This is a repost with expansion of “What is the best diet in your opinion?” on my CFS Remission blog back in 2018. It consists of the following
- Basic Logic for this diet
- How diets have changed in recent years — today’s “normal diet” is radically different than your recent ancestors
- The manifestation of “keeping up with the Jones” eating habits
- Finding Your Historic Diet – my own exploration
I have been asked this often. My answer is extremely logical but not what you will get from most health experts (and unfortunately, may not be easy to determine for some, see “mutts” below). It is based on actual science and not idealogy.
The Diet…. it’s Logic
Very simple — the type of diet that your ancestors ate 300+ years ago! Diet changes gene expression, i.e. microbiome AND DNA adapts.
Last year, researchers discovered that these kinds of environmental genetic changes can be passed down for a whopping 14 generations in an animal – the largest span ever observed in a creature, in this case being a dynasty of C. elegans nematodes (roundworms)…. Usually, environmental changes to genetic expression only last a few generations.
… studies have shown that both the children and grandchildren of women who survived the Dutch famine of 1944-45 were found to have increased glucose intolerance in adulthood.Scientists Have Observed Epigenetic Memories Being Passed Down For 14 Generations
What is 14 human generations? 300 to 420 years.
Maternal undernutrition during pregnancy (F(0)) programs reduced birth weight, IGT, and obesity in both first- and second-generation offspring. Sex-specific transmission of phenotypes implicates complex mechanisms including alterations in the maternal metabolic environment (transmaternal inheritance of obesity), gene expression mediated by developmental and epigenetic pathways (transpaternal inheritance of LBW), or both (IGT)
Intergenerational transmission of glucose intolerance and obesity by in utero undernutrition in mice [2009]
” Thus, it is possible to construct a chain of events, based on experimentally verified biochemical mechanisms, through which an environmentally induced change in the activity of chromatin-modifying enzymes can lead to a change in DNA sequence.”
Epigenetic responses to environmental change and their evolutionary implications [2009]
A diet based on typical diet of your ancestors 400 – 1400 years ago is likely a better choice than any healthy diet pitched by most people. Your gut bacteria is likely closer to the optimized bacteria your ancestors evolved from eating the same food for a thousand years.
Risk of introducing atypical foods
A new atypical food will have some bacteria/body tolerate it. For others, it may throw the body’s balance off; leading to autoimmune disease, diabetes, gluten sensitivity, autism, ADSD and a host of other conditions that appear to be increasing in western population ‘for no apparent cause’ (… cough, cough, cough). It’s a gamble for you and for your children. Yes, people will adapt and survive — but your offspring may not.
You should avoid the newly introduced foods (for your regions) that were not in use a couple of hundred years ago, for example, potatoes, peanuts (1920’s), and banana (which has been reduced to a single species, Cavendish – because it was the most profitable). The charts below show some of the abnormalities of diet seen recently. You also avoid process foods and modern additives (especially emulsifiers and new preservatives).
Some Drastic Changes seen in Diet
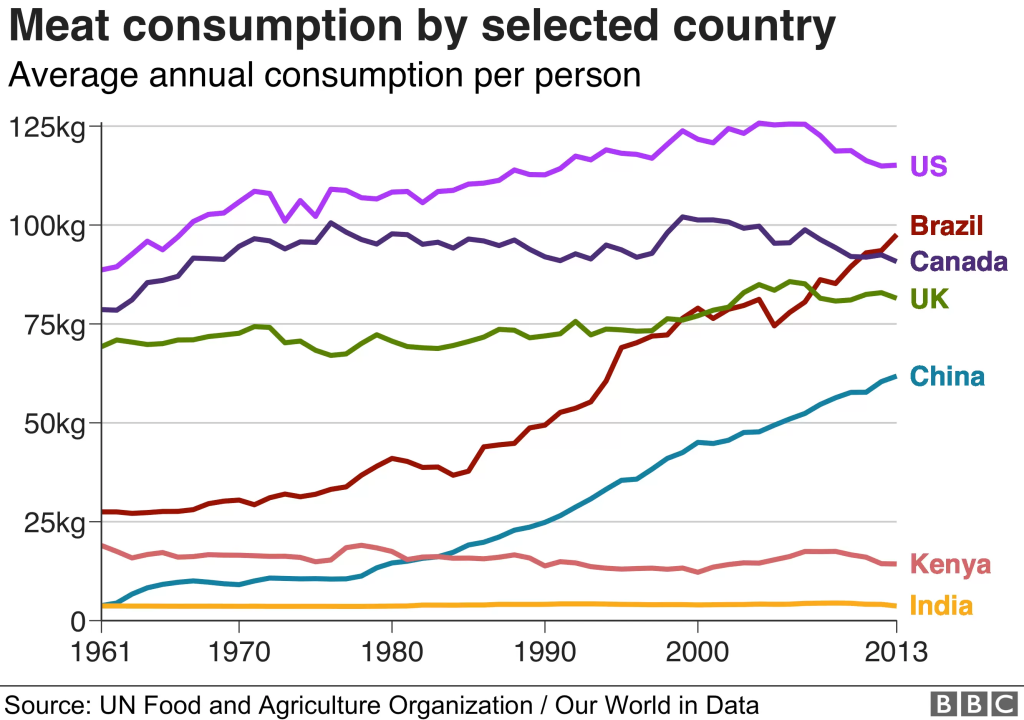
We can see that Americans have DOUBLED their meat consumption with almost a 10 fold increase of “healthy” chicken.
- ” In conclusion, consumption of lean red meat (lamb) or lean white meat (chicken) as part of the usual diet is associated with a similar lipid response.” [2011]
- “Consumption of lean red meat (Pirenaica breed) or lean white meat (chicken) as part of the usual diet is associated with a similar response. ” [2022]
- “There was no difference in BMI or any other marker of adiposity between consumption of pork, beef and chicken diets. ” [2014]
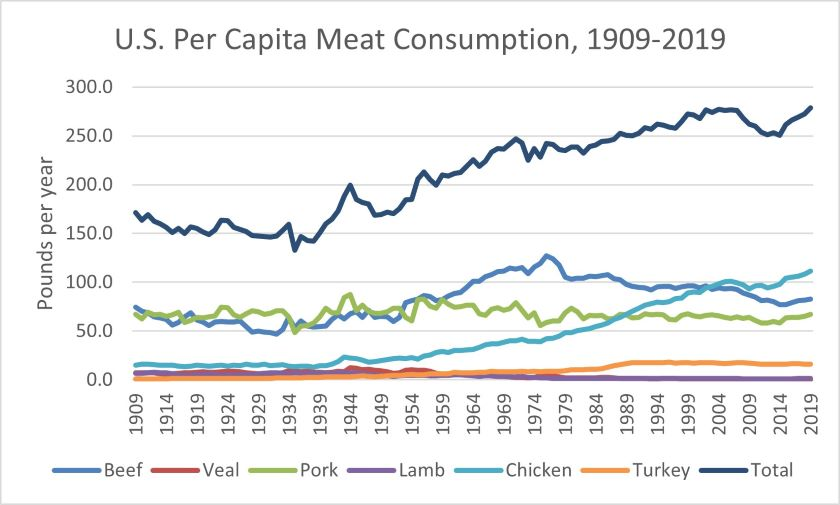
Drivers of U.S. Per Capita Meat Consumption over the Last Century
There are implication that this increase of meat may be a factor in increasing ADHD, Autism rates and autoimmune conditions:
- Maternal Western-style diet reduces social engagement and increases idiosyncratic behavior in Japanese macaque offspring [2022]
- The Influence of Maternal Metabolic State and Nutrition on Offspring Neurobehavioral Development: A Focus on Preclinical Models [2022]
- “Maternal obesity, metabolic conditions, and high fat diet consumption increase maternal leptin, insulin, glucose, triglycerides, and inflammatory cytokines. This leads to increased risk of placental dysfunction, and altered fetal neuroendocrine development. Changes in brain development that likely contribute to the increased risk of behavioral and mental health disorders include increased inflammation in the brain, as well as alterations in the serotonergic system, dopaminergic system and hypothalamic-pituitary-adrenal (HPA) axis.” [2015]
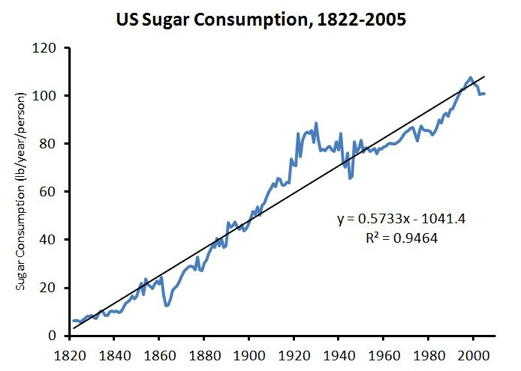
Sugar is added to almost all prepared foods. The reason is simple, it encourages consumption and thus more sales.
And we are eliminating other very tradition foods from our diet, for example legumes and dry beans.
legume consumption remained low in US adults and declined from 2011 to 2014 (mature legumes: 12.8 to 8.3%; dry beans: 10.0 to 6.5%).
Legume Consumption Patterns in US Adults: National Health and Nutrition Examination Survey (NHANES) 2011–2014 and Beans, Lentils, Peas (BLP) 2017 Survey [2020]
Keeping up with the Jones [Health Issues]!
My daughter has seen this in Vancouver, Canada – where almost 50% of the people were born outside of Canada.
Having grown up around such a large amount of immigration, the changes have been really apparent. Interestingly enough, those from India and area tend to keep the traditions at home for eating, so they don’t have such a big impact on their bodies. But those from Asia, they all essentially know that when they come to North America, they are going to gain a lot of weight. Whether it’s food culture or additives in food, it’s a big struggle. They tend to also have problems with both dairy and alcohol.
Daughter
Keeping up with the Jones often include eating upscale for your own culture group or the population that you are residing in. A food that was once a special occasion food becomes a regular food as a statement of prosperity (and possibly stupidity!)
- Following the Indian Immigrant: adoption of westernization results in a western gut microbiome and an increased risk of inflammatory bowel diseases [2022]
- A Pilot Study of the Gut Microbiota Associated With Depressive Symptoms and Sleep Disturbance Among Chinese and Korean Immigrants in the United States [2022]
- “results showed that altitude was the most important factor affecting the variation in the microbial community” Succession of the Gut Microbiome in the Tibetan Population of Minjiang River Basin [2022]
- “Among US Hispanics/Latinos, US exposure is associated with unfavorable gut microbiome profiles for obesity risk, potentially related to westernized diet during acculturation.” Microbial co-occurrence complicates associations of gut microbiome with US immigration, dietary intake and obesity[2021]
- The Impact of Migration on the Gut Metagenome of South Asian Canadians. [2021]
- The Impact of Childhood Growth Stunting and Post-Migration Dysbiosis on the Development of Metabolic Syndrome Among Indigenous Immigrant Mexican Women. [2020]
- Linking the westernised oropharyngeal microbiome to the immune response in Chinese immigrants. [2020]
- US nativity and dietary acculturation impact the gut microbiome in a diverse US population. [2020]
- Western oropharyngeal and gut microbial profiles are associated with allergic conditions in Chinese immigrant children.[2019]
Evidence of significant impact
- “Adherence to the ‘ethnic breads, legumes and nuts’ and ‘whole grains, fruit and dairy’ patterns was associated with a lower predicted cardiovascular diseases risk, and an inverse association for the ‘processed food and sugar-sweetened beverages’ pattern in an Asian population. ” [2022]
- “participants in the highest quintile of the refined-foods pattern had a greater risk of elevated 10-y cardiovascular diseases risk” [2016]
- “Patterns emphasizing higher consumption of vegetables, legumes, fruit, nuts, whole grains, fish, lean meat or poultry, … were generally associated with decreased risk of all-cause mortality. “
- Consumption of added sugars has been associated with increased risk of obesity [23,24,25] as well as increased risk factors for cardiovascular disease (CVD) [26], including dyslipidemia [27,28], elevated blood pressure [20,29,30], diabetes [21,31,32], non-alcoholic fatty liver disease [33,34], and even cognitive decline [35] and cancer [36,37].” [2016]
- “An estimated increase of 10 g/day in total sugar intake (about 2.4 teaspoons) was associated with an increased Alzheimer’s disease risk [2022]
Finding Your Historic Diet – my own exploration
From a post that I did seven years ago [2015], I am using myself as an example — you will likely need to do your own research. Beware of revisionist view of traditional diets — research!
Some nuggets that I found in a Christmas Present…
My wife gave me “Danish Cookbooks” by Carol Gold. This is NOT a cook book, but rather an academic study of cookbooks published in Denmark. I’m 100% Danish and very interested in history.
I have always been inclined towards going for ancestral diet patterns, and did Paleo for a while. My problem with Paleo is that it is more ideological based than actual (scientific-evidence) archeologically based. It is also trying to jump the diet back thousands of years which effectively ignores how our bacteria evolved to meet our changes of diet.
In this book, I found two gems from the historical records:
- We have decreased the use of spice considerably — in 1600, the common spices were:
- cumin, anise, coriander, dill, fennel, lavender, sage, rosemary, mint, bay leaves, cloves, pepper, saffron, thyme, marjoram, nutmeg, cardamon, ginger, cinnamon, hyssop, wormwood, lemon balm, angelica-root.
- “The issue here is … the use of seasonings in general slackens” p.47
- Many of these spices (like wormwood and ginger) have strong antibacterial characteristics which would have kept some gut bacteria families in control well.
- “Their most common food was meat” p. 122
- White (wheat) bread was very uncommon, expensive, and typically seen only in upper class homes on special occasions(not as part of the regular menus) —Note this is in Northern Europe. It appears that most of the carbohydrates came from Rye Bread.
I am sure that some readers who favor a diet that is vegan or vegetarian on ideological grounds would object to these suggestions. My response is simple, if your ancestors were vegetarians for centuries or millenniums (as some friends who were born in India can validly claim), then that is the right diet without any doubts.
Evidence shows that gut bacteria is inherited through generations — hence it is good to know what your ancestors ate because your gut bacteria have likely adapted to that diet. Given my heritage (which likely applies to people from the UK, Poland, northern France and Germany etc), this boils down to:
- Rye Bread without any wheat flour
- Meat and Fish (especially since the family seemed to always been within 5 miles of the coast back to 1500..)
- Often goat milk and goat cheese (Gjetost) were the norm and not cow milk.
- Vegetables:
- Cauliflower
- Artichoke
- Rutabaga
- Turnip
- Beets “From the Middle Ages, beetroot was used as a treatment for a variety of conditions, especially illnesses relating to digestion and the blood.”
- For more, see http://www.oldcook.com/en/medieval-vegetables
No potatoes — they really did not enter my ancestor dies until the early 1800’s – after one of my great-grandfathers was born. Little or no sugar (“Worldwide through the end of the medieval period, sugar was very expensive[1] and was considered a “fine spice“,[2] but from about the year 1500, technological improvements and New World sources began turning it into a much cheaper bulk commodity.” – Wikipedia)
Dropping back earlier in my ancestry, the Vikings. We have an excellent summary here “Viking Diet: Why you should eat like the Vikings did!” which cites historic text describing the food with archeological findings.
“Vikings farmed cold-hardy vegetables like cabbage, carrots, leeks, turnips, parsnips, garlic, onions, and other root vegetables to add vitamins and variety to their diets. They ate peas, beans, and other legumes. They were fond of apples and cherries from wild or cultivated trees and collected berries and nuts when they were in season.“
There is an excellent interview with a specialist: Nordic food culture – A historical perspective by Henry Notake. He cites “the practice of soaking fish in lye is not an original Norwegian tradition, even though the actual raw material of dry fish is. I have found recipes for lutefisk in German cookbooks, Swedish documents from the 16th century, and Spanish and Polish cookbooks from the 17th century. ” He is also the author of Printed Cookbooks in Europe, 1470-1700
Frumenty for Breakfast?
Some foods that are common now were not the case in the past and vice versa.
A Dollop of History, describes this and how to make it. It used Furmente wt Porpays (Frumenty with Porpoise) from the 14th century English manuscript, The Forme of Cury. This food and similar recipes dates back to Roman Times. It uses saffron. If you can’t get porpoise, oogruk (bearded seal) is a good substitute (a unique taste according to my wife from her own experience). For other recipes see: Medieval Recipes and Ancient Recipes on the same site.
One item to keep in mind, often surviving recipe books were written to the upper class and not your ancestors! Many recipes on the internet are modern adaptions of old recipes to suit contemporary tastes — so be warned!
Project Gutenberg does have some historic cook books available (besides The Forme of Cury cited above)
- The accomplisht cook [1588] by Robert May
- The Queen-like Closet or Rich Cabinet [1670] Hannah Woolley
- English Housewifry [1752] by Elizabeth Moxon
A list of 13-16th century cook books is on Old Cook with a list of recipes in English. Compare to this, a modern omelet is rather plain!
Ingredients (1 tsp = 1 teaspoon)
Omelette with herbs, from Arboulaste , Ménagier de Paris, 1393.
6 leaves of tansy
1 rue leaf
4 leaves of Apium (wild celery)
4 mint leaves
4 sage leaves
6 leaves of marjoram or oregano
handful of fennel (aromatic foliage)
large handful of parsley
2 handfuls of the mixture: violet leaves, spinach, lettuce, green chard
16 eggs
1tsp of ginger
salt.
This Wikipedia article may be a helpful start for many.
The last item needs to be taken with a touch of salt and sung: “A spoonful of soil helps the microbiome recover!” We have become hyper-hygienic. See the Hygiene hypothesis. This comes from a post in 2016:
“The Amish and Hutterites are U.S. agricultural populations whose lifestyles are remarkably similar in many respects but whose farming practices, in particular, are distinct; the former follow traditional farming practices whereas the latter use industrialized farming practices….Despite the similar genetic ancestries and lifestyles of Amish and Hutterite children, the prevalence of asthma and allergic sensitization was 4 and 6 times as low in the Amish” – i.e. industrialized farming practices resulted in six times (600%) the rate of asthma and allergies. See Innate Immunity and Asthma Risk in Amish and Hutterite Farm Children(2016). This is also echoed in their farm products!!! Amish and Hutterite Environmental Farm Products Have Opposite Effects on Experimental Models of Asthma [2016]. Given a choice of buying groceries from a Hutterite farm or a Amish farm, buy the Amish (non industrialized) groceries!!!!
So I advocate not a Paleo diet, but a regional medieval-food diet (partially modified for modern nutritional needs). No prepared foods (talk about being extremely unnatural!), so food prepared from scratch — ideally organic with heritage seeds. Orange carrots are unnatural! Carrots should be white! The food should also be seasonal! The rotation of food with the seasons is a significant factor. Having fresh strawberries at Christmas is so very wrong.
Are you a Mutt?
The term mutt or “Heinz 57″means mixed ancestry – for example, Asian with African, Icelander with Italian. If you are not sure, a DNA test is suggested.
If you are a mutt, look for commonality of historic foods from the dominant ancestors.
Are what you have been told is healthy wrong?
Chances are that it is corrected relative to the typical common western diet. That is the base line that most studies are done against. If you change the base line, the answer may change…
One other factor?
There is evidence that a combination of blood type and being a secretor or non-secretor impacts the body and the microbiome. There is a nice blood type table by country listed here. Iceland and Ireland are very similar (partially because both had major Viking settlements 1200 years ago). One could propose a model that traditional regional diet influenced the survival rate of different blood type which would be reflected in their blood type distribution. Compare the Scandinavian (meat eaters) to India/Sri Lanka (Vegetarians) below for aNeg,bPos and oNeg.
| country | oPos | aPos | bPos | abPos | oNeg | aNeg | bNeg | abNeg |
| Denmark | 35 | 37 | 8 | 4 | 6 | 7 | 2 | 1 |
| Norway | 33.2 | 41.6 | 6.8 | 3.4 | 5 | 7.4 | 1.2 | 0.6 |
| Sweden | 32 | 37 | 10 | 5 | 6 | 7 | 2 | 1 |
| Iceland | 46.8 | 27.2 | 9 | 2 | 8 | 4.8 | 1.6 | 0.4 |
| Sri Lanka | 43.42 | 21 | 25.78 | 5.13 | 2 | 1.04 | 1.25 | 0.26 |
| India | 32.53 | 21.8 | 32.1 | 7.7 | 2 | 1.36 | 2 | 0.48 |
| United Kingdom | 44 | 28 | 8 | 2 | 9 | 6 | 2 | 1 |
| United States | 37.4 | 35.7 | 8.5 | 3.4 | 6 | 6.3 | 1.5 | 0.6 |
| Ireland | 47 | 26 | 9 | 2 | 8 | 5 | 2 | 1 |
Bottom Line
Showing off prosperity by what you eat, trying to assimilate into local or trendy eating habits and convenient “get-healthy” diets are excellent ways to cripple your microbiome (and likely future generations). One simple example is going gluten-free. For some medical conditions it is necessary — but for a person without those conditions, available studies suggests that it is a poor choice advocated by naïve people
Food taste is acquired — cutting sugar and salt from the diet can be hard for many people. Eating turnips and rutabaga may be unfamiliar tastes. Eating 100% rye bread with goat cheese is definitely a different taste. It will take time and may present extra challenges if you have kids or other in the family that want to stick to contemporary eating habits.
My daughter states “There’s a reason why old recipes don’t always work, because ingredients are either no longer available, or they have changed over the years, or techniques have changed (see this post)”
So that is my logic and my reasoning and my evidence…
Comments from Social Media


Recent Comments