This was a request from a reader and I will do a direct approach Items reported from studies.
Items from Published Studies
- Tryptophan: This is an amino acid that the body converts into serotonin. It’s found in foods like turkey, cheese, and nuts, but it’s also available as a supplement.
- “Tryptophan, an indispensable amino acid, is needed to support protein deposition, and the synthesis of the neurotransmitter serotonin,”[2022]
- “Tryptophan is the only precursor of serotonin and mediates serotonergic activity in the brain. Previous studies have shown that the administration of tryptophan or tryptophan depletion significantly alters cognition, mood and anxiety. ” [2017]
- “Supplementation with B vitamins and magnesium has an influence on the Trp concentration.” [Tryptophan status in autism spectrum disorder and the influence of supplementation on its level, 2017]
- Tryptophan supplementation and serotonin function: genetic variations in behavioural effects [2018]
- 5-HTP (5-Hydroxytryptophan): This is a by-product of tryptophan and is directly converted into serotonin in the body. It’s often used as a supplement for mood enhancement.
- Tryptophan-enriched diet or 5-hydroxytryptophan supplementation given in a randomized controlled trial impacts social cognition on a neural and behavioral level [2021]
- 5-Hydroxytryptophan (5-HTP): Natural Occurrence, Analysis, Biosynthesis, Biotechnology, Physiology and Toxicology [2020]
- “An excess of 5-HTP may be responsible for serotonin syndrome (see Section 8.2.1) and an excessive treatment was found to be associated with severe side effects, including behavioral disturbances, abnormal mental functions, and intolerance.”
- St. John’s Wort: Often used for depression, St. John’s Wort is believed to affect serotonin levels, although its exact mechanism is not fully understood.
- Extractive from Hypericum ascyron L promotes serotonergic neuronal differentiation in vitro [2018]
- Mechanism of action of St John’s wort in depression : what is known? [2003]
- “St John’s wort extract leads to a downregulation of beta-adrenergic receptors and an upregulation of serotonin 5-HT(2) receptors in the rat frontal cortex”
SAMe (S-adenosylmethionine): This is a compound naturally found in the body that is thought to enhance neurotransmitter production, including serotonin.- “Use of SAMe elicited no significant adverse effects beyond placebo, however it was implicated in one case of serotonin syndrome-like symptoms.” [2018]
- Omega-3 Fatty Acids: Found in fish oil and certain plant oils, omega-3 fatty acids are linked to improved mental health and mood regulation, possibly through influencing serotonin pathways.
- Effect of the dietary intake of fish oil on psycho-social behavioral disorder caused by social-defeat stress [2022] “This improvement could be explained by the increase in serotonin synthesis in the hippocampus.”
- “Fish-oil supplementation decreases Indoleamine-2,3-Dioxygenase expression and increases hippocampal serotonin levels in the LPS depression model” [2020]
- Vitamin B6 and B12: These vitamins are important for serotonin production. A deficiency in these vitamins can lead to reduced serotonin levels.
- “vitamin B6, a cofactor in the tryptophan-serotonin pathway critical to mood regulation.” [2023]
- Link between higher levels of homocysteine and depression [2012]
- “Homocystcinc is reconstituted into methionine, which is essential to the production of neurotransmitters such as serotonin and dopamine which elevate mood. This reconstitution requires B-group vitamins, especially folic acid and B12. “
- Magnesium: This mineral plays a role in many biochemical reactions in the body and has been suggested to have a mood-stabilizing effect, possibly by influencing serotonin.
- Effect of subacute manganese feeding on serotonin metabolism in the rat [1978]
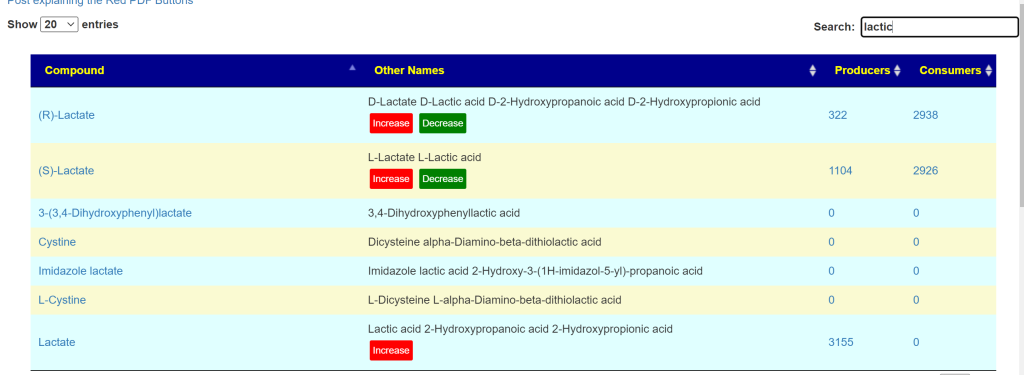
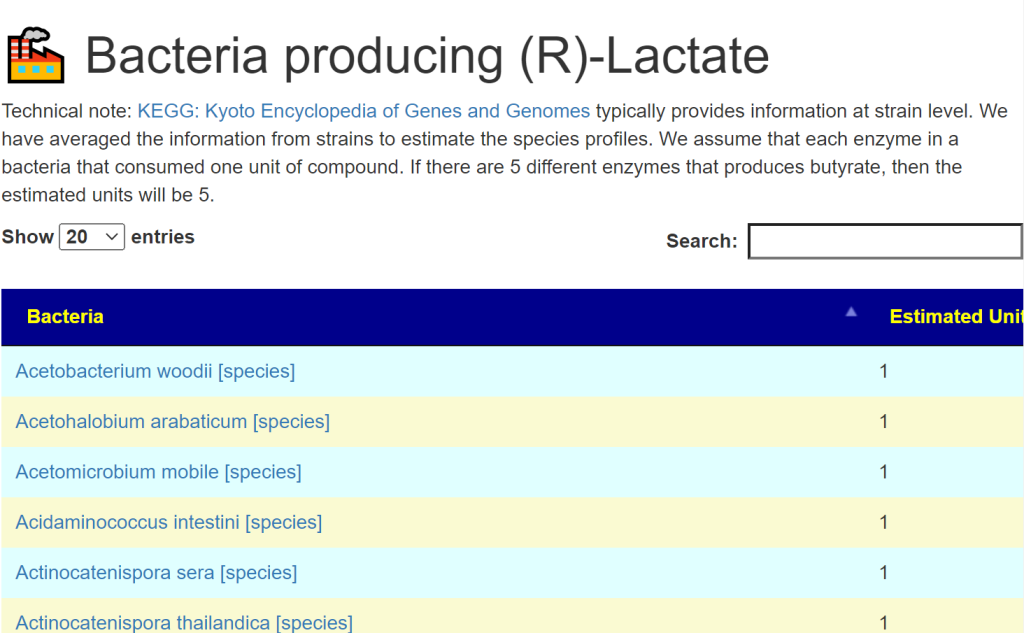
- Probiotics: Some research suggests that gut health can impact serotonin levels, as a significant amount of this neurotransmitter is produced in the gut.
- lactobacillus plantarum
- Lactobacillus rhamnosus GG
- Mutaflor (Escherichia coli strain Nissle 1917)
Foods
- Foods with Tryptophan: “chicken, soya beans, cereals, tuna, nuts and bananas’ may serve as an alternative to improve mood and cognition. ‘ [2013]
- Withania somnifera ( ashwagandha)
- “subjects showed significant increases in serum serotonin, gastrin,” [2024]
- kiwifruit
- ” treatments increased urinary concentration of the serotonin metabolite” [2023]
- poly-γ-glutamic acid with vitamin B6
- “a greater increase in the group C intervention (4.59 ± 38.5 ng/mL) in serum serotonin concentrations’ [2021]
Vitamin D has no effect (multiple studies)





Recent Comments