Probiotics are a HUGH profit margin. The cost to produce is pretty constant. The difference per BCFU from the cheapest to the most expensive is 650x (i.e. 65,000% difference). You can cut your supplement costs greatly with some careful shopping around and computing the cost per BCFU.
Below are some buying options. I will use Lactobacillus reuteri to illustrate the price issues
50 grams at 20 BCFU/gram = 1000 BFCU for $15.00 = 66 BCFU per dollar They are probiotics with fructooligosaccharides only, no other fillers. Certified Organic
As a reminder, Microbiome Prescription is a “best efforts” site. We do the best that we can with the data that is available.
Request from Reader
Hello Ken,
I would kindly like to ask your opinion on this. I did three BiomeSight tests in three years, then one Xenogene. The Xenogene and last BiomeSight were 10 days apart.
BiomeSight was telling me for three years that my butyrate producers were awesome and my F.Prau was great. Then Xenogene told me the exact opposite. BiomeSight results being so good for so long, I always assumed I have no problem in the microbiome so I kept my diet (15g of fiber at max, lots of meat, veggiest mainly potatoes – no 30-40 different veg/fruit per week). Butyrate producers and F.Prau this high on this diet is a little hard to believe, so I came to the conclusion that BiomeSight is completely off, at least for me.
I remember the Taxonomic nightmare article you wrote and I understand that I cant directly compare two test providers. But when one test tells you that your microbiome is a rockstar and the other tells you its a zombie, its hard to see the usefulness of biomeSight testing. I kindof hope there is some magic that Im forgetting and the biomeSight tests will not prove to be a waste of time and money.
The Xenogene values are percentages of bacteria only (i.e. # F. Prau / # total bacteria), so its “the same thing” as in biomeSight results. Just to be clear that its not # F.Prau / (# bacteria + # protozoa + # archaea + # fungi).
Explanation
Numbers always need to be interpreted against reference ranges.
In other words, both test results were within 1 standard deviation of the mean – that will usually be interpreted as in the normal/reference range. The formula is easy:
(Your Value - Mean) / Standard Deviation
You can do this for each of the bacteria in your report. If the resulting value is between -1.6 and +1.6, you are clearly in the reference ranges.
Lab Provided Ranges
Xenogene provides ranges — this means that over 70% of xenogene files uploaded to MP are below the reference range.
Biomesight reference ranges are below
Every value is within the reference ranges. We have a disagreement.
Dr. Jason Hawrelak Recommendations
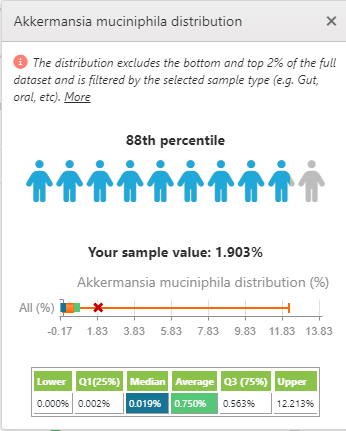
His ranges are 1-5% for Akkermansia. These are much less than Biomesight and bigger than xenogene. User Feedback: “Dr. Hawrelak’s ranges – how can Dr. Hawrelak have a general range on some bacterium w/o stating which lab he uses for this? Considering all labs report different numbers due to the taxonomy nightmare, I don’t understand how there can be “one range to rule them all”. “
I agree totally, some labs cites him as an authority because they lack the skilled resources to determine their lab specific ranges, Often I have seen ranges from a published studied applied to numbers from a totally different processing pipeline – when challenged they cite “it’s an authority“. Some more readings:
As a FYI: I include his ranges because people have requested it. I provide choices and not judgements.
Microbiome Prescription Ranges
We do not have enough data to independently compute xenogene. Xenogene samples are part of “Other Labs”. The Kaltoft-Møldrup ranges are:
Other Labs: 0 – 7%
Biomesight: 0 -9.6%
Similarly using BoxPlot methodology,
Other Labs: 0 – 3.8%
Biomesight: 0 -1.7%
Note that Zero (0) is in range for many of these.
The Symptoms Factor
Identifying bacteria associated with symptoms depends on the number of samples uploaded with annotated symptoms. We do not have sufficient results with Xenogene, we do have sufficient for Biomesight with some 289 associations at present. Note this is pattern matching. “It has the ears of a German Shepard, it has a double coat of a German Shepard, it eyes color matches a German Shepard…etc. ” It may be German Shepard or it may be a Wolf or a Welsh Pembroke Corgi
For the latest Biomesight, we see a lot of matches to existing patterns
For Xenogene (which uses “Other Labs”) we have less and weaker matched
If you want to include your symptom in the suggestions report, biomesight is a better choice.
Eubiosis
Eubiosis is not very comparable, because Xenogene is mixed with all of the other odd labs. We have just 19 xenogene, not sufficient to do that much data, We have 61 samples from Thorne – same issue.
Follow up Questions
So my question was how can BiomeSight tell me my butyrate producers are 60% when its highly unlikely, just as with F.Prau being 19%. And the answers that I could imagine getting would be
you having 60% butyrate producers is the result of taxonomic hell, in some cases the positive measurement errors can add up resulting in a hugely overestimated sum – judging the SCFA producers in the biomeSight report is unreliable and should not be taken into consideration at all
OR the only relevant marker for abundance of SCFA producers is stool pH or SCFA measured in stool – use that instead of the SCFA producers % reported by ANY test provider
OR something else if the former two are nonsense
Butyrate evaluation is a good illustration minefield. Some observations:
Labs will usually qualify with “It is important to note that this is not a measure of these metabolites found in the stool sample.“
MP is the only one that appears to include consumers (thus getting a net amount). The choice of genus and species is often based on the depth of research that each lab does. MP is based on the genetics of the bacteria as sequenced and aggregated by KEGG. We do not know if the genetics are activated or not (epigenetics).
What is missing are studies comparing various estimates from bacteria against actual directly determined levels of butyrate and other metabolites…
Second Issue: Percentage of WHAT?
Many labs pull a magical number out of the air, typically if you are over this number you are Satisfactory, below Not Satisfactory. MP gives a percentile ranking against others samples using the same lab. If you are over 30%ile, I would deem it to not need work — but that is a personal judgement call, the numbers are there for you.
Bottom Line
Microbiome reports are full of uncertainty aka fuzzy data. Fuzzy data is not a strong selling point for businesses. Claiming accuracy and correctness is a great marketing ploy. If there are no legal/financial consequences of these dubious claims then they will typically be made by some.
I have seen some labs that started by “just reporting the facts/numbers” and then drift into interpretations because marketing studies found that would increase business.
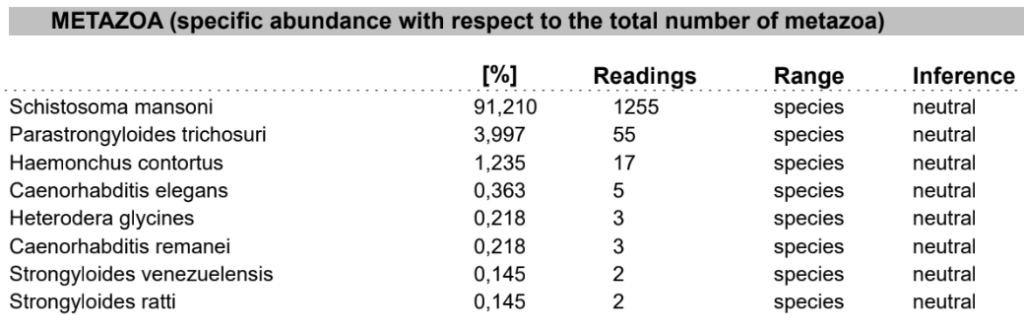
Xenogene (and Thorne) is good because of what else it reports that is not reported on Biomesight which may be part of your health issues. For items that seem very high, you should do some research on them and if any medical conditions are reported/associated with them.
On the other side, we have a lot of samples with annotated symptoms for Biomesight and Ombre. This means that suggestions to modify your microbiome (especially if symptoms are used) are likely better.
My usual advice is simple:
do one of Xenogene or Thorne to check for non bacteria issues (fungi, phages, etx)
use Biomesight or Ombre for regular testing and getting suggestions.
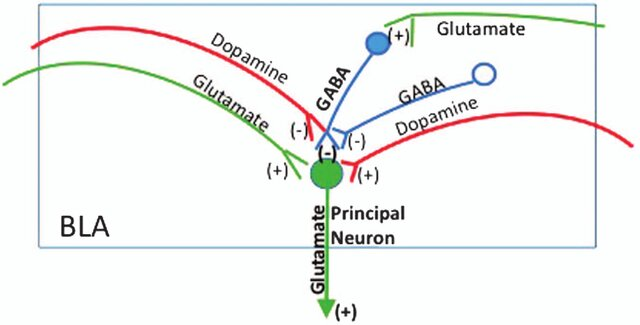
Excessive GABA may be associated with Huntington’s disease, epilepsy, and certain types of encephalopathies. Insufficient GABA may be associated with Anxiety Disorders, Epilepsy, Sleep Disorders, Mood Disorders, Substance Use Disorders, Movement Disorders, Neuropathic Pain and Autism Spectrum Disorders.
Excessive Dopamine may be associated with: Mania or Hypomania, Psychosis, Substance Use Disorders, Hyperactivity and Impulsivity, Tics and Tourette Syndrome, Sleep Disorders, Huntington’s Disease and Excessive Reward Seeking Behavior. Insufficient dopamine may be associated with: Parkinson’s Disease, Depression, Attention-Deficit/Hyperactivity Disorder (ADHD), Drug Addiction and Substance Use Disorders, Restless Legs Syndrome, Schizophrenia and Huntington’s Disease.
Excessive Glutamate may be associated with: Stroke, Traumatic Brain Injury (TBI), Neurodegenerative Diseases, Epilepsy, Migraine, Hypoxic-Ischemic Encephalopathy (HIE), Schizophrenia, Major Depressive Disorder, Bipolar Disorder and Trauma and Neuroinflammation. Insufficient Glutamate may be associated with Cognitive Impairment and Memory Disorders, Depression, Schizophrenia, Pain Disorders, Huntington’s Disease, Epilepsy, Neurodevelopmental Disorders and Sleep Disorders.
Protein-Rich Foods: Glutamate is naturally present in protein-containing foods. Foods high in protein, such as meat, poultry, fish, eggs, dairy products (especially aged cheeses), and legumes, contain significant amounts of glutamate.
Fermented Foods: Fermented foods contain glutamate due to the fermentation process, during which glutamate-producing bacteria break down proteins into amino acids. Examples include soy sauce, miso, tempeh, fermented vegetables (e.g., sauerkraut, kimchi), fermented dairy products (e.g., yogurt), and aged cheeses (e.g., Parmesan, Roquefort).
Seaweed: Certain types of seaweed, such as kombu (kelp), nori, and wakame, are rich sources of glutamate.
Tomatoes: Tomatoes and tomato-based products (e.g., tomato sauce, tomato paste) contain glutamate, contributing to their savory flavor.
Mushrooms: Some varieties of mushrooms, such as shiitake mushrooms, are naturally high in glutamate.
Producers
From Chat-GPT:
Lactobacillus species: Various species within the Lactobacillus genus are known to produce glutamate during fermentation. Examples include Lactobacillus brevis, Lactobacillus plantarum, and Lactobacillus fermentum. These bacteria are commonly used in the fermentation of foods such as sauerkraut, kimchi, pickles, and certain dairy products.
Bacillus subtilis: Bacillus subtilis is a Gram-positive bacterium known for its ability to produce glutamate. It is used in the fermentation of soybeans to produce traditional Japanese seasonings such as miso and soy sauce.
Corynebacterium glutamicum: This bacterium is widely used in industrial fermentation for the large-scale production of glutamate and glutamate-derived compounds. Corynebacterium glutamicum is a key organism in the production of monosodium glutamate (MSG), a food additive used to enhance flavor.
Streptococcus species: Some species of Streptococcus bacteria are capable of producing glutamate during fermentation. Streptococcus thermophilus, for example, is commonly used in the fermentation of yogurt and certain cheeses.
Propionibacterium freudenreichii: This bacterium is involved in the fermentation of Swiss cheese, where it produces various flavor compounds, including glutamate.
A reader asked me to do an update of my 2016 post Psychoactive Probiotics! There has been a lot of recent literature as shown on PubMed. Note that often these are strain specific and not generalized for species cited below. If you cannot find the strains specified in the studies, it may be worthwhile trying different brands of the species (with the most studied species being most probable).
Excessive Dopamine may be associated with: Mania or Hypomania, Psychosis, Substance Use Disorders, Hyperactivity and Impulsivity, Tics and Tourette Syndrome, Sleep Disorders, Huntington’s Disease and Excessive Reward Seeking Behavior. Insufficient dopamine may be associated with: Parkinson’s Disease, Depression, Attention-Deficit/Hyperactivity Disorder (ADHD), Drug Addiction and Substance Use Disorders, Restless Legs Syndrome, Schizophrenia and Huntington’s Disease.
A reader asked me to do an update of my 2016 post Psychoactive Probiotics! There has been a lot of recent literature as shown on PubMed. Note that often these are strain specific and not generalized for species cited below. If you cannot find the strains specified in the studies, it may be worthwhile trying different brands of the species (with the most studied species being most probable).
Excessive GABA may be associated with Huntington’s disease, epilepsy, and certain types of encephalopathies. Insufficient GABA may be associated with Anxiety Disorders, Epilepsy, Sleep Disorders, Mood Disorders, Substance Use Disorders, Movement Disorders, Neuropathic Pain and Autism Spectrum Disorders.
“Metagenomic analyses suggest that the genomes of many gut bacteria encode glutamate decarboxylase (GAD), the enzyme that catalyzes GABA production.” [2023]
“Stress exposure induced a decline in Lactobacillaceae abundance and hence γ-aminobutyric acid (GABA) level in mice.” [2023]
Note: monosodium glutamate (MSG) can increase the production of GABA [2024]
NOTE: The current official name is used below. Most L. species were known as Lactobacillus with older names.
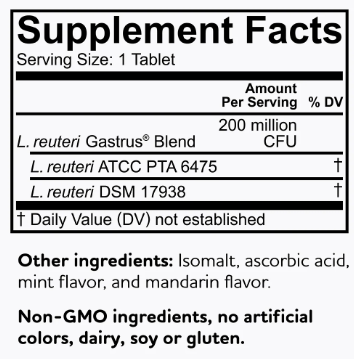
Note: Gamma aminobutyric acid production by commercially available probiotic strains [2023] cites that the best are: Levilactobacillus brevis LB01 [Source], Lactiplantibacillus plantarum 299v [Jarrow Formulas Ideal Bowel Support].
Lactiplantibacillus plantarum 299v is the most available with many suppliers. A dosage of 10-60 BCFU per day is recommended.
“These results suggest that chronic ingestion of Lactobacillus plantarum strain PS128 could ameliorate anxiety- and depression-like behaviors and modulate neurochemicals related to affective disorders.Thus PS128 shows psychotropic properties and has great potential for improving stress-related symptoms.” [2015]
“PS128 is safe and could induce changes in emotional behaviors…These findings suggest that daily intake of the L. plantarum strain PS128 could improve anxiety-like behaviors and may be helpful in ameliorating neuropsychiatric disorders.”[2016]
“We previously have demonstrated that administration of Lactobacillus rhamnosus (JB-1) to healthy male BALB/c mice, promotes consistent changes in GABA-A and -B receptor sub-types in specific brain regions, accompanied by reductions in anxiety and depression-related behaviors.”[2016] [2014] [2014]
“Within minutes of application, JB-1 increased the constitutive single- and multiunit firing rate of the mesenteric nerve bundle, but Lactobacillus salivarius (a negative control) or media alone were ineffective.” [2013]
One study showed improved mood in healthy volunteers following 3-week consumption of a probiotic-containing milk drink that contained Lactobacillus casei Shirota” [2007]
“administration of the probiotic, L. casei Shirota, decreased anxiety in patients with chronic fatigue syndrome.”[2009]
I think I grew up with dysbiosis, as evidenced by allergies, mild asthma, and neuro divergencies (extremely withdrawn and attention deficit). In my 20s developed mild semi-functional CFS due to chronic stress.
In 2020 was exposed to black mold, and had a short very strange illness around this time. Then later I got the first 2 covid vaccines, followed by the booster Dec 2021, which was my major trigger. Symptoms: Shortness of breath, CFS, chest pain,chest pressure, palpitation, insomnia, fight or flight/anxiety, hallucinations, joint pain, food intolerance, histamine issues, exercise intolerance, PEM, tinnitis, nausea, apparent veinous insufficiency, endotheliatis head pressure, neck pain, POTS, etc. I also grew a nerve tumor (this appeared 2 years later). EBV antibodies showed very high.
Some of these symptoms have gone away, and my intensity of illness is maybe 1/3 of what it was in the beginning, but I seem to have reached a plateau. My Biomesight showed a bunch of issues and I’m looking to correct it in order to give my immune system a chance to normalize.
Analysis
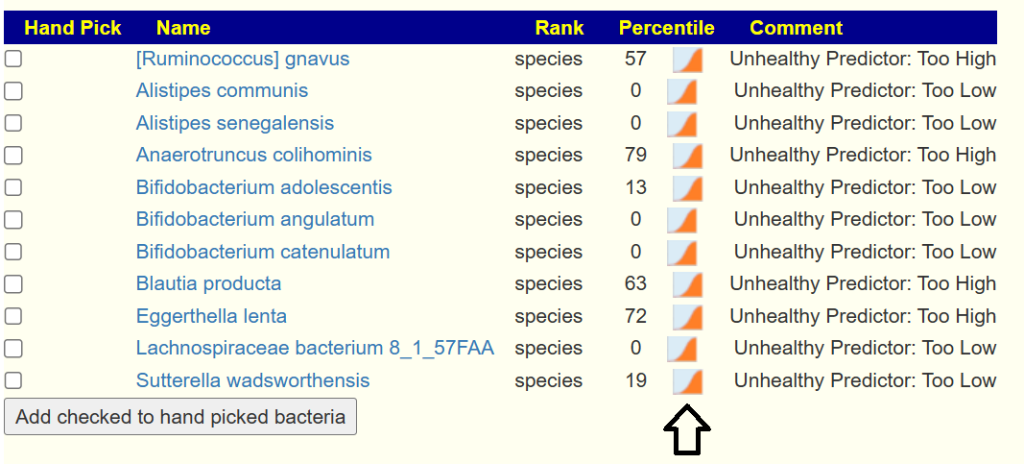
We see an excessive number of bacteria/taxa at very high levels, suggesting they are dominating the microbiome.
Drilling down to Health Indicators
With Dr. Jason Hawrelak Recommendations, we are at the 66%ile, a reasonable level. The MHI-A ratio is low, indicating issues. With Bacteria deemed Unhealthy, Streptococcus vestibularis(An unhealthy Predictor) was at 98%ile and Escherichia coli was at 96%ile. E.Coli can be good or bad (16s is not able to tell them apart) — an ad-hoc test is to try Mutaflor probiotics (E-Coli Nissle 1917) and if there is either a major herx or major improvement, then we can assume a major bad E.Coli component. Mutaflor is aggressive against bad E. Coli.
Using Potential Medical Conditions Detected, one items is a strong match: Postural orthostatic tachycardia syndrome at 85%ile
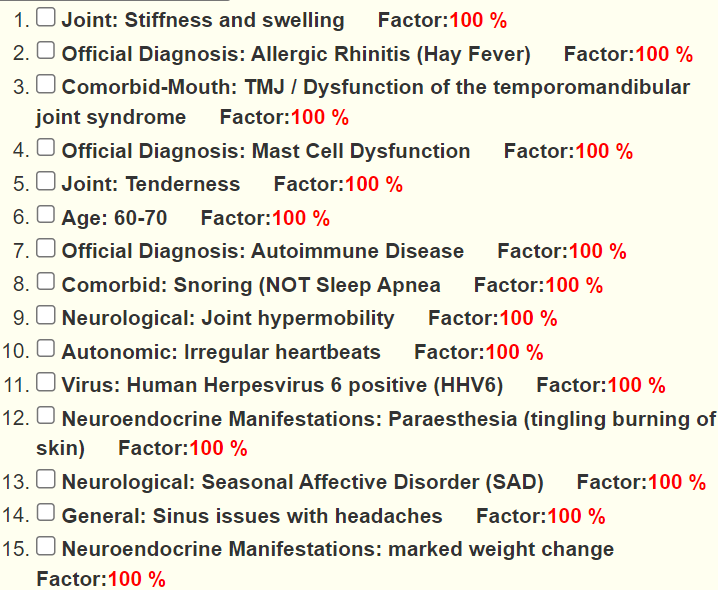
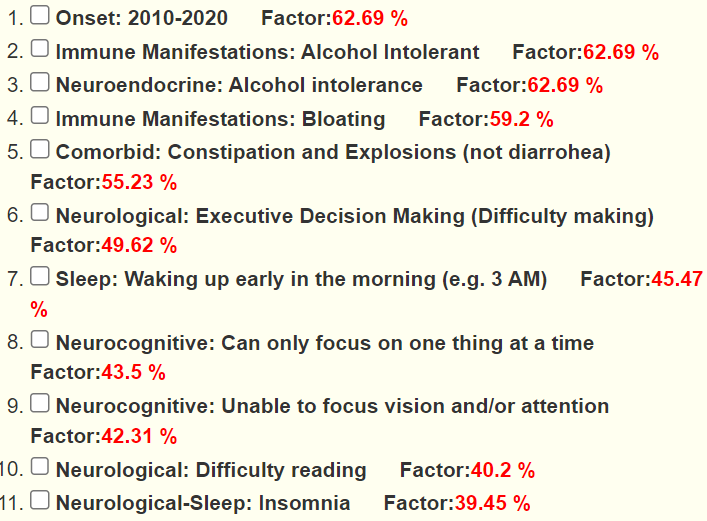
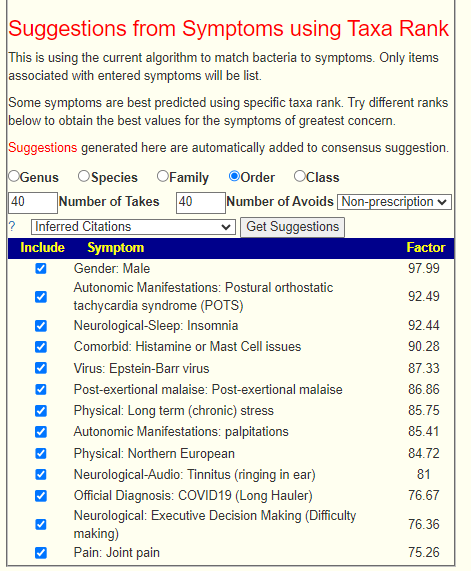
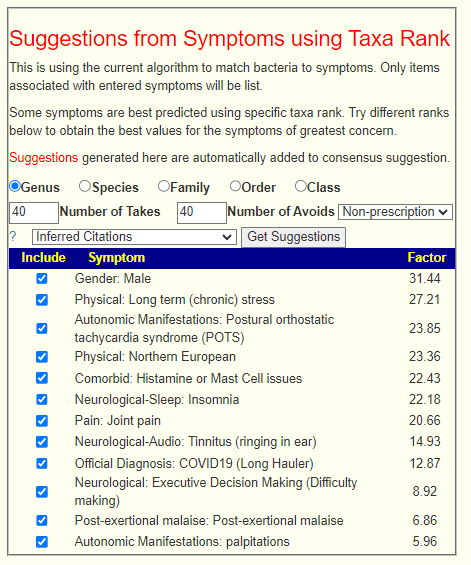
Using the new Taxa-Symptom Association, we find some strong matches at the order level, which are not there at the genus level. The highest possible factor is 100 (matching every association).
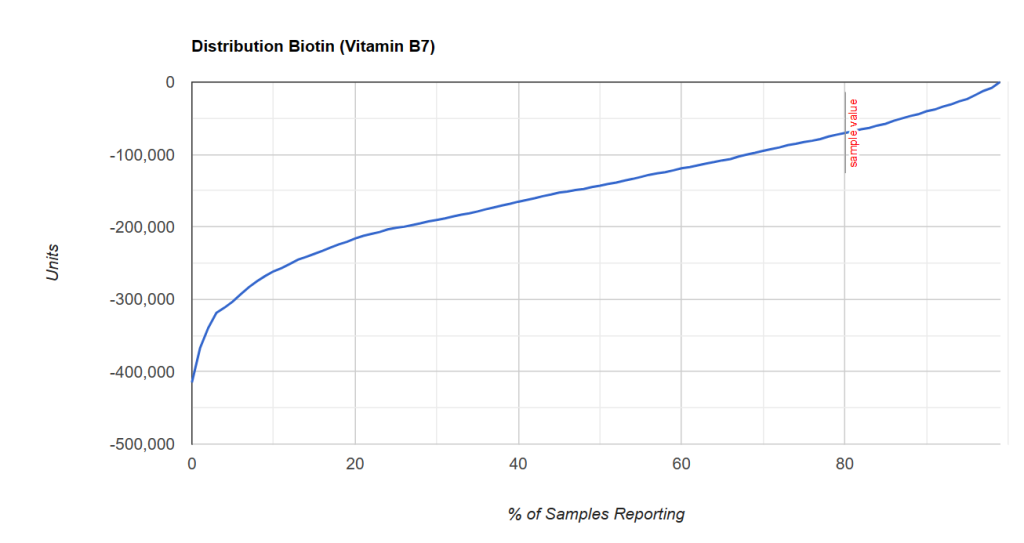
Scanning General Health Predictors, the only item that stood out was low Vitamin K2 production, which suggests that Vitamin K supplements may be beneficial.
Going Forward
I am going to do [Just Give me suggestion with symptoms] and then suggestions using Order above (the taxa rank that has the highest factor (best match)]. This gives us 6 sets of suggestions. Taxa “Order” is above the data for antibiotics, so sorting to only those items with 6 Takes, we end up with a clean list shown below of all suggestions saying take with high Priorities — sweet!. Lactobacillus casei, siblings (paracasei) and lactobacillus casei shirota (probiotics) dominate probiotics to the exclusion of other probiotics. This group is well known to help allergies and reduce histamine issues.
I was also a person who responded very well to Mutaflor (we always have some in the fridge). In my case, the initial response was massive herxing for two weeks.
General Guidance
For items to take, remember that goal is to disrupt the dysbiosis. This means subjecting it to constantly changing “shocks” so it is unable to adapt. This has been shown to be effective when dealing with antibiotics (i.e. rotating between different antibiotics with breaks is more effective than taking the same antibiotic continuously).
My suggestion for a rotating 4 week cycle changing probiotics and herbs every week. Be aware of not falling into either the homeopathic or product labelling traps — that is, taking less then therapeutic levels. To determine those dosages see Supplement Dosages. In general, you want to be close to the maximum dosages used in studies (i.e. “deemed safe dosages”).
Vitamins and polyphenols can be taken continuously.
Feedback
Honestly, whatever algorithm is being used for symptoms is nothing short of amazing
POTS is probably my main challenge, and I have all but two of the other symptoms. And the two that I don’t currently have (joint pain and insomnia) I have had in the past. So basically it’s 100% accurate in my case
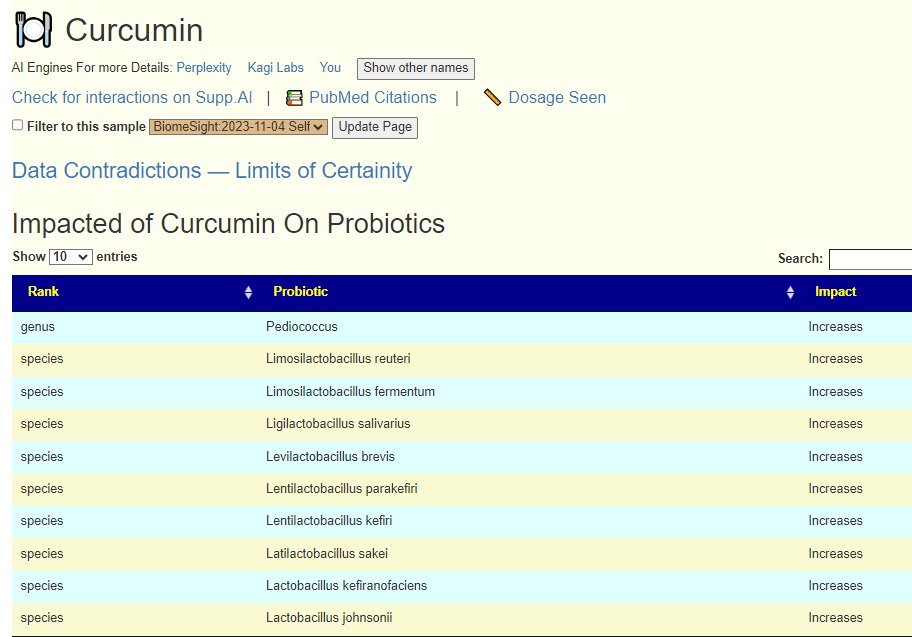
For interventions- A friend of mine just mentioned diosmin to me the other day. B3, B1, HMO, caffeine have all been helpful. Amazed to see Curcumin so high as it’s not really something I considered trying.
Mutaflor has been amazingly helpful the last few days (neurotransmitters and gut and fatigue) but I’ve heard it can’t be taken with other probiotics due to competing?
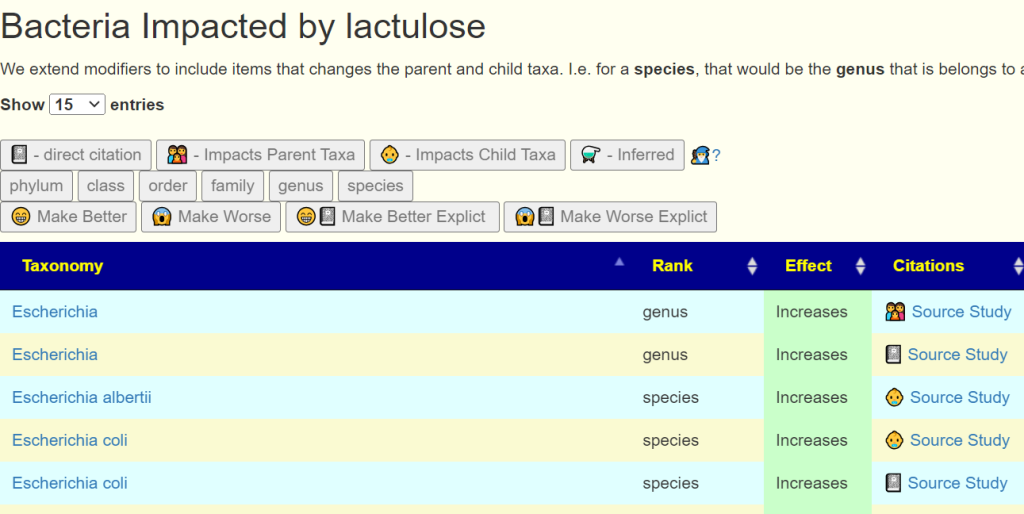
I’m interested in Lactulose for the bifido also, as I’ve heard a lot about this recently.. Thanks for taking the time, very very interesting! Also, one question if you have a moment. Are the interventions supposed to – directly improve the biome Or improve symptoms?
From first draft sent to him.
Answer: The data is computed to correct the bacteria shifts with statistical associations to symptoms. Adding suggestions for symptoms is another massive data extraction and entering. Readers can do cross validation for symptoms if they are inclined to search the literature (https://pubmed.ncbi.nlm.nih.gov/ )
Many suggestions have never been tried against the symptoms.
Q: Or can the herbs possibly be mixed w probiotics?
Yes they can, but you should check that the herb does not inhibit the probiotics currently being taken. To do this, just click on the herb, You want compatible probiotics with the herbs.
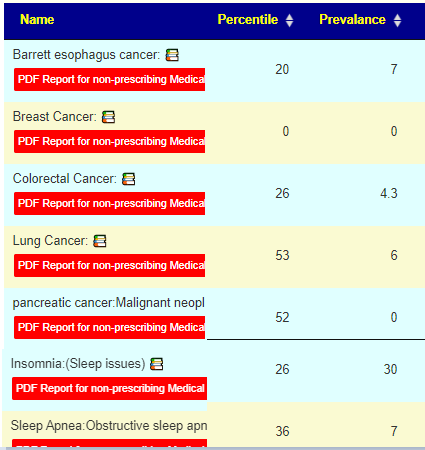
Q: Also, do your algorithms pick up probability of sleep apnea and cancer? These are conditions I’m trying to assess my risk of having / getting
They do pattern matching by two methods:
Articles on the US National Library of Medicine (go to https://microbiomeprescription.com/Library/PubMed ) AFTER LOGGING IN. It gives the percentile ranking of the number of matches you have compare to other samples.
Citizen Science based on self-reported symptoms and diagnosis. At present only Sleep Apnea Diagnosis has sufficient data for biomesight samples. For Sleep Apnea, you have 63% of the shifts matching which suggests that you may be heading in that direction, but sleep disturbances have much higher matches.
Q: This is extremely helpful Do you have any idea if there would be an interaction between mutaflor and lactulose? Mutaflor has still been amazing , semi- miraculous. It’s working so well I haven’t tried anything else yet. But I am very keen to get my bifido up
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.Posted on by Research and tagged
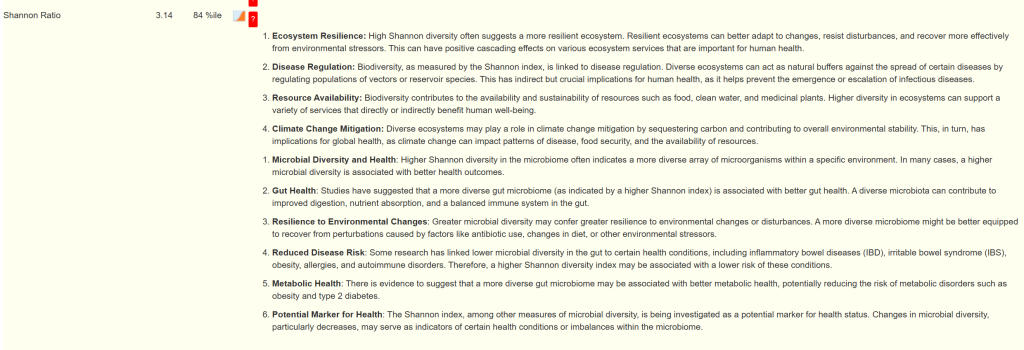
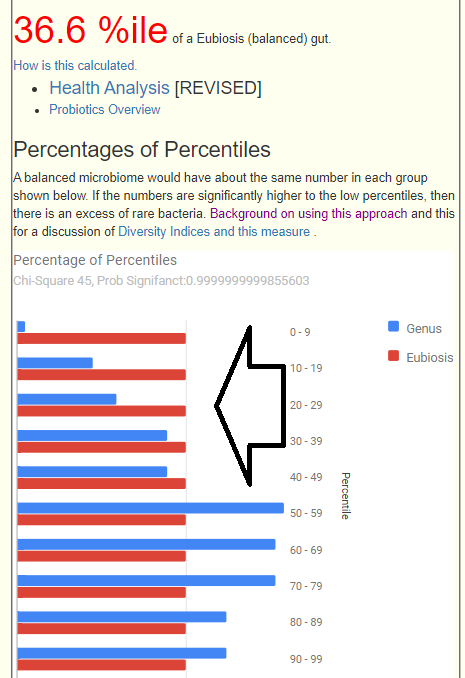
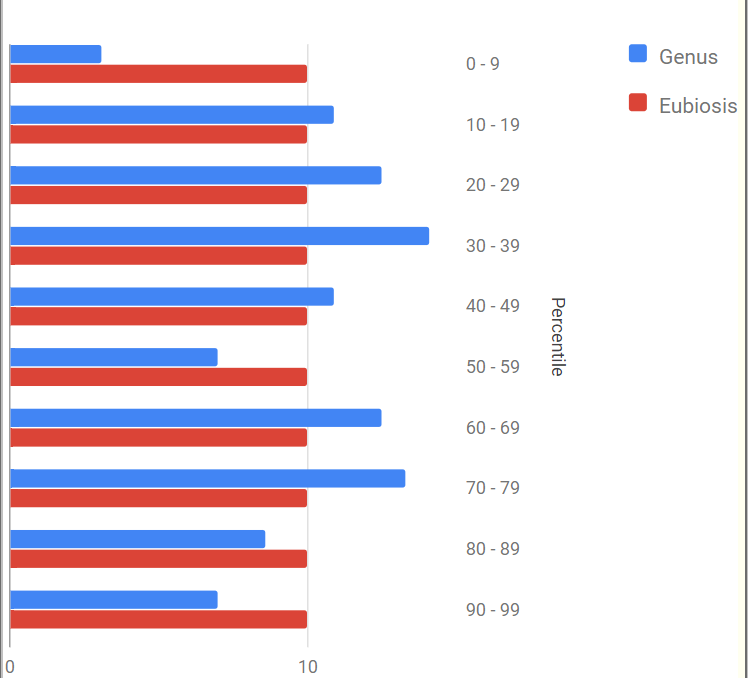
Recently I have gotten some messages concerned about Eubiosis scores dropping. Eubiosis is a measure of evennessof the bacteria representation. It cannot be used to identify which bacteria needs to be changed. It is a representation of the Chi2 value of the genus converted to %ile with values over 80%ile deemed 100%.
What is statistically ideal is:
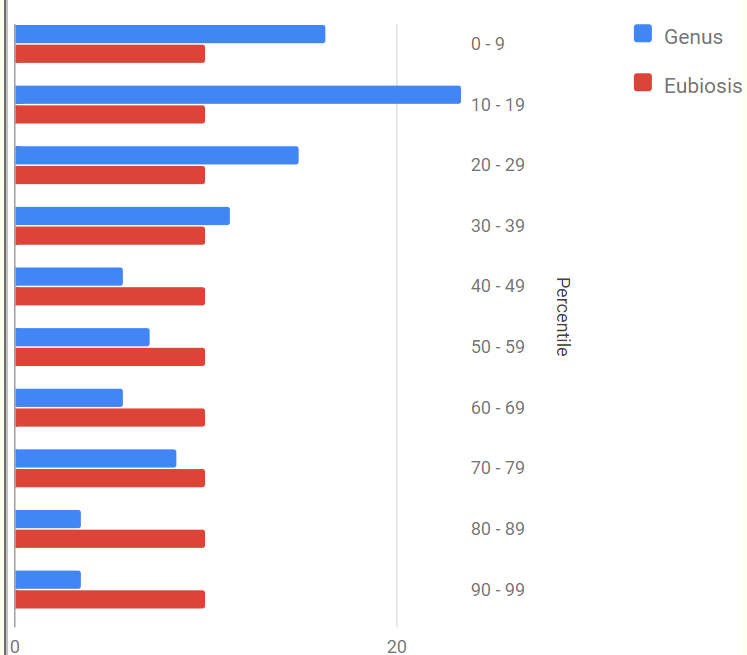
Below is an example of a low score of 1.2%
Dr. Jason Hawrelak score is 28%ile, MHI-A Ratio is 47%
It is saying that you have very few bacteria genus that have high representations and a ton of bacteria with high representation. This patterns suggest that the gut has become destabilized (which if you have dysbiosis is a good thing) but has not stabilized.
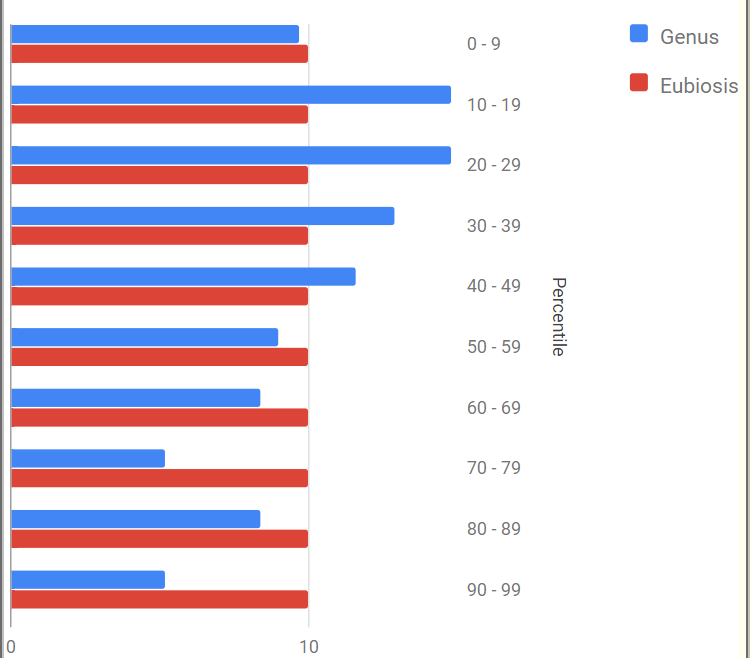
Same Person – Prior Pattern
The person has improved compared to this pattern. The “peak: was at 10-19 and above it has shifted to 10-29 range. Dr. Jason Hawrelak score is 46%ile MHI-A Ratio 67%
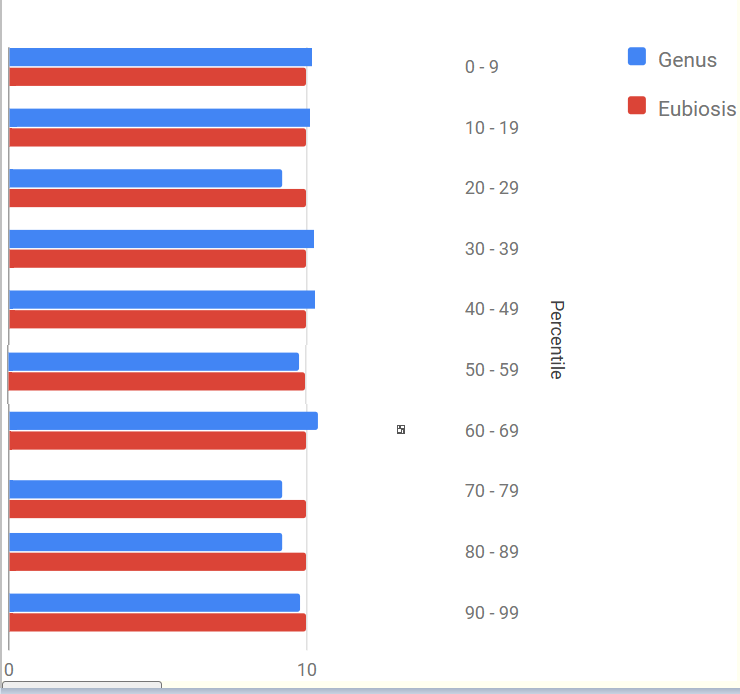
Same Person — further back
This is a better looking pattern. But remember this is not a primary measure for a gut score, but an adjunct dimension to be considered. For example, Dr. Jason Hawrelak score is a low 5%ile. MHI-A Ratio 66%ile
A question was ask – are there significant gender differences with ME/CFS. A partial answer is possible from our citizen science data (Available here). The number of bacteria identify as statistical significant drops because we are reducing sample sizes. The table below shows the shifts that are seen in common with P < 0.01.
For Symptom of ME/CFS
Source
Tax_name
tax_rank
Male
Female
Male_Chi2
FeMale_Chi2
thryve
Thermodesulfobacteria
phylum
increases
increases
234.0375
138.4544
biomesight
Verrucomicrobiaceae
family
increases
increases
8.333333
7.262051
biomesight
Rhodothermaeota
phylum
increases
increases
179.2
217.3071
biomesight
Akkermansiaceae
family
increases
increases
8.718378
9.965634
biomesight
Erysipelothrix muris
species
increases
increases
9.533889
10.08333
biomesight
Akkermansia
genus
increases
increases
8.718378
9.965634
biomesight
Rhodothermales
order
increases
increases
179.2
217.3071
biomesight
Akkermansia muciniphila
species
increases
increases
8.718378
9.965634
biomesight
Erysipelothrix
genus
increases
increases
9.663289
9.663289
biomesight
Rhodothermia
class
increases
increases
179.2
217.3071
biomesight
Thermodesulfobacteria
phylum
increases
increases
281.1738
299.9112
ME/CFS With IBS
We find differences here.
Source
Tax_name
tax_rank
Taxon
Male
Female
Male_Chi2
FeMale_Chi2
biomesight
Sutterella
genus
40544
decrease
increases
8.333333
11.25018
biomesight
Rhodothermales
order
1853224
increases
increases
139.9274
114.5716
biomesight
Dorea
genus
189330
increases
decrease
18.75
16.17875
biomesight
Rhodothermia
class
1853222
increases
increases
139.9274
114.5716
biomesight
Thermodesulfobacteria
phylum
200940
increases
increases
280.3333
187.9779
biomesight
Sutterellaceae
family
995019
decrease
increases
8.333333
11.25018
biomesight
Alcaligenaceae
family
506
decrease
increases
8.333333
9.120714
biomesight
Rhodothermaeota
phylum
1853220
increases
increases
139.9274
114.5716
ME/CFS Without IBS
We found no differences yet (given the sample size)
Source
Tax_name
tax_rank
Taxon
Male
Female
Male_Chi2
FeMale_Chi2
biomesight
Bacteroides fluxus
species
626930
increases
increases
7.355161
7.910588
biomesight
Thermodesulfobacteria
phylum
200940
increases
increases
124.4571
170.4624
Irritable Bowel Syndrome
Following up from above and noting that there is a gender bias in incidence, we find some differences
thryve
Thermodesulfobacteria
phylum
200940
increases
increases
252.8232
95.10095
biomesight
Rhodothermales
order
1853224
increases
increases
125.1467
110.6182
biomesight
Rhodothermia
class
1853222
increases
increases
125.1467
110.6182
biomesight
Thermodesulfobacteria
phylum
200940
increases
increases
314.4971
174.6182
biomesight
Rhodothermaeota
phylum
1853220
increases
increases
125.1467
110.6182
biomesight
Sharpea azabuensis
species
322505
increases
increases
16.18526
6.80625
biomesight
Sharpea
genus
519427
increases
increases
16.18526
6.80625
thryve
Mycoplasma
genus
2093
increases
decrease
12.81524
20.3229
thryve
Mycoplasmataceae
family
2092
increases
decrease
14.88581
20.3229
thryve
Phocaeicola vulgatus
species
821
increases
decrease
7.893492
17.06273
thryve
Mycoplasmatales
order
2085
increases
decrease
14.88581
26.01485
Depression
Another condition with a gender association
Source
Tax_name
tax_rank
Taxon
Male
Female
Male_Chi2
FeMale_Chi2
thryve
Thermodesulfobacteria
phylum
200940
increases
increases
227.7557
148.4336
thryve
Parabacteroides distasonis
species
823
decrease
increases
9.118356
13.46941
thryve
Eubacterium oxidoreducens
species
1732
decrease
increases
12.99507
6.76
biomesight
Rhodothermales
order
1853224
increases
increases
121.2002
91.125
biomesight
Rhodothermia
class
1853222
increases
increases
121.2002
91.125
biomesight
Thermodesulfobacteria
phylum
200940
increases
increases
223.4402
189.2431
biomesight
Rhodothermaeota
phylum
1853220
increases
increases
121.2002
91.125
thryve
Lactobacillus rogosae
species
706562
decrease
decrease
23.88368
12.12781
Symptom: Problems remembering things
This is one of the characteristics of ME/CFS, Long Covid, etc
Source
Tax_name
tax_rank
Taxon
Male
Female
Male_Chi2
FeMale_Chi2
thryve
Thermodesulfobacteria
phylum
200940
increases
increases
316.4446
120.0944
biomesight
Rhodothermales
order
1853224
increases
increases
171.7445
133.3333
biomesight
Rhodothermia
class
1853222
increases
increases
171.7445
133.3333
biomesight
Thermodesulfobacteria
phylum
200940
increases
increases
369.0078
289.0992
biomesight
Odoribacteraceae
family
1853231
increases
increases
12.79311
7.962632
biomesight
Rhodothermaeota
phylum
1853220
increases
increases
171.7445
133.3333
biomesight
Acetivibrio
genus
35829
decrease
increases
9.180865
17.49208
biomesight
Odoribacter
genus
283168
increases
increases
9.334949
12
biomesight
Acetivibrio alkalicellulosi
species
320502
decrease
increases
9.180865
19.95636
biomesight
Hathewaya histolytica
species
1498
decrease
increases
9.180865
7.262051
biomesight
Hathewaya
genus
1769729
decrease
increases
9.180865
7.262051
biomesight
[Clostridium] thermoalcaliphilum
species
29349
increases
increases
7.35
6.880909
thryve
Intestinimonas
genus
1392389
decrease
increases
16
8.552727
thryve
Intestinimonas butyriciproducens
species
1297617
decrease
increases
16.48646
9.992258
ubiome
Bacteroides sp. EBA5-17
species
447029
increases
decrease
9.055577
7.314286
Symptom: Worsening of symptoms with stress.
Another common symptom of ME/CFS
Source
Tax_name
tax_rank
Taxon
Male
Female
Male_Chi2
FeMale_Chi2
thryve
Thermodesulfobacteria
phylum
200940
increases
increases
282.4023
185.22
biomesight
Thermoanaerobacterales Family III. Incertae Sedis
family
543371
decrease
increases
22.00454
8.491649
biomesight
Sharpea
genus
519427
increases
increases
17.55625
12.38345
biomesight
Hathewaya
genus
1769729
decrease
increases
16.98612
11.70814
biomesight
Rhodothermales
order
1853224
increases
increases
142.9353
188.8704
biomesight
Hathewaya histolytica
species
1498
decrease
increases
16.98612
11.70814
biomesight
Sharpea azabuensis
species
322505
increases
increases
17.55625
12.97965
biomesight
Rhodothermia
class
1853222
increases
increases
142.9353
188.8704
biomesight
Thermodesulfobacteria
phylum
200940
increases
increases
352.2616
362.7038
biomesight
Acetivibrio alkalicellulosi
species
320502
decrease
increases
12.65818
8.491649
biomesight
Rhodothermaeota
phylum
1853220
increases
increases
142.9353
188.8704
biomesight
Acetivibrio
genus
35829
decrease
increases
12.65818
8.491649
Other Symptoms with Significant Gender Differences in patterns
Immune Manifestations: Abdominal Pain
Sleep: Unrefreshed sleep
Comorbid: High Anxiety
General: Fatigue
Neurological-Audio: hypersensitivity to noise
DePaul University Fatigue Questionnaire : Unrefreshing Sleep, that is waking up feeling tired
DePaul University Fatigue Questionnaire : Fatigue
Neurocognitive: Brain Fog
Neurocognitive: Problems remembering things
DePaul University Fatigue Questionnaire : Anxiety/tension
It is not all strains of Staphylococcus aureus, but about 10% of the strains.
Normally, I look at modifying the gut microbiome — but many items are likely to help. So the question becomes, what are possible for use as skin ointments?
From the list of inhibitors, likely candidates are:
Zinc or silver ointments
acetic acid (vinegar) – likely diluted, possibly with a sprayer
The following available as oils, mixed with creams:
A person with this issue looked over the list and found that the items in the above list that she has tried, reduced the itch.
The obvious cheapest solution to try is simple: a shower with soap (ideally antibacterial soap). Followed by using a spray bottle with vinegar that is allowed to dry on the skin.






Recent Comments