| Symptom Name | Shannon | Simpson | Chao | Shannon Rank | Simpson Rank | Chao Rank | Obs |
| Asymptomatic: Minor Health Issues (a few symptoms only) | 1.931 | 0.048 | 4856.983 | 50.7 | 40.5 | 26 | 58 |
| Official Diagnosis: Ulcerative colitis | 1.705 | 0.08 | 5547.478 | 35.2 | 54.7 | 27.5 | 23 |
| Neurological: Spatial instability and disorientation | 2.049 | 0.072 | 5981.804 | 55.2 | 51.8 | 29.5 | 56 |
| Asymptomatic: No Health Issues | 2.012 | 0.066 | 8924.899 | 53.7 | 45.4 | 29.6 | 188 |
| Joint: Sudden and severe episodes of pain | 2.185 | 0.058 | 6160.833 | 58.5 | 48.5 | 30.6 | 48 |
| Neuroendocrine: Feeling like you have a high temperature | 1.967 | 0.075 | 6704.373 | 50.9 | 53.8 | 32.6 | 75 |
| Autonomic: Blurred or tunnel vision after standing | 1.907 | 0.054 | 6777.784 | 49.9 | 42.1 | 33.2 | 51 |
| Neuroendocrine Manifestations: abnormal appetite | 2.012 | 0.06 | 7345.455 | 53.2 | 44.8 | 34.1 | 77 |
| Neurological: fasciculations | 1.863 | 0.055 | 8333.9 | 47.9 | 43.3 | 34.2 | 70 |
| Onset: over 31 years since onset | 1.657 | 0.089 | 7253.219 | 38.7 | 47.2 | 34.6 | 32 |
| Neurological: Confusion | 1.918 | 0.067 | 7627.785 | 49.4 | 48.4 | 35 | 93 |
| Immune Manifestations: Diarrhea | 1.936 | 0.075 | 12798.57 | 48.9 | 52.4 | 35 | 178 |
| Neuroendocrine: Feeling like you have a low temperature | 1.963 | 0.069 | 7193.583 | 51.5 | 48 | 35.3 | 60 |
| Neurological-Vision: Blurred Vision | 1.867 | 0.059 | 7616.119 | 46.4 | 44 | 35.4 | 151 |
| Autonomic: Graying or blacking out after standing | 2.037 | 0.058 | 7603.086 | 55.9 | 45.3 | 35.5 | 35 |
| Neuroendocrine: Chills or shivers | 1.813 | 0.083 | 7818.411 | 45.2 | 52.6 | 35.6 | 56 |
| Neuroendocrine Manifestations: recurrent feelings of feverishness | 1.975 | 0.059 | 8146.892 | 51.2 | 48 | 36.2 | 65 |
| Neurological: Difficulty processing information (Understanding) | 1.9 | 0.071 | 8249.883 | 48.3 | 48.1 | 36.3 | 197 |
| Neuroendocrine Manifestations: Neuralgia | 1.91 | 0.067 | 10588.14 | 47.2 | 49.6 | 36.4 | 44 |
| Neurological-Sleep: Chaotic diurnal sleep rhythms (Erratic Sleep) | 2.009 | 0.059 | 11433.45 | 51.6 | 43.4 | 36.5 | 231 |
| Neuroendocrine: Temperature fluctuations throughout the day | 1.957 | 0.065 | 7482.103 | 49.8 | 50.3 | 36.5 | 68 |
| Neurological: Impairment of concentration | 1.981 | 0.059 | 10024.12 | 51.6 | 43.8 | 36.8 | 345 |
| Immune Manifestations: tender lymph nodes | 1.981 | 0.057 | 8632.264 | 51.6 | 43.2 | 36.9 | 110 |
| Sleep: Sleeping all day and staying awake all night | 2.07 | 0.074 | 7632.563 | 56.3 | 54.3 | 37.1 | 32 |
| Autonomic: Nausea | 1.911 | 0.07 | 8689.976 | 48.8 | 51.7 | 37.1 | 85 |
| Neurological: Short-term memory issues | 2.001 | 0.062 | 8048.832 | 52.5 | 45.6 | 37.2 | 220 |
| Neurological: Neuropathy | 1.926 | 0.051 | 11019.76 | 48.2 | 41.4 | 37.5 | 71 |
| Official Diagnosis: Metabolic Syndrome | 1.748 | 0.067 | 8212.524 | 43.3 | 44.1 | 37.6 | 21 |
| DePaul University Fatigue Questionnaire : Fever & Chills | 1.728 | 0.102 | 9503.591 | 40.5 | 56.2 | 37.6 | 22 |
| Neuroendocrine: Lack of appetite | 1.946 | 0.064 | 9142.984 | 50.5 | 44.5 | 37.6 | 61 |
| Neurological: Executive Decision Making (Difficulty making) | 2.006 | 0.061 | 11185.76 | 52.4 | 44.4 | 37.7 | 289 |
| Immune: Sensitivity to smell/food/medication/chemicals | 1.979 | 0.067 | 9401.077 | 50 | 47.4 | 37.8 | 194 |
| Immune Manifestations: Genitorinary / Nocturia – Urinary issues | 2.085 | 0.07 | 7840.608 | 56 | 51.7 | 37.8 | 51 |
| Neurological: emotional overload | 2.065 | 0.066 | 8548.668 | 54.8 | 49.5 | 37.8 | 196 |
| Neuroendocrine Manifestations: Muscle weakness | 1.95 | 0.062 | 8751.741 | 49.6 | 46.2 | 37.9 | 216 |
| General: Myalgia (pain) | 2.009 | 0.059 | 13779.4 | 52.4 | 46.3 | 37.9 | 216 |
| Onset: 2000-2010 | 1.949 | 0.064 | 8244.574 | 49.8 | 47.3 | 38 | 122 |
| Neuroendocrine: Lost or gained weight without trying | 1.993 | 0.07 | 8316.814 | 51.6 | 50.7 | 38.2 | 118 |
| Immune Manifestations: new food sensitivities | 1.983 | 0.067 | 9932.414 | 50.6 | 47.7 | 38.2 | 157 |
| Onset: Gradual | 2.043 | 0.062 | 13699.92 | 55 | 47.6 | 38.2 | 172 |
| Neurological: High degree of Empathy before onset | 1.975 | 0.07 | 8434.465 | 51 | 51.1 | 38.3 | 86 |
| Comorbid-Mouth: Dry Mouth | 1.856 | 0.055 | 8600.484 | 45.7 | 41.3 | 38.4 | 124 |
| Neuroendocrine Manifestations: subnormal body temperature | 1.999 | 0.057 | 12240.34 | 52.1 | 40.8 | 38.4 | 235 |
| Neurological-Vision: Acquired or exertional dyslexia | 1.911 | 0.076 | 8275.381 | 49.7 | 54.1 | 38.5 | 21 |
| Neuroendocrine Manifestations: Dry Eye (Sicca or Sjogren Syndrome) | 1.873 | 0.056 | 10422.66 | 45.7 | 42.4 | 38.5 | 136 |
| Neurocognitive: Slowness of thought | 1.958 | 0.061 | 12656.61 | 50.6 | 44.9 | 38.6 | 361 |
| Neuroendocrine: Sweating hands | 1.91 | 0.091 | 8249.438 | 48.2 | 56.6 | 38.7 | 48 |
| Pain: Chest pain | 2.124 | 0.069 | 10019.41 | 58.3 | 52.3 | 38.7 | 54 |
| Blood Type: B Positive | 1.753 | 0.085 | 8271.444 | 40.4 | 55.8 | 38.7 | 36 |
| Neurological-Vision: inability to focus eye/vision | 1.946 | 0.061 | 12655.22 | 49.6 | 42.1 | 38.8 | 224 |
| Neurological: Difficulty reading | 1.966 | 0.066 | 11904.13 | 50.5 | 45.1 | 39 | 283 |
| Neurological-Vision: Impaired Depth Perceptions | 1.917 | 0.093 | 9048.091 | 46.3 | 49.7 | 39 | 33 |
| Asymptomatic: Live in house with person with probable microbiome dysfunction | 1.954 | 0.057 | 9649.831 | 50.1 | 43.2 | 39 | 71 |
| Neurocognitive: Absent-mindedness or forgetfulness | 1.989 | 0.064 | 12091.81 | 51.5 | 45.6 | 39 | 389 |
| Pain: Pain or aching in muscles | 1.958 | 0.068 | 12992.8 | 49.7 | 51.1 | 39 | 182 |
| Comorbid: Raynaud’s syndrome (Skin discoloration) | 1.917 | 0.052 | 15270.64 | 48 | 44.7 | 39 | 33 |
| Autonomic Manifestations: cardiac arrhythmias | 1.955 | 0.054 | 9592.803 | 51.4 | 40.8 | 39 | 61 |
| Pain: Myofascial pain | 2.009 | 0.064 | 19489.55 | 53 | 47.8 | 39.1 | 89 |
| Neuroendocrine Manifestations: Excessive adrenaline | 2.027 | 0.064 | 8756.423 | 53.6 | 50.5 | 39.1 | 78 |
| Official Diagnosis: Inflammatory Bowel Disease (IBD) | 1.906 | 0.093 | 8392.806 | 47.6 | 58.5 | 39.2 | 31 |
| Pain: Joint pain | 2.003 | 0.066 | 10602.51 | 51.9 | 50.6 | 39.3 | 178 |
| Joint: Stiffness and swelling | 2.041 | 0.059 | 12655.61 | 53.1 | 43 | 39.3 | 246 |
| Neurological-Sleep: Vivid Dreams/Nightmares | 2.06 | 0.058 | 9058.67 | 54.6 | 45.4 | 39.3 | 100 |
| Infection: Mycoplasma | 2.054 | 0.075 | 11920.39 | 54 | 54 | 39.4 | 111 |
| Neurological: Disorientation | 2.102 | 0.077 | 8725.15 | 56.9 | 55 | 39.5 | 80 |
| Comorbid-Mouth: Gingivits / Gum Disease | 2.04 | 0.06 | 8021.06 | 55.7 | 47.7 | 39.8 | 67 |
| Autonomic Manifestations: Cortisol disorders or irregularity | 2.015 | 0.064 | 8834.639 | 51.8 | 47.6 | 39.8 | 97 |
| General: Headaches | 1.991 | 0.06 | 12468.8 | 51.2 | 44.8 | 39.9 | 309 |
| Official Diagnosis: Mast Cell Dysfunction | 2.012 | 0.06 | 13066.28 | 51.8 | 43.1 | 39.9 | 208 |
| Autonomic: Dizziness or fainting | 1.932 | 0.062 | 8867.455 | 49.6 | 45.5 | 39.9 | 112 |
| Immune Manifestations: general malaise | 1.962 | 0.061 | 13005.88 | 50.5 | 44.9 | 40 | 339 |
| Comorbid: Hypothyroidism | 1.982 | 0.061 | 12229.72 | 50.9 | 43.5 | 40 | 258 |
| Autonomic Manifestations: nausea | 1.862 | 0.067 | 9328.009 | 46.5 | 47.9 | 40.1 | 108 |
| Age: 60-70 | 1.997 | 0.057 | 14128.26 | 51.2 | 40.1 | 40.2 | 195 |
| Neuroendocrine Manifestations: Rapid muscular fatiguability | 2.024 | 0.063 | 9405.636 | 53.4 | 46.7 | 40.2 | 165 |
| Pain: Aching of the eyes or behind the eyes | 1.954 | 0.058 | 11520.93 | 49.6 | 44.7 | 40.3 | 98 |
| Immune Manifestations: Alcohol Intolerant | 1.967 | 0.059 | 12012.28 | 49.9 | 41.8 | 40.5 | 303 |
| Neurocognitive: Difficulty understanding things | 1.942 | 0.071 | 9540.413 | 49.8 | 49.6 | 40.5 | 189 |
| Neurological-Vision: photophobia (Light Sensitivity) | 2.004 | 0.063 | 12593.74 | 51.2 | 44.7 | 40.5 | 276 |
| Onset: less than 16 years since onset | 1.954 | 0.057 | 8948.205 | 49.7 | 46.3 | 40.7 | 83 |
| Autonomic Manifestations: irritable bowel syndrome | 1.963 | 0.063 | 13226.9 | 50.8 | 44.2 | 40.8 | 378 |
| Neurocognitive: Feeling disoriented | 1.976 | 0.065 | 9168.405 | 50.8 | 49.3 | 40.8 | 126 |
| Comorbid-Mouth: TMJ / Dysfunction of the temporomandibular joint syndrome | 1.986 | 0.057 | 13336.82 | 50.9 | 40.2 | 40.8 | 223 |
| Autonomic Manifestations: palpitations | 1.876 | 0.064 | 9256.654 | 47 | 45.9 | 40.9 | 133 |
| Infection: Human Herpesvirus 6 (HHV6) | 2.056 | 0.068 | 14020.15 | 54.2 | 49.5 | 40.9 | 149 |
| Neuroendocrine Manifestations: worsening of symptoms with stress. | 1.989 | 0.061 | 10591.72 | 51.1 | 44.9 | 40.9 | 414 |
| Autonomic Manifestations: Postural orthostatic tachycardia syndrome (POTS) | 1.927 | 0.067 | 9603.289 | 48.8 | 45.2 | 40.9 | 128 |
| Onset: less than 04 years since onset | 2.034 | 0.073 | 8956.183 | 54.1 | 53.2 | 40.9 | 71 |
| Immune Manifestations: Abdominal Pain | 1.947 | 0.068 | 14265.76 | 49.4 | 46.5 | 41.1 | 326 |
| Neurological: Word-finding problems | 2.057 | 0.064 | 10858.39 | 53.5 | 46.9 | 41.2 | 289 |
| Neurological-Audio: hypersensitivity to noise | 1.958 | 0.064 | 11562.53 | 49.7 | 45.7 | 41.2 | 347 |
| Immune Manifestations: recurrent flu-like symptoms | 2.001 | 0.066 | 15145.96 | 51.8 | 48.4 | 41.2 | 124 |
| Neuroendocrine: Alcohol intolerance | 1.951 | 0.06 | 13204.94 | 49.6 | 41.8 | 41.3 | 278 |
| Post-exertional malaise: Rapid muscular fatigability, | 2.024 | 0.06 | 9815.645 | 52.8 | 44.1 | 41.4 | 169 |
| Neurocognitive: Problems remembering things | 1.99 | 0.065 | 11390.81 | 51.3 | 46.9 | 41.4 | 415 |
| Comorbid: Constipation and Explosions (not diarrohea) | 2.014 | 0.062 | 14823.47 | 52.2 | 41.9 | 41.5 | 170 |
| Neuroendocrine Manifestations: intolerance of extremes of heat and cold | 1.987 | 0.064 | 9946.112 | 50.9 | 47.3 | 41.5 | 249 |
| Pain: Eye pain | 1.978 | 0.046 | 14356.53 | 51 | 37.8 | 41.5 | 57 |
| Neurological-Audio: Tinnitus (ringing in ear) | 1.96 | 0.061 | 13969.85 | 49.5 | 44.8 | 41.5 | 392 |
| Blood Type: A Negative | 1.87 | 0.06 | 8845 | 47.9 | 42.9 | 41.5 | 24 |
| Neurocognitive: Unable to focus vision and/or attention | 2.01 | 0.065 | 12425.26 | 52 | 45.7 | 41.6 | 302 |
| Other: Sensitivity to mold | 2.043 | 0.067 | 9442.872 | 53.5 | 50.5 | 41.7 | 141 |
| Neurocognitive: Can only focus on one thing at a time | 1.981 | 0.06 | 11138.71 | 50.7 | 45 | 41.7 | 394 |
| Neurological: Cognitive/Sensory Overload | 1.988 | 0.067 | 10058.01 | 50.7 | 49.4 | 41.7 | 219 |
| Immune Manifestations: medication sensitivities. | 2.092 | 0.061 | 13364.06 | 55.5 | 44.5 | 41.7 | 142 |
| Neurocognitive: Difficulty paying attention for a long period of time | 2.002 | 0.064 | 11330.78 | 52 | 46.8 | 41.8 | 429 |
| Immune Manifestations: hives | 1.973 | 0.056 | 10904.28 | 50.2 | 38.6 | 41.9 | 46 |
| Onset: Sudden | 1.704 | 0.068 | 8797.214 | 39.9 | 47.7 | 41.9 | 70 |
| Autonomic Manifestations: exertional dyspnea | 1.771 | 0.061 | 9788.978 | 45.3 | 39.9 | 42 | 46 |
| Comorbid: Mold Sensitivity / Exposure | 2.072 | 0.066 | 9522.613 | 54.2 | 49.7 | 42.1 | 137 |
| Sleep: Need to nap daily | 1.955 | 0.061 | 9768.217 | 49.7 | 46.3 | 42.1 | 129 |
| Neuroendocrine Manifestations: sweating episodes | 2.074 | 0.071 | 13323.83 | 54.6 | 47.9 | 42.1 | 183 |
| Post-exertional malaise: Inappropriate loss of physical and mental stamina, | 2.034 | 0.063 | 9683.478 | 52.7 | 46.7 | 42.1 | 255 |
| Autonomic Manifestations: urinary frequency dysfunction | 2.023 | 0.07 | 8986.062 | 53.6 | 49.5 | 42.2 | 113 |
| Neurocognitive: Difficulty expressing thoughts | 1.996 | 0.074 | 10247.57 | 51.8 | 49.4 | 42.2 | 232 |
| General: Fatigue | 1.971 | 0.058 | 12031.46 | 50.6 | 44.5 | 42.3 | 554 |
| Immune: Flu-like symptoms | 2.032 | 0.067 | 17995.01 | 53.2 | 47.3 | 42.3 | 116 |
| Neuroendocrine Manifestations: marked weight change | 2.115 | 0.069 | 13678.23 | 55.3 | 50.2 | 42.3 | 119 |
| Comorbid-Mouth: Bruxism – Jaw cleanching / Teeth grinding | 2.005 | 0.062 | 13571.29 | 51.6 | 43.2 | 42.3 | 318 |
| Neuroendocrine: Feeling hot or cold for no reason | 1.985 | 0.067 | 10345.56 | 50.5 | 48.5 | 42.4 | 158 |
| Autonomic: Ocassional Tachycardia (Rapid heart beat) | 1.908 | 0.067 | 9478.579 | 48.1 | 49.2 | 42.4 | 121 |
| Gender: Female | 2 | 0.055 | 9736.427 | 51.3 | 43.3 | 42.4 | 372 |
| Immune: Recurrent Sore throat | 1.961 | 0.063 | 11439.67 | 49.5 | 45.9 | 42.5 | 134 |
| Neurological-Sleep: Sleep Apnea | 2.148 | 0.066 | 19898.1 | 58.2 | 52.3 | 42.6 | 103 |
| Comorbid: Snoring (NOT Sleep Apnea | 2.031 | 0.059 | 14436.91 | 52.7 | 41.6 | 42.6 | 185 |
| Sleep: Waking up early in the morning (e.g. 3 AM) | 2.057 | 0.062 | 12919.95 | 53.3 | 45 | 42.7 | 349 |
| Neuroendocrine Manifestations: marked diurnal fluctuation | 2.115 | 0.06 | 10086.79 | 58 | 45.6 | 42.7 | 24 |
| Immune Manifestations: Mucus in the stool | 2.045 | 0.078 | 14352.74 | 52.9 | 51.6 | 42.7 | 176 |
| Neuroendocrine Manifestations: cold extremities | 1.961 | 0.061 | 14395.2 | 49.6 | 45.3 | 42.8 | 267 |
| Neuroendocrine Manifestations: loss of adaptability | 1.963 | 0.065 | 22154.92 | 51 | 47.4 | 42.9 | 62 |
| Neurological-Sleep: Night Sweats | 2.071 | 0.065 | 13304.88 | 53.3 | 46.3 | 42.9 | 141 |
| Pain: Sensitivity to pain | 2.049 | 0.072 | 12457.74 | 53.1 | 51.1 | 42.9 | 181 |
| Immune Manifestations: Bloating | 1.977 | 0.063 | 13344.09 | 50.3 | 45 | 42.9 | 504 |
| Post-exertional malaise: Difficulty reading after mild physical or mental activity | 1.991 | 0.065 | 10766.63 | 51.2 | 47 | 42.9 | 192 |
| Onset: less than 08 years since onset | 2.054 | 0.059 | 9535.966 | 54.9 | 43.3 | 43 | 58 |
| Neurological-Sleep: Insomnia | 2.03 | 0.061 | 14473.17 | 52.3 | 44.6 | 43 | 339 |
| Neuroendocrine: Cold limbs (e.g. arms, legs hands) | 1.969 | 0.067 | 12977.49 | 50.6 | 46.4 | 43 | 191 |
| Sleep: Unrefreshed sleep | 1.989 | 0.059 | 12300.45 | 51.3 | 44.1 | 43 | 479 |
| Immune Manifestations: Constipation | 2.004 | 0.059 | 14280.13 | 52.1 | 43.2 | 43 | 395 |
| General: Depression | 2.11 | 0.067 | 12559.02 | 55.7 | 49.1 | 43 | 278 |
| Official Diagnosis: Irritable Bowel Syndrome | 1.999 | 0.065 | 14433.07 | 51.3 | 45 | 43.1 | 349 |
| Comorbid: Multiple Chemical Sensitivity | 2.053 | 0.056 | 12104.99 | 53.9 | 41.3 | 43.1 | 131 |
| Neuroendocrine Manifestations: Air Hunger | 1.931 | 0.058 | 9873.469 | 48.8 | 44.5 | 43.1 | 81 |
| Sleep: Daytime drowsiness | 2.018 | 0.065 | 14393.73 | 52.2 | 46.6 | 43.1 | 349 |
| Autonomic: Shortness of breath | 1.976 | 0.067 | 9794.895 | 50.5 | 47.8 | 43.1 | 124 |
| Immune Manifestations: Thick blood / Hypercoagulation | 1.99 | 0.061 | 9581.985 | 51.2 | 46.8 | 43.2 | 66 |
| Sleep: Problems falling asleep | 2.031 | 0.065 | 10621.44 | 52.4 | 47.8 | 43.2 | 221 |
| Infection: Lyme | 2.029 | 0.057 | 11234.89 | 52.6 | 46.8 | 43.2 | 71 |
| Neurological-Sleep: Inability for deep (delta) sleep | 2.097 | 0.071 | 14421.58 | 55.9 | 48.9 | 43.2 | 151 |
| Onset: less than 02 years since onset | 1.896 | 0.063 | 9318.657 | 46.1 | 46.3 | 43.3 | 67 |
| Onset: 2010-2020 | 1.99 | 0.064 | 12458.24 | 50.4 | 44.7 | 43.4 | 325 |
| Age: 10-20 | 2.014 | 0.071 | 9357.475 | 53.2 | 49.8 | 43.4 | 40 |
| Autonomic Manifestations: light-headedness | 1.988 | 0.07 | 10053.82 | 50.4 | 49.3 | 43.6 | 145 |
| Sleep: Problems staying asleep | 2.051 | 0.059 | 13891.49 | 52.9 | 44.1 | 43.7 | 380 |
| Autonomic: Irregular heartbeats | 2.047 | 0.068 | 14841.51 | 52.8 | 48 | 43.8 | 141 |
| Comorbid: Histamine or Mast Cell issues | 1.969 | 0.059 | 13247.94 | 49.7 | 43.5 | 43.8 | 355 |
| Other: Sensitivity to vibrations | 1.929 | 0.044 | 12403.73 | 47.9 | 37.3 | 43.9 | 52 |
| Post-exertional malaise: Mentally tired after the slightest effort | 2.018 | 0.063 | 10731.34 | 51.5 | 47.2 | 43.9 | 161 |
| Official Diagnosis: Allergic Rhinitis (Hay Fever) | 1.965 | 0.057 | 13655.98 | 49.7 | 41.6 | 43.9 | 232 |
| Infection: Epstein-Barr virus | 2.117 | 0.06 | 13402.13 | 55.8 | 45.4 | 44 | 240 |
| Infection: Coxsackie | 2.1 | 0.061 | 9782.615 | 57.3 | 47.6 | 44.2 | 39 |
| Post-exertional malaise: Rapid cognitive fatigability, | 2.055 | 0.061 | 10488.19 | 53.6 | 46.8 | 44.2 | 212 |
| Neurocognitive: Brain Fog | 1.982 | 0.064 | 12153.58 | 50.4 | 46.3 | 44.3 | 597 |
| Comorbid: Small intestinal bacterial overgrowth (SIBO) | 2.02 | 0.071 | 13923.31 | 51.2 | 52.7 | 44.4 | 191 |
| Immune: Tender / sore lymph nodes | 2.096 | 0.068 | 14842.85 | 53.6 | 46.7 | 44.4 | 111 |
| Post-exertional malaise: Worsening of symptoms after mild mental activity | 2.016 | 0.071 | 10902.02 | 51.9 | 51.4 | 44.4 | 165 |
| General: Sinus issues with headaches | 2.024 | 0.065 | 13296.41 | 52 | 46.4 | 44.5 | 124 |
| Age: 20-30 | 1.974 | 0.07 | 16286.07 | 51.1 | 50.9 | 44.5 | 136 |
| Post-exertional malaise: Next-day soreness after everyday activities | 2.104 | 0.064 | 12530.68 | 54.4 | 47.2 | 44.5 | 198 |
| Immune Manifestations: Inflammation of skin, eyes or joints | 2.097 | 0.068 | 16251.55 | 54.8 | 51.1 | 44.6 | 228 |
| Post-exertional malaise: General | 2.053 | 0.063 | 13379.21 | 53.4 | 48.9 | 44.6 | 243 |
| Neurological: Slowed speech | 2.179 | 0.08 | 14630.11 | 57.9 | 49.4 | 44.7 | 108 |
| Post-exertional malaise: Post-exertional malaise | 2.072 | 0.06 | 10683.72 | 53.8 | 46.3 | 44.7 | 269 |
| Neurological: Joint hypermobility | 2.063 | 0.072 | 15030.99 | 53.3 | 48.8 | 44.8 | 167 |
| Neurological: Seasonal Affective Disorder (SAD) | 2.171 | 0.073 | 12976.18 | 58.7 | 49.8 | 44.9 | 127 |
| Neuroendocrine Manifestations: Laboured breathing | 2.003 | 0.077 | 11266.07 | 52.1 | 51.8 | 44.9 | 30 |
| Autonomic Manifestations: delayed postural hypotension | 2.091 | 0.08 | 10730.32 | 56.3 | 51.3 | 44.9 | 28 |
| Infection: Parasite – Other | 2.089 | 0.079 | 13683.44 | 55.4 | 52.2 | 44.9 | 81 |
| Autonomic: Heart rate increase after standing | 1.946 | 0.058 | 10621.93 | 50.4 | 44.6 | 44.9 | 145 |
| Comorbid: Inflammatory bowel disease | 2.096 | 0.078 | 15575.55 | 54.1 | 51.6 | 45 | 162 |
| Immune: Chronic Sinusitis | 1.969 | 0.056 | 9423.875 | 49.4 | 44.9 | 45 | 80 |
| Neuroendocrine Manifestations: Paraesthesia (tingling burning of skin) | 2.177 | 0.075 | 15722.67 | 57.3 | 52.5 | 45.1 | 129 |
| Immune Manifestations: Hair loss | 2.111 | 0.075 | 17633.89 | 55.2 | 53.5 | 45.1 | 218 |
| Onset: 1990-2000 | 2.132 | 0.056 | 30905.83 | 56.2 | 46.3 | 45.1 | 42 |
| Post-exertional malaise: Physically drained or sick after mild activity | 2.092 | 0.063 | 11092.9 | 55.3 | 47.1 | 45.1 | 207 |
| Neurological-Sleep: Prolonged Sleep | 1.922 | 0.059 | 9645.784 | 48.1 | 41.6 | 45.2 | 37 |
| Official Diagnosis: Autism | 2 | 0.081 | 11715.03 | 50.2 | 52.3 | 45.2 | 207 |
| Age: 50-60 | 2.013 | 0.049 | 16092.02 | 50.4 | 37 | 45.4 | 142 |
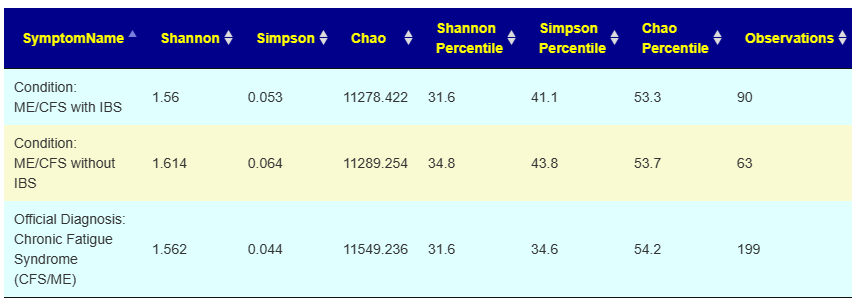
| Official Diagnosis: Chronic Fatigue Syndrome (CFS/ME) | 2.046 | 0.052 | 13112.63 | 52.8 | 40.9 | 45.6 | 528 |
| Post-exertional malaise: Muscle fatigue after mild physical activity | 2.087 | 0.069 | 12312.77 | 54 | 50.1 | 45.6 | 265 |
| Autonomic Manifestations: Orthostatic intolerance | 2.087 | 0.069 | 14092.74 | 54.9 | 49.7 | 45.7 | 164 |
| Comorbid: Fibromyalgia | 2.099 | 0.074 | 18779.22 | 55.9 | 53.2 | 46 | 107 |
| Neurological: Myoclonic jerks or seizures | 1.982 | 0.053 | 11801.6 | 49.9 | 36.9 | 46 | 50 |
| Official Diagnosis: Depression | 2.137 | 0.069 | 13752.19 | 57 | 50.9 | 46 | 99 |
| Autonomic Manifestations: bladder dysfunction | 1.947 | 0.064 | 10480.63 | 50.3 | 43.6 | 46.1 | 56 |
| Official Diagnosis: Fibromyalgia | 2.042 | 0.071 | 20205.99 | 53.1 | 50.8 | 46.1 | 73 |
| Age: 40-50 | 1.989 | 0.073 | 10590.26 | 50.3 | 52.1 | 46.2 | 216 |
| Joint: Tenderness | 2.141 | 0.074 | 19366.06 | 56.4 | 51.8 | 46.2 | 173 |
| Gender: Male | 2.066 | 0.067 | 14723.23 | 53.5 | 49 | 46.2 | 507 |
| Post-exertional malaise: Physically tired after minimum exercise | 2.053 | 0.064 | 13813.96 | 52.7 | 47.5 | 46.2 | 268 |
| Post-exertional malaise: Worsening of symptoms after mild physical activity | 2.1 | 0.062 | 12504.35 | 54.6 | 46.6 | 46.4 | 282 |
| Immune Manifestations: High Altitude Intolerance | 1.997 | 0.067 | 27233.9 | 51.5 | 48 | 46.5 | 49 |
| Official Diagnosis: High Blood Pressure (Hypertension) | 2.149 | 0.079 | 24512.04 | 56.7 | 62.8 | 46.6 | 27 |
| Comorbid: High Anxiety | 2.085 | 0.066 | 16472 | 54.3 | 47.4 | 46.6 | 302 |
| Blood Type: O Positive | 2.107 | 0.061 | 14366.56 | 54.8 | 43.4 | 46.7 | 262 |
| Autonomic: Inability to tolerate an upright position | 2.119 | 0.074 | 16184.94 | 56.3 | 50.2 | 47 | 136 |
| Official Diagnosis: Autoimmune Disease | 2.217 | 0.069 | 18238.23 | 59.4 | 49.8 | 47.3 | 184 |
| Comorbid: Methylation issues (MTHFR) | 2.158 | 0.066 | 11514.35 | 57.8 | 52 | 47.3 | 113 |
| Comorbid: Restless Leg | 2.071 | 0.065 | 10681.73 | 54.5 | 48.8 | 47.4 | 93 |
| Official Diagnosis: Mood Disorders | 2.294 | 0.074 | 10430.17 | 62.8 | 57.7 | 47.6 | 54 |
| Immune Manifestations: Inflammation (General) | 2.087 | 0.071 | 16527.17 | 54.1 | 51.9 | 47.6 | 277 |
| Onset: less than 32 years since onset | 2.053 | 0.063 | 12146.14 | 51.7 | 52.7 | 47.6 | 70 |
| Neurological: Dysautonomia | 2.025 | 0.067 | 14155.11 | 51.8 | 46.9 | 47.8 | 156 |
| Age: 30-40 | 2.058 | 0.066 | 11989.15 | 53.1 | 49.9 | 48 | 330 |
| DePaul University Fatigue Questionnaire : Feeling like you have a temperature | 1.938 | 0.074 | 10889.88 | 47.3 | 55.3 | 48.2 | 43 |
| DePaul University Fatigue Questionnaire : New trouble with math | 2.19 | 0.072 | 11232.03 | 54.9 | 57.6 | 48.4 | 35 |
| DePaul University Fatigue Questionnaire : Chilled or shivery | 1.931 | 0.071 | 26909.26 | 46.4 | 50.9 | 48.6 | 47 |
| DePaul University Fatigue Questionnaire : Sweating hands | 1.859 | 0.091 | 10413.74 | 42.2 | 55.8 | 48.9 | 27 |
| Official Diagnosis: COVID19 (Long Hauler) | 1.617 | 0.083 | 10288.01 | 33.5 | 54.3 | 48.9 | 203 |
| Comorbid-Mouth: Mouth Sores | 2.146 | 0.066 | 17904.74 | 55 | 45.6 | 48.9 | 70 |
| Comorbid-Mouth: Ulcers (mouth) | 1.964 | 0.062 | 11296.41 | 49.6 | 45.9 | 49 | 27 |
| Official Diagnosis: Osteoporosis | 1.888 | 0.054 | 10854.14 | 47.1 | 40.8 | 49 | 21 |
| Immune: Viral infections with prolonged recovery periods | 2.066 | 0.066 | 11620.85 | 53.6 | 48.8 | 49 | 99 |
| Comorbid: Salicylate sensitive | 1.529 | 0.048 | 10532.92 | 30.1 | 37.5 | 49.1 | 36 |
| Comorbid: Mood Swings | 1.99 | 0.07 | 11071.23 | 48.6 | 51.5 | 49.4 | 97 |
| DePaul University Fatigue Questionnaire : Tingling feeling | 1.705 | 0.072 | 14165.09 | 37.1 | 49.1 | 49.4 | 66 |
| Blood Type: O Negative | 1.945 | 0.077 | 11344.33 | 47.7 | 45.4 | 49.5 | 30 |
| Comorbid: Electromagnetic Sensitivity (EMF) | 2.224 | 0.065 | 12963.08 | 60.2 | 47.6 | 49.5 | 39 |
| Neurological-Sleep: Sleep Reversal | 2.225 | 0.065 | 10837.67 | 60.1 | 53.2 | 49.6 | 33 |
| Neuroendocrine Manifestations: Painful menstrual periods | 2.145 | 0.059 | 11232.21 | 57.6 | 45.4 | 49.6 | 57 |
| DePaul University Fatigue Questionnaire : Impaired Memory & concentration | 2.037 | 0.069 | 17173.98 | 51.4 | 49.3 | 49.7 | 298 |
| Comorbid: Carbohydrate intolerance | 1.961 | 0.061 | 12491.89 | 51.1 | 45.3 | 49.9 | 46 |
| DePaul University Fatigue Questionnaire : Frequently get words or numbers in the wrong order | 2.095 | 0.077 | 12878.05 | 53 | 54.6 | 49.9 | 56 |
| DePaul University Fatigue Questionnaire : Chest pain | 1.966 | 0.078 | 13689.93 | 47.9 | 55.4 | 50.3 | 27 |
| Onset: 1980-1990 | 2.043 | 0.047 | 37107.56 | 53.8 | 36.7 | 50.4 | 32 |
| DePaul University Fatigue Questionnaire : Poor Appetite | 1.949 | 0.054 | 14012.92 | 48.5 | 43.7 | 50.5 | 37 |
| Official Diagnosis: Attention deficit hyperactivity disorder (ADHD) | 2.081 | 0.078 | 11843.49 | 55.1 | 54.8 | 50.5 | 80 |
| Comorbid-Mouth: Periradicular periodontitis inflammatory / chronic lesion around roots of teeth | 2.031 | 0.048 | 11195.24 | 54.4 | 38.9 | 50.6 | 25 |
| DePaul University Fatigue Questionnaire : Nausea | 1.856 | 0.074 | 12353 | 44.3 | 51.8 | 50.7 | 63 |
| Physical: Eastern European | 1.71 | 0.057 | 11299.21 | 36.8 | 45.9 | 50.8 | 34 |
| DePaul University Fatigue Questionnaire : Difficulty reasoning things out | 1.955 | 0.078 | 11585.79 | 48 | 52.9 | 50.9 | 79 |
| Joint: Redness | 2.274 | 0.072 | 22181.72 | 61.8 | 50 | 51 | 46 |
| DePaul University Fatigue Questionnaire : Blurred Vision | 1.766 | 0.062 | 11329.24 | 39.4 | 45.9 | 51 | 62 |
| DePaul University Fatigue Questionnaire : Difficulty falling asleep | 2.024 | 0.08 | 12073.2 | 50.1 | 53.8 | 51 | 133 |
| DePaul University Fatigue Questionnaire : Unrefreshing Sleep, that is waking up feeling tired | 2.062 | 0.068 | 16938.43 | 52 | 48.9 | 51.4 | 334 |
| DePaul University Fatigue Questionnaire : Racing heart | 1.953 | 0.075 | 22527.55 | 46.7 | 51.5 | 51.4 | 67 |
| DePaul University Fatigue Questionnaire : Feel unsteady on feet | 2.026 | 0.057 | 13562.46 | 50.1 | 37.9 | 51.9 | 41 |
| DePaul University Fatigue Questionnaire : Fatigue | 2.093 | 0.067 | 16345.97 | 53.2 | 48.8 | 52.1 | 380 |
| DePaul University Fatigue Questionnaire : Muscle Pain (i.e., sensations of pain or aching in your muscles. This does not include weakness or pain in other areas such as joints) | 1.968 | 0.072 | 20265.4 | 47.3 | 53.1 | 52.2 | 117 |
| General: Heavy feeling in arms and legs | 2.066 | 0.066 | 12763.22 | 53.3 | 48.9 | 52.3 | 104 |
| DePaul University Fatigue Questionnaire : Upset stomach | 1.839 | 0.07 | 21705.82 | 42.8 | 47.5 | 52.3 | 79 |
| DePaul University Fatigue Questionnaire : Weight change | 2.006 | 0.067 | 11665.45 | 50.4 | 50.4 | 52.5 | 60 |
| DePaul University Fatigue Questionnaire : Pain in Multiple Joints without Swelling or Redness | 1.946 | 0.06 | 15796.95 | 46.6 | 49.3 | 52.5 | 74 |
| Autism: More Inappropriate Social Interaction | 2.086 | 0.086 | 11929.54 | 54.1 | 54.1 | 52.6 | 24 |
| Comorbid: Constipation and Diarrohea (not explosions) | 1.957 | 0.063 | 12512.67 | 48.7 | 48 | 52.7 | 98 |
| Comorbid: Sleep Apnea Diagnosis | 2.054 | 0.059 | 41891.19 | 52.7 | 47.8 | 52.7 | 47 |
| DePaul University Fatigue Questionnaire : Difficulty retaining information | 2.028 | 0.066 | 18395.93 | 50.8 | 48.6 | 53 | 134 |
| DePaul University Fatigue Questionnaire : Mood swings | 2.14 | 0.073 | 12088.44 | 53.3 | 52.2 | 53.2 | 81 |
| DePaul University Fatigue Questionnaire : Shortness of breath | 2.031 | 0.072 | 12631.27 | 49.1 | 47.8 | 53.2 | 71 |
| DePaul University Fatigue Questionnaire : Difficulty recalling information | 1.98 | 0.067 | 17335.97 | 49 | 49.5 | 53.2 | 152 |
| DePaul University Fatigue Questionnaire : Eye pain | 1.881 | 0.051 | 16658.33 | 43.1 | 42.9 | 53.3 | 60 |
| DePaul University Fatigue Questionnaire : Headaches | 1.938 | 0.077 | 21075.7 | 46.7 | 51.7 | 53.3 | 97 |
| Physical: Long term antibiotics(over 6 months) | 1.953 | 0.082 | 13398.78 | 47.4 | 62.5 | 53.3 | 32 |
| Comorbid: Migraine | 2.07 | 0.072 | 18043.71 | 51.2 | 50.5 | 53.4 | 90 |
| DePaul University Fatigue Questionnaire : Sore Throat | 1.964 | 0.068 | 14178.04 | 48.4 | 45.3 | 53.5 | 57 |
| Physical: Long term (chronic) stress | 1.849 | 0.06 | 19406.05 | 43.2 | 46.1 | 53.5 | 102 |
| DePaul University Fatigue Questionnaire : Forgetting what you are trying to say | 2.039 | 0.069 | 18515.81 | 50.3 | 51.4 | 53.6 | 122 |
| DePaul University Fatigue Questionnaire : Night sweats | 2.038 | 0.068 | 12137.17 | 49.1 | 47.1 | 53.8 | 46 |
| DePaul University Fatigue Questionnaire : Frequently loose train of thought | 2.105 | 0.079 | 12781.15 | 53.7 | 57.3 | 53.8 | 107 |
| DePaul University Fatigue Questionnaire : Difficulty following things | 1.995 | 0.08 | 13048.19 | 49 | 53.9 | 54 | 89 |
| DePaul University Fatigue Questionnaire : Depression | 2.069 | 0.065 | 19883.27 | 52.7 | 49.7 | 54 | 99 |
| DePaul University Fatigue Questionnaire : Allergies | 1.921 | 0.059 | 12296.65 | 47.2 | 45.5 | 54 | 141 |
| DePaul University Fatigue Questionnaire : Difficulty comprehending Information | 1.972 | 0.083 | 12479.67 | 47.7 | 54.4 | 54.1 | 121 |
| DePaul University Fatigue Questionnaire : Abdomen pain | 1.958 | 0.074 | 22318.12 | 48.2 | 53 | 54.2 | 78 |
| DePaul University Fatigue Questionnaire : Hot or Cold spells | 1.935 | 0.065 | 23234.88 | 47.4 | 45.4 | 54.2 | 68 |
| Blood Type: A Positive | 2.167 | 0.078 | 16858.1 | 55.6 | 53 | 54.2 | 112 |
| DePaul University Fatigue Questionnaire : Muscle weakness | 1.958 | 0.066 | 12329.4 | 47.8 | 49.4 | 54.2 | 123 |
| DePaul University Fatigue Questionnaire : Sensitivity to Alcohol | 2.056 | 0.065 | 16243.8 | 51.6 | 46.2 | 54.3 | 98 |
| DePaul University Fatigue Questionnaire : Difficulty finding the right word | 2.031 | 0.069 | 17169.14 | 50.8 | 49.8 | 54.4 | 181 |
| DePaul University Fatigue Questionnaire : Does physical activity make you feel worse | 2.04 | 0.059 | 17569.78 | 51.4 | 47.2 | 54.5 | 160 |
| Physical: Steps Per Day 2000-4000 | 1.898 | 0.057 | 12403.9 | 45.5 | 41.9 | 54.7 | 69 |
| Physical: Northern European | 1.847 | 0.062 | 13131.31 | 43.2 | 44.9 | 54.7 | 116 |
| DePaul University Fatigue Questionnaire : Temperature lower than normal | 2.05 | 0.06 | 13048.24 | 50.3 | 44.8 | 54.8 | 63 |
| Comorbid: Sugars cause sleep or cognitive issues | 1.988 | 0.071 | 14434.56 | 51.9 | 54.8 | 54.8 | 32 |
| DePaul University Fatigue Questionnaire : Difficulty staying asleep | 2.135 | 0.065 | 18877.49 | 54 | 48.8 | 54.9 | 141 |
| Age: 0-10 | 2.083 | 0.116 | 14335.89 | 55.4 | 62.6 | 54.9 | 87 |
| Official Diagnosis: Celiac Disease | 2.036 | 0.08 | 20864.15 | 51.1 | 54.9 | 55 | 34 |
| Condition: Acne | 1.926 | 0.055 | 18545.04 | 47.3 | 45.1 | 55.1 | 80 |
| DePaul University Fatigue Questionnaire : Walking up early in the morning (e.g. 3AM) | 2.136 | 0.06 | 21152.2 | 54.3 | 47.7 | 55.1 | 102 |
| Autism: More deficits in Language Comprehension | 2.118 | 0.093 | 12237.69 | 55.8 | 60.2 | 55.1 | 35 |
| DePaul University Fatigue Questionnaire : Confusion/disorientation | 1.905 | 0.075 | 12532.17 | 45.7 | 53.7 | 55.1 | 60 |
| DePaul University Fatigue Questionnaire : Need to nap during each day | 1.869 | 0.065 | 25116.62 | 44.8 | 47.6 | 55.3 | 85 |
| DePaul University Fatigue Questionnaire : Trouble expressing thoughts | 2.048 | 0.079 | 12709.91 | 50.5 | 56 | 55.3 | 91 |
| Autism: More Decrease in Speaking | 1.956 | 0.089 | 11878.78 | 49.8 | 52.4 | 55.4 | 41 |
| DePaul University Fatigue Questionnaire : Tense muscles | 1.884 | 0.065 | 21790.03 | 45.6 | 46.9 | 55.5 | 81 |
| DePaul University Fatigue Questionnaire : Post-exertional malaise, feeling worse after doing activities that require either physical or mental exertion | 2.044 | 0.064 | 13295.65 | 50.9 | 49.3 | 55.5 | 191 |
| Condition: Non-alcoholic Fatty Liver Disease | 1.927 | 0.071 | 12291.76 | 48.4 | 49 | 55.7 | 29 |
| DePaul University Fatigue Questionnaire : Rash | 2.141 | 0.07 | 12809.34 | 56 | 49 | 55.9 | 41 |
| Condition: Post-Traumatic Stress Disorder | 2.073 | 0.066 | 13172 | 52.1 | 51.4 | 56.1 | 61 |
| Autism: More Avoidance of Eye Contact or Poor Eye Contact | 1.954 | 0.087 | 14132.08 | 49.9 | 52.4 | 56.2 | 26 |
| Condition: ME/CFS with IBS | 1.941 | 0.064 | 21176.43 | 47.6 | 46.6 | 56.2 | 146 |
| DePaul University Fatigue Questionnaire : Absent-mindedness | 2.006 | 0.07 | 19498.31 | 49.6 | 52 | 56.2 | 119 |
| Autism: More Behavioral Disturbances | 2.381 | 0.105 | 13815.91 | 66.7 | 63.9 | 56.3 | 23 |
| Condition: ME/CFS without IBS | 1.984 | 0.062 | 12510.58 | 49.1 | 45.9 | 56.4 | 89 |
| Physical: Paleo Diet | 1.768 | 0.038 | 12820.74 | 40.5 | 31.5 | 56.5 | 23 |
| DePaul University Fatigue Questionnaire : Slowness of thought | 1.941 | 0.07 | 12898.63 | 46.8 | 49.4 | 56.6 | 104 |
| DePaul University Fatigue Questionnaire : Abnormal sensitivity to light | 2.014 | 0.069 | 14154 | 48.9 | 49.3 | 56.7 | 102 |
| Official Diagnosis: Gastroesophageal reflux disease (GERD) | 2.015 | 0.057 | 19077.8 | 51.7 | 44.8 | 56.7 | 65 |
| Autism: More Sleep Disturbances | 2.136 | 0.084 | 13719.14 | 56.2 | 55.9 | 56.8 | 36 |
| Physical: Good Air Quality | 1.715 | 0.055 | 12224.21 | 37.6 | 42.9 | 56.8 | 29 |
| DePaul University Fatigue Questionnaire : Need to have to focus on one thing at a time | 1.949 | 0.061 | 13809.39 | 48.2 | 45.6 | 56.8 | 120 |
| Physical: Steps Per Day 4000-8000 | 1.913 | 0.066 | 12897.58 | 45.5 | 47.1 | 57 | 60 |
| Autism: More Repetitive Movements | 2.038 | 0.105 | 12658.48 | 53.6 | 62.3 | 57 | 29 |
| DePaul University Fatigue Questionnaire : Ringing in the Ears | 1.998 | 0.062 | 20337.6 | 48.4 | 47.5 | 57.2 | 126 |
| DePaul University Fatigue Questionnaire : Dizziness | 1.983 | 0.066 | 14162.57 | 46.5 | 48.5 | 57.3 | 65 |
| DePaul University Fatigue Questionnaire : Chemical sensitivity | 2.221 | 0.066 | 14833.72 | 57.1 | 48.5 | 57.3 | 79 |
| DePaul University Fatigue Questionnaire : Anxiety/tension | 2.037 | 0.067 | 18111.31 | 51.4 | 49.2 | 57.5 | 159 |
| Autism: More Intense Focus on One Topic | 2.355 | 0.059 | 15148.77 | 63.7 | 47.7 | 57.5 | 22 |
| Physical: Tonsils removed | 2.077 | 0.069 | 13512.92 | 54.6 | 45.4 | 57.7 | 49 |
| General: Anhedonia (inability to feel pleasure) | 1.983 | 0.069 | 16245.07 | 47.5 | 54.1 | 57.8 | 27 |
| DePaul University Fatigue Questionnaire : Poor hand to eye coodination | 2.329 | 0.07 | 14096.38 | 57.2 | 52.1 | 58 | 21 |
| Condition: Psoriasis | 2.174 | 0.08 | 26532.52 | 56.8 | 54.4 | 58.2 | 33 |
| Neuroendocrine Manifestations: Poor gut motility | 1.888 | 0.067 | 19063.31 | 44.1 | 48.4 | 58.3 | 133 |
| DePaul University Fatigue Questionnaire : Concern with driving | 2.084 | 0.053 | 13892.65 | 53.3 | 43.1 | 58.3 | 40 |
| DePaul University Fatigue Questionnaire : Easily irritated | 2.077 | 0.07 | 15797.35 | 52.6 | 51.3 | 58.4 | 142 |
| Physical: Work-Sitting | 1.924 | 0.062 | 18699.64 | 46.1 | 45.2 | 58.5 | 139 |
| Physical: Breastfed | 2.17 | 0.049 | 16236.93 | 54.1 | 41.1 | 58.8 | 73 |
| Neurocognitive: Aphantasia ( inability to visualize mental images) | 1.939 | 0.078 | 14582.46 | 47.7 | 57.4 | 58.8 | 26 |
| Official Diagnosis: Hypercholesterolemia (High Cholesterol) | 2.034 | 0.063 | 13217.88 | 50.9 | 48 | 59.2 | 40 |
| Condition: Non-Celiac Gluten Sensitivity | 2.019 | 0.057 | 13551.54 | 50.2 | 44.8 | 59.4 | 78 |
| DePaul University Fatigue Questionnaire : Slow to react | 2.113 | 0.07 | 14951.93 | 52.7 | 51.2 | 59.4 | 75 |
| Condition: Asthma | 2.202 | 0.071 | 14193.31 | 56.9 | 55.2 | 59.5 | 32 |
| Physical: Steps Per Day 8000-16000 | 2.18 | 0.063 | 19185.95 | 55.5 | 47.8 | 60.1 | 37 |
| Immune Manifestations: Chronic Flatus / Flatulence / gas | 2.058 | 0.071 | 22413 | 52.4 | 49.4 | 60.2 | 98 |
| Physical: Amalgam fillings | 2.108 | 0.055 | 29287.59 | 54.2 | 39.9 | 60.4 | 49 |
| Condition: Generalized anxiety disorder | 2.183 | 0.077 | 39061 | 57.5 | 54.7 | 60.5 | 45 |
| Physical: Appendix removed | 2.159 | 0.052 | 19123.71 | 55.6 | 42 | 60.8 | 28 |
| Physical: Pets | 2.122 | 0.068 | 24978.46 | 53.6 | 45.7 | 60.8 | 90 |
| DePaul University Fatigue Questionnaire : Does physical activity make you feel better | 1.909 | 0.07 | 20720.16 | 47.4 | 51.9 | 61.3 | 38 |
| Autism: High Functioning | 2.383 | 0.061 | 15824.14 | 66.9 | 46.5 | 61.3 | 42 |
| Physical: Steps Per Day < 2000 | 1.998 | 0.056 | 16104.52 | 49.7 | 42.5 | 61.5 | 63 |
| Comorbid: Panic Attacks | 2.194 | 0.073 | 32169.33 | 57 | 50.3 | 62.3 | 48 |
| Official Diagnosis: COVID19 (Fully Recovered) | 2.09 | 0.058 | 15757.67 | 52.4 | 47.1 | 62.4 | 27 |
| Condition: Osteoarthritis | 1.892 | 0.057 | 14280.87 | 48.6 | 44 | 63.1 | 23 |
| Physical: Organic Diet | 2.131 | 0.071 | 26542.31 | 53.6 | 46 | 63.5 | 65 |
| Immune Manifestations: Hyperphagia (abnormally hunger or desire to eat) | 2.01 | 0.051 | 14582.67 | 49.9 | 43.5 | 63.7 | 21 |




Recent Comments