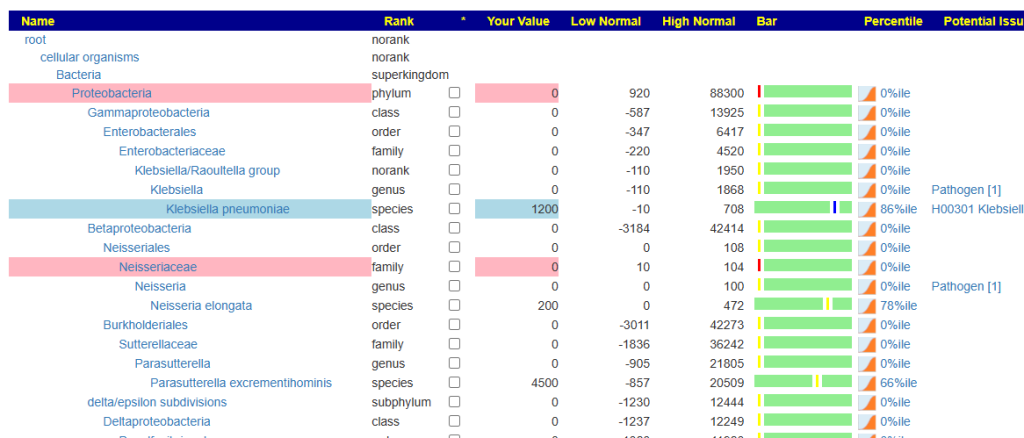
This study Microbial patterns in patients with histamine intolerance. Journal of physiology and pharmacology : an official journal of the Polish Physiological Society 2018 reports low Bifidobacteriaceae (NCBI:31953). The Artificial Intelligence Algorithms on Microbiome Prescription (and most medical professionals) would suggest Bifidobacterium probiotics as a possible treatment. Unfortunately, very few medical professionals outside of Poland would have read the above study!
I decided to look at the literature to see if the AI suggestions have been validated by actual studies. This is a few of the studies that I found (the ones where the title alone is sufficient):
- Combined IgE neutralization and Bifidobacterium longum supplementation reduces the allergic response in models of food allergy. [2022]
- Bifidobacterium longum IM55 and Lactobacillus plantarum IM76 alleviate allergic rhinitis in mice by restoring Th2/Treg imbalance and gut microbiota disturbance. [2019]
- Expression and Purification of Extracellular Solute-Binding Protein (ESBP) in Escherichia coli, the Extracellular Protein Derived from Bifidobacterium longum KACC 91563.[2019] ” it was demonstrated that the protein effectively alleviated food allergy symptoms via mast cell specific apoptosis, “
- Post-sensitization administration of non-digestible oligosaccharides and Bifidobacterium breve M-16V reduces allergic symptoms in mice. [2016]
- Three Novel Candidate Probiotic Strains with Prophylactic Properties in a Murine Model of Cow’s Milk Allergy [2016] One of these was Bifidobacterium longum subsp. infantis
- Extracellular vesicle-derived protein from Bifidobacterium longum alleviates food allergy through mast cell suppression.[2016]
- Longitudinal study of effects of oral dosage of Bifidobacterium bifidum G9-1 on Japanese cedar pollen-induced allergic nasal symptoms in guinea pigs. [2015]
- Bifidobacterium breve and Lactobacillus rhamnosus treatment is as effective as budesonide at reducing inflammation in a murine model for chronic asthma.[2014]
- The combination of Bifidobacterium breve with non-digestible oligosaccharides suppresses airway inflammation in a murine model for chronic asthma.[2014]
- Bifidobacterium longum lysate, a new ingredient for reactive skin. [2010]
- Effect of oral probiotics (Bifidobacterium lactis AD011 and Lactobacillus acidophilus AD031) administration on ovalbumin-induced food allergy mouse model. [2008]
Bottom Line
Bifidobacterium Longum appears to be the best researched and easily available as a single species. Different species of probiotics can cause a different response — so keep to single species probiotics and avoid probiotic mixtures as a general rule. My personal favorite source is Custom Probiotics (no financial interest), they are:
- by far the cheapest per BCFU,
- his recommended daily dosages are at therapeutic levels (80- 320 BCFU per day)
- his recommended method of taking is, IMHO, the correct way: NOT IN CAPSULES, but in a glass of water so it impacts the entire system from the mouth downwards (see 24 Years of ME/CFS with Mouth Microbiome for more information and studies)
Watch out for shooting yourself in the Microbiome!
Often I have encounter people frustrated over their inability to increase bifidobacterium or Lactobacillus. When they disclose what they are also taking — it becomes apparent why!
Going to Details about Bifidobacterium: NCBI 1678 we see what increases or decrease it. You may wish to consider reducing or eliminating these items.
| General Substance | Specific Substance | Effect |
|---|---|---|
| Herb or Spice | ascophyllum nodosum (sea weed) | Studies report Decreases in consensus |
| Herb or Spice | berberine | Studies report Decreases in consensus |
| Herb or Spice | Curcumin | Studies report Decreases in consensus |
| Herb or Spice | galla chinensis (herb) | Studies report Decreases in consensus |
| Herb or Spice | garlic (allium sativum) | Studies report Decreases in consensus |
| General Substance | Specific Substance | Effect |
|---|---|---|
| Amino Acid and similar | Leonurine | Studies report Decreases in consensus |
| Amino Acid and similar | melatonin supplement | Studies report Decreases in consensus |
| General Substance | Specific Substance | Effect |
|---|---|---|
| Diet Style | animal-based diet | Studies report Decreases in consensus |
| Diet Style | gluten-free diet | Studies report Decreases in consensus |
| Diet Style | high beef diet | Studies report Decreases in consensus |
| Diet Style | high-fat diets | Studies report Decreases in consensus |
| Diet Style | high-protein diet | Studies report Decreases in consensus |
| Diet Style | high-saturated fat diet | Studies report Decreases in consensus |
| Diet Style | lacto-ovo-vegetarian diet | Studies report Decreases in consensus |
| Diet Style | low carbohydrate diet | Studies report Decreases in consensus |
| Diet Style | low fodmap diet | Studies report Decreases in consensus |
| Diet Style | low-fat diets | Studies report Decreases in consensus |
| Diet Style | magnesium-deficient diet | Studies report Decreases in consensus |
| General Substance | Specific Substance | Effect |
|---|---|---|
| Vitamins, Minerals and similar | Ferric citrate | Studies report Decreases in consensus |
| Vitamins, Minerals and similar | fluorine (i.e. tooth paste) | Studies report Decreases in consensus |
| Vitamins, Minerals and similar | folic acid,(supplement Vitamin B9) | Studies report Decreases in consensus |
| Vitamins, Minerals and similar | pyridoxine hydrochloride (vitamin B6) | Studies report Decreases in consensus |
| Vitamins, Minerals and similar | retinoic acid,(Vitamin A derivative) | Studies report Decreases in consensus |
| Vitamins, Minerals and similar | thiamine hydrochloride (vitamin B1) | Studies report Decreases in consensus |
| Vitamins, Minerals and similar | Vitamin B-12 | Studies report Decreases in consensus |
| Vitamins, Minerals and similar | vitamin b3 (niacin) | Studies report Decreases in consensus |
| Vitamins, Minerals and similar | vitamin b7 biotin (supplement) (vitamin B7) | Studies report Decreases in consensus |
| Vitamins, Minerals and similar | Vitamin C (ascorbic acid) | Studies report Decreases in |
The beef/protein diet are high in B-vitamins – thus very logical that both groups decreases.



Recent Comments