I am living with LongCOVID following infection in March / April 2020. I contracted COVID-19 in the workplace, employed as a pharmacist at an NHS hospital in South Wales, U.K.
I shared my story with WalesOnline at the latter stages of 2020 due to the lack of awareness around LongCOVID, and I share with you below for your interest.
Unfortunately, I am still troubled by GI symptoms and despite improving over the past few months, I’m still having difficulty with bowel urgency / diarrhoea and mild abdominal pain. I lost 10kg in 10 weeks between July – Sept. 2020 (72kg at my lowest); thankfully this has recovered and I have gained weight, albeit chubbiness, weighing 88kg last week. I was diagnosed at the start of 2021 with ‘post-viral IBS’ and ‘leaky gut syndrome’, but GI clinicians are at a loss of how to proceed with my symptoms, hence my purchase of the BiomeSight kit. I have tried numerous diets (FODMAP, dairy-, gluten-free), again, to no avail.
I approach my 20th month since first being infected and I am still quite a distance from where I was pre-COVID doing all I possibly can to recover, so I would be extremely grateful for your insight, not only to help myself, but others in a similar situation.
Approach #1
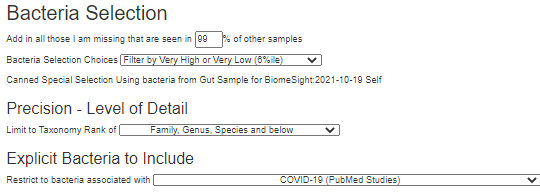
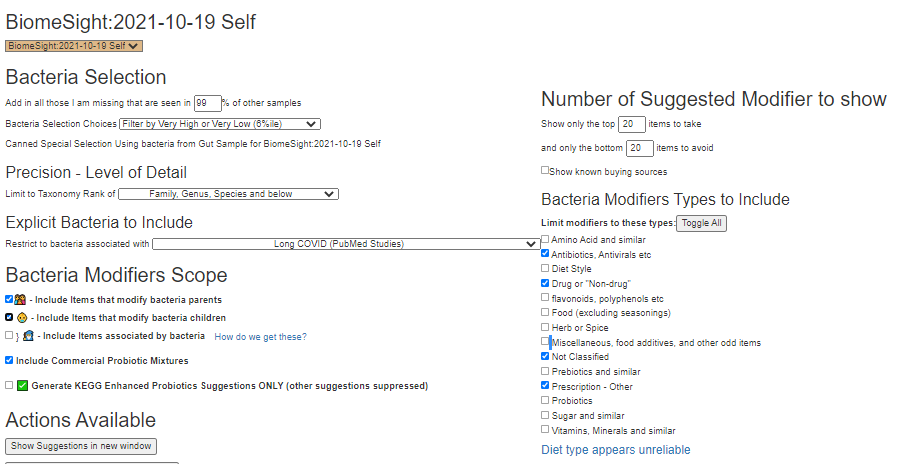
As we have two microbiome profiles for COVID from the US Nation Library of Medicine, I will apply each one using 6%ile filter (values in the top or bottom 6%ile) to get a feel for the ground work. Then I will apply the ME/CFS for a third one (because of the similarity of Long COVID and ME/CFS).
For those not familiar with selecting
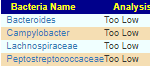
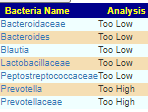
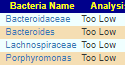
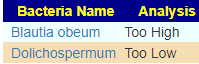
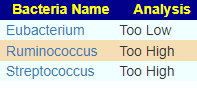
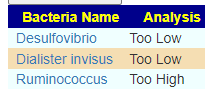
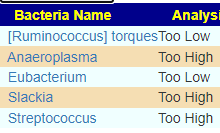
We end up with a short lists of bacteria (the titles links to the bacteria and studies reporting these shifts)
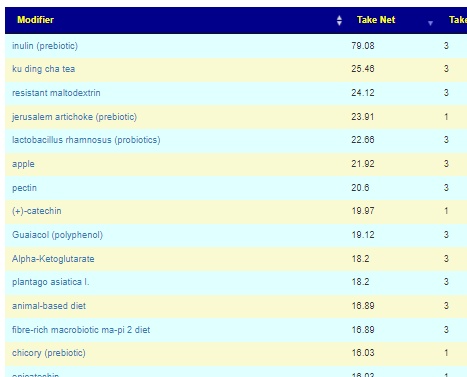
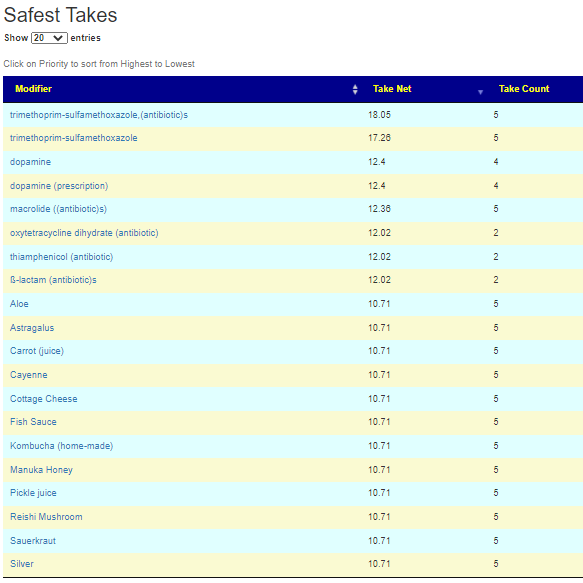
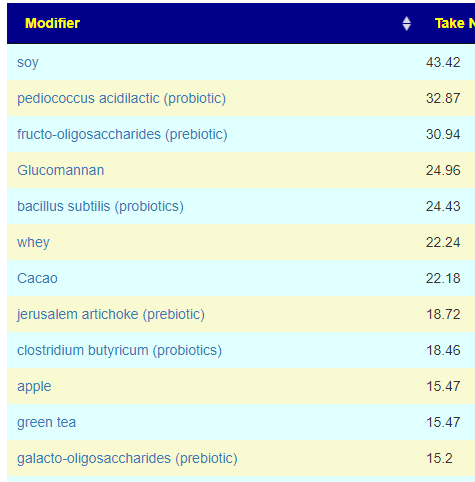
Almost everything is too low. Rather than examining suggestions from each of them, I will go directly to the consensus report. We hit a surprising 108 items on the safest take (items that will not shift any of the above in the wrong direction). Most are recommended in each case (Take Count = 3)
Safest Take
A few quick notes: Apples are very rich in pectin (some studies used apples and other pectin — I always try to keep data as reported and not do ‘well it’s just like…’ simplification). Similar with inulin and chicory.
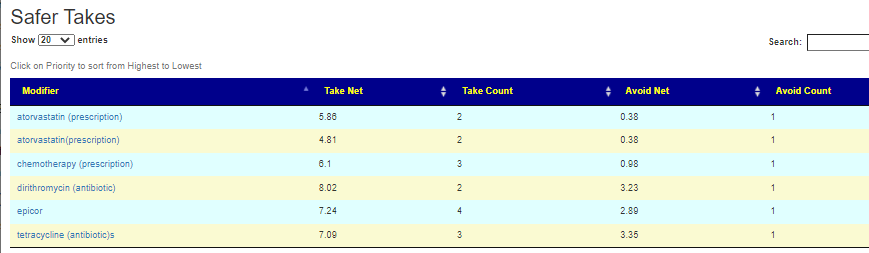
The Safer text (some pro and some con) list was short and a bit of a mixed bag. With 108 items on safest, I would tend to ignore these. No need to include them.
On the avoid list we have “magnesium deficient diet” — which usually translates to magnesium rich or supplements.
I attach the complete list below of 304 different items.
This person is a pharmacist and thus looking at off-label drugs may be interesting for him to review. There are no accepted drugs for Long COVID, however, for ME/CFS often the top off-label drugs have often been used (with good results) by ME/CFS specialist (often at risk of professional censure). I have also added in CFS/ME with IBS (only Bacteroides Low was a match), and IBS to the consensus report.
The Criteria Selection being tried
Bacteria selected from IBS
The number of drugs that could influence these bacteria (good or bad) was almost 1300. I included some non prescription items to serve as a reference point (i.e. do drugs do better than some alternatives). In the small list of antibiotics at the top, I see several of the works for ME/CFS antibiotics — especially, those used by Cecile Jadin, MD: Tetracyclines, macrolides. Jadin does antibiotic rotation: 10 days on and 20 days off, then change to the next antibiotic. I have seen a few PubMed studies finding rotation was superior.
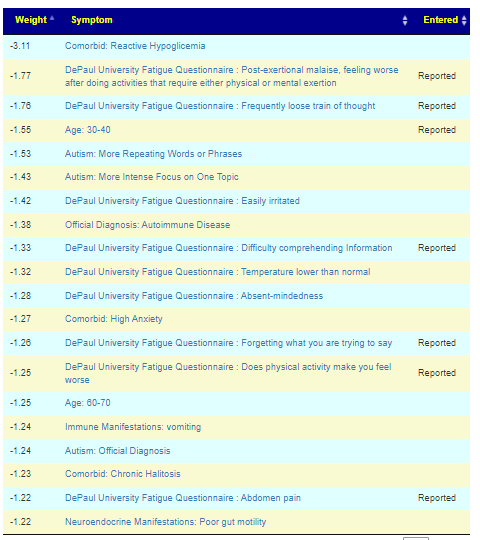
Above we worked on diagnosis, we are now going to switch to symptoms. My experience is that symptom-to-bacteria associations are much stronger than diagnosis to bacteria. Mileage will vary.
Oh have I mentioned that the symptom prediction from bacteria matches my symptoms almost completely? I think it’s 17 out of 20. Pretty incredible.
From a user in Europe by email on 11/11/2021
Below are his reported symptoms against predicted symptoms. It is interesting that many several predicted symptoms are autism related (which he does not have). This approach uses the bacteria that citizen science has associated to the symptoms (instead of clinical studies to the diagnosis). In theory, it will often be more sensitive for identifying the bacteria of concern.
See the video for how we do this. The final suggestions in Excel/csv format is below
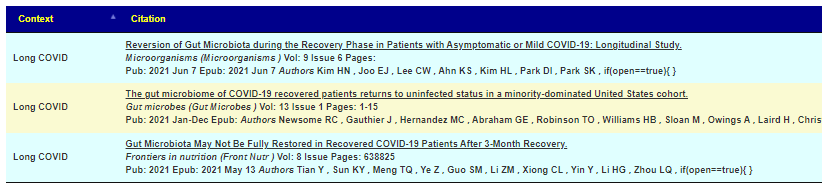
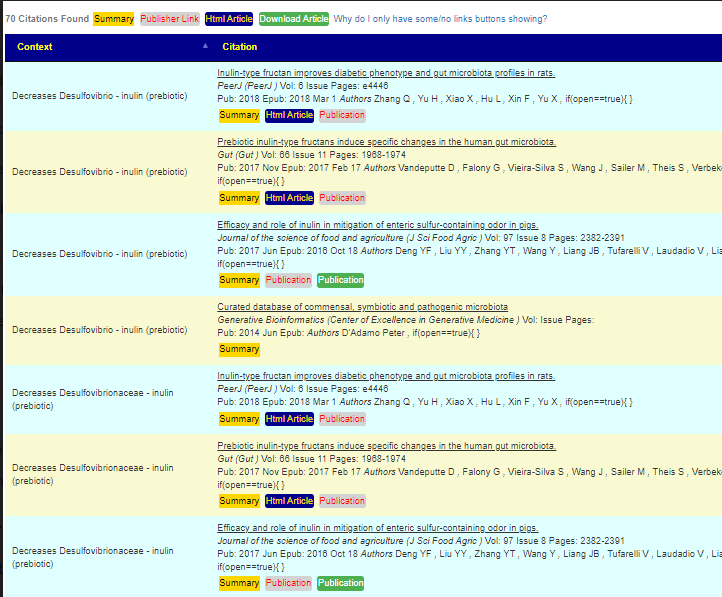
The intent of Microbiome Prescription site is to improve the odds of helping by working off studies on the US National Library of Medicines (at present, there are almost 6000 articles that we were able to harvest information from). We are very open on the where we get data, for example – for where we get the list of bacteria associated with a condition
From https://microbiomeprescription.com/citations/PubMedCitations?Code=LCV
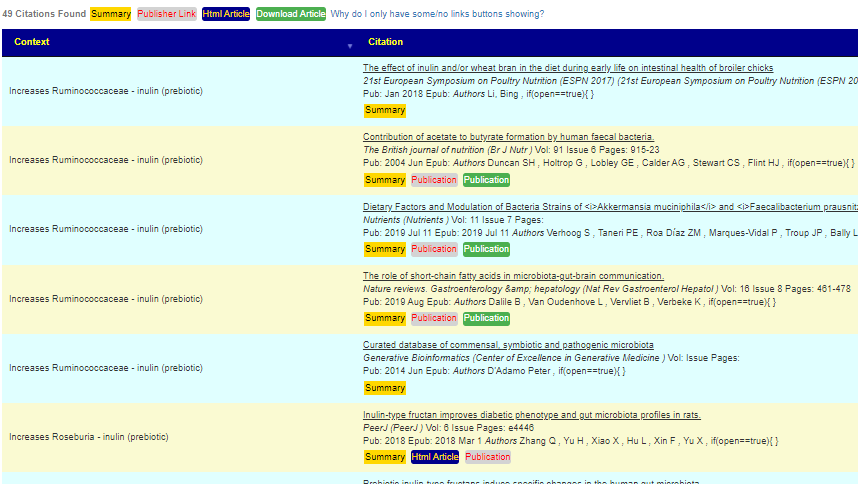
And sources for how we know that something changes bacteria populations. In this case because of the high number of studies on inulin it will receive a high weight if certain bacteria are being targeted.
Example of what inulin impacts
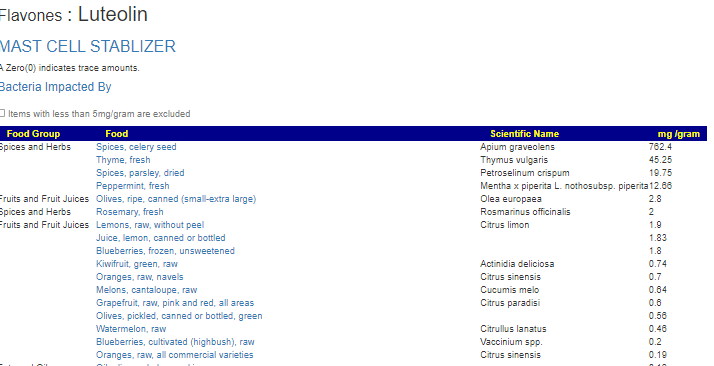
We also try keeping faithful to the term used in the studies — apple contains large amounts of pectin, while some would just combined these to pectin (or apples), we attempt to keep the fine details. One related area that needs calling out is studies using items like luteolin (flavonoid). If you click on these, you will go to a summary page with a link to foods containing it
We have a list of foods and amounts that contain it. It’s an extra step, but since these foods were not cited in the study, we “keep religion” and only cite what was used.
I am not licensed medically, and thus there is no clinical experience (or bias) for the suggestions. It is an uber-logical model.
With that said, this person needs to sit down with his significant other, look thru the lists and decide which options they wish to try. Being a trained pharmacist means that he can also evaluate the prescription options for risk and in some cases, try to game the system… for example: Atorvastatin … he may want to test for the conditions where it would be prescribed, if he is a little high — he may wish to use that as a “standard of care” rationale for getting a prescription — it’s an off label use (like Viagra was not intended for what it is prescribed for today).
As always, any planned action should be reviewed by their knowledgeable medical professional before starting.
Before COVID, you had a unique microbiome, COVID “infection formed” it to suit its needs. These changes caused symptoms, made it easier for secondary infection and allow “alternative community of bacteria” to become established. How it changed depends on what it was like before and which variant of the virus. While the above suggestions are likely similar to what your suggestions could be, it is really important to get your own microbiome sample to work from. There will be large differences between people. With this approach, we can be single person specific for a treatment plan.
P.S. This sample was done via Biomesight, a UK based firm
A few weeks ago, I stumbled on some algorithms that had good results for predicting symptoms from bacteria. The next logical step was using the associations to get suggestions. While working on a blog post, I was getting odd results and digging into why, I discovered both logic and computational errors. Two readers had also raised questions about apparent bizarre logic. They were right — my logic was too simplistic and needed revision as well as better exposure of the logic being used.
The corrected version is up now. The main differences are:
Auto checking check boxes will happen less
Possible additions (unchecked) are marked with a ?
For Premium users, you get to see more of the gears that are turning.
To explain the issue, let us look at some details shown when in professional mode.
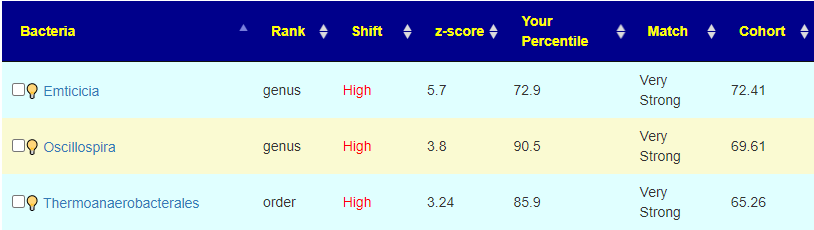
The old logic made suggestions to move away from the Cohort number. So for Emticicia, because we were higher than the Cohort value, we would try to raise it. This revision tries to lower it towards the 50%ile instead. The conceptual logic of moving away from the cohort was correct ignoring the sample percentile was incorrect. This implementation revision should correct this. For the other two bacteria above, we see that the cohort was high and the shift was even higher — again, moving away from the cohort is the desired, but moving higher than 90%ile is likely a poor choice, in this case you want to really move it down a lot.
The other factor is taking into account the z-score, etc. Some pages may have no automatic check. If you just click thru, you may get this message:
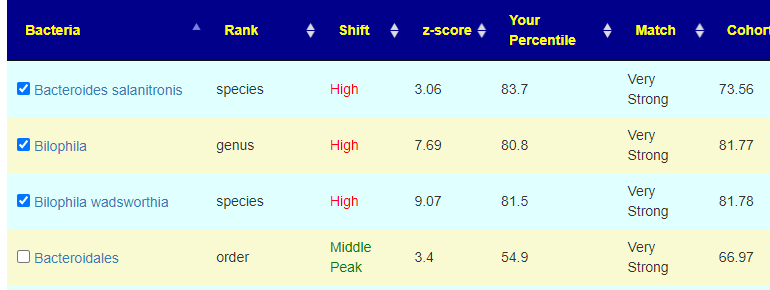
Let us look at some of the automatic checked
Both the person’s percentile and the Cohort are high, one was below the cohort and one was above. Because they are both high, the logic is to move them down to the middle (ignoring which side of the cohort it was on). The last one was not checked despite being Very Strong because the sample percentile was so close to the 50%ile (middle value)
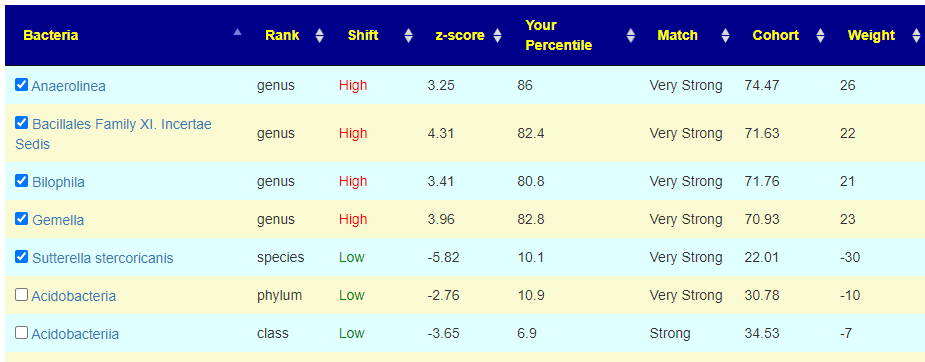
A third set of examples is below, which include the weight being visible (likely will be moved to a professional feature — mainly because it can be more complicated to interpret well)
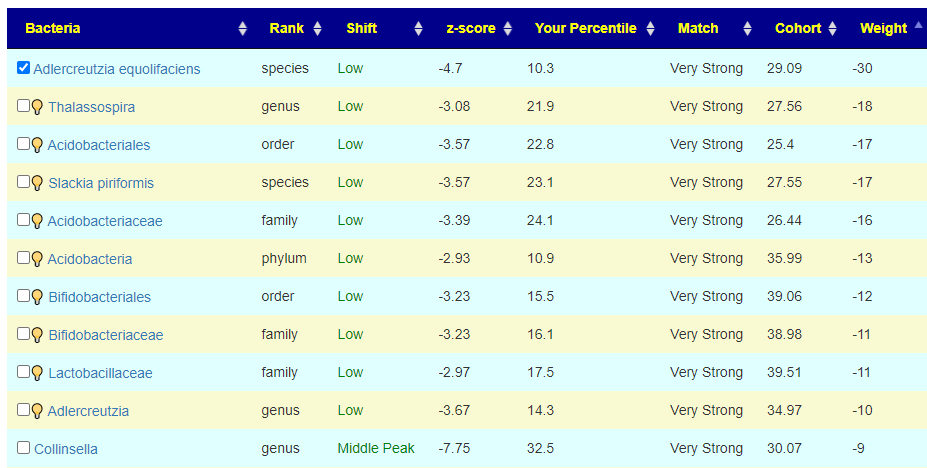
To get an automatic check the weight needs to be at least 20, for the ? , at least 10. For Acidobacteria, it is low but it is also a considerable distance from the cohort average. If selected, we declare a negative value and thus attempt to increase it (potentially moving it much closer to the cohort typical value — i.e. increase symptom). On the flip side, at only the 10%ile, you do not really want to decrease it more. A dilemma – excluding it is actually the best path. It has significance for the symptom forecast but has no clear action for altering the associated bacteria.
For this last one, we see Collinsella is a middle peak, and the desired direction is to increase it (negative value). Remember that these weights are used in computing the weights for suggestions.
Bottom lIne
The site is always in a state of change — from new studies being added, new samples being uploaded (and many statistics recalculated daily) and tuning and adjust algorithms — in this case readers questions lead to looking at the working data and seeing potential issues to correct (as well as displaying those numbers so people may ask questions — leading to still better algorithms).
A reader reached out for an educational review of their 16s microbiome results. I usually try to make time to do an education review once a fortnight unless I am deep in coding or analysis issues. He provided a nice very detailed back story, which is verbatim below
My problem started out approaching eight years ago when I went on a ketogenic diet. I had a massive energy collapse and weight loss (I was not overweight at the start), and I incorrectly believed this was about insufficient calories rather than macronutrients.
It turns out I have some uncommon genetics that make my ability to process fats for energy inefficient, under conditions of severe catabolic stress. Severe catabolic stress would be conditions like starvation, high fever, etc. Keto diet mimics starvation and is an extremely catabolic stress to the body. It looks like this diet was a suicide diet for me, and it started a set of symptoms that are persistent even after reverting to a higher carb diet.
The original symptoms were like CFS, but I have since been able to correct most of those by going to a higher carb diet, mostly using lower-glycemic whole food carbs like lentils, fruit, and vegetables. This took about three years to figure out and I think some infections may have exploited the period of low energy. Those infections may include dysbiosis as well as possibly some kind of brain infection.
During the first month of the diet I had some “event” where I tried to correct the energy collapse with a higher level of exercise, and after one high-intensity running session I spent the entire night drinking a liter of water every hour. I was desperately thirsty and was unable to quench the thirst.
The high levels of water probably induced an electrolyte imbalance, further aggravating the underlying cause. I should have made a trip to the emergency room, but I did not. After that one night I started with a tinnitus that has been with me 24×7 for approaching eight years. At first that tinnitus was like something at the brain core activating and literally consuming consciousness. That has improved over time and in the last year feels like it could become just a sound at some point soon. Together with the tinnitus I have some irritation of my optical nerve that gets worse when the tinnitus gets worse. These problems are severe and constant, and I cannot survive the stress of employment with such severe stressors on my brain.
It is worth mentioning that I was an entrepreneur for more than 10 years, working 14+ hour days. So I am the opposite of lazy. I had lifelong IBS-D, which is now well controlled, and most of that IBS I attribute to gluten and to dairy. I am gluten free, and now I get my only dairy exposure from carefully prepared yogurt.
I have neurological symptoms of brain fog (along with tinnutus) tied to food. About 60 to 90 minutes after eating the symptoms begin. I have multiple SIBO tests, that show an ongoing set of issues. My first SIBO test had enormous levels of background methane. My practitioner treated this as a colonic issue and we corrected that completely. My next SIBO test showed completely flat-line hydrogen and methane, a hydrogen sulfide (H2S) SIBO. I went on a heavy yogurt diet and that improved my symptoms. I stopped the yogurt, but when I repeated a SIBO test using the Trio test, it showed totally normally hydrogen, methane, and H2S. So I cured the SIBO. I have organic acid markers suggesting SIFO, and since I still have neurological issues after eating, we will start to treat for SIFO soon.
In terms of microbiome testing, the main trend I perceive here is: ? I started with 18% butyrate producers. I corrected this by a heavy diet of prebiotics including GOS, PHGG, and Acacia. Butyrate producers are now close to 40%. ? I have near extinction levels of Bifidobacterium and Lactobacillus. This I attribute to both antibiotics as well as not eating dairy foods for 20 years. I simply starved these genera out of existence. I do not tolerate Lactobacillus supplements or foods. They induce huge levels of brain fog. I am currently making a Bifido only yogurt that I load with prebiotics, and this has been extremely helpful to my health. The dairy is being completely tolerated, which I suspect is because I have thriving Bifido populations eating the lactose all the way through digestion. ? I have low and inconsistent levels of Faecalibacterium prausnitzii which is a key species I have identified that is almost universally associated with good health. I am addressing this by taking stewed apples as my main breakfast meal each morning. Pectin feeds this bacteria. ? I have low levels of Akkermansia, suggesting possible problems with my mucosal layer. I test with very low secretory IgA and somewhat leaky gut, so these might confirm a mucosal layer issue. I am trying to correct this with Bacillus coagulans, which gave me some success in earlier trials. ? I have slight elevations of methanogens and H2S producers. Biomesight and Thryve disagree about which species are present. I feel my best strategy for keeping these controlled is to focus on enhancing butyrate producers and trying to re-establish my acetate producers. ? My Proteobacteria are usually under 4% but I seem to have a large population of Sutterella wadsworthensis, always over 1%. This bacteria is worth calling out because we are measuring levels in the colon with 16s testing, and the research says this bacteria gets more dense as you travel up the small intestine. So I may have a fair amount of it in my duodenum. Since it is a gram negative bacteria, there might be some LPS issues. I plan to treat this with the yogurt.
As far as brain infection, this is unfortunately something for which good tests do not exist. I do show significant volume loss in my brain, confirmed by a radiologist on the MRI as well as by software that analyzes brain volume from those images. The severity of my neurological symptoms does seem consistent with some viral load that may have been pre-existing, and that simply exploited a number of years of low energy. There is a really interesting study out of Japan in the last few years where they treated people who had certain viruses with anti-virals and followed them for years after that. Treating with anti-virals effectively eradicated all risk of Alzheimer’s in later years, strongly suggesting a cause and effect between resident viral infection and neurodegeneration. This establishes some credibility for the hypothesis. At some point I may try to find a specialist and do some test around anti-virals to see if that affects symptoms.
My first impressions
One item stood out greatly in his story, the parallelism to what is seen with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Let me document out some of the parallelisms, I will cite just one publication for each:
Volume loss in brain: “The outcomes from the articles include changes in gray and white matter volumes, cerebral blood flow, brain structure, sleep, EEG activity, functional connectivity and cognitive function.” A systematic review of neurological impairments in myalgic encephalomyelitis/ chronicfatiguesyndrome using neuroimaging techniques.Maksoud R, du Preez S, Eaton-Fitch N, Thapaliya K, Barnden L, Cabanas H, Staines D, Marshall-Gradisnik S.PLoS One. 2020 Apr 30;15(4):e0232475. doi: 10.1371/journal.pone.0232475. eCollection 2020.
Tinnitus (hyperacusis): “Posttraumatic stress disorder, chronic fatigue syndrome, generalized anxiety disorder, depression, exhaustion, fibromyalgia, irritable bowel syndrome, migraine, hearing impairment, tinnitus, and back/joint/muscle disorders were comorbid with hyperacusis. ” Characteristics of hyperacusis in the general population.Paulin J, Andersson L, Nordin S.Noise Health. 2016 Jul-Aug;18(83):178-84. doi: 10.4103/1463-1741.189244.
He eliminated sufficient ME/CFS symptoms to likely not qualify for that diagnosis.
Ketogenic diet Literature
As usual, I go for gold-standard information from the US National Library of Medicine instead of internet rumor and snake-oil cure-alls. There are over 3800 studies. There medical cases when it is used with success (i.e. Epilepsy, Parkinson, Alzheimer’s diseases), but many of the studies have been with mice or with an apparent bias for positive results. Despite this, there was a good number of studies indicating general risks and complications. I have just cited a few studies from 2020 onwards, studies not available when this person made a regretted choice.
“In all, 21 % of patients under modified Atkins diet had unfavorable effects, while 52.63 % of patients on classic ketogenic diet had complications” [2021]
Clearly there are frequent downsides (beyond having DNA issues) that are not declared by advocates.
Testing Predictions
In my recent blog post, Predicted Symptoms – Performance Review, we found at least 50% of symptoms were correctly predicted using either KEGG Products or the Bacteria. This is a fresh test case sample. I forwarded the top 20 symptoms from these two predictors to the reader and he reported back. Results are below with the prediction engine reaching 60%.
Symptom
Z-Score
Reader Comment
Comorbid-Mouth: Periradicular periodontitis inflammatory / chronic lesion around roots of teeth
3.71
I have now-well-controlled significant erosion of the gums. It is not reversing but is hopefully not getting rapidly worse.
Comorbid: Small intestinal bacterial overgrowth (SIBO)
3.35
I apparently treated it and it no longer exists.
Post-exertional malaise: Worsening of symptoms after mild mental activity
3.32
Reading and focusing on written work quickly brings on fatigue and eye focus problems.
Age: 40-50
3.21
50+
Autonomic Manifestations: Cortisol disorders or irregularity
2.94
Fasting brings on high cortisol and high fasting glucose.
DePaul University Fatigue Questionnaire : Tense muscles
2.92
Tense in general, not just muscles
30% hit rate
Symptom
Z-Score
Reader Comment
Physical: Work-Sitting
1.86
☑️
Physical: Northern European
1.82
☑️
DePaul University Fatigue Questionnaire : Need to nap during each day
1.77
☑️
Neuroendocrine Manifestations: Poor gut motility
1.65
3.5 hour transit time through small intestine
Infection: Varicella Zoster Virus
1.62
I had chicken pox as a child. Both parents had shingles.
Comorbid: Sugars cause sleep or cognitive issues
1.53
☑️
Physical: Long term (chronic) stress
1.49
☑️
DePaul University Fatigue Questionnaire : Ringing in the Ear
1.44
24×7 tinnitus that varies from bad to horrific
DePaul University Fatigue Questionnaire : Abnormal sensitivity to light
1.41
☑️
Neuroendocrine: Cold limbs (e.g. arms, legs hands)
1.4
Particularly in the feet, I have poor circulation
Post-exertional malaise: Worsening of symptoms after mild mental activity
1.3
Reading and focusing on written work quickly brings on fatigue and eye focus problems.
Immune Manifestations: Chronic Flatus / Flatulence / gas
1.27
☑️
60% hit rate
Some of the agreements were interesting, especially for Varicella Zoster Virus. The person does not have active, but we know because of Shingles that the virus persists. If the virus persists, then it will do some ‘taxonomy-forming’ of the gut to be friendly to it. I hope this person has gotten a Shingles Vaccinations.
My Approach
I will start by using some citizen science patterns from Microbiome Prescription. Specifically
Obsessive-compulsive disorder – while not diagnosed with it, it was a prediction that he agreed with
I will do a consensus report from the collection of suggestions for the 5 items cited above. I picked the largest cohort to get the best precision.
Second, I will clear the consensus report and do a naive consensus report with just the Kaltoft-Moltrup outliers and Dr. Jason Hawrelak. As with most of these educational reviews, I will often explore different paths for analysis.
Third, I will clear the consensus report and do all 15 prediction matches. I will leave it to the reader to do an uber consensus approach of everything together, including these items connected to vision:
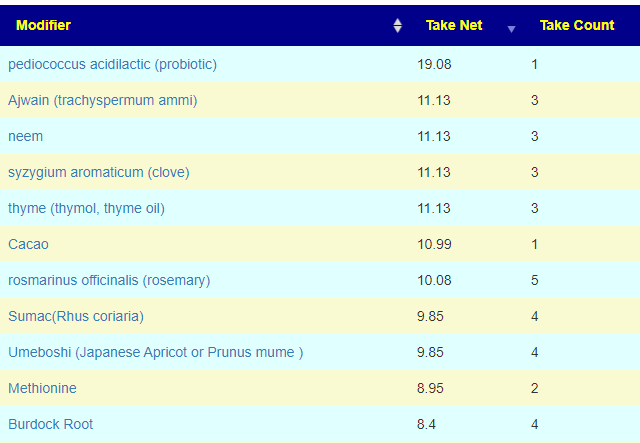
To confirm Kaltoft-Moltrup Ranges, I did a visual scan of his results, and there were no other extreme items. The default result was only 9 items on all lists, and they were only for Safest takes as shown below
Dropping the cut off point to 2 (from the default 3) increased the count to 18, with the items below added
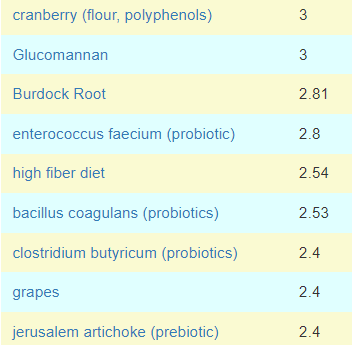
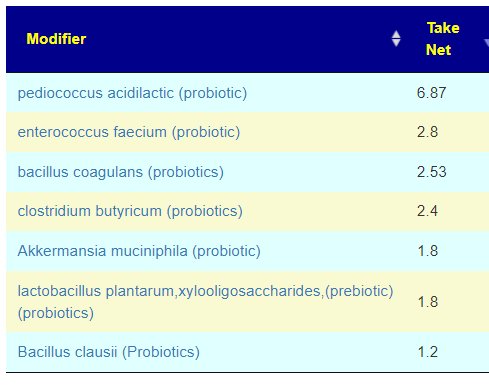
It is interesting to note that we have 3 probiotics listed, none of them are Lactobacillus — the specific type that the reader reported severe issues with. Dropping the filter point to 1 (from default 3) we end up with 47 items and filtering to probiotics, we have the list below. A Lactobacillus showed up but only in combination with a prebiotic. Decreasing further, we see the following added next: bifidobacterium infantis,(probiotics), bifidobacterium longum bb536 (probiotics), bifidobacterium catenulatum,(probiotics)
Third Pass
This may seem to be a lot of work, but you can see that it may be done quickly from the YouTube video for this post. Note that we are doing only Bacteria (KEGG Products are too indirect to get suggestions). Remember that we did 12 sets of suggestions so the “Take Count” should be a matter of interest.
This is a revision based on the revised algorithms Suggestions from Symptoms are Changed. I only did the auto checked items. The second level suggestions were not checked.
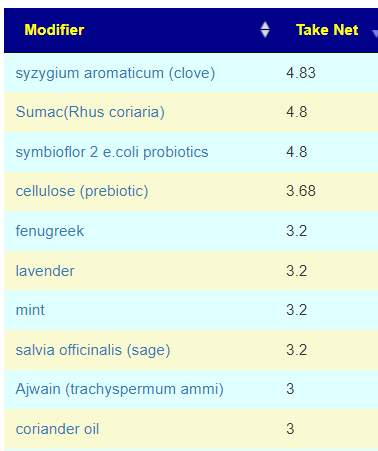
This obtains suggestions using genes and is independent of the the above processes, all of suggestions had a very low weight of 2 (often we see numbers of 200-300), so these are likely weak suggestions, with the three best candidates below (any one of them is likely sufficient)
I personally would advocate symbioflor 2 e.coli probiotics, (or Mutaflor) – because E.Coli probiotics appeared to make a major impact on reducing the time to recover for my own relapses/
I noticed what seems to be more than normal of polyphenols, herbs and spices. This is apparent on the third pass safest list and also second pass safest list but not on the first pass. I am inclined to ignore the first pass list for several: small number of bacteria in scope, symptoms and medical conditions were ignored.
Below you will find a YouTube of the analysis with additional commentary.
Reader feedback
“Your studies under Keto literature raise the possibility that a high fat diet may have exploded my levels of B wadsworthia during the active keto diet phase, and this alone may have promoted most of my brain fog. That’s an interesting hypothesis I had not considered. “
“On the various suggestions lists, do I understand that AI is not able to give us reasons for the suggestion, but rather it is just making associations between suggestions and reversal of symptoms that have been studied? ” INCORRECT, for the professional user, I detailed out the evidence as shown below
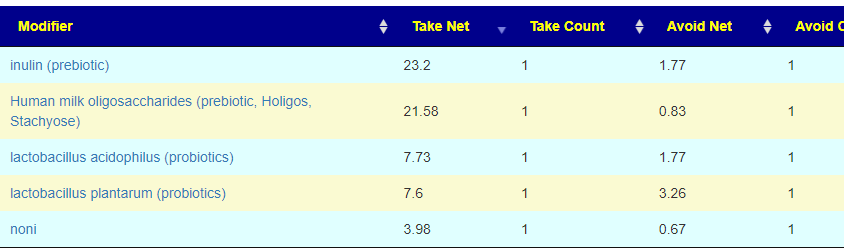
“It might help to define “Take Counts”. Maybe you do that on the video. What is also confusing is that on the Safer Takes list you have a “Take Net” and it is not clear how it is calculated.” The calculation something like this:
SUM( For each Bacteria (Magnitude of Shift desired + Function(Number of studies shifting in the right direction, Number of studies shifting in the wrong direction))
so substance with only a few (or just one) study for a bacteria will have a lower number
so substance with many studies for a bacteria will have a higher number
a bacteria that is slight off will have a lower number
a bacteria that is very off will have a higher number
The actual computational functions are proprietary and the results of 3 years of experiments.
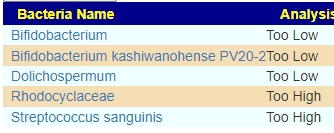
“it is confusing because the same genus Bacteroides is alternately Too Low and then Too High.” There are THREE reference point the highs, the lows and the middle peaks (used for symptoms). People with a specific symptom may average at 35% of the median, so the goal is to shift you away from the 35% area. This it becomes a question of which direction? I made an “arbitrary” decision that if you are > 35% then we want to push you higher. If you are < 35%, we want to push you lower (ideally keeping you within the Kaltoft-Moltrup range of normal values). There is logic behind this “arbitrary” decision, but explaining it is complex.



Recent Comments