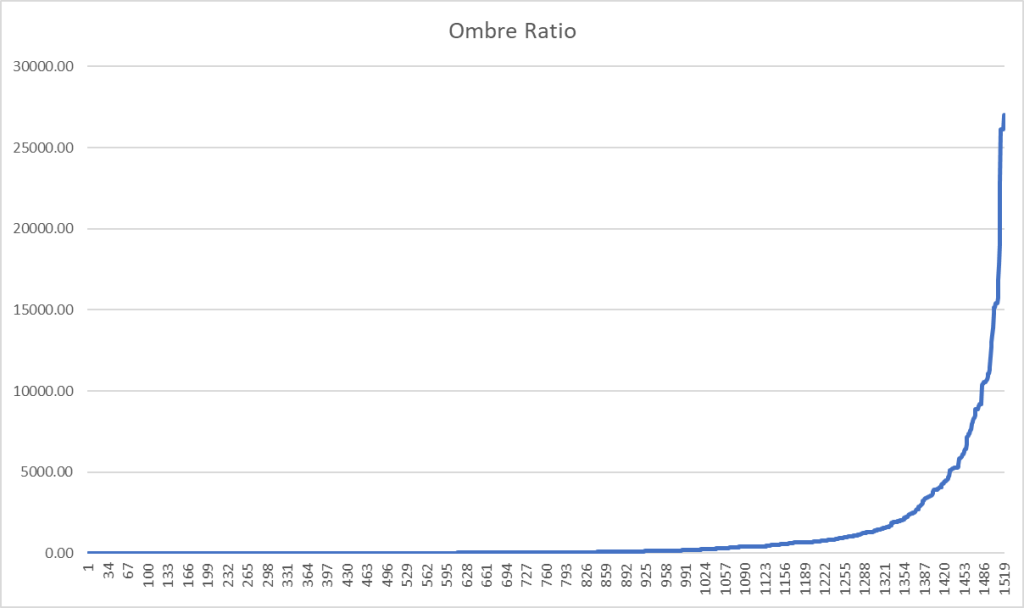
Ombre Ratios
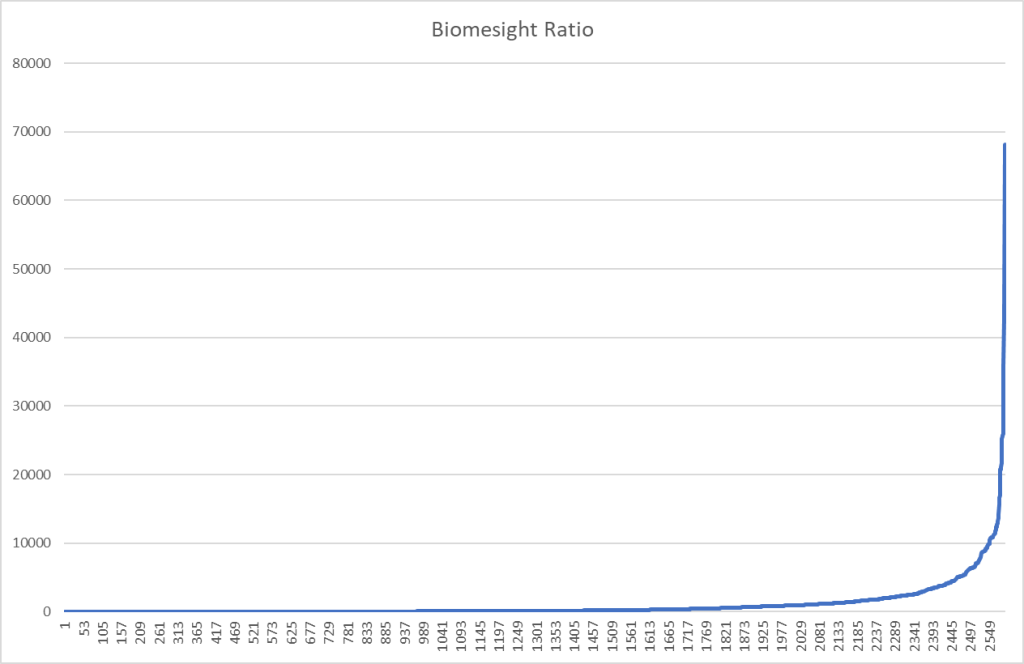
BiomeSight Ratios
Bottom Line
I would suggest a ratio > 500 to 1000 is High, Below 200 is low
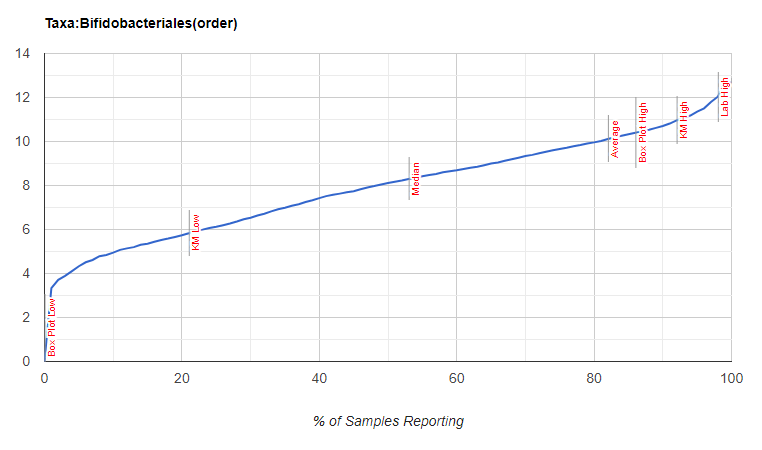
The following is based on Biomesight data uploaded with some annotated by uploaders. Technically, interpretation of microbiome results should factor these issues in. At least 10 samples had to have Symptom Name to be included. The numbers shown are averages (on count per million) on samples that reported the bacteria.
As a spot check, we see multiple Bifidobacterium in the 0-10 range which agrees with the literature.
In general, the symptom has more than the population because we filtered by using a high T Score to keep the list shorter for illustration purposes. A variety of other factors are not shown, for example: FUT2 non-secretor or FUT2 secretor.
Dropping the T-Score filtering to 1.96 resulted in 3600 rows.
I wanted to share some good news with you. In the last 3 weeks I’ve noticed my time going to the bathroom has decreased in half and my gut has been less irritable. Over the last 2 weeks, my mood has steadily improved and I’ve enjoyed more energy than usual. It appears that your guidance has pointed me in the right direction!
Note: I didn’t end up performing the FMT.
I thought about why my Firmicutes would get to 97%+. It’s most likely because the majority of the foods I eat are continually pushing my gut towards Firmicutes. And it could also explain why after adding 5+ daily supplements to push my gut the other direction, it hasn’t worked. You noted that my being a vegetarian may be acting as a significant counter balance to the direction we’re trying to go.
Besides adding a small amount of meat in the morning, I cut out the foods I eat most frequently. Bananas, raspberries, blueberries, nut bars. And then I added in the Seaweed you recommended. I think the seaweed has made a massive difference and with all these changes implemented collectively, the boat has begun to turn around! I’m hoping this continues
Backstory
I’m 39 and have suffered from moderate CFS since i was an early teenager. My major 3 symptoms are low energy, brain fog, and IBS. My CFS didn’t affect me as much when I was 18, but combined with the effects of aging, I’ve been feeling the fatigue more impactfully the last two years.
Journey over last 10 months
When I first began working on this in January, my samples showed my Firmicutes at 98%. That seemed to be the smoking gun as you described it, and I was eager to begin shifting my microbiome. Over the next 6 weeks I felt markedly better but unfortunately I now believe that was merely a placebo effect. Once I started to believe the benefits I had received were from a placebo, I rapidly returned to baseline. Over this time period, I cut out many of the foods that pushed my gut in the wrong direction, and I was taking 4 supplements 2-3x a day. By my second test 2 mos later, my firmicutes adjusted downwards from 98% to 93%. In terms of how I felt, it was difficult to assess whether it was better than my baseline. I was hopeful that it was, but I couldn’t say for sure.
Over the last 6 mos my Firmicutes has reduced from 93% to 89%. During this time period I continued to cut out foods that were counter-recommended. I ordered 4 more vitamins & supplements that were in my consensus list, and I was taking 4 supplements 1X/ day, while also rotating the supplements every 4 weeks to prevent resistance.
Once again, it’s difficult to assess now how i feel versus my baseline. I don’t feel significantly better, that I know. And while I’m disappointed my sample isn’t improving drastically, the upshot from my perspective is that at least my sample results match how i’ve been feeling.
Reader Addendum After reading
“I’m mostly vegetarian… which may help to explain why after 9 months of supplements I’m partially moving in the wrong direction. I’ll incorporate the seaweed and increase my red meat.”
Analysis
We have three samples to compare.
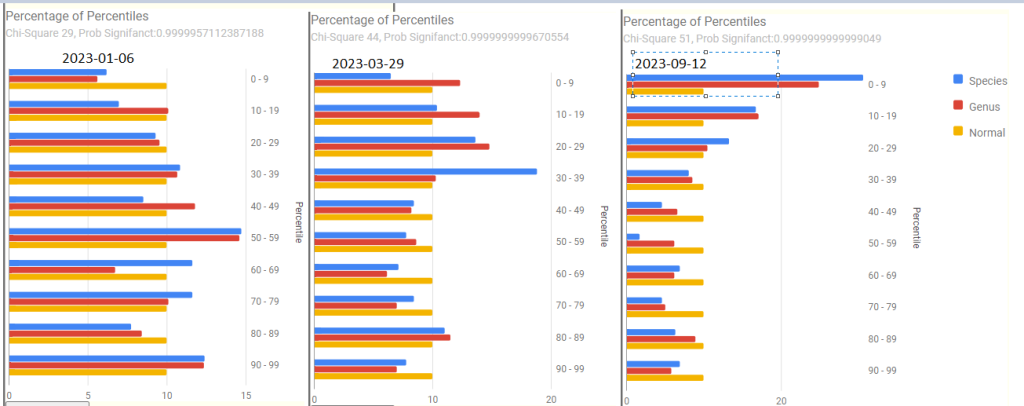
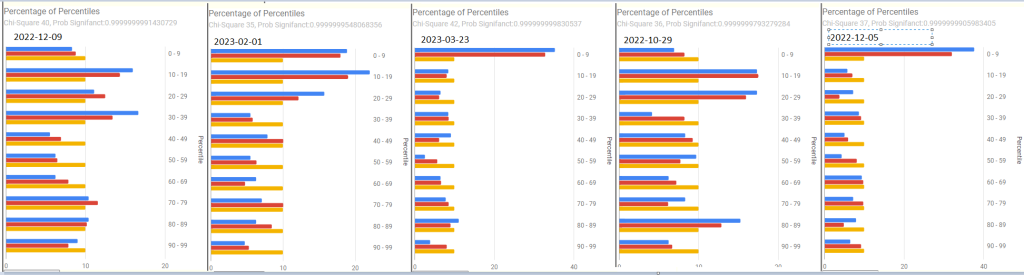
Percentage of Percentiles
We see significant shifts between samples with chi2 values increasing (meaning more abnormal) instead of decreasing. What is interesting is that the two earlier samples does not the typical ME/CFS or Long COVID pattern, but the third sample shifted to the pattern of spikes in the 0-9%ile range. This is open to many interpretations; some good and some concerning.
Evaluation Criteria
The numbers below are mixed, some showing improvement, others showing loss.
Criteria
1/6/2023
3/29/2023
9/12/2023
Lab Read Quality
4.3
5.9
8.7
Outside Range from JasonH
3
3
6
Outside Range from Medivere
18
18
20
Outside Range from Metagenomics
8
8
7
Outside Range from MyBioma
9
9
15
Outside Range from Nirvana/CosmosId
23
23
24
Outside Range from XenoGene
38
38
43
Outside Lab Range (+/- 1.96SD)
18
15
10
Outside Box-Plot-Whiskers
54
53
56
Outside Kaltoft-Møldrup
85
125
181
Bacteria Reported By Lab
431
553
591
Bacteria Over 90%ile
49
32
34
Bacteria Under 10%ile
43
72
174
Shannon Diversity Index
2.852
2.937
2.49
Simpson Diversity Index
0.083
0.098
0.101
Chao1 Index
8592
11807
15969
Pathogens
26
35
40
Condition Est. Over 90%ile
11
7
2
Kegg Compounds Low
821
731
1190
Kegg Compounds High
134
251
99
Kegg Enzymes Low
359
204
259
Kegg Enzymes High
208
311
243
Kegg Products Low
201
124
170
Kegg Products High
130
199
158
Kegg Substrates Low
195
114
156
Kegg Substrates High
149
216
162
Forecast symptoms
The top 3 forecasted items are below. See this post: Post Exertional Malaise (PEM) with diminished ME/CFS for more information on forecast symptoms in use. The earliest sample had no forecasts being reliable (i.e. > 60% match). What we also see in that the symptom patterns are becoming stronger. Again, this is usually not desired.
2023-01-06
54.3 % match for Neurological-Vision: Blurred Vision on 35 taxa
52.4 % match for General: Headaches on 42 taxa
50 % match for Immune Manifestations: new food sensitivities on 56 taxa
2023-03-29
65.9 % match for Pain: Pain or aching in muscles on 44 taxa
56.2 % match for Immune Manifestations: Diarrhea on 89 taxa
56 % match for Neurocognitive: Brain Fog on 50 taxa
2023-09-12
65.7 % match for Neurocognitive: Difficulty paying attention for a long period of time on 70 taxa
62.3 % match for Neurocognitive: Can only focus on one thing at a time on 53 taxa
61 % match for Neurological-Vision: Blurred Vision on 41 taxa
Impression and Possible Model
This is the first follow up sample where there was neither clear objective or subject improvement. What we see clearly above was that the microbiome has changed. Subjectively, there was no deterioration reported.
Objectively it seems that the microbiome has been de-noised. This person has had ME/CFS for 20+ years and thus the microbiome dysfunction will evolve. His latest sample changed to the typical pattern for ME/CFS for percentage/percentile chart above. The forecasted symptoms values are increasing for what are likely correct forecasts. The bacteria associated with ME/CFS and IBS are showing themselves better and other bacteria causing noise are diminished.
Going Forward
I first looked at the US National Library of Medicine studies for bacteria reported for the conditions he reported.
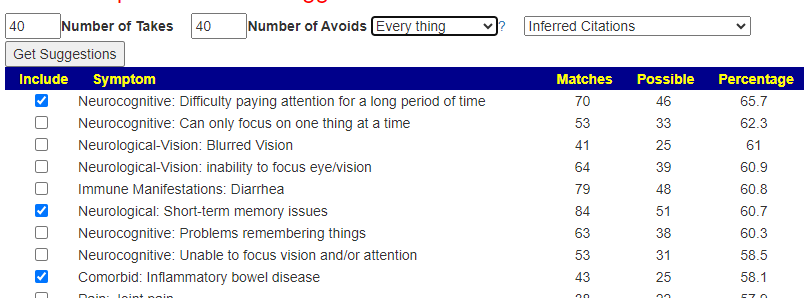
Symptom matching on these is a clear miss. I did note some high matches that are typical symtpoms so I add in the results from these selections:
The result was just 84 unique taxa and we have 5 sets of suggestions in our consensus.
So we fall back to the “Just give me suggestions”. The high priority value was 300 and the low priority value was -405. Adding in special studies suggestions moderated the ranges but most items stayed the same.
Antibiotics: There was only 1 over the 150 (300/2) threshold. None are associated/studied with his conditions so I would pass one them. This antibiotic is usually used for tuberculosis.
It looks the a modified Surf And Turf diet, i.e. Steak and Seaweed (our local Costco does sell a nice seaweed salad that is a regular for me)
The AVOIDS
The avoid values are so high compared to the takes that we need to review them to try reducing or excluding them. The threshold value is -300 (-600/2).
This has been a challenging set of samples to do an analysis on. I have often used the analogy of going from the port of sickness to the port of health in a sailing ship along a rugged coast. There may be a long series of course corrections needed.
The suggests above are very atypical. Given that there appear to be a lot of noise in his microbiome, we may have some more denoising to do (bring out more the ME/CFS and IBS bacteria into the light). I would advocate attempting to get a course of rifaximin. It has been well used for his IBS diagnosis so there should be little push back from his MD.
Questions and Answers
Q: I’ve read through my new Simplified Suggestions List, and The suggestions of what I need to take and avoid are the same as before…. but the impact score of each was adjusted. Although you’ve noted in the past that a higher impact doesn’t indicate it works more effectively, it looks from your suggestions that you stick to the highest impact items as there are the most studies to support them, right?
Correct. One study may report honey increases a bacteria, and another study report that it decreases the same bacteria. To determine the confidence of a suggestion we look at all reports. If you have 10 honey studies (8 increases and 2 decreases) and one study alone for roasted whale increasing the bacteria; most people will have greater confidence that honey is a better choice to try.
Q: One initial inquiry comes to mind- for complex cases, have you given any additional consideration to (probiotic) enemas as a way to make a big impact, and then to adjust with oral supplements from there?
I work from published clinical studies and not from influencers opinion. There is a good summary on WebMD, What to know about probiotic enemas that gives pros and cons.
Using commercial/retail probiotics have two significant risks:
Very often the declared species is not what is in the bottle, the exception is for those strains that are owned by someone.
Often they contain fillers that will be well consumed before they reaches the nether regions. These fillers being inserted here may give a feast to some bacteria that usually do not get much, sparking an unexpected overgrowth.
Q: Below are the supplements I’ve been taking each day. My plan is to cut out everything that doesn’t have an impact score north of a 150. Does that sound like a reasonable approach?
ground flaxseed. I took this every day for 4 months and had to stop because it began to make me nauseous. — Try it again at low dosages after one month
Luteolin – low positive
carboxymethyl cellulose — definite take
Dietary Fiber Cellulose – definite take
partially Hydrolyzed Guar Gum (SunFiber) — remove
licorice root —remove
Vit B1, B6, B7 — low positive
Gaba — definite take
Vit C — remove
Melatonin — low positive, suggest you try removing for a week then trying for a week to see if it still help sleep
Diosmin – low positive
Astragalus – low positive
Answer: The logic is good but I would restrict to only items that are negative. You may wish to revisit the reason that you started each; if it was symptom related and improved — then monitor that symptom and return it if the symptom returns. I have annotated the list above
Reflection
Suggestions could also be described as influencers. There is no need to get religious about taking everything. Take what you are comfortable with is my usual advice. In this case, the person being a vegetarian may have significantly counter-indicated the other influencers. Once the microbiome is normalize, a return to be a vegetarian is viable.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
This is from a person that have been using Microbiome Prescription for a while with significant success. He messaged me about a new sample and asked me to take a look. It was good timing because I have over the last week refactor forecast symptoms as well as allowing them to be used to generate suggestions. This gave me an opportunity to test the analysis and suggestions.
My impression is that they are both working well with better sensitivity than the older method. Prior posts include:
-PEM -Fatigue on and off specially in the morning. Lowest energy point -Some brain fog. If I take a binder my brain fog is much better. Guessing that could be related to mold/fungus issues? -unrefreshing sleep -hair shedding unless I take Lactoferrin -difficulty losing weight
– Reader
Review of Test Results
I am skipping the sample comparison table because the forecast symptoms seem more useful for between samples comparisons.
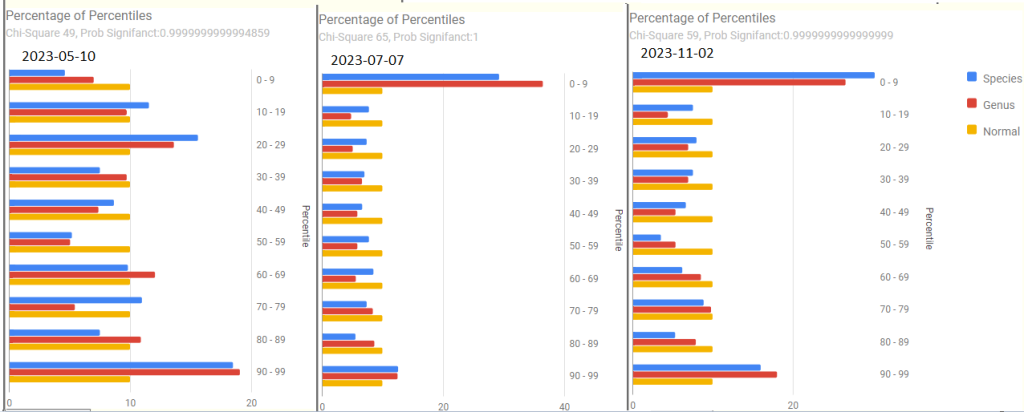
Percentages of Percentiles
These are helpful overview to see if there are problems. At the top is a chi2 value which a healthy person should have a value below 0.90 . All of his values were .99999…. indicating abnormal shifts.
Prior to 2023
2023, the impact of COVID in the latest sample is quite apparent.
Forecast Symptoms
What shocked (and delighted) me was how accurate the forecasts were, especially with the main issue, PEM being near the top on every sample. The percentage match ebbed and flowed with improvements and set backs (typically from COVID).
2023-11-02 – After recent COVID
74.2 % match for Neurological: Cognitive/Sensory Overload on 31 taxa
63.5 % match for Immune Manifestations: new food sensitivities on 52 taxa
61.5 % match for Neuroendocrine Manifestations: cold extremities on 65 taxa
60.9 % match for Neurological-Vision: Blurred Vision on 87 taxa
59.6 % match for Condition: ME/CFS with IBS on 52 taxa
58.3 % match for Post-exertional malaise: Worsening of symptoms after mild physical activity on 36 taxa
2023-07-07
57.1 % match for Post-exertional malaise: Worsening of symptoms after mild physical activity on 42 taxa
54.2 % match for Condition: ME/CFS with IBS on 59 taxa
48.1 % match for Post-exertional malaise: Post-exertional malaise on 54 taxa
2023-05-10
63.2 % match for Post-exertional malaise: Post-exertional malaise on 38 taxa
59.3 % match for Post-exertional malaise: Muscle fatigue after mild physical activity on 59 taxa
59.1 % match for Pain: Pain or aching in muscles on 44 taxa
57.1 % match for Condition: ME/CFS with IBS on 42 taxa
2022-12-05
82.4 % match for Official Diagnosis: Autoimmune Disease on 51 taxa
81.9 % match for Comorbid: Histamine or Mast Cell issues on 83 taxa
79.5 % match for Post-exertional malaise: Next-day soreness after everyday activities on 39 taxa
71.8 % match for Post-exertional malaise: Physically tired after minimum exercise on 39 taxa
2022-10-29
64.4 % match for Neurological-Sleep: Inability for deep (delta) sleep on 45 taxa
62.7 % match for Official Diagnosis: Mast Cell Dysfunction on 75 taxa
60.9 % match for Post-exertional malaise: Next-day soreness after everyday activities on 46 taxa
60 % match for Condition: ME/CFS with IBS on 40 taxa
55 % match for Post-exertional malaise: Muscle fatigue after mild physical activity on 60 taxa
54.5 % match for Post-exertional malaise: Post-exertional malaise on 44 taxa
2022-03-23
85.4 % match for Neurological-Sleep: Inability for deep (delta) sleep on 41 taxa
82.1 % match for Immune Manifestations: Inflammation (General) on 67 taxa
77.5 % match for Immune Manifestations: Inflammation of skin, eyes or joints on 111 taxa
75 % match for Post-exertional malaise: Worsening of symptoms after mild physical activity on 32 taxa
71.4 % match for Post-exertional malaise: Next-day soreness after everyday activities on 42 taxa
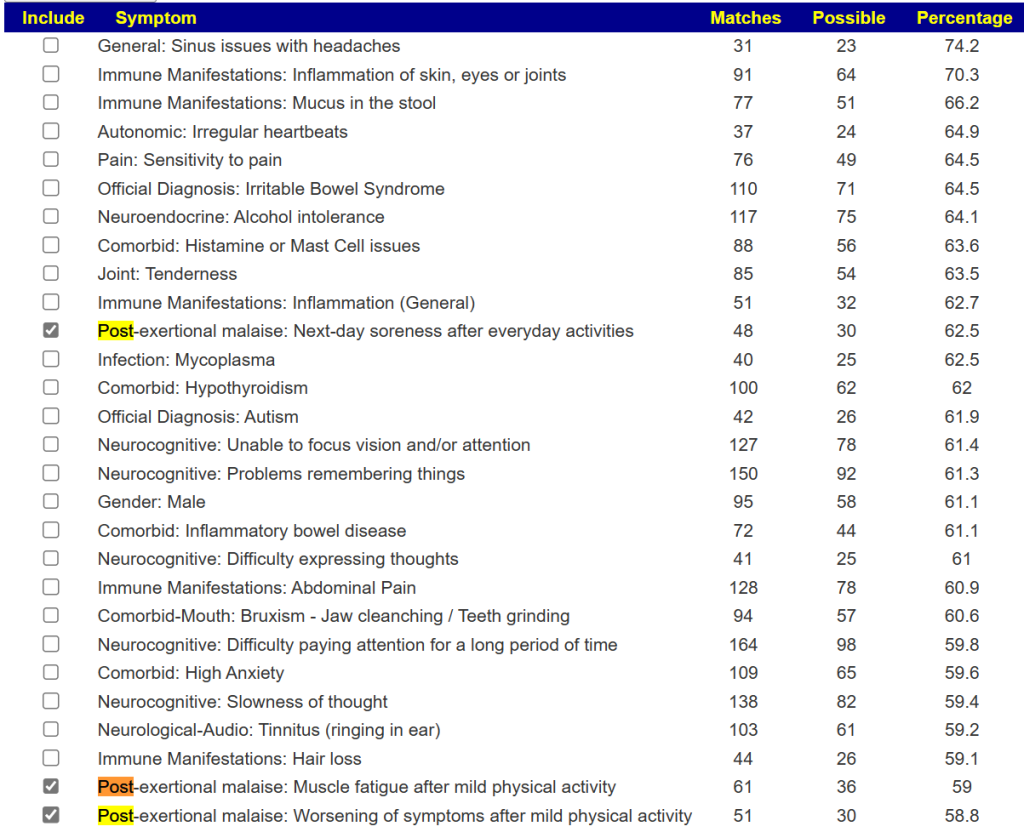
Drilling down on PEM
With the revised symptom-taxa association tool, I went to the 2022-12-05 sample because it had very high values for PEM in forecasting. I then went to [Special Studies] and selected all of the PEM items
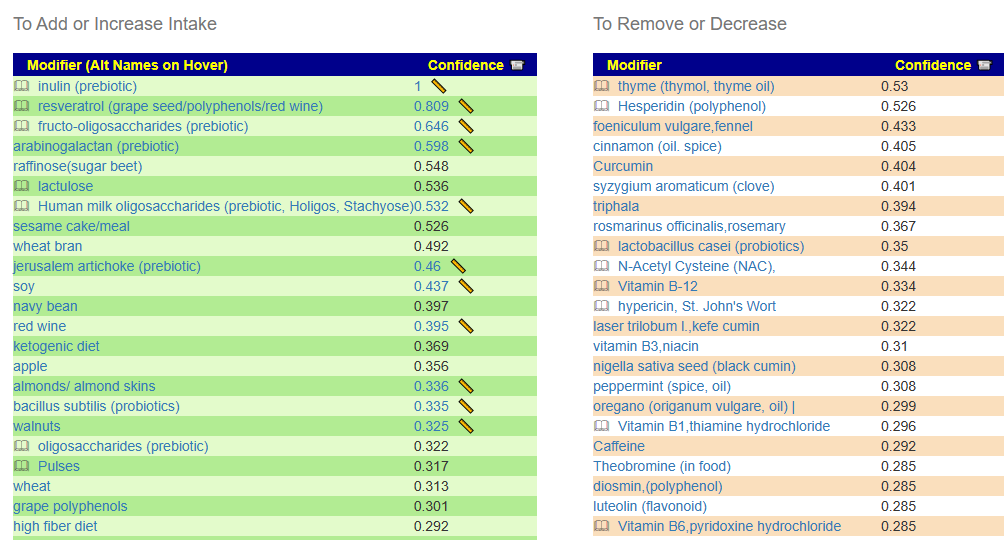
Some 78 bacteria were selected with the following being the top suggestions:
While this is not his current sample, it is reasonable guidance for dealing with the bacteria associated with PEM.
Going Forward
I am going to do [Just give me suggestions] and then special studies selecting only PEM items that are shown. We thus ended up with 5 packages. Looking at the details we have high at 555 -> 277 for high threshold and -542 –> -271 for low threshold
In general, it looks very pro-forma ME/CFS. He may wish to check the PEM suggestions against the details and include anything that is positive.
Bottom Line
I have often used the analogy of going from the port of sickness to the port of health in a sailing ship along a rugged coast. There may be a long series of course corrections needed. While there are still ME/CFS taxa shifts seen in his samples, subjectively the only symptom left of concern is a PEM after playing basketball for a while.
This is a good illustration that taxa/bacteria does not rule — DNA and other factors are involved with symptoms and the ability to tolerate microbiome dysfunctions.
Questions and Answers
Q: I may do another Thorne test if they’re back in stock. Wondering how much aspergillus is holding back healing/gut shifts
Aspergillus usually impacts lungs and breathing [CDC] (thus ability to get oxygen in). An alternative mechanism for oxygen issues than with hypercoagulation.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
The following are bacteria that have very unusual statistical behaviors in uploaded samples. This hints that they may be connected to some disease or symptom state.
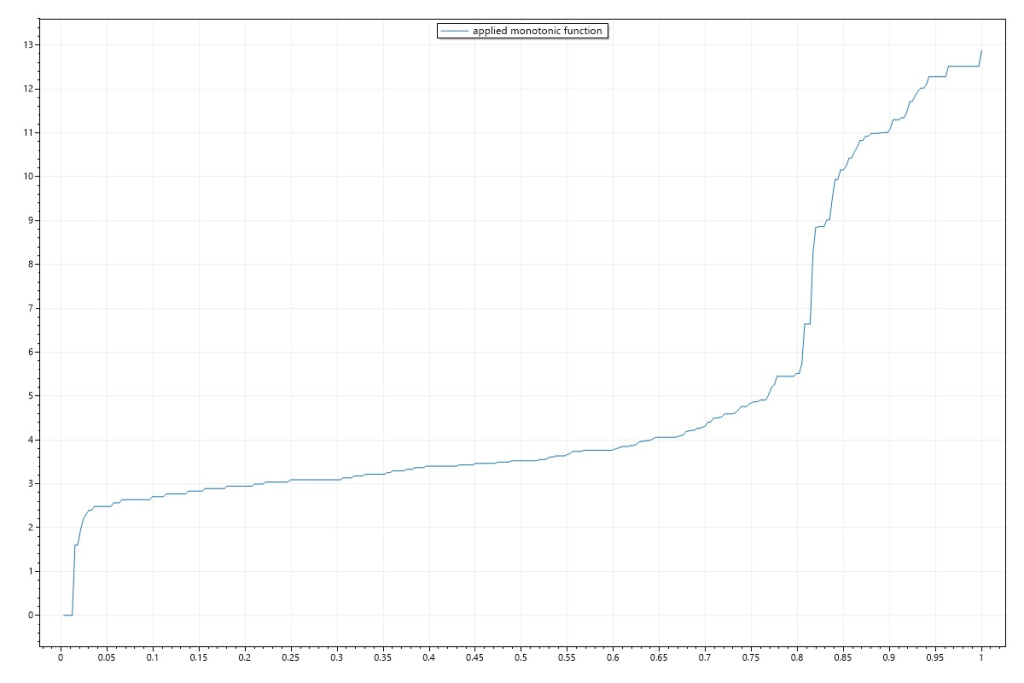
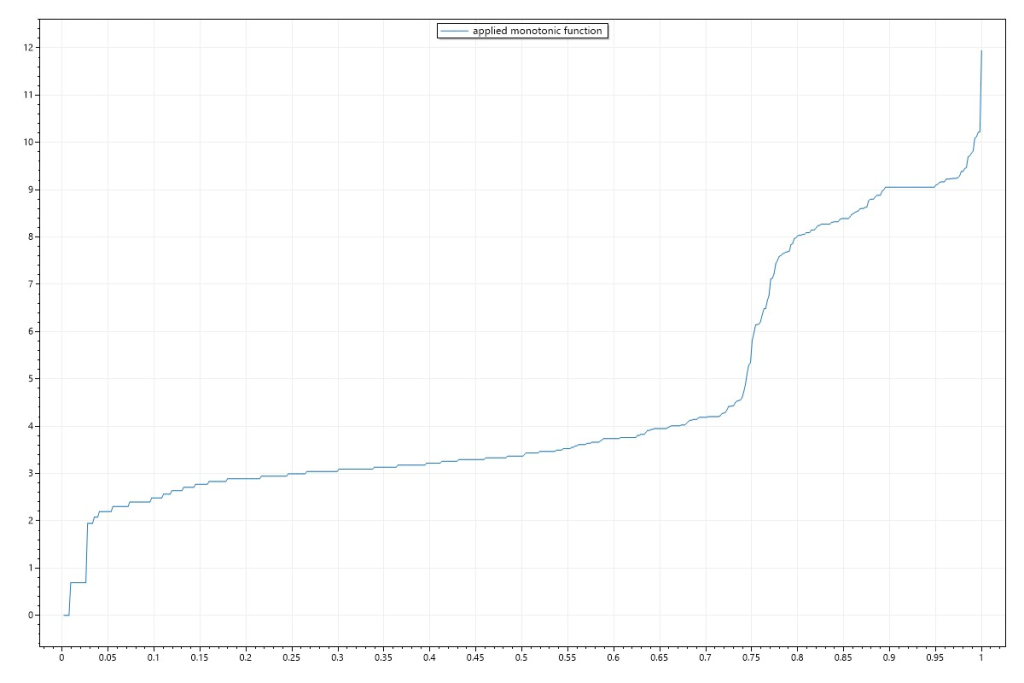
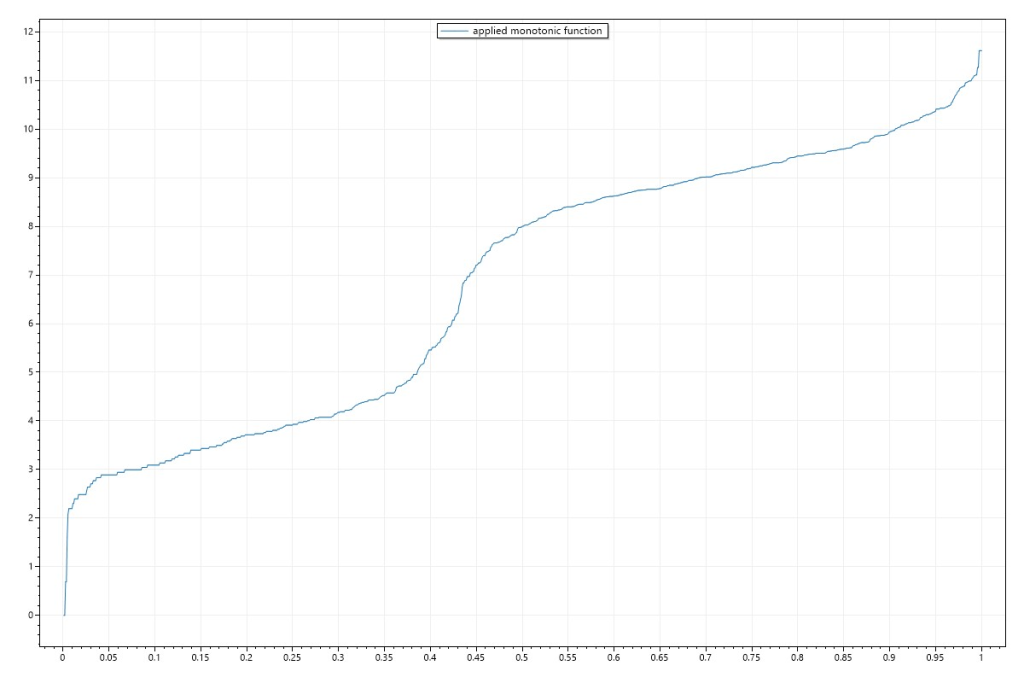
The common pattern seen with most bacteria is shown below. You can view each bacteria pattern by clicking on the chart icon after searching for a bacteria on https://microbiomeprescription.com/Library/Lookup
Preliminary evaluations have shown strong and accurate forecasting ability. I am working with a Ph.D. in Molecular Genetics and processing his microbiome sample the top forecasts were correct:
He was a male
He had no Health Issues
He was blood type O-positive
He snored
He woke up early
This was not from a blood sample, but from a stool sample. The methodology is described in my earlier posts.
The methodology is computing intensive. Unlike many contemporary artificial intelligence engines, it is easy to understand:
In the entire population(n:10,000), a bacteria like unclassified Clostridiales has 10% of samples reported this bacteria with a mean of 0.3%.
In the condition / sample population(n:1000) we find that 30% of the samples reported this bacteria with a mean of 4.8%
I used Chi2 to determine significance because significance using means assumes a normal distribution which is a false assumption.
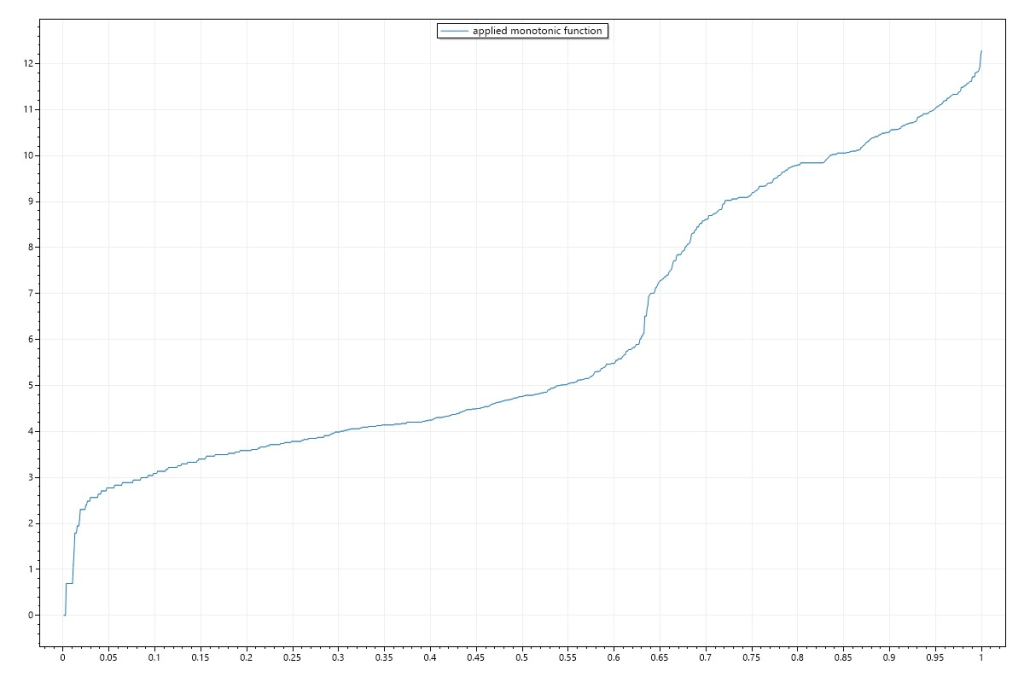
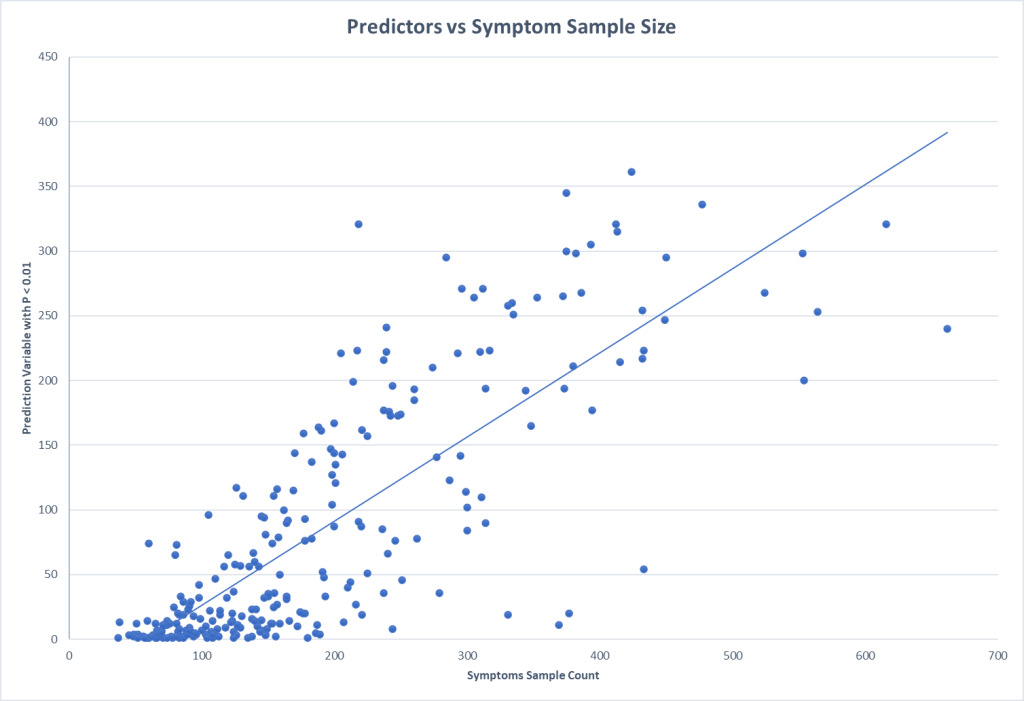
With this methodology it is good to get some indication of what sample sizes for conditions / symptoms is needed (assuming the control is at least the same size). A quick plot informs us that 200 looks like a minimum size with 300+ being desired.
One of the labs that I work with reports percentile ranking on their reports. This makes doing an exploration economical (i.e. cheap). Testing of the symptom/condition group is only needed because the control numbers are gifted you.
This also illustrates that the symptom is not with just one taxa, but the influence of many taxa working in unison to influence the symptom (or be influenced by the condition).
Samples of Symptoms / Conditions
The ones with the most predictors are below.
Neurocognitive: Absent-mindedness or forgetfulness
Neurological: Impairment of concentration
Neurocognitive: Difficulty paying attention for a long period of time
Only two were significant and we have the importance of sample size apparent.
Symptom Name
Sample N
Forecast Variables
Blood Type: O Positive
284
295
Blood Type: A Positive
126
3
For Age:
Symptom Name
Sample N
Forecast Variables
Age: 60-70
206
143
Age: 0-10
98
42
Age: 50-60
164
33
Age: 20-30
152
12
Age: 30-40
369
11
Age: 40-50
244
8
For Gender
Symptom Name
Sample N
Forecast Variable
Gender: Female
415
214
Gender: Male
554
200
Bottom Line
From the individual forecast variables, we can compute odds of a match. Consider a simplistic example of three factors
Factor A uses 5%ile
Factor B uses 10%ile
Factor C uses 20%ile
With A,B,C all being true has a 99% chance of being a taxa match (1 – .05 * .1 * .2). This does not mean the person has it, it indicate a significant risk of having it (depending on other factors, DNA, age, gender etc).
Of course, the more forecasting variables, the better the estimate becomes and also the more tolerant the forecast is to variations in the microbiome.
Fungi and the microbiome finally got on my radar. Apologies to some, but there is a lot of different items on the microbiome radar screen.
“Small intestinal fungal overgrowth (SIFO)… Two recent studies showed that 26 % (24/94) and 25.3 % (38/150) of a series of patients with unexplained GI symptoms had SIFO. …. but evidence for eradication is lacking.”Small intestinal fungal overgrowth [2015]
As I did with taxa years ago, I will be writing a blog on each one reviewing the literature. If there is sufficient data at the end, I may add it as a feature to Microbiome Prescription.
One of my reader’s results motivated this choice. The data from a Thorne Microbiome Test. Almost 9 out of 10 people have less of it. The person also has a Crohn’s diagnosis.
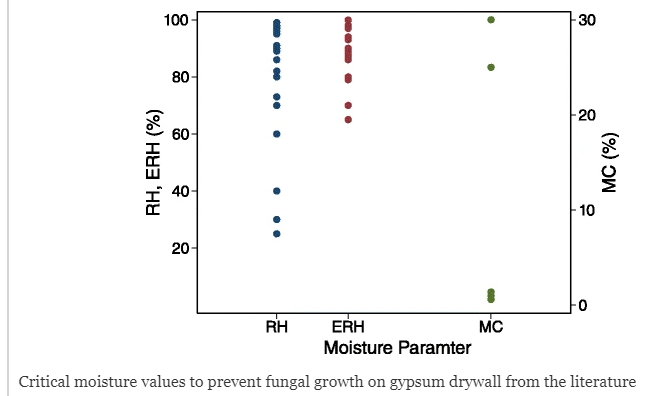
Preventive for Fungi
The following are suggestions:
Reduce and keep your living space humidity at 50% or lower (typically done by dehumidifiers). EPA recommends 30-50% [EPA]; we set our dehumidifiers for 35%.
Fungi and the microbiome finally got on my radar. Apologies to some, but there is a lot of different items on the microbiome radar screen.
“Small intestinal fungal overgrowth (SIFO)… Two recent studies showed that 26 % (24/94) and 25.3 % (38/150) of a series of patients with unexplained GI symptoms had SIFO. …. but evidence for eradication is lacking.”
As I did with taxa years ago, I will be writing a blog on each one reviewing the literature. If there is sufficient data at the end, I may add it as a feature to Microbiome Prescription.
One of my reader’s results motivated this choice. The data from a Thorne Microbiome Test. 9 out of 10 has less of it. The person also has a Crohn’s diagnosis.
Reduce and keep your living space humidity at 50% or lower (typically done by dehumidifiers). EPA recommends 30-50% [EPA]; we set our dehumidifiers for 35%.
Fungi and the microbiome finally got on my radar. Apologies to some, but there is a lot of different items on the microbiome radar screen.
“Small intestinal fungal overgrowth (SIFO)… Two recent studies showed that 26 % (24/94) and 25.3 % (38/150) of a series of patients with unexplained GI symptoms had SIFO. …. but evidence for eradication is lacking.”Small intestinal fungal overgrowth [2015]
As I did with taxa years ago, I will be writing a blog on each one reviewing the literature. If there is sufficient data at the end, I may add it as a feature to Microbiome Prescription.
One of my reader’s results motivated this choice. The data from a Thorne Microbiome Test. Almost 9 out of 10 people have less of it. The person also has a Crohn’s diagnosis.
Preventive for Fungi
The following are suggestions:
Reduce and keep your living space humidity at 50% or lower (typically done by dehumidifiers). EPA recommends 30-50% [EPA]; we set our dehumidifiers for 35%.
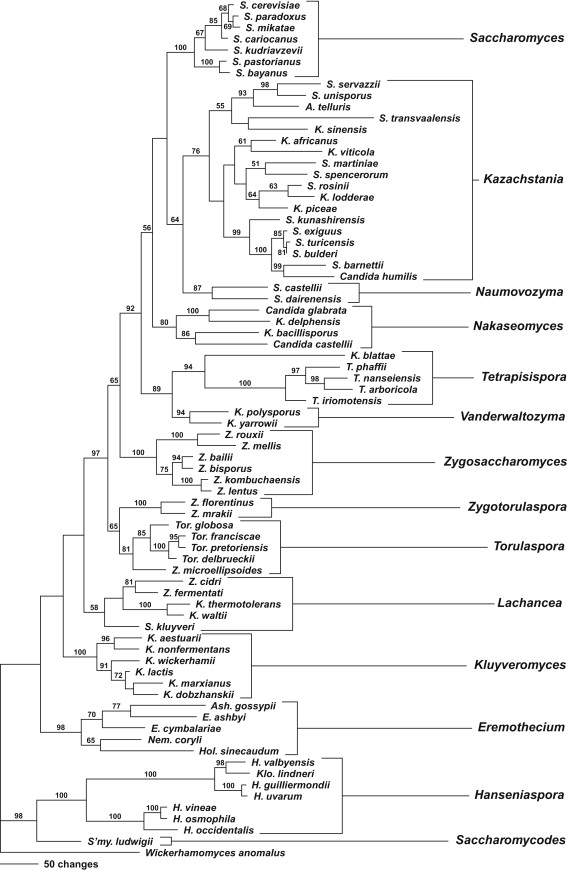
“Basidiomycota is the second most species‐rich phylum of Fungi with nearly 32,000 described species” [2019]
Members of the Trichosporonaceae show a global distribution and have been recovered from a wide range of environments. Cutaneotrichosporon spp. are most frequently associated with a human host, and may represent opportunistic human pathogens. Trichosporon spp. form part of the natural microflora on human and animal skin and result in a non-serious mycosis of hair termed white piedra3. However, they have also been implicated in trichosporonosis, a collection of opportunistic infections caused by a number of species, including Trichosporon asahii, T. asteroides and T. ovoide
“Invasive Trichosporon infections are common in immunosuppressed patients, such as those with hematological malignancies. Unfortunately, invasive trichosporonosis can be difficult to diagnose and treat, and the global incidence is increasing”
“In cases of central nervous system infection, the predominant symptoms are headache, nausea, vomiting, and fever.”
“Trichosporonosis has also been documented to cause peritonitis, pacemaker lead endocarditis, and pneumonia. Other rare manifestations include sinusitis in an immunocompetent patient, fungemia, and urinary tract infection in patients with diabetes mellitus, and nosocomial infection in patients with severe burns”








Recent Comments