We are likely the sole firm claiming the use of AI for microbiome analysis that is in conformity today. Most firms in this area that claim using AI, refuse to even disclose which type of AI that they are using. Since our founding, we have been OPEN DATA. The logic used for every suggestion is show and links to every data source. We are about to file patents for our proprietary, PATENT PENDING, algorithms – meaning that shortly even the algorithms will be available for inspection.
Our core AI model is an old classic: fuzzy logic expert systems.
The foundations of fuzzy logic were laid in 1965 by Lotfi Zadeh, a professor at the University of California, Berkeley. In his seminal paper “Fuzzy Sets”, Zadeh introduced the concept of fuzzy set theory, which allows for degrees of truth rather than the classical binary true or false [A brief History of Fuzzy Logic].
The concept of expert systems, which are computer programs designed to emulate the decision-making abilities of a human expert, began to take shape in the 1960s. One of the earliest and most notable examples was MYCIN, developed in the early 1970s at Stanford University. MYCIN was designed to diagnose bacterial infections and recommend antibiotics based on a set of if-then rules derived from expert knowledge. [Knowledge Discovery from Medical Data and Development of an Expert System in Immunology]
I have had a few emails asking if I am over-flagging these issues on MicrobiomePrescription.
I used Perplexity.AI to get some numbers…. here is what was reported (with references to sources). Given the typical reasons that people get microbiome samples, the rates appear reasonable.
The National Institute of Health (NIH) statistics indicate that biofilm formation is present in about 65% of all bacterial infections and approximately 80% of all chronic infections.
In the context of human health, biofilms are responsible for about 80% of bacterial infections
D-lactic acidosis is considered rare in humans overall, but it may be underdiagnosed. Some experts suggest it should be looked for more often in cases of unexplained metabolic acidosis.
It is most commonly associated with short bowel syndrome (SBS). The incidence of SBS is estimated at approximately 2 persons per million per year. While not all SBS patients develop D-lactic acidosis, they are at higher risk.
In patients with short bowel syndrome, D-lactic acidosis appears to be a relatively frequent complication. One study found that all 29 SBS patients examined had experienced neurologic symptoms associated with D-lactic acidosis at some point [NOTE: SBS have a very high incidence of SIBO [src], so SIBO likely have an increased risk of d-lactic].
Histamine intolerance is estimated to affect approximately 1-3% of the general population. However, some experts suggest this number could be higher as the condition is often underdiagnosed.
Among people with digestive symptoms or conditions like IBS, IBD, and Crohn’s disease, a surprisingly high 30-55%may have histamine intolerance.
One study found that diamine oxidase (DAO) deficiency, which is associated with histamine intolerance, was present in up to 44% of the control population.
A more dramatic estimate suggests that histamine intolerance may affect 50-60% of the population, according to one source. However, this figure seems significantly higher than other estimates and may need further verification.
In people with digestive symptoms, one study showed that 30-55% also have histamine intolerance.
A reader asked, Which genus should I give highest priority in general?
This is an easy answer using the Conditions populated from studies on the US National Library of Medicine on 127 different conditions. The results are below for those that are seen in at least 10% of conditions.
Below that is a table showing the direction of shifts.
Taxa Name
Percentage Of Conditions with Shifts
Bifidobacterium
55
Prevotella
54
Bacteroides
52
Faecalibacterium
51
Lactobacillus
47
Blautia
44
Ruminococcus
43
Streptococcus
41
Roseburia
40
Escherichia
40
Clostridium
38
Parabacteroides
37
Coprococcus
34
Alistipes
33
Eubacterium
31
Shigella
31
Veillonella
30
Akkermansia
29
Fusobacterium
27
Dorea
27
Enterococcus
27
Anaerostipes
26
Dialister
25
Collinsella
25
Haemophilus
25
Klebsiella
25
Odoribacter
25
Megamonas
23
Bilophila
22
Desulfovibrio
22
Subdoligranulum
22
Lachnospira
21
Turicibacter
21
Phascolarctobacterium
20
Eggerthella
20
Enterobacter
20
Butyricicoccus
18
Oscillibacter
18
Porphyromonas
18
Megasphaera
17
Lachnoclostridium
16
Sutterella
16
Staphylococcus
16
Butyricimonas
16
Actinomyces
16
Oscillospira
15
Romboutsia
14
Parasutterella
14
Barnesiella
14
Campylobacter
14
Anaerotruncus
14
Paraprevotella
14
Methanobrevibacter
14
Catenibacterium
13
Butyrivibrio
13
Flavonifractor
13
Citrobacter
13
Coprobacillus
12
Adlercreutzia
12
Parvimonas
12
Rothia
12
Pseudomonas
12
Acidaminococcus
11
Fusicatenibacter
11
Gemella
11
Corynebacterium
11
Agathobacter
11
Ruminiclostridium
11
Lactococcus
11
Weissella
11
Slackia
10
Alloprevotella
10
Eisenbergiella
10
Direction Of Shifts for each bacteria
For some it is balanced, for others only one direction is significant.
“H” means that this genus for medical conditions are abnormally high for people with a condition
“L” means that this genus for medical conditions are abnormally low for people with a condition
Only bacteria associated with condition from Pub Med Studies
Suggestions
All Modifiers
Only modifiers reported to help at least one of the conditions from Pub Med Studies
Priority
Weight given
No ranking, all are both agree without ranking
Target Audience
Microbiome educated Medical types
Conservative Medical Type that are not familiar with the microbiome and recent research.
Condition Citations
No condition citations included
Most available condition citations for bacteria shift and suggestions are listed on one page with hyperlinks.
Microbiome Citations
All are available by individual links.
Only a token number of citations on how suggestions modify bacteria (why? full list can be massive)
Algorithm
Monte Carlo Model with multiple algorithms
Single Algorithm using above 85%ile and below 15%ile as bacteria selection criteria
Goal
Best suggestions based on the art of the microbiome
Educating and getting buy-in with conventional MDs
Special Goals
Focus on the holistic microbiome independent of specific diagnosis
Help MD pick the best for the microbiome choice from possible pro-forma treatments.
A possible example: the MD wants to prescribe an antibiotics for a condition. Usually, there are a half dozen possible choices. Ideally, the MD will be willing to go with the one that is best for the microbiome when shown the evidence from the computations.
Which is best?
The Cross-Validated has a limited list because it is very time consuming to populate the data needed for it. For items like biofilm, d-lactic acid and histamine — it is likely the best choice but the suggestions should be checked with the “Just give me suggestions” and the final suggestions should be only ones that both agree with — subject to review by your medical professional.
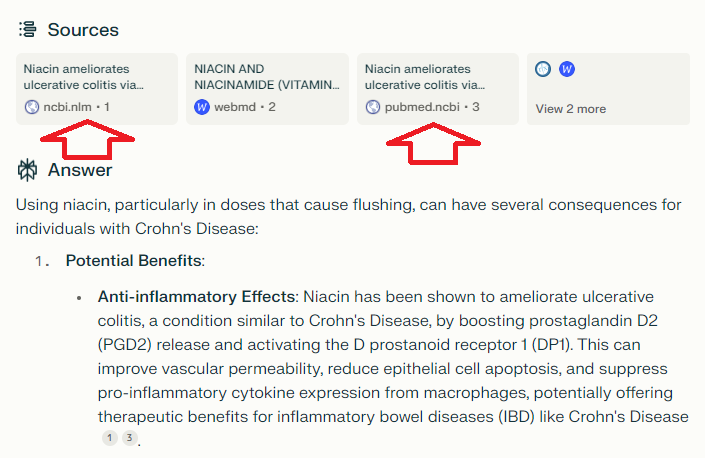
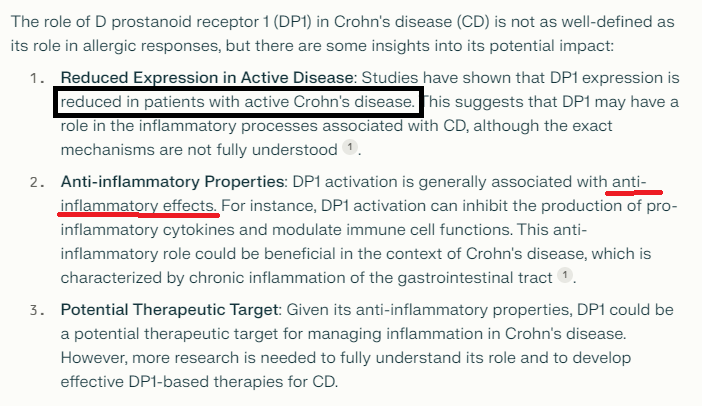
Should I be taking flushing niacin with Crohn’s Disease. I feel better after taking it, but I read that it encourages the release of prostaglandins, particularly prostaglandin D2 (PGD2) and prostaglandin E2 (PGE2), rather than histamine.
My first step is to go to Perplexity.AI and ask questions there and then check the sources cited. I then use this to jump into PubMed to get better information. As with all AI, you need to learn to ask clear specific questions.
Questions:
What are the consequences of using flushing niacin with Crohn’s Disease?
Daily energy, carbohydrate, monosaccharide, starch, sucrose, fructose, poly-unsaturated fatty acids, omega-3 fatty acids, fiber, vitamin E and C, thiamine, niacin, pyridoxine, Mg, P, Fe, Cu, Zn intakes were significantly lower in Crohn’s Group than in Control Group.
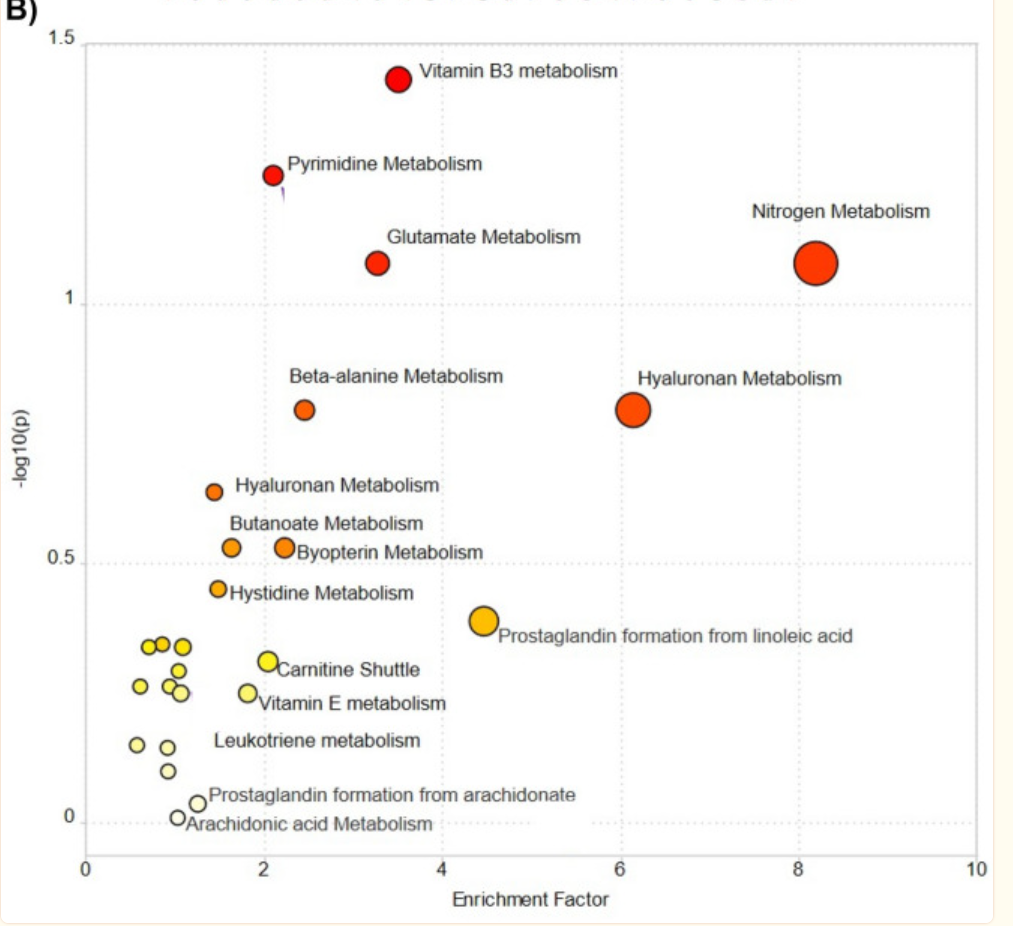
“Interestingly, high-dose vitamin B3 treatment has been shown to ameliorate ulcerative colitis through increased prostaglandin D2 synthesis in mice54. Thus, niacin supplementation can be a potential therapeutic target to be investigated in CD as well. In addition, untargeted metabolomics showed the dysregulation of pathways related to pyrimidine, glutamate, and nitrogen metabolism. “
Second Question: Niacin and MCAS
Mast cell activation syndrome (MCAS) is another issue that the person is dealing with.
Asking more we get a yes/no with lacking studies.
Digging more we see other things that are EITHER/OR. Thus PGD2 in isolation is not connected to activation; rather activation is conditional on multiple factors (one of them is PGD2). “MCAS is associated with a variety of mediators beyond PGD2, including histamine, tryptase, leukotrienes, cytokines, heparin, PAF, neuropeptides, and other eicosanoids.”
“Tests for serum PGD2 have similar drawbacks, as processing of peripheral blood samples can trigger non-MC cellular elements to release PGD2; ingestion of niacin is also associated with elevations in serum PGD2 ” [1994] so this may rendering test results invalid.
“Mediators other than tryptase, including urinary metabolites of histamine, prostaglandin D2 (PGD2), and leukotrienes, are also available but less specific for MCs and MCAS [28, 29, 30••]. Additionally, the sensitivity and specificity of these markers have not been determined, nor have the reliable indicators of systemic MC activation, such as significant increase and cut-off levels. ‘
“PGD2, while primarily released by MC, is also produced by other immune and nonimmune cell types [42–45]..elevations in PGD2 might be due to a pathologic process independent of MC activation.”
Concentrating on Niacin and Histamine, Perplexity gives plus and minus, concluding “In summary, niacin can both positively and negatively impact histamine levels and symptoms.” So, our bottom line is that it depends on the individual.
The responses mention S-adenosylmethionine (SAMe) being consumed with Niacin.
Which implies SAMe should be taken with the Niacin.
Bottom Line
The final decision is always the person in consultation with their medical professional. Using Niacin as a treatment for Crohn’s Disease is heading for clinical trial and suggested by a 2023 metabolic shifts study on Crohn’s. Given the low risk (assuming medical monitoring for niacin risk), I personally would favor doing it (making sure their usual MD is aware of the dosage and a possible need to monitor).
The purpose of this post is to show a method of gathering information to make better health choices. I have fallen in love with Perplexity.AI because it cites studies on PubMed often and it’s suggestions are easy to verify and evaluate. It also prompts for follow up questions.
We discovered a multitude of deficiencies that may need to be supplemented (factoring in poor absorption due to Crohn’s) including:
SAMe (because of the niacin use)
fructose,
poly-unsaturated fatty acids,
omega-3 fatty acids,
vitamin E and C,
thiamine,
niacin,
pyridoxine,
Mg,
P,
Iron,
Copper,
Zinc
This lead to the logic questions: What are all the deficiencies seen in Crohn’s disease that can be supplemented? Full Answer.
P.S. The time it took to do the above was about 90 minutes,
Over the years, I ended up with some simple rules for what I will buy. The rules are simple:
Trademarked/copyrighted/patented species, ideally ones with some research. All of them are listed on this page with links to the research. Ideally, just the one researched for your conditon.
Single species with (almost) no fillers. There are precisely three sources that I use:
Maple Life Science™: No strains yet, but shipments usually have manufactured date within 4 weeks of arrival (i.e. FRESH). Contains FOS. EBAY BASED — Ships world wide, best pricing!
Bulk Probiotics: US based Newbie — but has some species not available at the other two sites. No other ingredients just the bacteria. Specifically, Lactobacillus Jensenii that has great potential for Crohn’s disease.
NOTE: none of these sell though retail outlets. This keeps their costs down and their product fresh.
Personal Experience
This family experience with all of the single strain probiotics has been:
If we have not used before, we notice changes within 1-3 days in stools, symptoms, etc. These may not always be desired symptoms (i.e. one probiotic before bed, kept us awake all night; other probiotics give us deeper and longer sleep than normal). In some cases, changes are observed within 60 minutes. Changes of stools are a common change.
We usually do one new probiotic at a time for 2 weeks to get “a feel” for what it does
We constantly rotate – never more than 1 month on any probiotic “It has done what it is going to do“
“If there is no changes, the probiotic is dead, Jim” or not of benefit to you. Move on. A common observation that we saw using most probiotics purchased from local stores.
Medical Claims
I do not trust any claims on the bottle
The outcome of the first series of health claim applications for probiotics in Europe as evaluated by the European Food Safety Authority (EFSA) has, up to 2013 almost completely yielded negative results. All recent applications also have been rejected, including the latest on prevention of mastitis in breastfeeding mothers.
Bacterial species were misidentified 35-43% of the time
Misidentifications included stating a name that had been changed
i.e. “Streptococcus faecium” and not Enterococcus faecium
Non existent species: “Lactospore sporogenes“
Identification and antibiotic resistance of isolates from probiotic products. Abstracts of 101st ASM General Meeting. The American Society for Microbiology, Washington DC, USA,
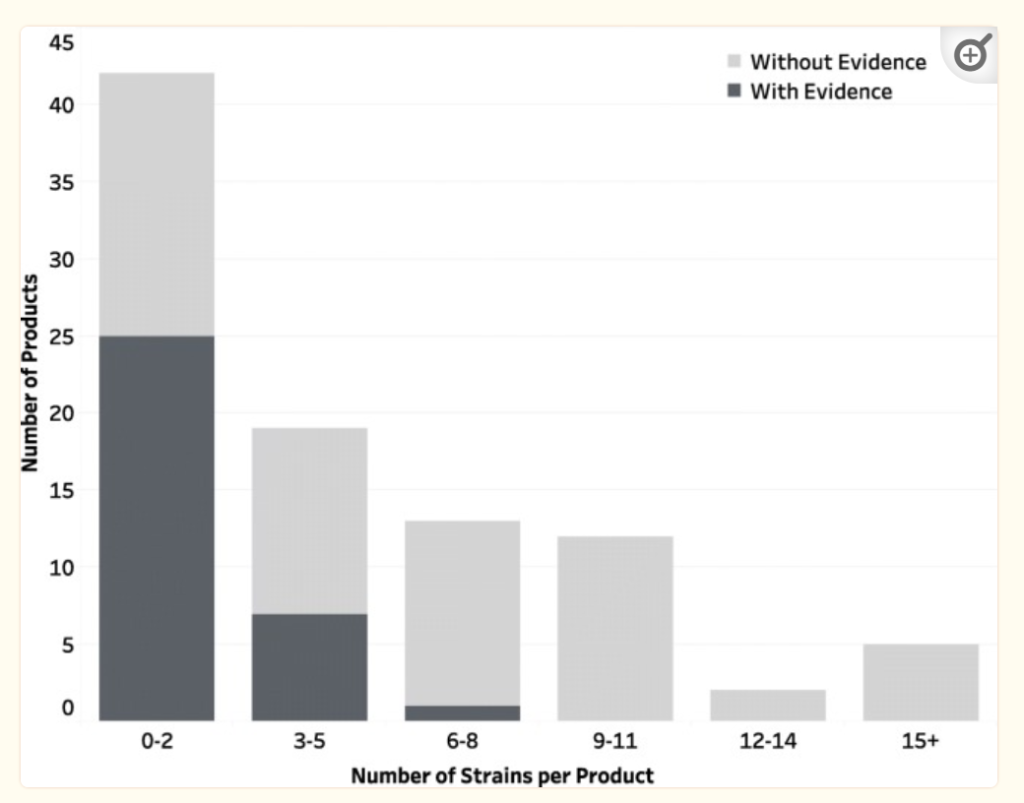
for 30 dried probiotic supplements tested,
11 contained no viable bacteria,
only 7 contained all claimed species
18 had species other than those on-label.
Deficiencies in microbiological quality and labelling of probiotic supplements [2002]
63% of the UK products tested were below standard.
Enterococcus faecium (not stated on label) and was labelled with the misleadingand invalid name ‘‘L. bifidus’’.
This cites this as the minimum recommended standard.
Genus and species names, which should adhere to current scientifically valid nomenclature.
Strain designations for each strain in the product. Designations used should enable tracking of the strain to entries in strain depositories and linking to published studies.
Statement of quantity (using CFU or other validated measure) of live/active microorganisms through the use-by date.
Use-by date.
Statement of benefit is not required, but if present must be supported by a human study showing the benefit at the dose delivered in the product.
Proper storage conditions Required.
Company contact information.
Warns of genetic drift (bacteria mutations) and cites the popular
L. rhamnosus (GG) that exhibited multiple genotypes in consumer products (Sybesma et al., 2013). So the bottom of LGG you buy may not be the same strain as the studies used.
Today, I looked at the bacteria associated to histamine conditions and found the quality of research lacking. I had imported a lot of data from Alison Vickery web site. Unfortunately some of the bacteria cited as producing histamines according to Kyoto Encyclopedia of Genes and Genomics lack the enzymes to produce histamine. Today, I spent the morning checking published studies on the US National Library of Medicine to see if there is any evidence of histamine production there — little luck. As a result, I deleted the data since it was not at the desired quality.
Quick Summary
It is strongly recommended that the sources be read before taking any actions
Items that may help:
DAO
Anti-Histamines
HNMT histamine N-methyltransferase (prescription)- is possible help
Items to Avoid:
Vitamin B1
Vitamin C
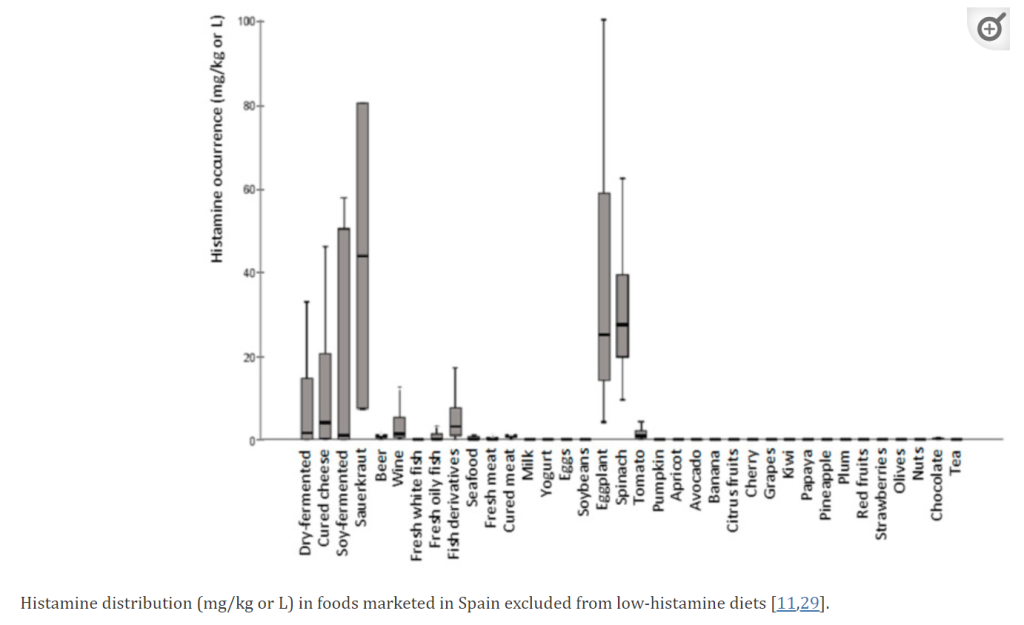
Histamine Liberators [2015] – Many of these items have zero histamine (research is sparse)
Tomatoes, eggplant, spinach, fish, chicken and every stored meat. All fermented food (cheeses, sausages, sauerkraut, wine, beer, champagne …
MECHANISM: “The presence of putrescine, which may interfere with histamine degradation by the DAO enzyme at the intestinal level, could partly explain the reason why certain foods (i.e., citrus fruits and bananas) were also frequently reported in low-histamine diets” [2021] This link has a table showing the amount in various foods.
rs1050891 (C314T polymorphism) with the minor T allele [2010]
Gastrointestinal Disorders
Medications: Certain medications like antibiotics, antidepressants, antiarrhythmics, muscle relaxants, and NSAIDs can inhibit DAO activity or block histamine breakdown. Table below is from a [2021] article.
Diet: Consuming foods rich in histamine (aged cheese, fermented foods, alcohol, etc.) can overwhelm the body’s ability to break down histamine, leading to an accumulation.
Repeatedly state with reference in this [2021] study.
“Reduction of Proteus and Raoultella and the species Proteus mirabilis. “
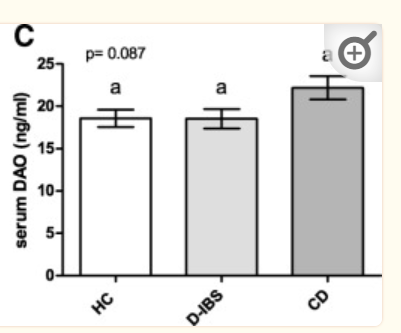
Perplexity AI suggested: “Conditions like inflammatory bowel disease (IBD), leaky gut syndrome, and other gastrointestinal disorders can impair DAO production and histamine breakdown.” Unfortunately it’s sources were poor. Checking PubMed, we see the following studies indicate that it appears to apply possibly apply only to one type of IBS.
“DAO levels were significantly higher in Crohn’s patients with the active stage compared to controls.” [2019]
“histamine levels were normal in CD and UC.” [2015]
“subjects with irritable bowel syndrome[IBS] could be discriminated from healthy controls using their metabolic fingerprints… Levels of some urinary metabolites including histamine correlated significantly with irritable bowel syndrome symptom severity scores.” [2019]
“The mast cells’ histamine release appears linked to GI-involving diseases like celiac disease (CD), eosinophilic gastroenteritis (EGE), and mast cell activation syndrome (MCAS) “[2020]
Intestinal barrier dysfunction: Impaired intestinal barrier function (leaky gut) can allow increased absorption of histamine from the gut into the bloodstream, contributing to histamine overload.
No clear strong evidence found, a reasonable speculation
Reduced Prevotellaceae, Ruminococcus, Faecalibacterium and Faecablibacterium prausnitzii [2022],
Bacterial overgrowth: An overgrowth of certain bacteria in the gut can lead to excessive production of histamine, overwhelming the DAO enzyme’s capacity to break it down
“a significantly higher abundance of histamine-secreting bacteria, including the genera Staphylococcus and Proteus, several unidentified genera belonging to the family Enterobacteriaceae and the species Clostridium perfringens and Enterococcus faecalis” [2022]
Probiotics
For a list of studies, click here. The following has some evidence of reducing histamines
Bifidobacterium bifidum
Bifidobacterium lactis
Enterococcus faecium
Lactobacillus casei Shirota
Lactobacillus paracasei
Lactobacillus reuteri
Lactobacillus rhamnosus GG & GR-1
Mutaflor (Escherichia coli strain Nissle 1917)
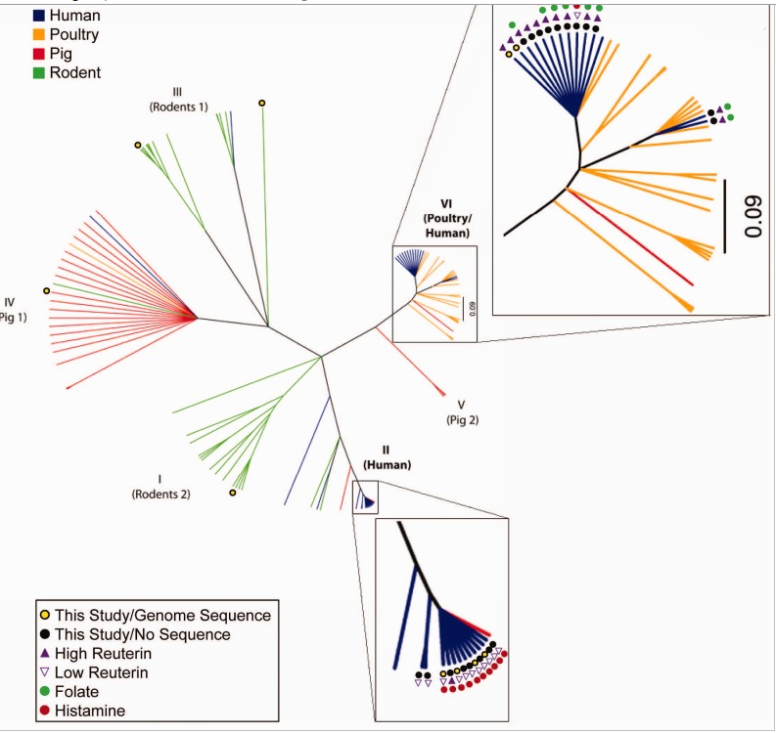
Caution should be taken because one strain may produce histamine and another reduces it. The chart below show different strain of Lactobacillus reuteri. Some produces histamine and others do not. Bifidobacterium are in general safe. Lactobacillus has risks — if you try them, do one at a time when you are stable. Remember most probiotics are sold by Species and not Strain; same species from two different manufacturers may be different strains — so how lucky do you feel.
This is now on Microbiome Prescription and is based on the count of species known to produce histamine in your sample.
Histamine N-methyltransferase
A reader asked about this item that I missed.
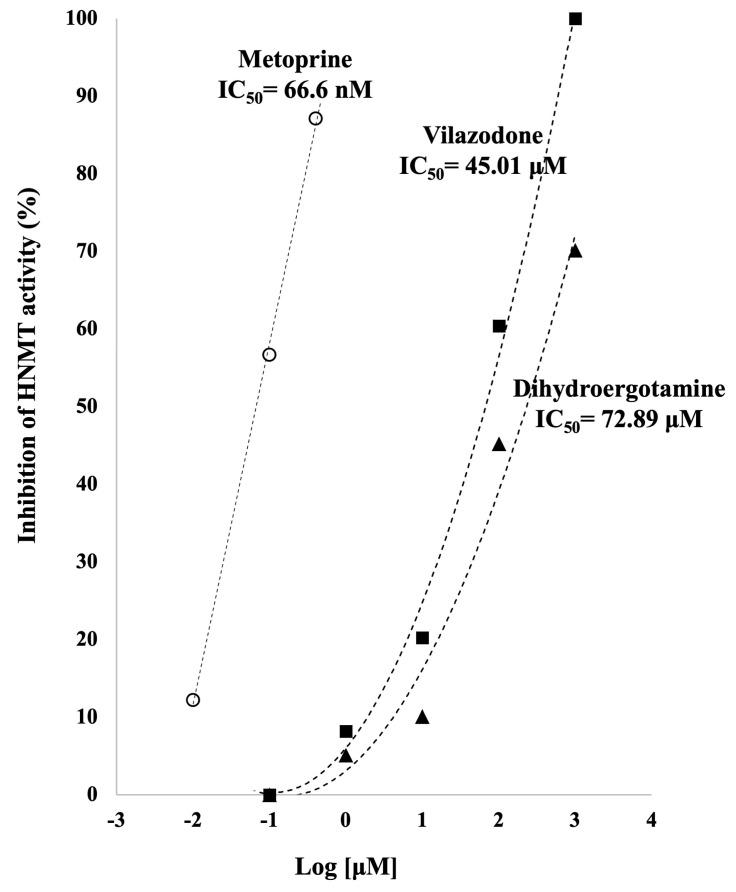
Histamine N-methyltransferase (HNMT) is an enzyme that plays a crucial role in the inactivation of histamine in central nervous system, kidneys and bronchi. Inhibition of HNMT is known to have a potential role in treating attention-deficit hyperactivity disorder, memory impairment, mental illness and neurodegenerative illnesses.
Genetic polymorphisms in histamine-related genes, including FcεRI and HNMT, were suggested to be involved in mast cell activation and histamine metabolism. Several genetic polymorphisms of leukotriene-related genes, such as ALOX5, LTC4S, and the PGE2 receptor gene PTGER4, were suggested to be involved in leukotriene overproduction, a pathogenic mechanism.
A common complaint that I have heard is a lack of knowledge about the microbiome by treating MDs. This issue is compounded by MDs allowing only 10-15 minutes appointments. Many of complaints are from EU Countries where their MD have limited mastery of English.
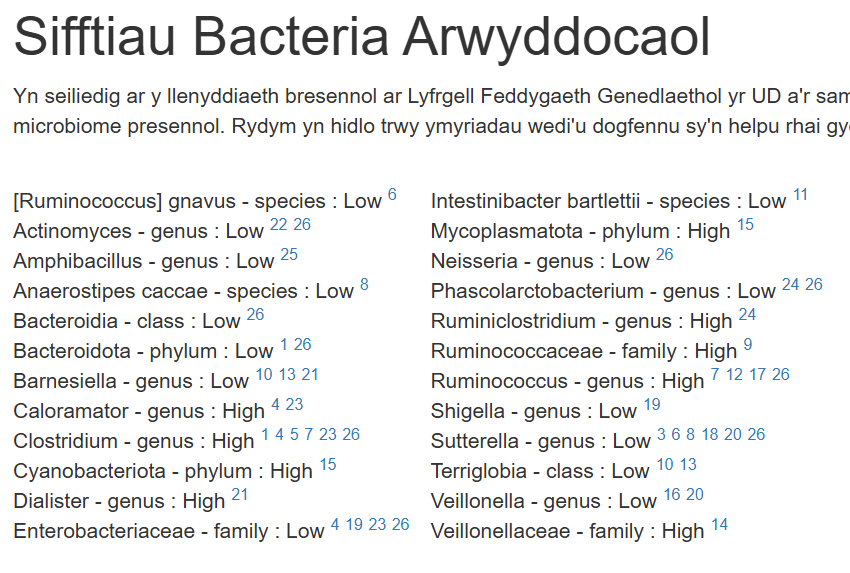
This reported is targeted for those MDs using the following strategy:
A short section of what should be substances should be tried to be reviewed by the MD.
Every item is linked to one or more studies where it was found helpful for some people (responders)
Every item is linked to the bacteria that it changes
A break down of all bacteria out of range according to studies on this condition, with links.
A detail cross reference on the bacteria that each substances. The goal is to encourage MDs to insure at least one substance is advocated for each bacteria
A long list of the studies cited. This list is intended to overwhelm the MD with evidence. One or two studies is easy to dismiss for many MDs. A long list is hard to dismiss psychologically..
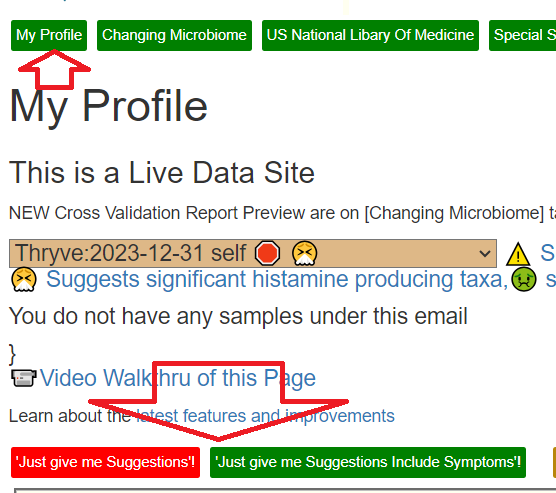
How do I get this Report?
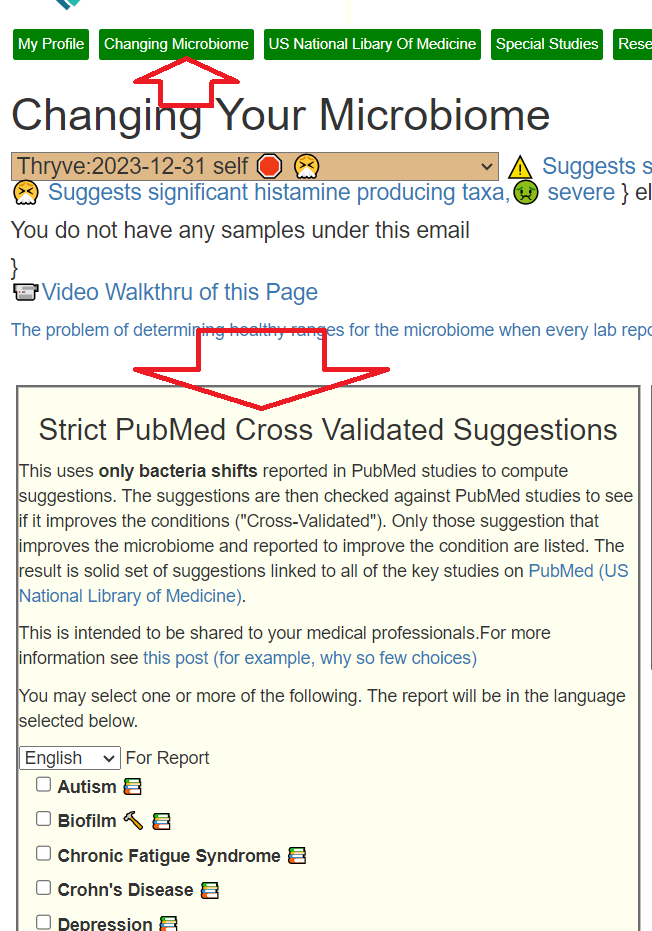
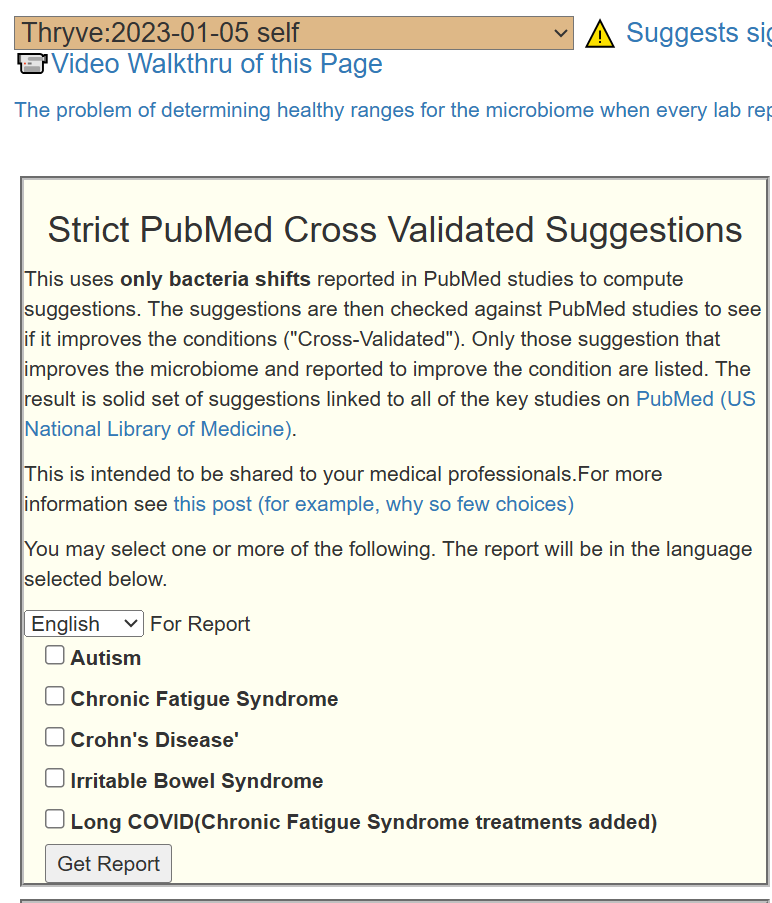
Assuming you have transfer or uploaded a sample to Microbiome Prescription, go to the [Changing Microbiome] tab. You will see your samples (and the active one). Below it is this section:
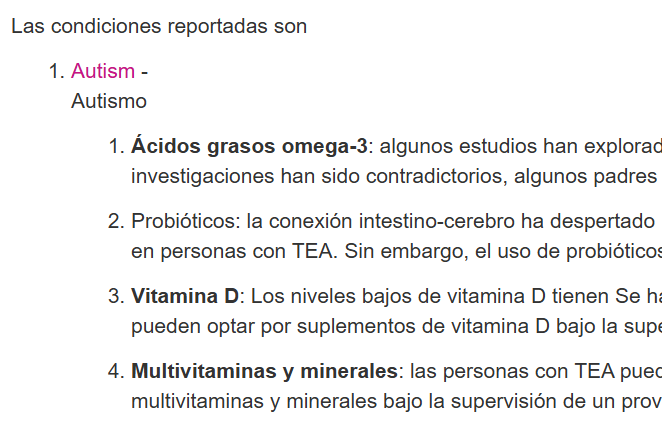
Pick the preferred language. Click the conditions you have. Click Get Report. If your condition is missing, see the bottom of this post for why and how you can change this.
How this Report is different
This uses a strictly “by the medical book” analysis and will likely generate some suggestions different from other reports on the site. This is required to be able to do cross references for every item.
Typical Knowledge Section
This is actually coming from ChatGPT and is a likely match to the MD’s “common sense”
Bacteria Being Targeted
This is next because we want to explain WHY we are making suggestions before presenting them.
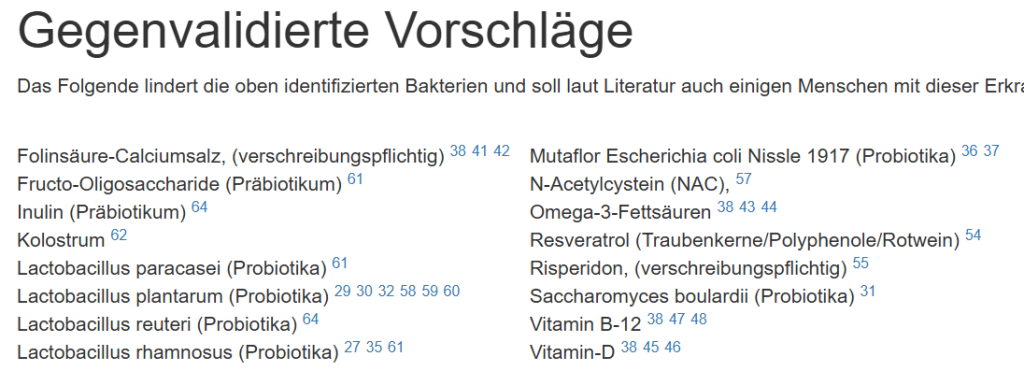
Substances to Consider
This list may be long or short (depending on conditions). Many MDs will likely be happy with most of these suggestions. For those that they are unsure about, we have a link to studies that may persuade them over time.
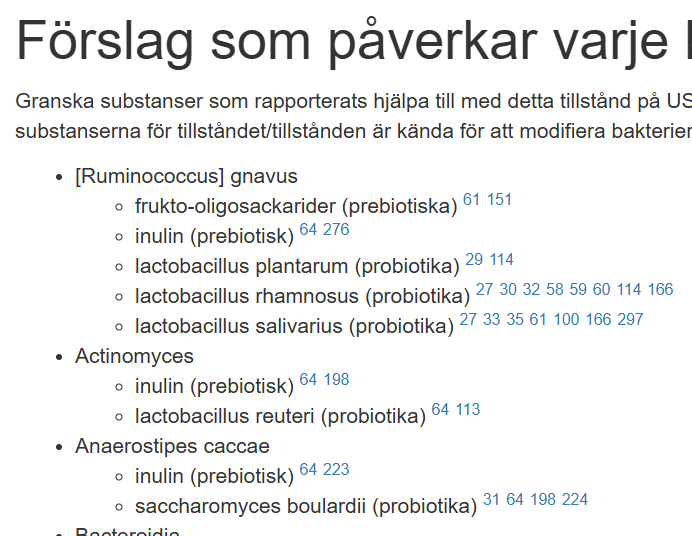
Substance Impact on Bacteria
This is intended for MD education. It illustrates that the microbiome can be manipulated and there are lots of studies.
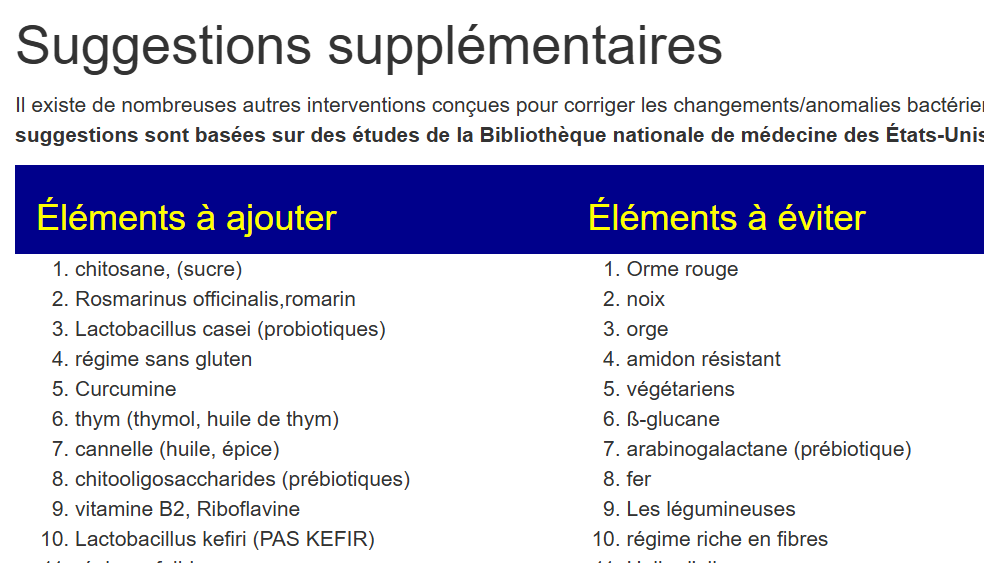
Additional Suggestions
This is intended to be a carrot for the MD to learn more.
References
This speaks for itself, and that the suggestions are well researched.
Why is your Condition not listed?
The simple reason is that someone has to diligently go through the literature to assemble all of the information by hand. Often a report will have more than 600 citations – that’s a lot of work. For Autism, some parents did the work and this we have a report for autism. If you are interested in doing this research for your missed condition(s) see Help Needed to Improve Suggestions for Autism. for the steps needed.
Just Identifying the Bacteria for more conditions….
Bottom Line
This report was engineered by trying to walk in the mind frame and world of the MD. Speak to him in his preferred language and way of thinking.
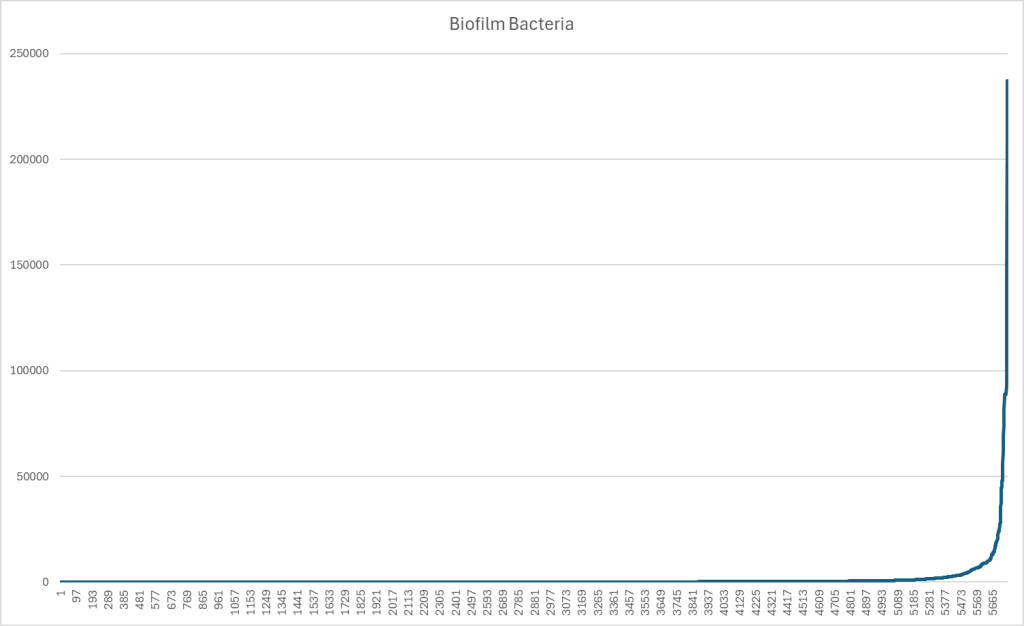
A reader in Europe asked about this. I know it is a popular topic. So, I searched PubMed for the known biofilm forming bacteria and will be adding percentile ranking by labs in the coming days.
Raw Count Chart
As you can see below — a lot of people have ZERO of these bacteria. Other people may have 25% of their microbiome containing them. IMHO, influencers have seized on this concept as a “boogey man” for every one; it is not.
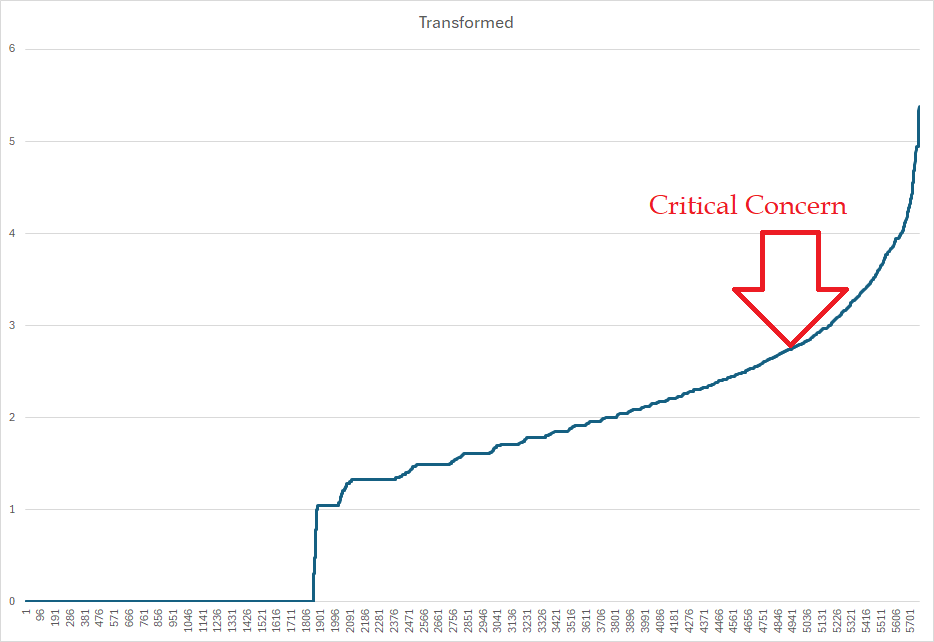
Transforming the data to get a Kaltoft-Møldrup estimator of the point of concern, we get a count of 565/million or 0.0565% being the threshold that action is strongly suggested. That is, with 85% of samples, it does not appear to be a significant issue. For 15%, it is
Stay tune. It will be added to the health analysis page with suggestions annotated with possible biofilm breakers for people exceeding 80%ile.


Recent Comments