After a good night sleep after doing the video below, I realized the next step in this journey. With hundreds of bacteria in the microbiome the question arises which ones to focus on if the condition is not a known single bacteria condition. I.e. Crohn’s, Asthma vs Tuberculosis, Ulcers.
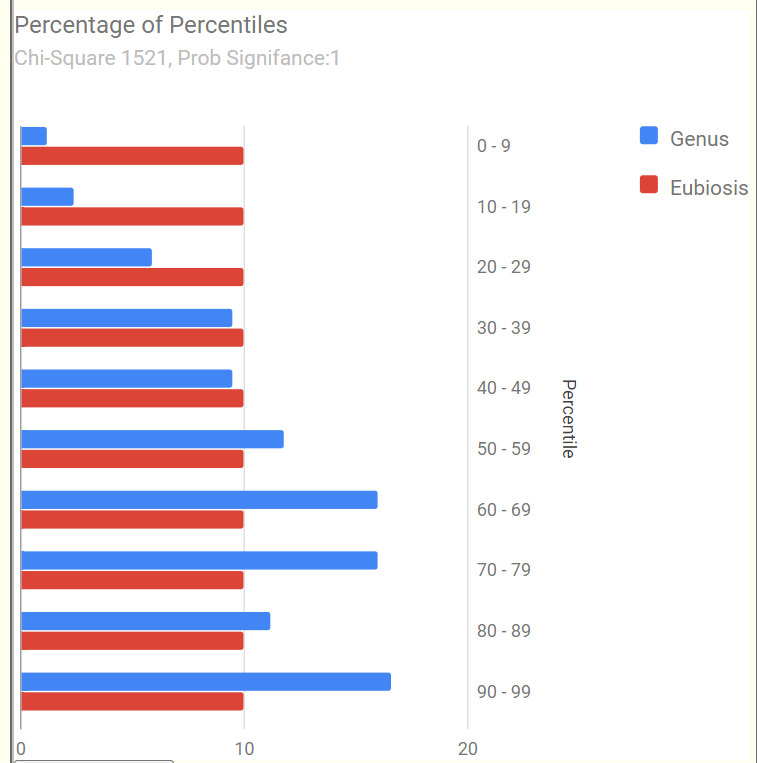
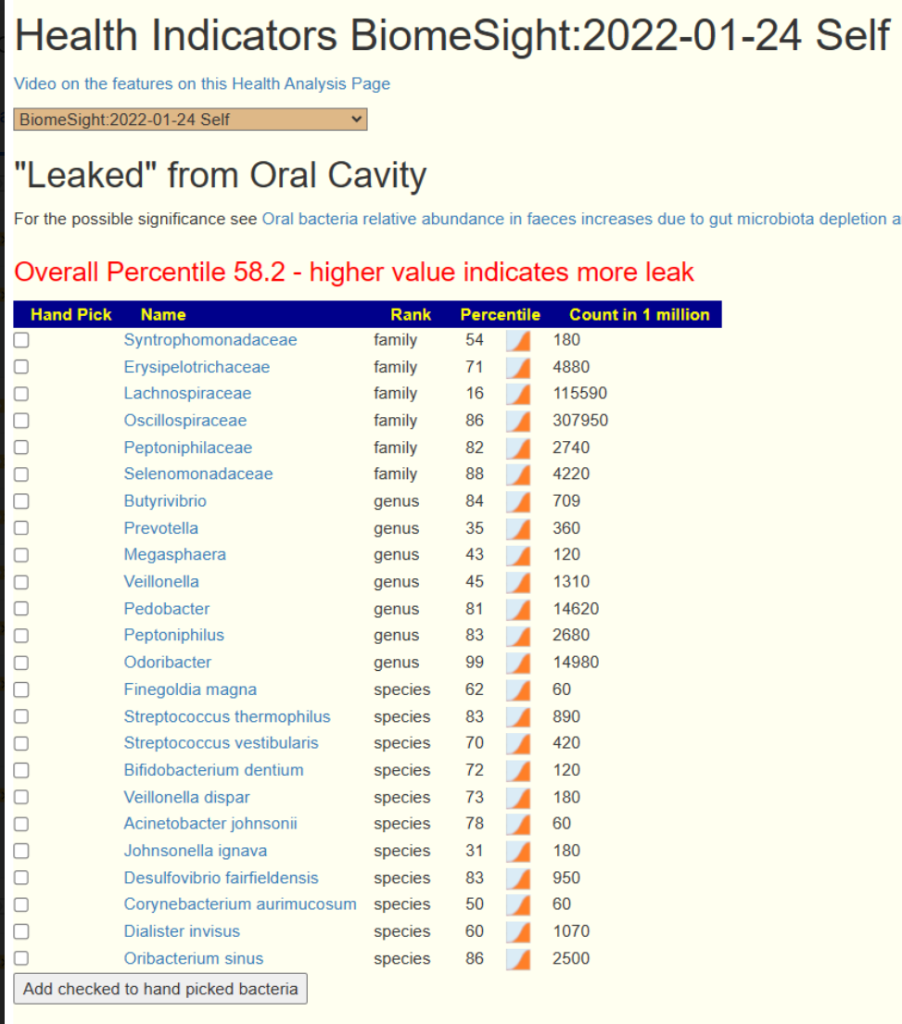
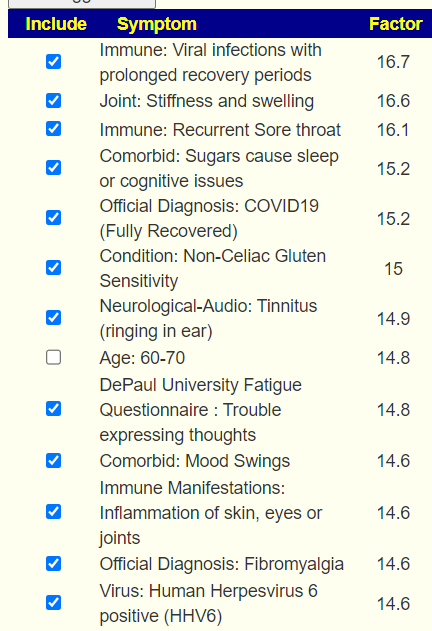
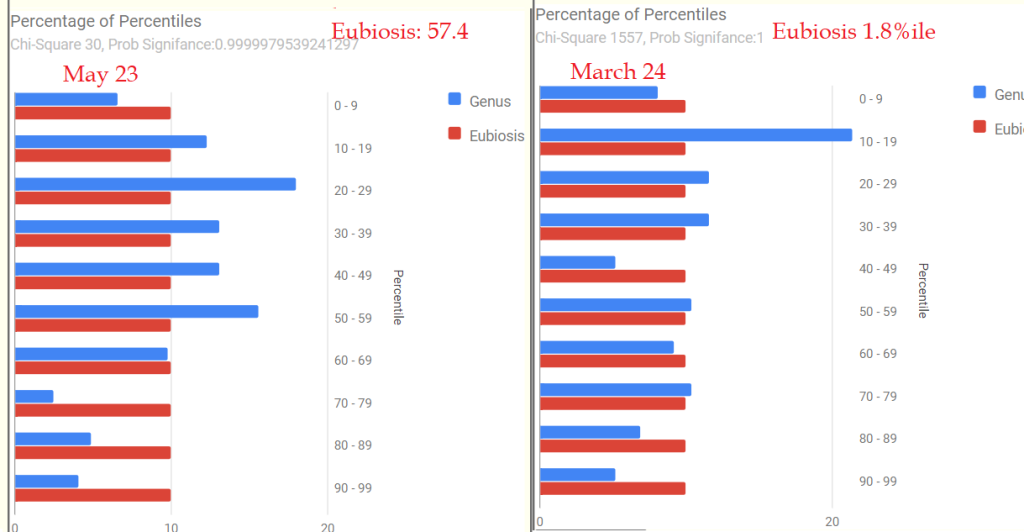
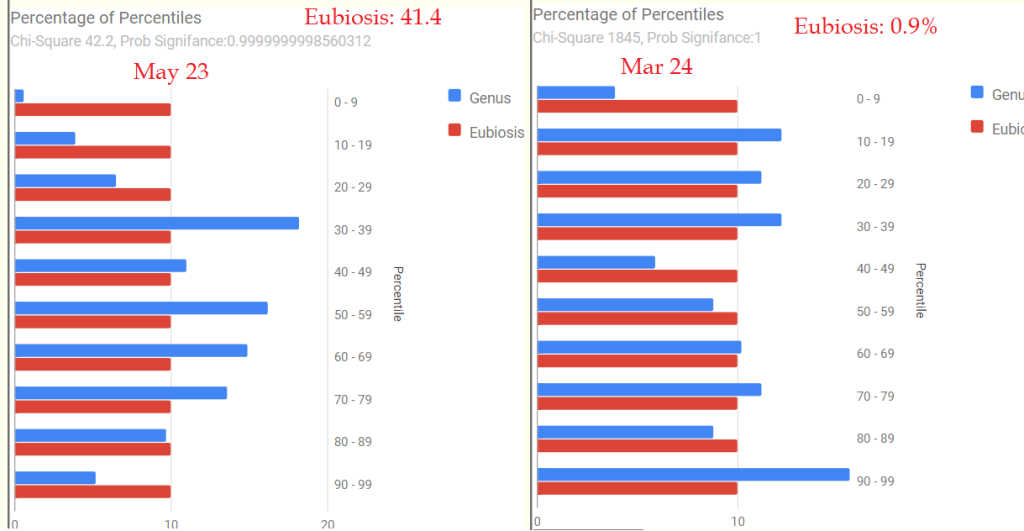
Recently I had major success is identifying bacteria associated to hundreds of symptoms. This was done by using the percentile ranking of each microbiome sample over the population and then examining the counts of the top and bottom 15%ile (simplified version). These should be equal if there is no relationship of the bacteria to the symptom. The difference allows a Chi2 value and probability to be computed for significance. Comparing the averages perform very poorly for finding equivalent statistical significance.
The result was a list of bacteria where the high in these end 15%ile was associated with symptoms / diagnosis. This allows us to filter out the noise from the significance in a sample. The question arises, should all of these be used or is there a critical limit? The current count is 1,960 taxa-shifts with one or more
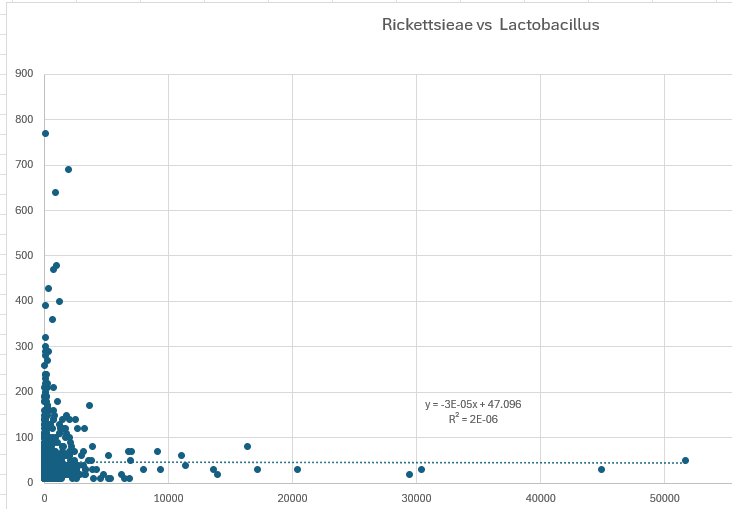
To address this issue, I decided to plot the counts.
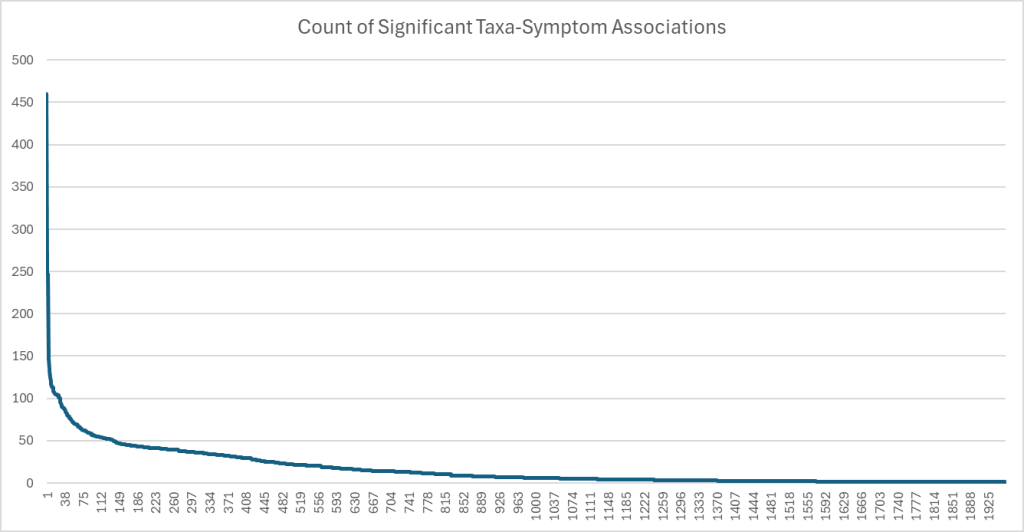
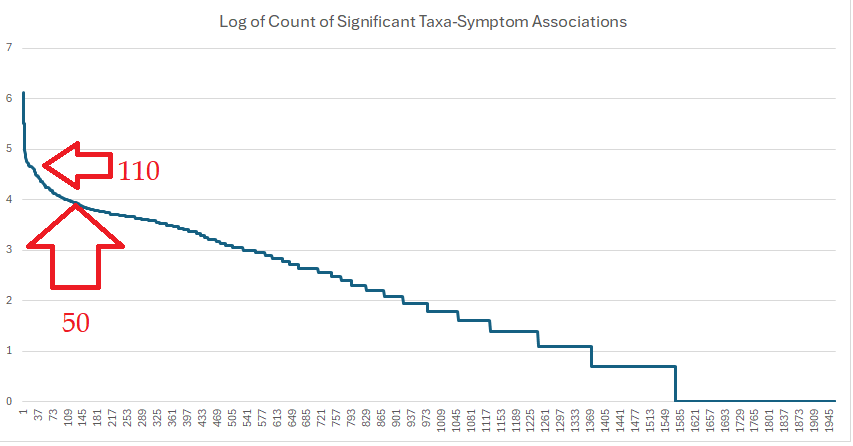
Applying a log function found a region became a straight line. Two apparent inflection points are suggested. Applying different function kept showing the same inflection points.
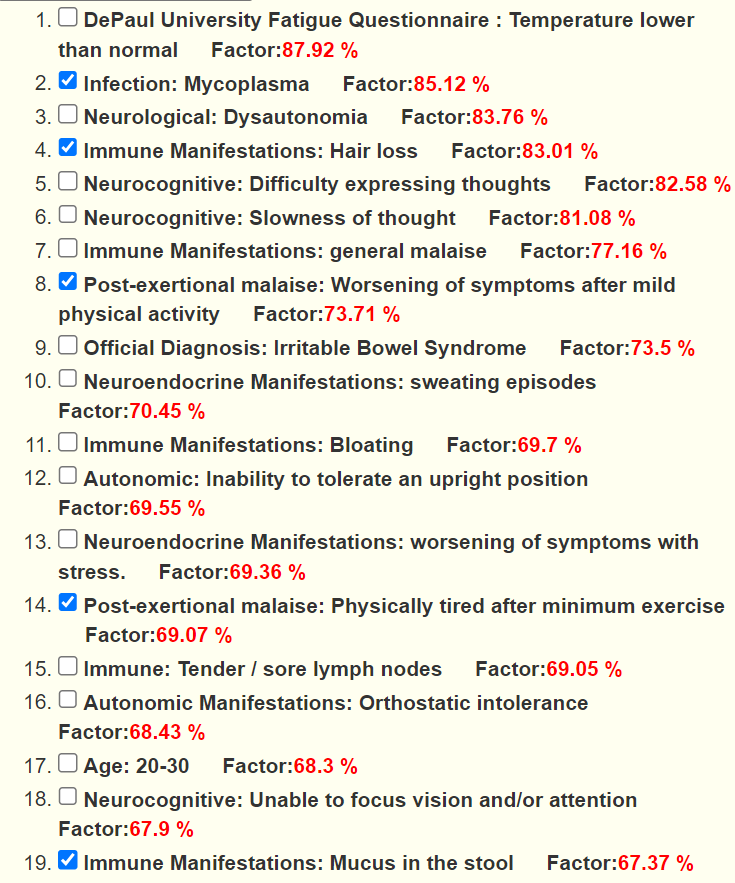
Bacteria with high and low associated to Symptoms
There are two species in this list. Both are reported in published clinical studies often.
| Bacteria | Rank |
| Faecalibacterium prausnitzii | species |
| Dorea formicigenerans | species |
| Weissella | genus |
| Faecalibacterium | genus |
| Acidaminococcaceae | family |
| Acidaminococcales | order |
The Short List of Bacteria
We see many bacteria not usually associated plus two familiar ones. Increases means more are in the 85-100%ile, decrease means more are in the 0-15%ile
| Bacteria | Rank | Direction | Count of Associations |
| Thermodesulfobacteriota | phylum | increases | 460 |
| Rhodothermota | phylum | increases | 247 |
| Rhodothermia | class | increases | 247 |
| Rhodothermales | order | increases | 247 |
| Actinomycetota | phylum | decrease | 146 |
| Holdemania | genus | increases | 135 |
| Faecalibacterium | genus | decrease | 133 |
| Coriobacteriaceae | family | decrease | 125 |
| Coriobacteriales | order | decrease | 120 |
| [Clostridium] thermoalcaliphilum | species | increases | 116 |
| Coriobacteriia | class | decrease | 115 |
| Lactobacillaceae | family | decrease | 114 |
| Bifidobacterium | genus | decrease | 113 |
| Sphingobacteriaceae | family | increases | 113 |
Longer List of Bacteria
| Bacteria | Rank | Shift | Count |
| Oscillospiraceae | family | decrease | 108 |
| Anaerotruncus colihominis | species | increases | 107 |
| Actinomycetes | class | decrease | 106 |
| Bacteroides | genus | increases | 106 |
| Hathewaya | genus | increases | 105 |
| Sharpea azabuensis | species | increases | 105 |
| Bacillota | phylum | decrease | 105 |
| Sharpea | genus | increases | 105 |
| Anaerotruncus | genus | increases | 104 |
| Sphingobacteriia | class | increases | 104 |
| Sphingobacteriales | order | increases | 104 |
| Lactobacillales | order | decrease | 101 |
| Ruminococcaceae | family | decrease | 101 |
| Erysipelothrix muris | species | increases | 100 |
| Erysipelothrix | genus | increases | 96 |
| Veillonellaceae | family | increases | 94 |
| Bacteroides caccae | species | increases | 92 |
| Clostridia | class | decrease | 90 |
| Bacteroides fluxus | species | increases | 89 |
| Eubacteriales | order | decrease | 89 |
| Ethanoligenens | genus | increases | 89 |
| Finegoldia | genus | increases | 88 |
| Hathewaya histolytica | species | increases | 87 |
| Hymenobacter xinjiangensis | species | increases | 87 |
| Roseburia faecis | species | decrease | 85 |
| Blautia obeum | species | decrease | 84 |
| [Clostridium] leptum | species | increases | 83 |
| Hymenobacter | genus | increases | 82 |
| Negativicutes | class | increases | 80 |
| Terrabacteria group | clade | decrease | 79 |
| Bifidobacteriaceae | family | decrease | 79 |
| Bacilli | class | decrease | 78 |
| Bifidobacterium adolescentis | species | decrease | 78 |
| Marvinbryantia | genus | increases | 77 |
| Phocaeicola vulgatus | species | increases | 77 |
| FCB group | clade | increases | 76 |
| Odoribacter denticanis | species | increases | 75 |
| Mediterraneibacter | genus | increases | 74 |
| Faecalibacterium prausnitzii | species | decrease | 73 |
| Eggerthella | genus | increases | 72 |
| Bifidobacteriales | order | decrease | 72 |
| Lachnoclostridium | genus | increases | 70 |
| Acidaminococcales | order | increases | 70 |
| Odoribacter | genus | increases | 70 |
| Acidaminococcaceae | family | increases | 70 |
| Blautia schinkii | species | increases | 69 |
| Dorea formicigenerans | species | increases | 69 |
| Collinsella | genus | decrease | 69 |
| Bacteroides stercoris | species | decrease | 69 |
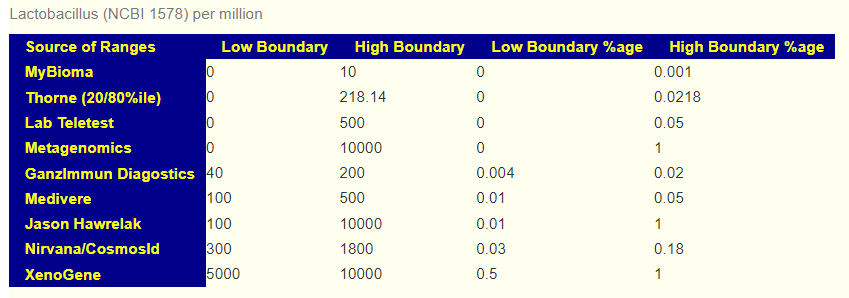
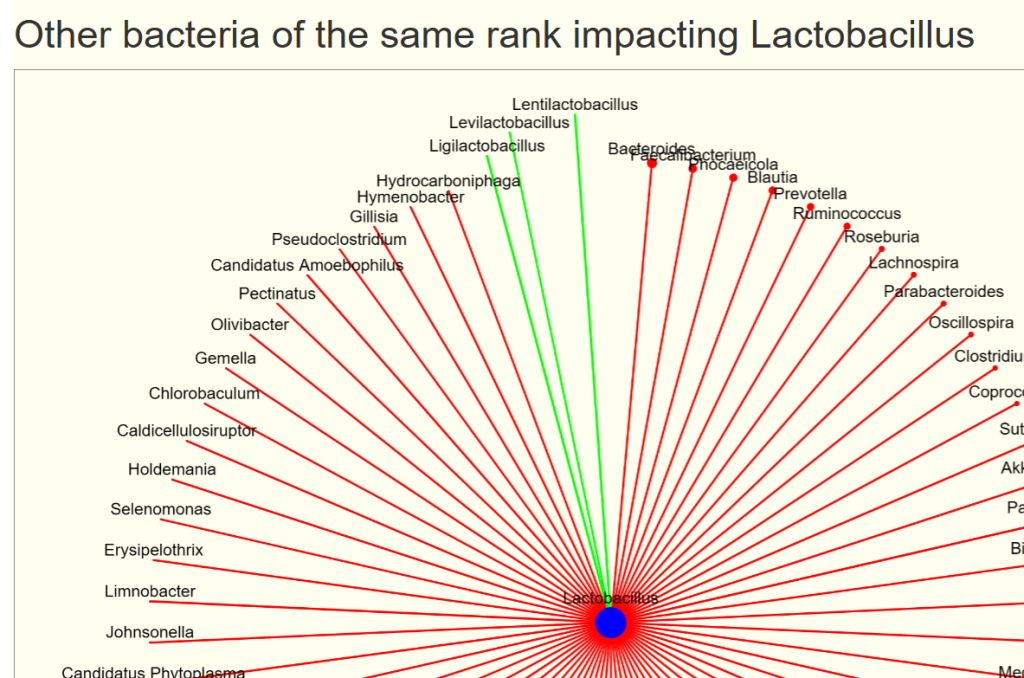
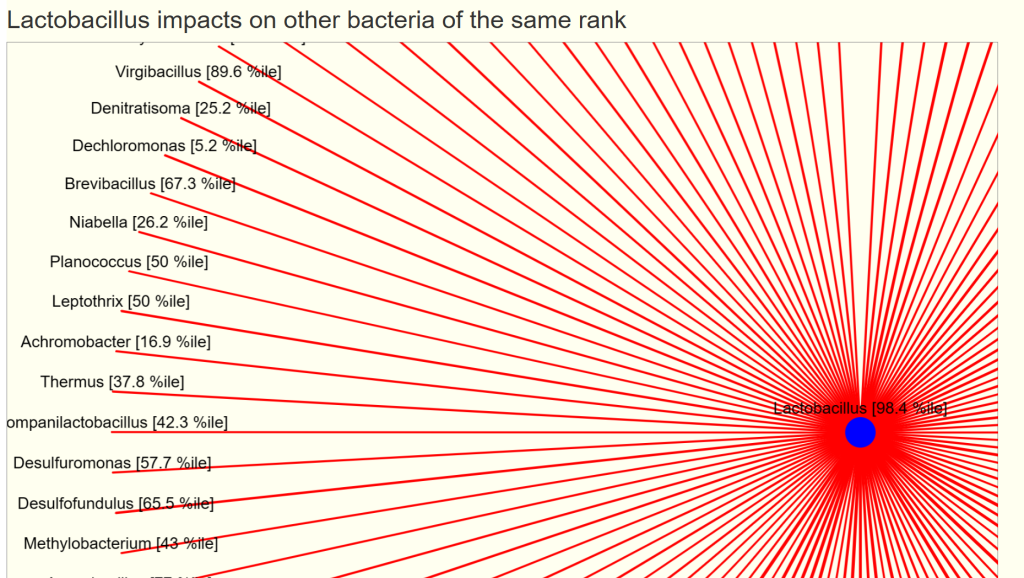
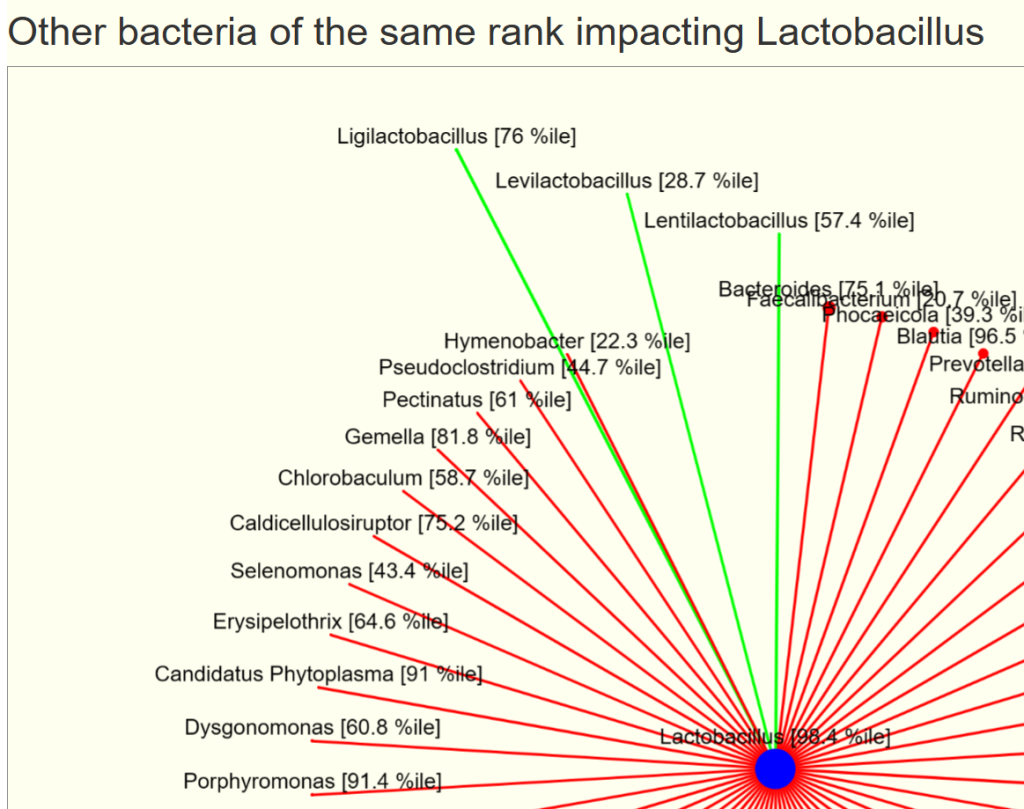
| Lactobacillus | genus | decrease | 68 |
| Pseudomonadota | phylum | increases | 67 |
| Odoribacteraceae | family | increases | 67 |
| Peptoniphilaceae | family | increases | 67 |
| Fusobacteriaceae | family | decrease | 66 |
| Dorea formicigenerans | species | decrease | 66 |
| Amedibacillus dolichus | species | increases | 65 |
| Amedibacillus | genus | increases | 65 |
| Candidatus Glomeribacter | genus | increases | 64 |
| Eggerthella lenta | species | increases | 63 |
| Finegoldia magna | species | increases | 63 |
| Oscillatoria corallinae | species | increases | 62 |
| Ruminiclostridium cellobioparum subsp. termitidis | subspecies | decrease | 62 |
| Oscillatoria | genus | increases | 62 |
| Tissierellales | order | increases | 62 |
| Ruminiclostridium cellobioparum | species | decrease | 62 |
| Hymenobacteraceae | family | increases | 62 |
| Pseudoflavonifractor | genus | increases | 61 |
| Mycobacteriales | order | increases | 61 |
| Tissierellia | class | increases | 60 |
| Lachnoanaerobaculum | genus | decrease | 60 |
| Coprococcus | genus | decrease | 59 |
| Blautia | genus | increases | 59 |
| Collinsella aerofaciens | species | decrease | 59 |
| Verrucomicrobiota | phylum | increases | 59 |
| Veillonellales | order | increases | 58 |
| [Ruminococcus] gnavus | species | increases | 58 |
| Selenomonas infelix | species | increases | 58 |
| Eubacterium ventriosum | species | decrease | 58 |
| Lactonifactor | genus | increases | 57 |
| Bacteroides cellulosilyticus | species | increases | 57 |
| Enterococcaceae | family | decrease | 57 |
| Fusobacterium | genus | decrease | 57 |
| Alistipes putredinis | species | increases | 57 |
| Sutterella | genus | decrease | 56 |
| Anaerotignum lactatifermentans | species | increases | 56 |
| Anaerotignum | genus | increases | 56 |
| Clostridium akagii | species | increases | 56 |
| Burkholderiaceae | family | increases | 55 |
| Akkermansiaceae | family | increases | 55 |
| Turicibacter | genus | decrease | 55 |
| Butyricimonas | genus | increases | 55 |
| Segatella copri | species | decrease | 55 |
| Mycoplasmoidales | order | increases | 55 |
| Turicibacteraceae | family | decrease | 55 |
| Turicibacter sanguinis | species | decrease | 55 |
| Akkermansia muciniphila | species | increases | 54 |
| Sporomusaceae | family | increases | 54 |
| Limnobacter | genus | increases | 54 |
| Limnobacter litoralis | species | increases | 54 |
| Lactobacillus rogosae | species | decrease | 54 |
| PVC group | clade | increases | 54 |
| Thiocapsa | genus | increases | 53 |
| Sphingobacterium bambusae | species | increases | 53 |
| Enterobacteriaceae | family | increases | 53 |
| Pseudoflavonifractor capillosus | species | increases | 53 |
| Blautia hansenii | species | increases | 53 |
| Akkermansia | genus | increases | 53 |
| Marvinbryantia formatexigens | species | increases | 52 |
| Enterococcus | genus | decrease | 52 |
| Corynebacteriaceae | family | increases | 52 |
| Lachnospira | genus | increases | 52 |
| Lachnospira eligens | species | increases | 52 |
| Corynebacterium | genus | increases | 52 |
| Mycoplasmataceae | family | increases | 52 |
| delta/epsilon subdivisions | clade | decrease | 52 |
| Bacteroides faecis | species | increases | 52 |
| Bacteroides gallinarum | species | increases | 52 |
| Veillonella | genus | increases | 51 |
| Weissella | genus | increases | 51 |
| Dialister invisus | species | increases | 51 |
| Blautia hydrogenotrophica | species | increases | 51 |
| Lactonifactor longoviformis | species | increases | 50 |
| Dorea longicatena | species | decrease | 50 |
Best Test/Lab?
The above is based on percentile and not the typical percentage. The results from Clinical Microbiomics A/S (a.k.a. CosmosId) provides percentile ranking again a regionalized healthy population. In the US, their tests are available retail from Thorne. They will soon be available retail from Precision Biome in the EU.







Recent Comments