During the questions period of Jadin’s presentation: Dr. Jadin’s Current Protocol for ME/CFS; Questions were asked about her treatment in terms of it’s target and what microbiome prescription does. I thought a blog post may help people understand how microbiome prescription side-steps a Pandora box of theories.
A simple Premise: Fix the microbiome and symptoms will improve!
In Dr. Jadin’s presentation, she identifies a host of causes that could result in ME/CFS and similar conditions. For example Giardia — IBS/CFS/Long Covid Insight from Bergen’s Giardia Infection, Lyme, or my post from 2016, Post Infection Fatigue, virus: HHV6, EBV and of recent note: COVID. The question arises: Is the source still there? The pragmatic answer is likely yes, at low but significant levels (i.e. maintenance levels).
Not only is it there, but there is likely a half dozen low level infections associated with ME/CFS. WHY? When the microbiome goes off, the immune system follows it. Virus reactivation happens because the immune system is not firing on all cylinders. For example, your body may keep fungus well controlled in your living environment before; now you have fungi problems added to the mix.
Chasing Symptoms Trap
Often people will be focused on one symptom or lab result. For example: How do I reduce my methane levels, How do I reduce my Interleukin 6 levels, how do I get rid of brain fog, etc etc etc.
I do not have the answers for those questions, nor do I care. I review the body as a very complex dynamic organism with a great amount of interactions. My sole target is the microbiome and that is a big target — over 18000 different bacteria are reported from retail microbiome tests, 8,000+ different enzymes, 18,000 different compounds.
Let us take just one ME/CFS associated item: Epstein-Barr virus. Some of the interactions and interplays are shown in the chart below (See KEGG for full chart). So, you are wanting a single magic supplement?
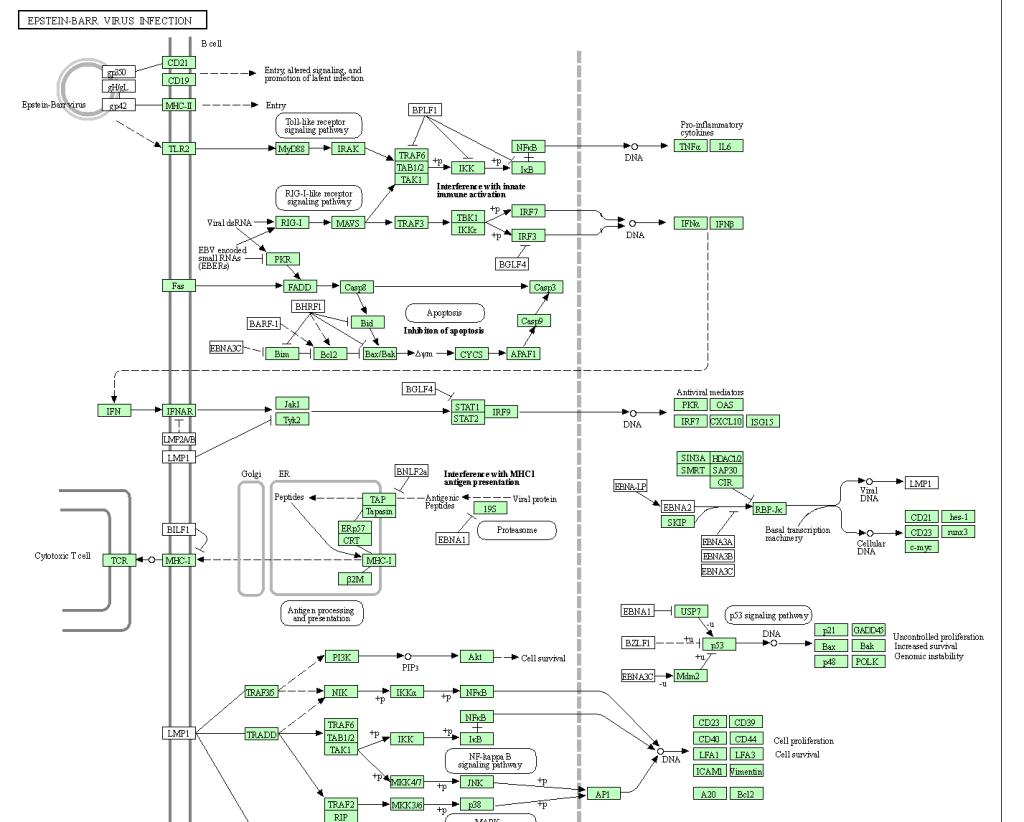
My goal is very simple, normalize the microbiome and thus normalize the immune system and the levels of the 26,000+ substances involved. Then, and only then, will issues of substance appear (if any).
No matter what the infection (virus, fungi, bacteria) – they need “food”
Where does the food come from? The microbiome. Correcting the microbiome should starve the bad guys and feed the good guys is the simple concept. All of these infections are known to alter the microbiome — and we can reasonably assume that it is done to make the human body more friendly to the infection.
Now with 18,000 bacteria and 26,000 substances, no person can either read nor keep all of the available data in their brain. I happen to have the skill sets to encode much of the data and build a fuzzy logic expert system around the data – that’s my skill set.
Why does my recommendations often matches Jadin’s protocol?
If we assume the infection is still there, we likely have a strong association between the infection and the microbiome bacteria. What encourages the infection, likely also encourages a subset of microbiome bacteria; and the reverse. The microbiome may just be a proxy for the infection with the odd-characteristic that we may be able to determine effective antibiotics without needing to identify all of the infections present. The infection and the microbiome in one sense are mirrors of each other.
This is the philosophical basis that I am working from. As with best modelling practices, if a model predicts and the predictions are correct, you keep to the model (even if it is full of orcs and hobbits) until it breaks — then you work on building a better model.
The microbiome may be a sufficient proxy for the co-infections involved with ME/CFS.
It is easier, faster and cheaper to test – especially because it is available at a low cost, direct to consumers.
Recent Comments