As a result of some readers asking for a PDF that they could shared with their medical professional I have created two reports and deployed the first versions today. The readers requested these features:
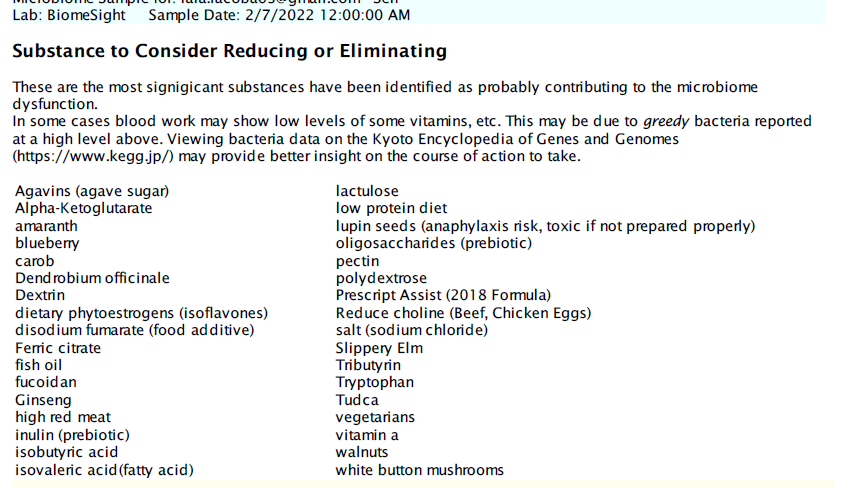
Simplify the suggestions into shorter list without extra data like Priority.
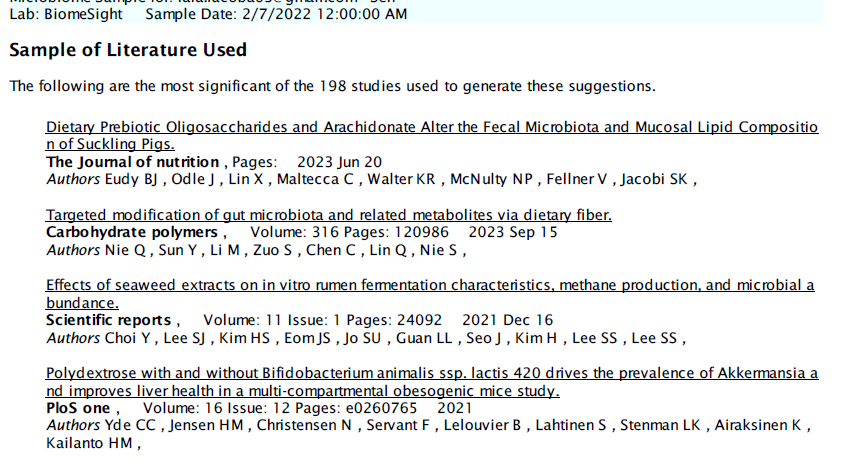
Provide some of the literature used to generate the suggestions
Provide the bacteria being targeted.
The reports are based on the consensus reports (so you can build them as you like).
For the automatic emailing of the PDF, we run “Just Give Me Suggestions” — which executes 4 different algorithms (Mean +/- 2 Standard Deviation, Box-Whiskers, Kaltoft-Moltrup and top/bottom 5%ile) and to obtain a consensus report. From the consensus report, we pick those that are at least 50% of the highest value to take, and below 50% of the lowest value to avoid. We then sort the items alphabetically for the lists.
The suggestions are from Microbiome Prescription and may disagree with suggestions from the lab used. To see how we get suggestions (tracing back to source studies), see this video. You will need to ask the lab how they do theirs — in some cases, it is opinion from a dietician.
Links are on various pages, for example, changing Microbiome tab.
First Page is an introduction to what the report is
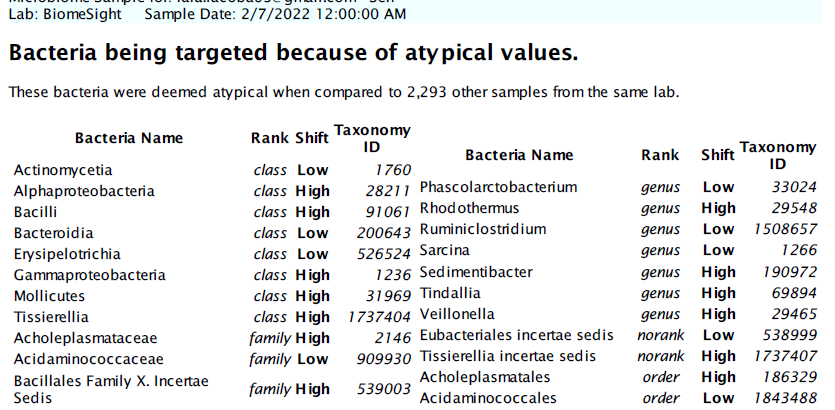
Second Page is the bacteria being targeted, group by taxonomy rank
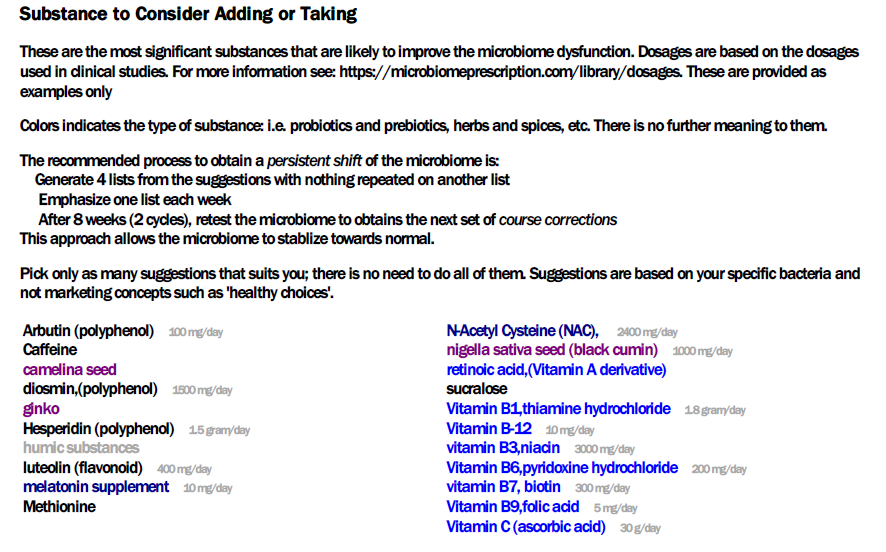
Third page are suggestions to take. Where dosages from clinical studies are available, they are shown
The next page are things to avoid
The last page are a partial listing of citations explicitly used. The newest studies are listed first to pre-emptively answer the question about how old the data being used is.
This is in Beta Testing Mode
Open for suggestions and improvements. Remember this is targeted for the typical medical professional with limited knowledge and understanding of the microbiome.
Based on several online meeting that I had, I thought a series of online meeting for people to ask questions, be shown features, etc would benefit many. All meetings were recorded and then posted on YouTube. After viewing these, you may wish to view this from Jan 2023 also.
The second in a series of online sessions. Shows how dosages are determined from EXISTING studies and shows how just one suggestion may be based on over 20 different studies (with working links to the studies). This is several magnitude better than ANY microbiome testing company suggestions
One link was broken in the demo. It is now fixed and a walk through is done below.
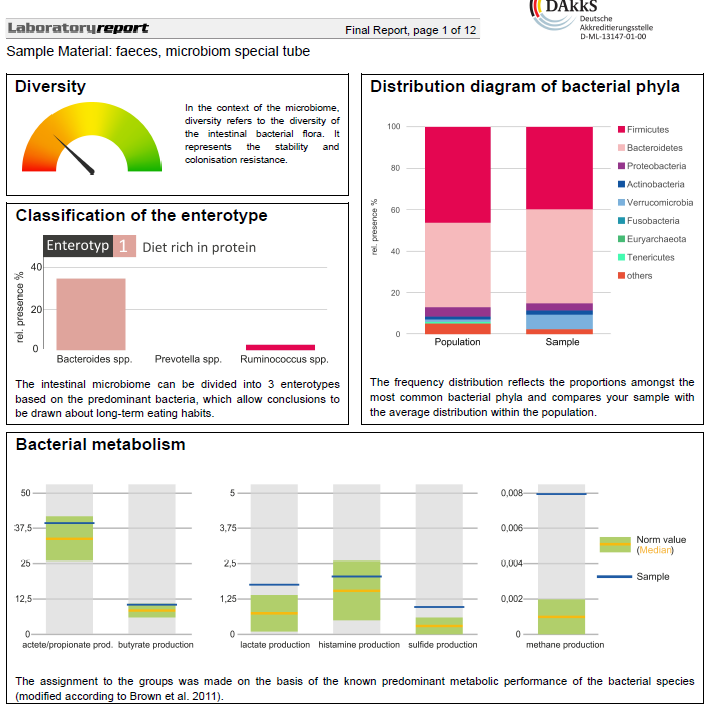
A reader message me and sent over two files. One was familiar and my advise has been to transcribe the data; the other was a new format and it was very possible to code an uploader for in less than a day.
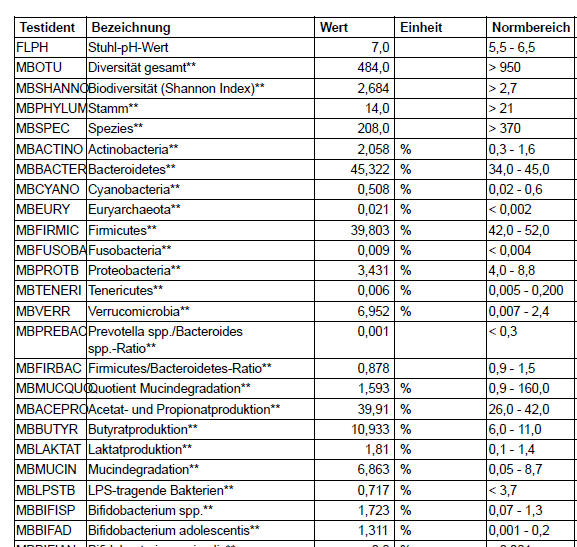
The small one, bacteria-count is what can be uploaded.
The analysis one has less taxonomy data than the bacteria count one and starts up with the type of page shown below. Dissecting it to get the data would likely be six full man-weeks of development. My attitude is for clients to hassle the provider to make a more friendly format (i.e. tab or comma delimited text files).
The Sweet Bacteria Count File
This file looks like below and is relatively easy to extract the data for (i.e. less than one developer day).
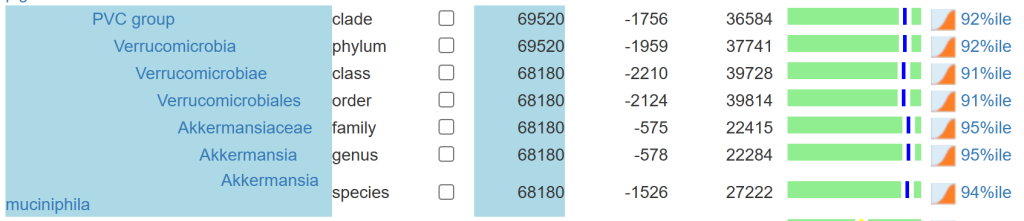
We have only a hundred bacteria at different levels reported. If you go to the microbiome tree, you will see a lot more! Why, we build all of the missing levels of the bacteria hierarchy from the missing data. The upload has no family, order or class information … so we make a best effort attempt to estimate them.
We also apply percentile based on all samples uploaded (until we get 200 samples for a specific test) … again best efforts. See The taxonomy nightmare before Christmas… for background.
For more information on this project see Health Rising post. Both participants has granted me to do a review with their real names. This is the second of a series of posts on this project, the first one was on The Remission Biome Project: Tess Falor.
The earliest use of antibiotics for treating ME/CFS that I am aware of, dates from the late 1990’s with articles in Journal of Chronic Fatigue Syndrome (and conference reports prior)
My remission from ME/CFS was done by combining C.L. Jadin protocol with Dave Berg anticoagulant protocol.
A big thanks to BiomeSight.com for donating some testing kits to the project. If interested in using their kits, there is a discount code (“micro”).
Overview of results
First, let us show the numbers and then talk about them. It is clear that there are significant changes. There are a lot of dimensions to consider. Some highlights:
The number of bacteria with abnormally high representation has gone from 123 down to 29
The number of bacteria with abnormally low representation has gone from 222, dropping down to as low as 19, before rebounding to 162 (still better than the start)
Most measure showed great improvement and then some relapse.
Criteria
7-Mar
23-Mar
15-Apr
22-Apr
29-Apr
Shannon Diversity Index
33.8
78.0
97.1
76.5
77.1
Simpson Diversity Index
0.7
65.1
58.6
60.3
73.4
Chao1 Index
91.3
61.6
72.0
89.4
14.8
Chi-Square (Lower is better)
55
47
46
50
30
Lab Read Quality
8.6
7.1
5.4
2.2
6.9
Bacteria Reported By Lab
755
638
628
765
461
Bacteria Over 99%ile
27
11
13
56
5
Bacteria Over 95%ile
72
25
30
105
18
Bacteria Over 90%ile
132
46
63
178
29
Bacteria Under 10%ile
222
218
62
19
162
Bacteria Under 5%ile
191
195
18
12
144
Bacteria Under 1%ile
177
179
0
3
112
Lab: BiomeSight
Rarely Seen 1%
8
4
3
66
2
Rarely Seen 5%
22
24
27
128
14
Pathogens
39
32
33
31
29
Outside Range from JasonH
8
8
8
8
8
Outside Range from Medivere
18
18
16
16
16
Outside Range from Metagenomics
9
9
6
6
6
Outside Range from MyBioma
10
10
6
6
6
Outside Range from Nirvana/CosmosId
18
18
12
12
12
Outside Range from XenoGene
52
52
39
39
39
Outside Lab Range (+/- 1.96SD)
43
15
17
36
7
Outside Box-Plot-Whiskers
146
51
83
227
43
Outside Kaltoft-Møldrup
251
189
105
212
158
Condition Est. Over 99%ile
1
5
0
0
3
Condition Est. Over 95%ile
2
14
0
5
13
Condition Est. Over 90%ile
11
28
2
11
21
Enzymes Over 99%ile
7
68
5
19
37
Enzymes Over 95%ile
22
281
209
123
250
Enzymes Over 90%ile
58
435
361
317
409
Enzymes Under 10%ile
219
354
59
48
201
Enzymes Under 5%ile
173
265
34
24
144
Enzymes Under 1%ile
138
94
13
12
79
Compounds Over 99%ile
3
44
1
13
16
Compounds Over 95%ile
15
186
82
68
87
Compounds Over 90%ile
27
297
154
153
183
Compounds Under 10%ile
882
889
985
987
875
Compounds Under 5%ile
862
859
959
963
841
Compounds Under 1%ile
845
802
935
952
820
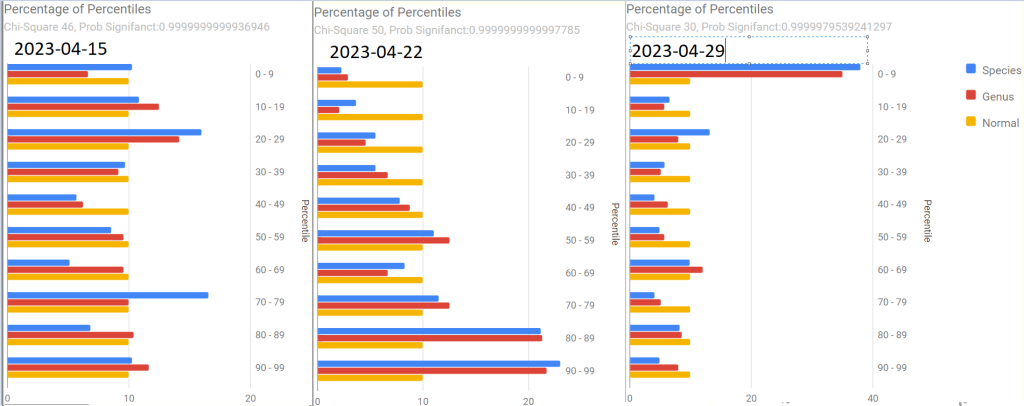
As with Tess, the percentages by percentile which I noticed tend to have over representation with ME/CFS and Long COVID in the 0-9 percentile. We see this pattern at the start, with improvement and then a bounce back to high numbers in the last sample
Tamara suggested that I convert the tables below to charts. Both are now available on the site.
Pretty Pictures
Tamara suggested that I convert the tables below to charts. Both are now available on the site.
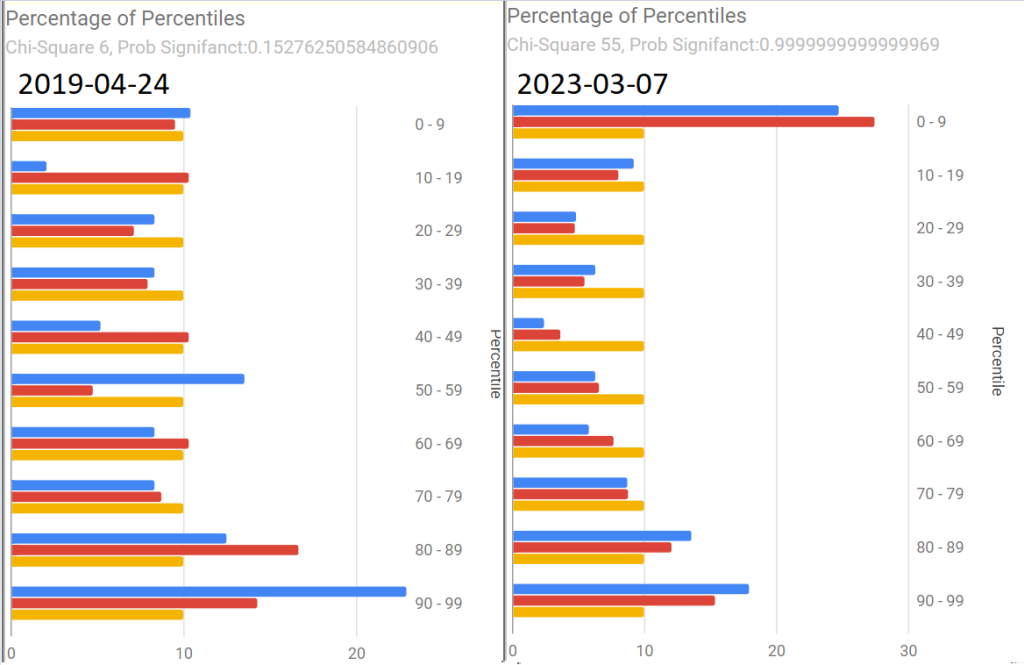
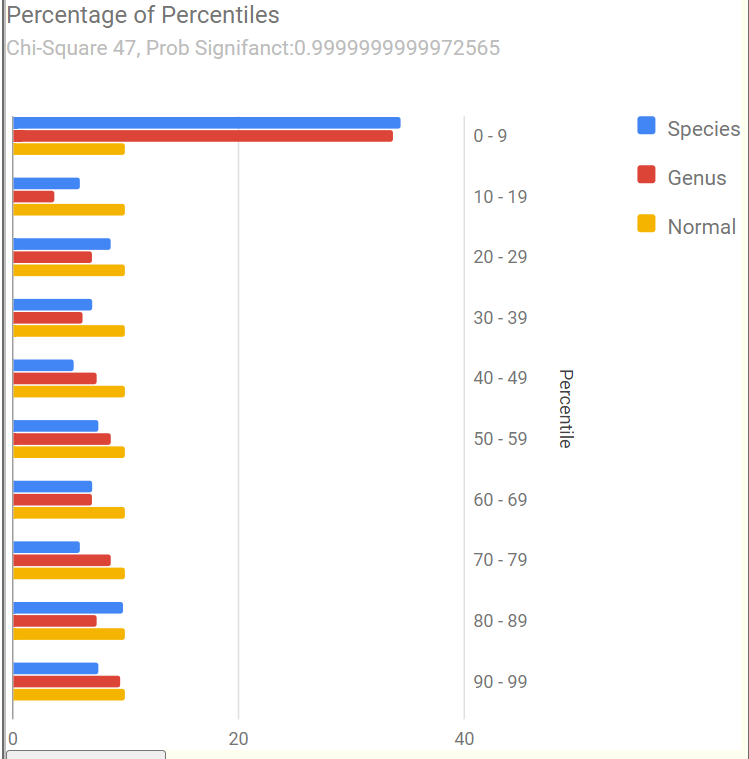
First, an old sample that she happened to have where we see Chi-Square at 6. The first of the recent samples had it jumping to 55, A normal microbiome is expected to have a Chi-square < 13. A higher value indicates a statistically significant, abnormal microbiome.
The next three show the changes with antibiotics. Chi-square went from 46 to 50 with a dramatic shift and then drifted down to 30.
The latest sample increased upward again, with the pronounced spikes that are common with ME/CFS being there.
The raw numbers are also shown. I will spare your eyes by omitting them.
The Events Around the above Samples
7 Mar – Before
23 Mar – Day 4 AmoxClav
15 Apr – More
22 Apr – Final Day of AmoxClav (30 days of AC)
This sample has a low Lab Read Quality, this may account for the number of spikes in its report.
29 April – After 3 days of Aprepitant + Erythromycin (this was a BIG difference from Tess and was the intervention that seemed to give me the baseline increase this time).
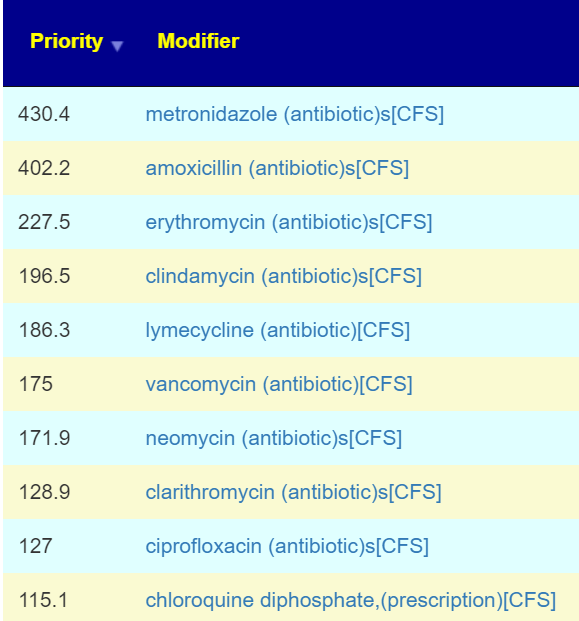
As with Tess, let us see how these items rank in each sample. As with Tess, imipenem is the most common best suggestion.
As a result of a conference call with some of the Remission Biome Project, and Dr. Jadin’s Current Protocol for ME/CFS. I annotated all of the antibiotics used in studies for ME/CFS, Lyme, and related conditions with [CFS]. This allows us to quickly see the “consensus” antibiotics (i.e. used in studies and suggested by microbiome prescription algorithms).
The top ones are shown before (Just enter “CFS” in the Search dialog)
Only two of these were negative for her (doxycycline and ampicillin) with docycline sibling, minocycline being just 21).
I would suggest using this list to pick 2 antibiotics to do a one week course and then take a 3 week break. After the course, then do some of these probiotics. I am inclined to omit L.Casei because the strain used in Yakult is a negative. Thus we end up with these three as top suggestions. P.S.
Note the weight of these are above many of the antibiotics above. I usually advocate single species. The Bifido is available from Custom Probiotics with their recommended dosages above the amount listed above.
Part Deux — More Samples!
Her description of subjective changes: generally keep improving in terms of PEM, function etc. (was definitely a dip around the 2nd ‘constipation’ sample)
1st, [2023-06-14] in the series just a temporal sample, no additional treatments
2nd, [2023-07-15] in the series I had a major episode of constipation – wanted to catch that
3rd, [2023-07-20]last one was was post my 2nd treatment of aprepitant+erythromycin
Sample Comparison
We include the prior one above for easy reference). The key change items are:
The new Anti inflammatory Bacteria Score has seen a dramatic increase from 17%ile to 73%ile. The four prior samples were 7.6%ile, 8.2%ile, 3.9%ile and 6.9%ile
Outside Kaltoft-Møldrup is dropping. In terms of %age of reported: 32% -> 28% -> 29% ->16%
The high and low Enzymes also seem to be dropping
The last sample had a Chi-Square of 9, that is a probability of 0.54 instead of the .9999999… for all other samples. Unfortunately, the poor read quality makes this fuzzy.
Note: The last sample has a low read quality (thus less bacteria types are being reported)
Criteria
22-May
14-Jun
15-Jul
22-Jul
Shannon Diversity Index
69.4
29.20
43.00
15.00
Simpson Diversity Index
54.7
7.60
27.50
60.00
Chao1 Index
72.4
0.87
21.40
8.30
Anti inflammatory Bacteria Score
17.0
30.90
43.60
73.20
Chi-Square Score
49
51
32
9
Lab Read Quality
7.2
10.9
6.6
2.3
Bacteria Reported By Lab
659
752
512
375
Bacteria Over 99%ile
10
12
1
4
Bacteria Over 95%ile
22
24
2
20
Bacteria Over 90%ile
45
41
13
39
Bacteria Under 10%ile
199
229
189
19
Bacteria Under 5%ile
186
208
184
3
Bacteria Under 1%ile
167
165
166
0
Lab: BiomeSight
Rarely Seen 1%
25
13
0
0
Rarely Seen 5%
49
37
7
1
Pathogens
32
34
36
21
Outside Range from JasonH
4
7
7
4
Outside Range from Medivere
14
19
19
14
Outside Range from Metagenomics
6
7
7
6
Outside Range from MyBioma
4
6
6
4
Outside Range from Nirvana/CosmosId
18
19
19
18
Outside Range from XenoGene
33
34
34
33
Outside Lab Range (+/- 1.96SD)
11
12
1
13
Outside Box-Plot-Whiskers
56
75
23
50
Outside Kaltoft-Møldrup
209
212
150
61
Condition Est. Over 99%ile
0
0
1
0
Condition Est. Over 95%ile
0
0
1
0
Condition Est. Over 90%ile
1
0
3
0
Enzymes Over 99%ile
62
1
5
2
Enzymes Over 95%ile
130
3
18
11
Enzymes Over 90%ile
215
12
99
33
Enzymes Under 10%ile
429
211
171
304
Enzymes Under 5%ile
310
146
142
211
Enzymes Under 1%ile
152
85
73
47
Compounds Over 99%ile
31
0
3
1
Compounds Over 95%ile
64
2
9
11
Compounds Over 90%ile
106
7
48
24
Compounds Under 10%ile
959
1096
1009
1015
Compounds Under 5%ile
909
1041
981
971
Compounds Under 1%ile
860
1009
956
922
Since we had a symptom of constipation, let us see how well the samples match that reported from Studies on PubMed — there were no matched. When we went to our Special Studies, we see that the microbiome followed the reported symptoms. We then look at the top value from Special Studies — which was Long COVID for all samples. We see the lost of ground around the constipation and then regaining the progress.
Criteria
22-May
14-Jun
15-Jul
22-Jul
Special Studies
7%ile
14%ile
15%ile
7%ile
Top Item Long COVID
35 %
44 %
41 %
36 %
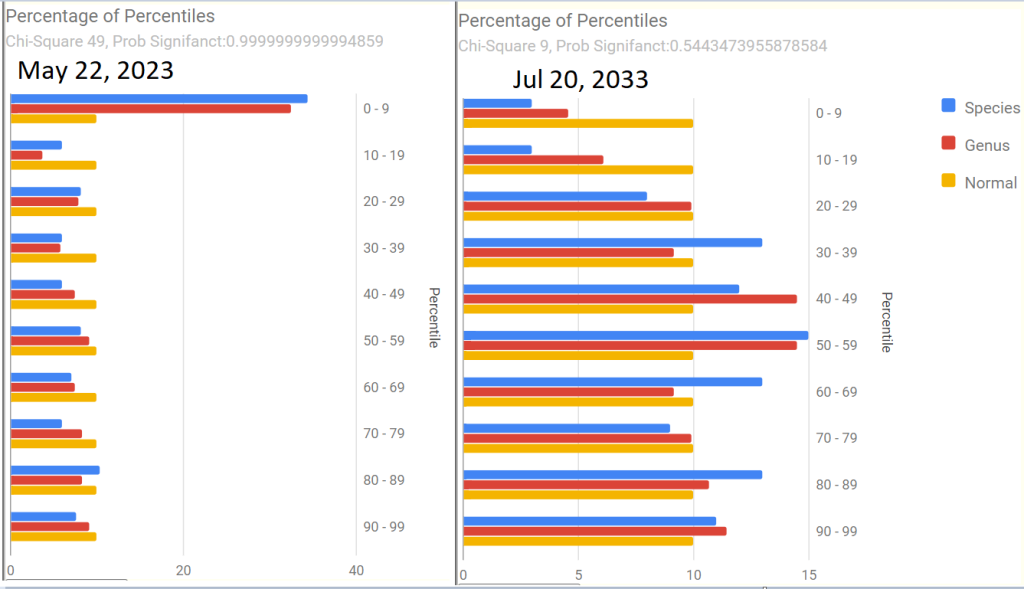
Next we go and look at aprepitant and erythromycin
The Percentage of Percentile show quite a shift — unfortunately, it is unclear if this is a temporary after effect of constipation, poor lab read quality, or the above aprepitant and erythromycin. The next sample may resolve this issue.
Is the Project working — YES
We are seeing both subjective improvement and object improvements.
Personally, I like what appears to be a shift towards Cecile Jadin’s approach — not continuous antibiotics but a course (7-10 days) followed by a break (ideally 3 weeks). Often I find that ME/CFS people tend to be impatient and just want to keep pressing on hard… which I have observed often result in tripping and rolling down the hill to where they were (or worst).
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide information on rotations etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
During the questions period of Jadin’s presentation: Dr. Jadin’s Current Protocol for ME/CFS; Questions were asked about her treatment in terms of it’s target and what microbiome prescription does. I thought a blog post may help people understand how microbiome prescription side-steps a Pandora box of theories.
A simple Premise: Fix the microbiome and symptoms will improve!
In Dr. Jadin’s presentation, she identifies a host of causes that could result in ME/CFS and similar conditions. For example Giardia — IBS/CFS/Long Covid Insight from Bergen’s Giardia Infection, Lyme, or my post from 2016, Post Infection Fatigue, virus: HHV6, EBV and of recent note: COVID. The question arises: Is the source still there? The pragmatic answer is likely yes, at low but significant levels (i.e. maintenance levels).
Not only is it there, but there is likely a half dozen low level infections associated with ME/CFS. WHY? When the microbiome goes off, the immune system follows it. Virus reactivation happens because the immune system is not firing on all cylinders. For example, your body may keep fungus well controlled in your living environment before; now you have fungi problems added to the mix.
Chasing Symptoms Trap
Often people will be focused on one symptom or lab result. For example: How do I reduce my methane levels, How do I reduce my Interleukin 6 levels, how do I get rid of brain fog, etc etc etc.
I do not have the answers for those questions, nor do I care. I review the body as a very complex dynamic organism with a great amount of interactions. My sole target is the microbiome and that is a big target — over 18000 different bacteria are reported from retail microbiome tests, 8,000+ different enzymes, 18,000 different compounds.
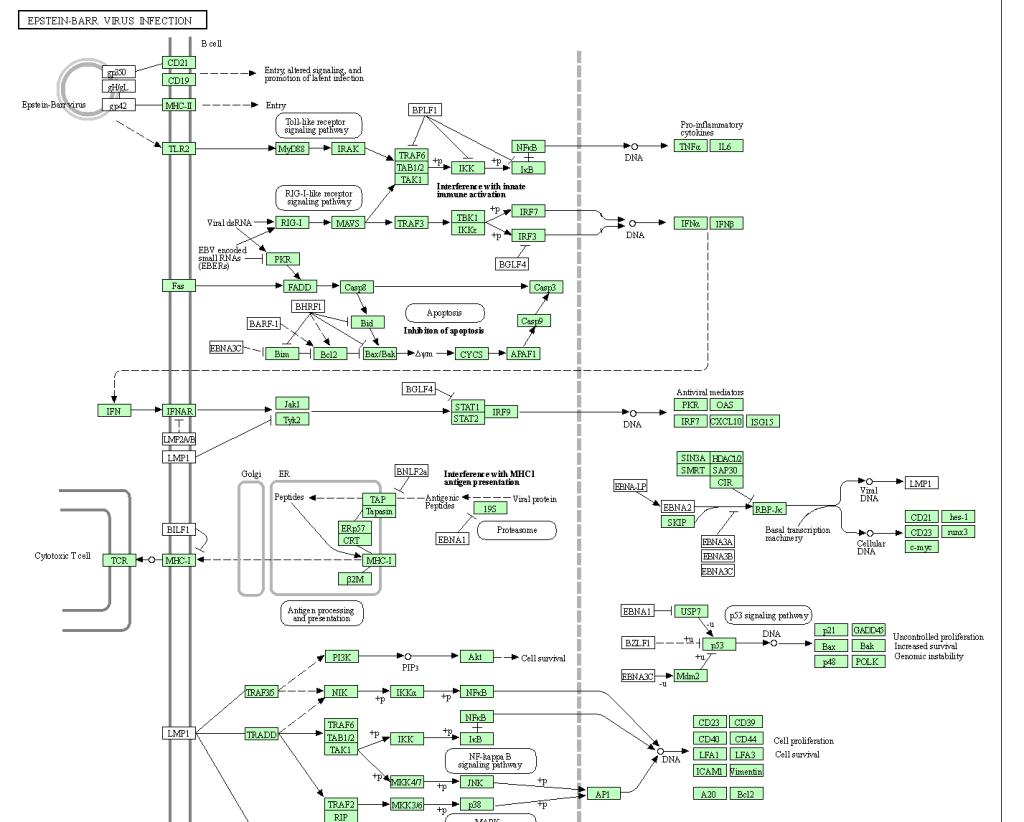
Let us take just one ME/CFS associated item: Epstein-Barr virus. Some of the interactions and interplays are shown in the chart below (See KEGG for full chart). So, you are wanting a single magic supplement?
My goal is very simple, normalize the microbiome and thus normalize the immune system and the levels of the 26,000+ substances involved. Then, and only then, will issues of substance appear (if any).
No matter what the infection (virus, fungi, bacteria) – they need “food”
Where does the food come from? The microbiome. Correcting the microbiome should starve the bad guys and feed the good guys is the simple concept. All of these infections are known to alter the microbiome — and we can reasonably assume that it is done to make the human body more friendly to the infection.
Now with 18,000 bacteria and 26,000 substances, no person can either read nor keep all of the available data in their brain. I happen to have the skill sets to encode much of the data and build a fuzzy logic expert system around the data – that’s my skill set.
Why does my recommendations often matches Jadin’s protocol?
If we assume the infection is still there, we likely have a strong association between the infection and the microbiome bacteria. What encourages the infection, likely also encourages a subset of microbiome bacteria; and the reverse. The microbiome may just be a proxy for the infection with the odd-characteristic that we may be able to determine effective antibiotics without needing to identify all of the infections present. The infection and the microbiome in one sense are mirrors of each other.
This is the philosophical basis that I am working from. As with best modelling practices, if a model predicts and the predictions are correct, you keep to the model (even if it is full of orcs and hobbits) until it breaks — then you work on building a better model.
The microbiome may be a sufficient proxy for the co-infections involved with ME/CFS.
It is easier, faster and cheaper to test – especially because it is available at a low cost, direct to consumers.

Recent Comments