In common medical practice, bacteria ranges tend to be very random. Often it becomes values above or below average plus/minus 1.96 Standard Deviations. Bacteria are abnormal (i.e. are not a normal or bell curve distribution).
My training is in statistics and operations research. This post and other posts are intended to ask “why not do things this way” and to inspire lifting the bar in approaching the microbiome.
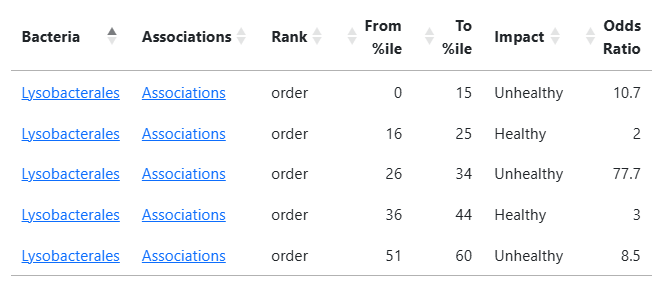
From some 7,500 samples I computed statistical ranges for 2,470 different bacteria with a threshold of Chi2 > 6.6 (around p < 0.01). The higher the odds, the more significant. The ranges apply only is the bacteria was detected in the sample. The page is available here.
So far, most of the numbers appear to follow common sense (see Highlights above). Bacteria with multiple ranges is more of a challenge to understand and exposes a concept close to a “Yin/Yang” of the microbiome.
A more interesting one is: Lysobacterales. The low odds ratios for healthy hints that we may wish to discard those values resulting in < 60 as unhealthy.
Adding to Microbiome Prescription
I am planning to add it as a bacteria selection method using a higher Chi2 value then used for the demo table. Stay tune.
I will be using P < 0.001 to safely identify the bacteria of concern.
The organization Vitract.com recently referenced Jona Health during a conference call, noting that Jona’s platform reportedly incorporates approximately 200,000 studies. This claim prompted closer examination, particularly regarding how such figures are defined and communicated.
Public-facing descriptions of Jona’s methodology indicate that its system has “read” approximately 220,000 peer-reviewed studies, with an ongoing ingestion rate of roughly 2,000 new studies per month as microbiome research evolves. However, the distinction between studies that are “read” versus those that are critically evaluated and actively utilized is nontrivial. The use of the term “read” appears to function as a marketing construct, potentially conflating exposure to literature with meaningful incorporation into a validated analytical framework.
For comparative purposes, equivalent metrics from the Microbiome Prescription database demonstrate substantially greater scale and curation rigor. The system has processed a total of 2,953,169 studies—an order of magnitude greater than the figures cited above. Recent weekly ingestion rates further illustrate this difference:
May 29, 2026: 5,871 new studies
May 22, 2026: 4,984 new studies
May 15, 2026: 5,584 new studies
May 8, 2026: 5,582 new studies
Importantly, each study undergoes manual review prior to inclusion, reflecting the inherent complexity and nuance of microbiome literature that cannot be reliably interpreted through automated methods alone.
More critical than raw ingestion counts is the subset of studies that yield actionable, high-quality data. Within the Microbiome Prescription system, 21,391 studies have been identified as containing usable information and are actively incorporated into the knowledge base. These curated studies underpin approximately 14,518,553 PubMed-derived data points within the expert system. In addition, the platform includes approximately 71,000 experimentally derived bacterial interaction data points sourced from raw datasets.
These distinctions underscore the importance of evaluating not only the quantity of literature processed but also the depth of curation and the proportion of data that is methodologically sound and practically usable.
In conclusion, numerical claims regarding literature scale should be interpreted with caution, particularly when used in marketing contexts. The critical question is not how many studies are nominally “read,” but rather how many are rigorously evaluated and meaningfully integrated into a reliable analytical framework. Microbiome Prescription operates as a not-for-profit, citizen science initiative with the explicit goal of advancing microbiome-informed decision-making through careful curation and transparent methodology, rather than promotional positioning.
Bottom Line
As with all things marketing “Where’s the beef?” and not the hype. Microbiome Prescription is a not profit seeking citizen science endeavor seeking to improve the use of the microbiome.
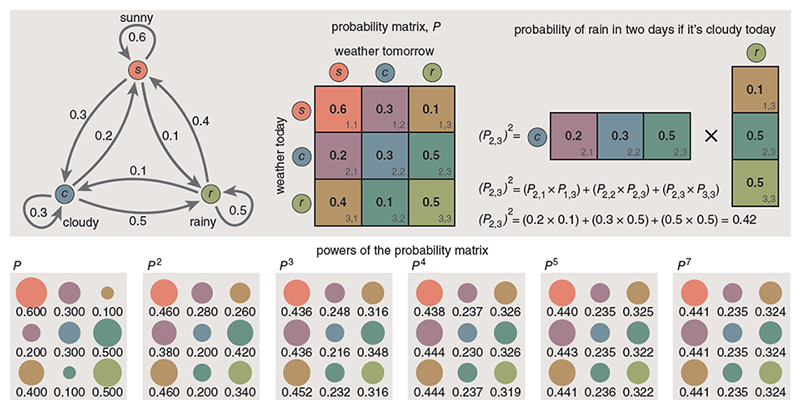
During my Probability and Statistics studies in the early 1970s, I developed a strong interest in Markov chains. The core idea behind a Markov process is straightforward: the next state of a system depends only on its current state and a set of transition probabilities. Given that the microbiome is full of interactions, it seems the ideal model.
In practical terms, this can be represented as a matrix—similar to an Excel spreadsheet—where each column represents an intervention or event, and each row represents a state variable. When a given event occurs, its associated column of values describes how each variable is expected to shift.
To illustrate this concept in a microbiome context, consider a simplified model using R²-derived relationships between probiotics and bacterial taxa. In this matrix, each value represents the directional influence of a probiotic on a specific bacterium, where zero indicates no measurable effect.
Example interaction matrix:
Target Bacteria
Pro 1
Pro 2
Pro 3
Pro 4
A
-0.23
0.44
0.11
0.00
B
0.2
0.32
-0.22
0.14
C
0.18
-0.11
0.11
0.12
D
-0.31
0.13
0.22
-0.28
From this, we can evaluate each probiotic independently by applying its column to the current microbiome state and observing whether each bacterium moves toward or away from its target range.
A simplified qualitative interpretation might look like this:
Target Bacteria
Pro 1
Pro 2
Pro 3
Pro 4
A
n/a
worse
worse
need improvement
B
worse
worse
better
worse
C
n/a
worse
better
better
D
n/a
worse
worse
better
In this example, Probiotic 1 appears to be the best initial choice, as it minimizes negative outcomes relative to the others.
Once the first intervention is applied, we update the microbiome to its predicted new state. This updated state becomes the input for the next evaluation cycle. For instance, after adjusting bacterium B, we might find:
Target Bacteria
Pro 1
Pro 2
Pro 3
Pro 4
B
worse
worse
better
n/a
This suggests that Probiotic 3 is the most suitable follow-up intervention for B.
In practice, this process must be applied across all bacteria simultaneously—including those currently within the acceptable range—to generate a full predicted microbiome after each intervention. The goal is to evaluate all candidate substances and select the one that produces the greatest overall improvement.
By iterating this process, we can construct a sequence of interventions such as:
Herb 1
Probiotic 2
Diet Change 3
Once a candidate sequence is identified, it is important to test whether the order of interventions materially affects the outcome. This can be done by randomizing the sequence and comparing predicted results. If the sequence proves immaterial, then some interventions may be applied concurrently rather than sequentially.
That is the basic concept, the mathematics are a little more complex. How do you estimate the amount of shift?
A Rule of Thumb
My working assumptions are:
All bacterial abundances are converted to percentiles, with defined target percentile ranges.
For probiotics, assume a ±10 percentile shift scaled by the R² relationship for a given bacterium.
For other substances, estimate impact based on available studies:
One study: approximately 1 percentile shift.
Mixed evidence: net effect equals positive studies minus negative studies (e.g., 8 positive and 2 negative yields a 6 percentile shift).
Cap the maximum effect at 10 percentiles regardless of study volume.
These values are approximations and likely imperfect, but they provide a consistent framework given current data limitations.
Method Summary
Convert microbiome measurements into percentiles.
Identify bacteria that fall outside their target ranges.
Apply each candidate intervention to the current state and compute the predicted microbiome.
Select the intervention that produces the greatest reduction in out-of-range bacteria (or other chosen objective function).
Update the microbiome to this predicted state.
Repeat the process until all bacteria are within range or no further improvement can be achieved.
The result is an ordered sequence of interventions designed to progressively normalize the microbiome. Questions of dosage, duration, and clinical appropriateness are intentionally excluded from this model and should be addressed by qualified professionals.
This is a major transition from “Let us try this and see what happens” to an objective/numeric prioritization based on a reasonable mathematic model. Odds are, that the results will be better for the patient.
I am going to use microbiome data from the 1998 Alison Hunter Memorial Foundation conference on ME/CFS. The pattern reported is very common with sufferers of ME/CFS and Long COVID. I will use that report to phrase some questions. In theory, this is what could have been suggested by a progressive MD using AI in 1999. At the bottom are some comments from reviewing these responses. I have not mentioned the condition to the AI.
With a microbiome with decreased E.Coli (50% below normal), Bifidobacterium, Lactobacillus AND increased klebsiella/Enterobacter and Enterococcus how should a patient diet and supplements be changed?
With a microbiome with decreased E.Coli (50% below normal), Bifidobacterium, Lactobacillus AND increased klebsiella/Enterobacter and Enterococcus what prescription drugs be given?
Remember, with multiple answers from different experts:
Just go there and copy the above questions for full details including references.
A high-fiber, plant-rich diet is the most evidence-supported single intervention — it creates SCFA production, lowers colonic pH, and suppresses Enterobacteriaceae overgrowth
Prebiotics (inulin, FOS, GOS) selectively stimulate Bifidobacterium and Lactobacillus and attenuate Enterobacteriaceae blooms
Berberine shows antimicrobial activity against Klebsiella and Enterococcus at gut-relevant concentrations but caution is warranted as it may paradoxically increase Enterococcus in some contexts
Avoid refined carbohydrates, simple sugars, and ultra-processed foods — these preferentially fuel Enterobacteriaceae and Enterococcus growth
Importantly, note that the low E. coli finding is likely a relative reflection of the Enterobacteriaceae dysbiosis, not an independent deficiency requiring specific treatment
Simple sugars feed pathogenic bacteria and worsen dysbiosis
Feed Bifido & Lactobacillus
High diverse fiber from non-starchy veggies: leafy greens, broccoli, cabbage, zucchini, cucumbers, bell peppers, mushrooms, asparagus (if tolerated), artichokes
Fiber → short-chain fatty acids (SCFAs) that protect against pathogens and support beneficial bacteria
Low-FODMAP prebiotics if SIBO symptoms: start with psyllium husk, small amounts of oats, berries, citrus, carrots, green bananas
Supports good bacteria without excessive fermentation; high-FODMAP prebiotics (garlic/onion/jerusalem artichoke) can worsen SIBO initially
Use under professional guidance only; cycle (e.g., 2–4 weeks), then re-test. Avoid long-term use.
E. coli probiotic (Mutaflor/Symbioflor)
Contains specific E. coli Nissle strain to replenish low E. coli; used clinically for gut balance
Discuss with clinician; some protocols pulse then maintain
Prescription
No specific “best” prescription drug is indicated purely by this microbiome pattern; if treatment is needed, clinicians usually treat it as small intestinal/colonic bacterial overgrowth with short courses of narrowest‑possible antibiotics guided by symptoms, cultures, and resistance patterns, plus a prescription‐grade probiotic such as E. coli Nissle in some cases.
A Mediterranean-style dietary pattern rich in fruits, vegetables, whole grains, legumes, nuts, olive oil, and fish is the best-supported overall framework. This pattern is associated with favorable gut microbial profiles, increased fiber-degrading beneficial bacteria (including Faecalibacterium and Ruminococcus), and lower subclinical intestinal inflammation. [1-3] Ultraprocessed foods should be minimized, as they are linked to dysbiosis. [1]
Key dietary components to emphasize:
Prebiotic fibers — particularly fructans (inulin, FOS) and galacto-oligosaccharides (GOS) — have the strongest evidence for selectively increasing Bifidobacterium and Lactobacillus abundance. A meta-analysis of 64 RCTs (n=2099) demonstrated significantly higher Bifidobacterium (SMD 0.64, P<0.00001) and Lactobacillus (SMD 0.22, P=0.02) with dietary fiber interventions, with fructans and GOS showing the greatest effect. Food sources include chicory root, garlic, onions, leeks, asparagus, bananas, and Jerusalem artichokes. [4]
Resistant starch (found in cooked-and-cooled potatoes/rice, green bananas, legumes, and whole grains) acts as a fermentable substrate that promotes Bifidobacterium and Lactobacillus growth and increases butyrate production. [5-6]
Polyphenol-rich foods — berries, apples, grapes, green tea, dark chocolate, and extra-virgin olive oil — may help suppress Enterobacteriaceae (including Klebsiella). In vivo studies show resveratrol, phloretin (apples/strawberries), and other polyphenols can reduce Enterobacteriaceae levels while promoting beneficial bacteria, though most data are from animal models. [7-8]
Lactose restriction may be worth considering given the Enterococcus overgrowth. A recent study in a transplant unit found that implementing a lactose-free diet significantly reduced VRE carriage (16% → 3.6%), consistent with evidence that lactose can fuel Enterococcus growth. [9]
Fermented foods — yogurt, kefir, kimchi, sauerkraut, miso — provide live Lactobacillus and Bifidobacterium species that can transiently colonize the gut and modulate the microbiome. A high-fermented-food diet has been associated with increased microbial diversity and decreased inflammatory markers. [10-12]
Supplement Recommendations
Probiotic supplementation with multi-strain formulations containing Bifidobacterium (B. longum, B. lactis, B. bifidum) and Lactobacillus (L. rhamnosus, L. acidophilus, L. plantarum, L. paracasei) species is the most direct approach to replenishing depleted populations. L. paracasei CNCM I-3689 has specifically been shown to reduce Enterococcus persistence and promote Bacteroidetes recovery in a dysbiosis model. Probiotics suppress pathogens through competitive exclusion, bacteriocin production, pH lowering, and gut barrier enhancement. [13-17]
Prebiotic supplements — inulin-type fructans (ITF) and arabinoxylan-oligosaccharides (AXOS) — selectively stimulate Bifidobacterium growth and promote butyrate production through cross-feeding with butyrate-producing bacteria. A synbiotic approach (combining prebiotics with probiotics) may enhance probiotic colonization and provide synergistic benefits. [14][18-19]
Butyrate supplementation or butyrate-promoting strategies may help strengthen the gut barrier and create an environment less favorable to facultative anaerobes like Klebsiella and Enterococcus, as butyrate lowers colonic pH and supports epithelial integrity. [16][18]
Prescription
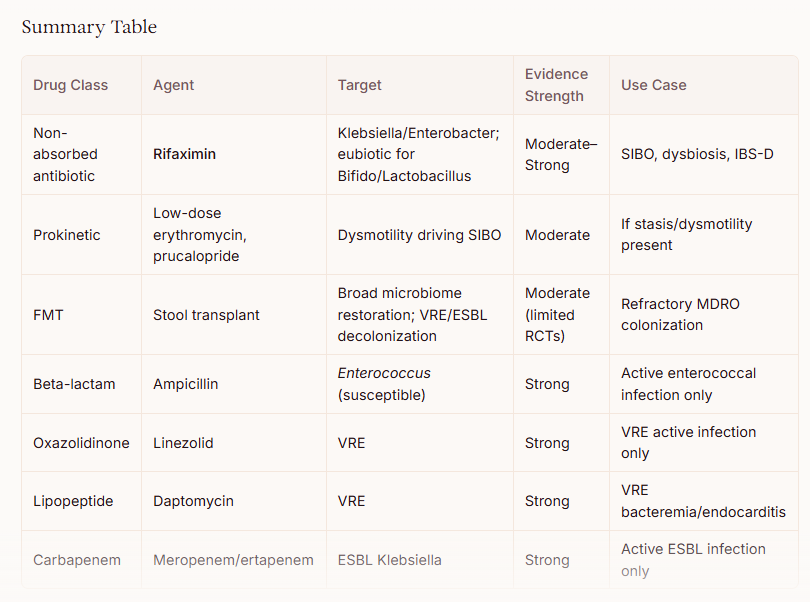
It is important to emphasize that no prescription drugs are FDA-approved specifically for treating gut dysbiosis as identified by stool microbiome testing. The clinical significance of specific bacterial abundance thresholds on commercial microbiome panels remains debated, and treatment should be guided by symptoms and clinical context rather than microbiome test results alone. That said, several prescription medications can be considered based on the specific dysbiotic pattern described:
Rifaximin (Xifaxan) — The Most Relevant Prescription Option
Rifaximin 550 mg TID for 14 days is the prescription drug with the strongest rationale for this dysbiotic profile. Unlike conventional antibiotics, rifaximin has unique “eubiotic” properties — it selectively increases Lactobacillus and Bifidobacterium abundance while suppressing pathobionts, without significantly disrupting overall microbial diversity. [1-3] Metagenomic analyses have confirmed a significant increase in Lactobacilli persisting in the short term after rifaximin treatment, independent of the underlying disease. [2] Rifaximin also reduces bacterial virulence and translocation, and has anti-inflammatory effects via PXR nuclear receptor activation. [4] The ACG recommends rifaximin as first-line therapy for SIBO at 550 mg TID for 14 days, with an overall ~70% eradication rate. [5-8] However, SIBO is not an FDA-approved indication, and insurance coverage may be challenging. [5]
E. coli Nissle 1917 (Mutaflor)
For the specific finding of depleted E. coli, E. coli Nissle 1917 (marketed as Mutaflor) is a prescription-grade probiotic available in some countries (Germany, Canada) but not FDA-approved in the United States. It is the only probiotic recommended in ECCO guidelines as an effective alternative to mesalazine for maintenance of remission in ulcerative colitis. [9] EcN stimulates human β-defensin 2 production, protects the mucosal barrier, and has demonstrated antagonistic effects against Salmonella, Shigella, and other invasive commensals. [10-11] It directly addresses the depleted commensal E. coli niche.
If the Klebsiella/Enterobacter overgrowth is causing clinical infection (not merely colonization), targeted antibiotics may be warranted:
For susceptible Enterobacterales: fluoroquinolones (ciprofloxacin), TMP-SMX, or amoxicillin-clavulanate based on susceptibility testing [5-6]
For AmpC-producing Enterobacter: cefepime is recommended by IDSA guidelines [12-13]
For ESBL-producing organisms: carbapenems (meropenem, imipenem) are preferred for serious infections [14-15]
However, broad-spectrum antibiotics for asymptomatic colonization are not recommended, as they would likely worsen the underlying dysbiosis. [6]
Antibiotics Targeting Enterococcus Overgrowth
Similarly, Enterococcus overgrowth in the absence of clinical infection does not typically warrant antibiotic treatment. If treatment is needed:
Ampicillin/amoxicillin is preferred when susceptible [16]
For VRE: linezolid or daptomycin have demonstrated clinical efficacy [16]
A novel decolonization approach combining bowel preparation with polyethylene glycol, oral linezolid + non-absorbable daptomycin, followed by Lactobacillus rhamnosus GG to maintain colonization resistance, has shown success in clearing VRE carriage in a small case series. [17]
Low-fermentation, low-starch approach initially: Klebsiella and Enterobacter thrive on resistant starch and certain fibers, producing gas, LPS, and histamine. A temporary low-FODMAP + low-starch phase (2–4 weeks) helps reduce their load.
Prebiotics with caution: Instead of high-FODMAP fibers (inulin, chicory, large amounts of legumes), use acacia fiber or PHGG (partially hydrolyzed guar gum) in small, increasing doses—these favor Bifidobacteria without overly feeding Klebsiella.
Polyphenol-rich foods: Berries, green tea, pomegranate, dark chocolate (>70%), and olive oil. Polyphenols inhibit Enterococcus and Klebsiella while promoting Lactobacillus.
Animal protein + low-carb vegetables: Grass-fed meat, eggs, fish, and leafy greens—limited fermentation in the colon.
Fermented foods if tolerated: Small amounts of sauerkraut, kimchi, or kefir (start with 1 tbsp) can reintroduce beneficial strains, but watch for histamine reactions due to possible gut permeability.
Colostrum or immunoglobulin G (IgG) – binds LPS from Enterobacter and helps clear pathobionts.
Butyrate (tributyrin or resistant starch only after pathogens reduced) – feeds colonocytes, suppresses Enterococcus.
3. Special considerations
Low E. coli means reduced production of colicins (natural antimicrobials against Klebsiella). In some contexts, supplementing a non-pathogenic E. coli strain (like E. coli Nissle 1917, Mutaflor) can be beneficial, but use only after pathogen load is reduced, and under medical guidance (risk of UTI in susceptible patients).
Low Bifidobacterium and Lactobacillus → consider human milk oligosaccharides (HMOs) like 2’FL (1–2 g/day) – very specific prebiotic for Bifidobacteria, minimally used by Klebsiella.
Biotin and B vitamins – overgrowth of Klebsiella/Enterococcus consumes biotin; supplementation may help host metabolism.
Prescription
? 1. Treating the Overgrowth: A Targeted Approach
Prescription antibiotics are only indicated if the overgrowth of Klebsiella, Enterobacter, or Enterococcus is causing a confirmed active infection (e.g., urinary tract infection, pneumonia, bacteremia) or a diagnosed condition like Small Intestinal Bacterial Overgrowth (SIBO).
If treatment is necessary, the choice is not one-size-fits-all. Because these bacteria have high rates of antibiotic resistance, therapy must be guided by antibiotic susceptibility testing (culture and sensitivity) .
Overgrown Organism
Condition
Potential Prescription Approach
Klebsiella / Enterobacter
Confirmed SIBO or specific infection
Rifaximin is a non-absorbable antibiotic often used for SIBO, but studies show its effectiveness varies significantly. It inhibits only about 43.6% of Klebsiella and 34.8% of Enterobacter strains . For systemic infections, other antibiotics like third-generation cephalosporins, carbapenems, or fluoroquinolones may be used, but this depends entirely on resistance testing .
Enterococcus
Confirmed infection (e.g., UTI, bacteremia)
Ampicillin or amoxicillin are the agents of choice for susceptible strains . High-level resistance is common, especially with E. faecium, often requiring infectious disease consultation for drugs like linezolid or daptomycin .
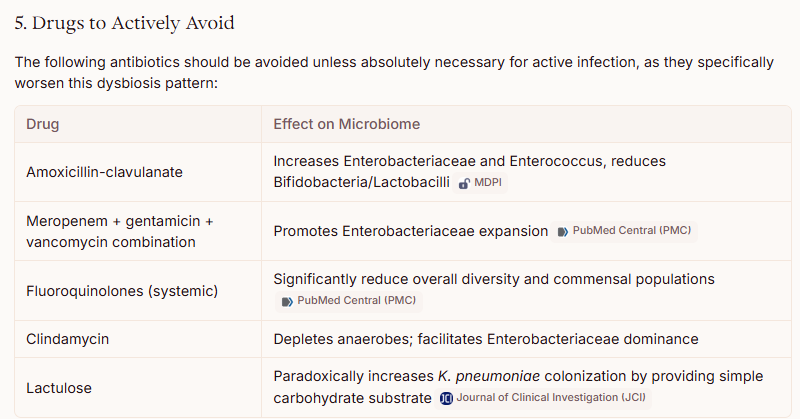
Important note on antibiotics: Using systemic antibiotics to target the bacteria in the gut lumen is generally avoided. It will likely worsen the underlying dysbiosis by further reducing beneficial Bifidobacterium and Lactobacillus, which are already low .
? 2. Restoring the Microbiome: Fecal Microbiota Transplantation (FMT)
Rather than using a drug to kill the “bad” bacteria, a more logical approach to restoring the balance of E. coli, Bifidobacterium, and Lactobacillus is Fecal Microbiota Transplantation (FMT).
FMT involves infusing healthy donor stool into the patient’s intestine to directly restore a diverse and balanced microbiome. However, its use is currently restricted by clinical guidelines:
Approved Use: FMT is strongly recommended by the American Gastroenterological Association (AGA) for patients with recurrent Clostridioides difficile infection (CDI) .
Off-Label and Experimental: For the specific pattern of dysbiosis you described (without a CDI diagnosis), FMT is not recommended outside of clinical trials . While Chinese expert consensus suggests it may be explored for severe gut dysbiosis, this is not a standard or approved practice in most other regions .
? A Note on E. coli Restoration
You noted that E. coli is 50% below normal. While E. coli is often thought of as a pathogen, certain strains are a normal part of a healthy gut microbiome. A specific probiotic called E. coli Nissle 1917 has been studied for its ability to support gut health. However, this is generally available as a medical food or supplement, not a standard prescription drug, and should only be used under the guidance of a physician. This is not a standard treatment in most clinical settings.
The most evidence-supported approach is usually to encourage beneficial bacteria through diet rather than trying to eliminate specific organisms.
Increase prebiotic fibers gradually
These preferentially support Bifidobacterium and other beneficial microbes:
Onions
Garlic
Leeks
Asparagus
Jerusalem artichokes
Oats
Barley
Legumes (if tolerated)
Green bananas
Cooked-and-cooled potatoes or rice (resistant starch)
If bloating is severe, introduce these slowly.
Increase diverse plant intake
Studies consistently associate greater microbial diversity with consuming a wide variety of plant foods.
A common target is:
25–40 g/day fiber (depending on tolerance and medical conditions)
20–30 different plant foods per week
Consider fermented foods
If tolerated:
Yogurt with live cultures
Kefir
Sauerkraut
Kimchi
Miso
These may help increase exposure to beneficial microbes, though they do not necessarily permanently colonize the gut.
Limit factors associated with Enterobacteriaceae overgrowth
Klebsiella and Enterobacter belong to the family Enterobacteriaceae.
Potentially helpful:
Reduce ultra-processed foods.
Reduce excessive refined sugars.
Moderate alcohol intake.
Ensure adequate fiber.
Evidence for aggressively restricting carbohydrates specifically to suppress these organisms is limited.
Supplements that may be discussed with a clinician
Bifidobacterium-containing probiotics
Given low Bifidobacterium, strains commonly studied include:
Bifidobacterium longum
Bifidobacterium lactis
Bifidobacterium bifidum
Lactobacillus-containing probiotics
Given low Lactobacillus, strains commonly studied include:
Lactobacillus rhamnosus GG
Lactobacillus plantarum
Lactobacillus reuteri
Prebiotics
Often more effective at increasing resident beneficial bacteria than probiotics alone:
Inulin
FOS (fructooligosaccharides)
GOS (galactooligosaccharides)
Resistant starch
GOS in particular is frequently associated with increases in Bifidobacterium.
Partially hydrolyzed guar gum (PHGG)
PHGG has some evidence for:
Increasing beneficial bacteria
Improving constipation and IBS symptoms in some people
Being better tolerated than some other fibers
Things to be cautious about
Antimicrobial supplements
Products marketed to “kill Klebsiella” or “eradicate Enterococcus” (oregano oil, berberine, etc.) can sometimes further disrupt the microbiome. Whether they are appropriate depends on the clinical situation and should not be based solely on a stool microbiome report.
Very restrictive diets
Long-term low-fiber or highly restrictive diets may further reduce Bifidobacterium and Lactobacillus populations.
Prescription
There is no standard prescription drug regimen that should be given solely because a microbiome report shows low E. coli, low Bifidobacterium, low Lactobacillus, and elevated Klebsiella/Enterobacter and Enterococcus.
In current clinical practice, doctors generally treat diseases and symptoms, not microbiome composition alone. A stool microbiome test cannot reliably determine which prescription drug is appropriate.
Summary
First unfortunate fact is that most retail and many clinical microbiome tests do not accurately measure E.Coli.In my own experience, the E.Coli probiotics cited several times above were very effective (with the warning that it can cause a major die off)
Concerning antibiotics, the Jadin approach of rotating with just one course per month is recommended.
Recent Comments