I would be interested to see how the three separate consensus suggestions compare (i.e. not doing the uber consensus). Do the top takes & avoids match across the different labs, or are they different? Because if they are different then the algorithm is not robust to changes in lab.
Using the same data, the process that I will use is where items suggested in both are the same (i.e. take or avoid) or different recommendations. In pseudo sql:
Select Percent(A.Take=B.Take) from Suggestions1 A Join Suggestions2 B on A.substance=B.substance
The results actually surprised me!
Lab Comparison
Items
Agreement
Avg Difference
Ombre vs Biomesight
1705
100%
52
Ombre vs Thorne
1706
100%
100
Biomesight vs Thorne
1694
100%
54
My expectation was somewhere between 80-90%, the same range that I got doing cross validation. The Priority and weight are different, but the take or avoid decision are the same. The difference between these pseudo values was also calculated and added to the table above. Magic Soy on Ombre may be 430, on Thorne 330, on Biomesight 530.
Conclusion, the algorithm is more robust than I expected!
Caveat: This was done using “Just give me suggestions” collection of algorithm on each lab’s data. Disagreements are definitely expected when bacteria selection are “over-focused” and not including the holistic picture of the microbiome.
Comparing standalone suggestions – 2E, a reader wanted to know how similar Microbiome Prescription suggestions were using different data
In this post we are going to combine all of the consensus from the above 3 different sample reports and see what is shared by all of the suggestions. The goal is to see whether there is come convergence of suggestions.
Uber Consensus
We select the Multiple Samples tab and then check the three consensus reports. We should note the number of modifiers in each sample suggestions (over 6000 items were consider). This on the surface appears to be at least one, if not two magnitudes more than the suggestions from the labs,
The following are selecting the highest positive or negative entries where there is good agreement.
There were no probiotics in the above to take, only those to avoid. Interesting that the labs whose business model includes selling probiotics actually suggested these probiotics (ones to be avoided above)!!This have a strong aroma of conflict of interests.
Many of the above items were not suggested by any lab despite a few being typical — i.e. melatonin.
Other Observations
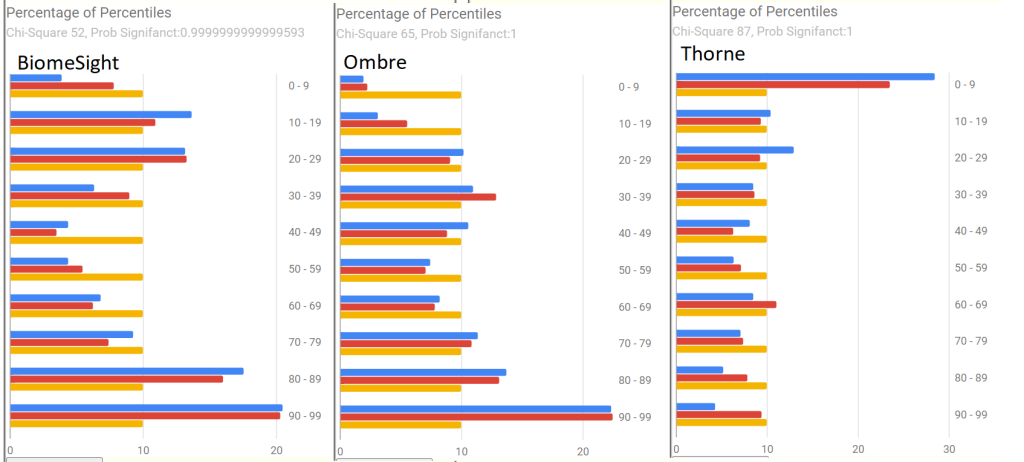
Percentages of Percentiles
For BiomeSight and Ombre, we compute percentiles based on samples uploaded. Thorne provides their own percentiles. We see a major contrast below.
Measure
BiomeSight
Ombre
Thorne
Jason Hawrelak
8 ideal (96%ile)
6 ideal (75%ile)
5 ideal (56%ile)
Bacteria Reported
748
886
3349
Shannon Diversity Index:
1.93 (89%ile)
3.34 (93%ile)
2.85 (70%ile)
Simpson Diversity Index:
0.2 (8%ile)
0.2 (5%ile)
0.3 (9%ile)
Chao1 Index :
17785 (89%ile)
33700 (89%ile)
341848 (70%ile)
The numbers are using based on the lab population
Bottom Line
The purpose of this series of post was to do a non-judgmental evaluation of the three lab reports and suggestions to help people make better choices. All of the steps that I did is very repeatable by anyone who wish to replicate this experiment. (P.S. If you do, I am not opposed to do a repeat set of posts with different data).
Key findings:
Only Biomesight provided AVOID lists (too short IMHO) — i.e. they are happy for you to keep feeding ‘bad’ bacteria
Only Biomesight provide studies links connected to their suggestions
The report from each lab are significantly different, howeverwhen that report is used with Microbiome Prescription algorithms, we get agreement. This is likely due to the nature of the algorithms used.
My impression is to use whichever lab is available to you (two sell in the US only, one world wide); ignore their suggestions and use the free suggestion engine on Microbiome Prescription.
Microbiome Prescription does provide detail evidence trail on every single suggestion it makes. Some of the evidence is less than ideal, but it is at least reasonable (and less than ideal data is diminished in weight).
I gave this an Excellent because it matched the criteria that I use:
Avoid lists are given
Evidence trail to studies for every suggestion
A large number of substances are evaluated
Weights are given for Take lists.
(And I acknowledge there is a conflict of interests here — but no financial gain).
The following videos illustrate the process to see the evidence trail.
Comparing standalone suggestions – 2E, a reader wanted to know how similar Microbiome Prescription suggestions were using different data
Process
It is very simple, look at their suggestions, look at any references they provided. Then look at Microbiome Prescription evidence trail for the same substances.
Suggestions
The number of suggestions were very few. They are listed below. None of the suggestions had links to studies supporting them.
Follow a ketogenic or low-carbohydrate diet
Avoid eating habits that interfere with sleep
Product Recommendations
Dipan-9®: Pancreatin
Effusio® Prebiotic+
Blueberry
Green Tea
Pomegranate
Xylitol
Stevia
FloraMend Prime Probiotic®
L. Gasseri KS-13
B. Longum MM-2
B. Bifidum G9-1
Undecylenic Acid – 10-Undecenoic Acid
Vitamins were:
Red: Vitamin B3, B12
Orange: Vitamin B6,B9
All probiotics were GREEN.
There was no scientific literature links provided to support these choices.
How do suggestions compare?
Analysis against Microbiome Prescription using the data they reported.
Vitamin B3: take 3, avoid 1
Vitamin B6: take 3, avoid 1
Vitamin B9: take 3, avoid 1
Vitamin B12, take 3, avoid 1
L. Gasseri: take 1, avoid 3
B. Longum: take 0, avoid 3
B. Bifidum: take 0, avoid 4
Blueberry: take 3, avoid 1
Green Tea: take 2, avoid 2
Pomegranate: take 1, avoid 3
Xylitol: take 2, avoid 1
Stevia: take 0, avoid 4
Pancreatin: take 1, avoid 0
ketogenic: take 1, avoid 3
low-carbohydrate diet: take 2, avoid 1
Undecylenic are in Microbiome Prescription database. Undecylenic has nothing on PubMed dealing with the microbiome that I could locate.
My Impression are:
For the 4 B-vitamins we have agreement.
For everything else, we have so-so agreement. In fact, the agreement is the same that you would expect with flipping a coin (random)
We have very few suggestions of what to take
We have no clear suggestions on what to avoid (beyond “other diet” types).
Bottom Line
Thorne gives almost no suggestions. There is no links to study supporting their suggestion. The suggestions seem to be ultra-safe suggestions that should work for most people. It if very questionable if the bacteria results were used for the suggestions.
As an ex-teacher, I would not give a grade, I would give an INCOMPLETE-FAILED, nothing of significance submitted. No real effort made.
The videos below shows how you can see the evidence for the suggestions on Microbiome Prescription.
Comparing standalone suggestions – 2E, a reader wanted to know how similar Microbiome Prescription suggestions were using different data
Process
It is very simple, look at their suggestions, look at any references they provided. Then look at Microbiome Prescription evidence trail for the same substances. My usual “Just the facts, ma’am” approach. This data was retrieved on 24 Aug 2023.
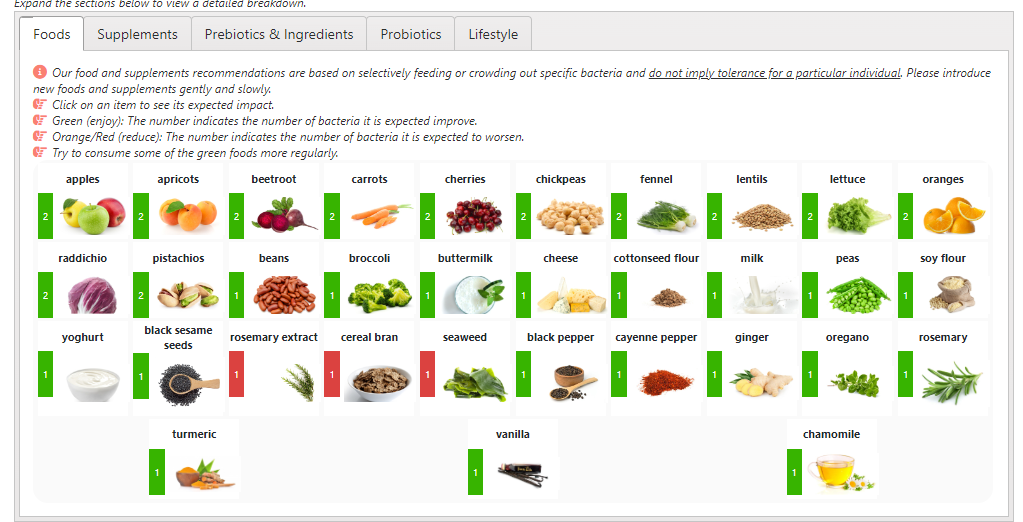
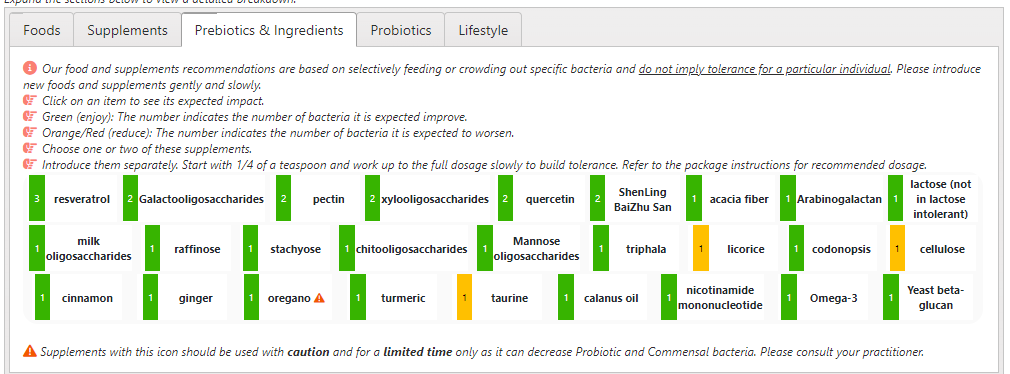
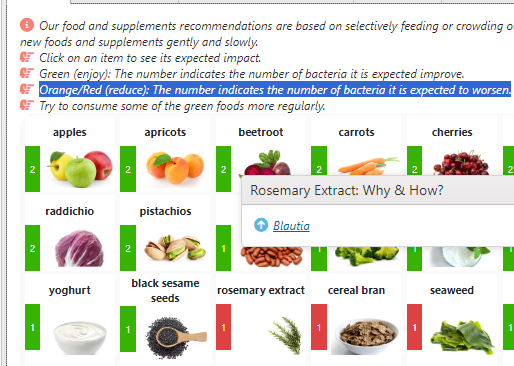
First item, the suggestions are far wider and deeper than Ombre. With Rosemary and Rosemary extract being separate!
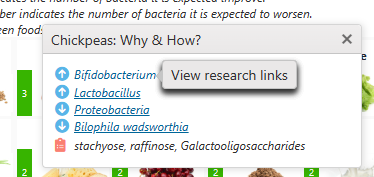
Clicking one the green bar describes the why with links to research.
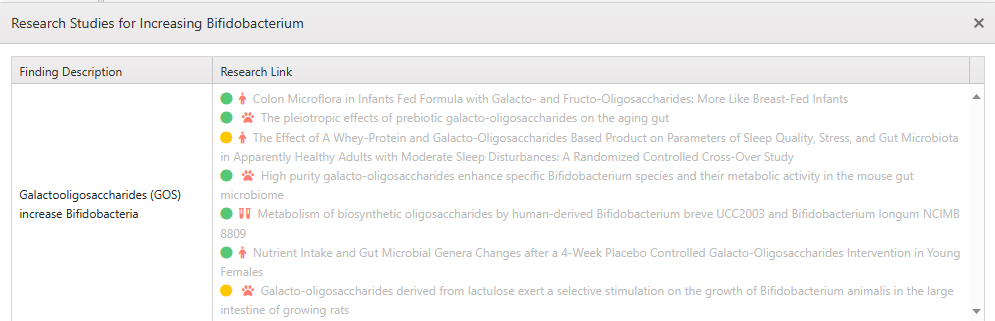
Unfortunately the research suggestions appears to be second generation. For example, when I clicked on Bifidobacterium, I see that Chickpeas are transformed to Galactooligosaccharides (GOS) which is reasonably correct with a risk of over simplification.
“The galacto-oligosaccharides (GOSs) naturally occur in legumes such as lentils, chickpeas, and beans.”[2016]
Chickpeas, lentils and beans contain other substances. A First generation reference would explicitly cite chickpeas. A second generation would cite a component that is significant in chickpeas(with fingers crossed that other components will not have an adverse effect).
This same process is done for Pre-biotics & Ingredients, Probiotics and LifeStyle
Items to avoid are shown in red (sometimes there are none). The “orange” color appears to be me to be more a yellow (to my eyes).
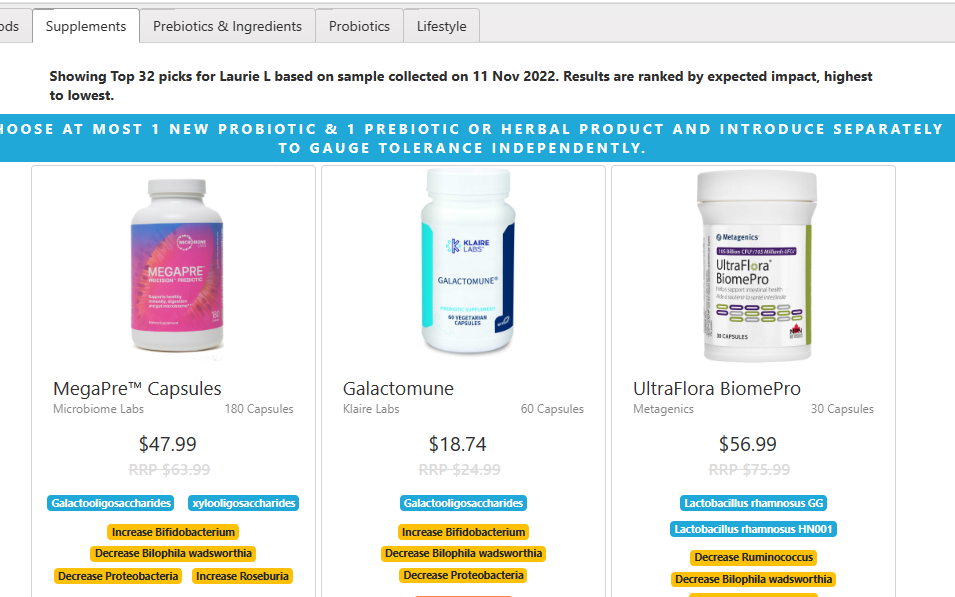
Supplements – Ugh
My preference is to name the explicit supplements to take (and to avoid) and have the user find a product somewhere. Biomesight provides the product name (which can be ordered thru them) and below the product list the whys. From the time it takes this page to render, I surmise they are computing them upon request
Spot checking the very first item, we see the ingrediants:
Galactooligosaccharides (Bimuno®)
Organic gold and green kiwifruit powder (Livaux® and ACTAZIN®)
Organic Xylooligosaccharides (PreticX®)
How do suggestions compare?
Microbiome Prescription tries to use first generation citations, BiomeSight appears to often use second generation citations [Ombre appears to use halogenic citations]. The ones that I checked are good as second generation citations.
Below are the take suggestions from Biomesight and what Microbiome Prescription consensus suggests. I skipped foods to minimize second generation citation issues.
Substance
MP Take
MP Avoid
resveratrol
4
0
Galactooligosaccharides
4
0
pectin
1
3
xylooligosaccharides
0
3
quercetin
4
0
ShenLing BaiZhu San
1
3
acacia fiber
–
–
Arabinogalactan
0
4
lactose (not in lactose intolerant)
3
0
milk oligosaccharides
3
1
raffinose
3
0
stachyose
3
1
chitooligosaccharides
4
0
Mannose oligosaccharides
4
0
triphala
2
2
licorice
4
0
codonopsis
3
0
cellulose
0
4
cinnamon
3
0
ginger
2
2
oregano
0
4
turmeric
4
0
taurine
0
1
calanus oil
–
–
nicotinamide mononucleotide
4
0
Omega-3
1
3
Yeast beta-glucan
0
4
Bacillus subtilis
1
3
Bifidobacterium longum BB536
0
3
Methylobacterium longum
–
–
Bacillus coagulans
1
3
Lactobacillus rhamnosus HN001
0
4
Lactobacillus rhamnosus GG
0
4
Lactobacillus rhamnosus CNCM I-3690
–
–
Remember that the suggestions are based on the bacteria selected to be modified. Different selections produces different results.
The first one with major disagreement was Arabinogalactan. I extracted the citations that I used with the bacteria impacted and attach it below.
For Supplements etc, we have 64% with reasonable agreement and 56% with strong agreement.
For Probiotics, we have zero agreement. 🙁
Items to AVOID are there — but the number is sparse, less than ideal.
The use of colors only is a poor UI choice (IMHO) because many people are color blind (8% of all males)
There is no words indicating this should be an avoid.
Bottom Line
Biomesight gives reasonable suggestions. The differences could be ascribed to the selection of bacteria needing modification. Microbiome Prescript default is to use 4 different algorithms to select bacteria and then aggregate into a consensus. I suspect Biomesight uses a single algorithm.
The absence of items to avoid is a significant omission IMHO.
I am a little concern for probiotic suggestions. This suggests two obvious possibilities: data entry issues or not sufficient coverage of available literature.
I would give their suggestions with supporting evidence a good rating. I suspect with enough time and manpower that they could raise it to excellent.
The videos below shows how you can see the evidence for the suggestions on Microbiome Prescription.
Comparing standalone suggestions – 2E, a reader wanted to know how similar Microbiome Prescription suggestions were using different data
Process
It is very simple, look at their suggestions, look at any references they provided. Then look at Microbiome Prescription evidence trail for the same substances. My usual “Just the facts, ma’am” approach. This data was retrieved on 24 Aug 2023.
They recommended their own brand mixture
Then we asked for suggests with no diet and no allergies.
Oyster, citing below: This word was not found in the full text of either
At this point, I deem their evidence is grossly insufficient. Not one solid piece of evidence in almost 30 “scientific evidence”. I will say myself frustration (and the reader boredome) .
Using Microbiome Prescription Evidence
Most of the studies cited above were references to FODMAP, either low or high with this being ignored.
Multivariate modelling of faecal bacterial profiles of patients with IBS predicts responsiveness to a diet low in FODMAPs. Gut (Gut ) Vol: 67 Issue 5 Pages: 872-881 Pub: 2018 May Epub: 2017 Apr 17 Authors Bennet SMP , Böhn L , Störsrud S , Liljebo T , Collin L , Lindfors P , Törnblom H , Öhman L , Simrén M ,
For Tagliatelle (Pasta), we find the following study with adverse effect on many bacteria (it was an avoid)
Carbohydrate Staple Food Modulates Gut Microbiota of Mongolians in China. Frontiers in microbiology (Front Microbiol ) Vol: 8 Issue Pages: 484, Pub: 2017 Epub: 2017 Mar 21 Authors Li J , Hou Q , Zhang J , Xu H , Sun Z , Menghe B , Zhang H ,
Yuzu (Yuzu is a citrus fruit). This is not in the database, but another citric food is there, and it is a take suggestion
Analysis of Temporal Changes in Growth and Gene Expression for Commensal Gut Microbes in Response to the Polyphenol Naringenin. Microbiology insights (Microbiol Insights ) Vol: 11 Issue Pages: 1178636118775100 Pub: 2018 Epub: 2018 May 30 Authors Firrman J , Liu L , Argoty GA , Zhang L , Tomasula P , Wang M , Pontious S , Kobori M , Xiao W
The inhibitory effect of polyphenols on human gut microbiota. Journal of physiology and pharmacology : an official journal of the Polish Physiological Society (J Physiol Pharmacol ) Vol: 63 Issue 5 Pages: 497-503 Pub: 2012 Oct Epub: Authors Duda-Chodak A ,
For beans — we have the same citation to bean and soy tempeh
For Garlic, we have it as an avoid with the following studies being the basis
Effect of garlic powder on the growth of commensal bacteria from the gastrointestinal tract. Phytomedicine : international journal of phytotherapy and phytopharmacology (Phytomedicine ) Vol: 19 Issue 8-9 Pages: 707-11 Pub: 2012 Jun 15 Epub: 2012 Apr 4 Authors Filocamo A , Nueno-Palop C , Bisignano C , Mandalari G , Narbad A ,
Dietary prophage inducers and antimicrobials: toward landscaping the human gut microbiome. Gut microbes (Gut Microbes ) Vol: Issue Pages: 1-14 Pub: 2020 Jan 13 Epub: 2020 Jan 13 Authors Boling L , Cuevas DA , Grasis JA , Kang HS , Knowles B , Levi K , Maughan H , McNair K , Rojas MI , Sanchez SE , Smurthwaite C , Rohwer F
Inhibitory activity of garlic (Allium sativum) extract on multidrug-resistant Streptococcus mutans. Journal of the Indian Society of Pedodontics and Preventive Dentistry (J Indian Soc Pedod Prev Dent ) Vol: 25 Issue 4 Pages: 164-8 Pub: 2007 Oct-Dec Epub: Authors Fani MM , Kohanteb J , Dayaghi M
Effects of garlic polysaccharide on alcoholic liver fibrosis and intestinal microflora in mice. Pharmaceutical biology (Pharm Biol ) Vol: 56 Issue 1 Pages: 325-332 Pub: 2018 Dec Epub: Authors Wang Y , Guan M , Zhao X , Li X
Black garlic melanoidins prevent obesity, reduce serum LPS levels and modulate the gut microbiota composition in high-fat diet-induced obese C57BL/6J mice. Food & function (Food Funct ) Vol: 11 Issue 11 Pages: 9585-9598 Pub: 2020 Nov 18 Epub: Authors Wu J , Liu Y , Dou Z , Wu T , Liu R , Sui W , Jin Y , Zhang M
Their recommended probiotic contains the following species (with the evidence based suggestions count after):
L. Acidophilus – Mixed impact (2 plus, 1 minus)
E. Faecium – Avoid (3 minus)
L. Paracasei – MAJOR Avoid ( 4 minus)
L. Helveticus – Avoid ( 3 minus, 1 plus)
L. Rhamnosus – Mixed (2 plus, 2 minus)
L. Plantarum – MAJOR Avoid (4 minus)
B. Lactis – MAJOR Avoid (4 minus)
S. Boulardi – Mixed (2 plus, 2 minus)
IMHO, this is NOT a good mixture to take.
Bottom Line
Ombre’s suggestions for both probiotic and diet style leaves great opportunity to be made better. Their scientific citations is almost an embarrassment. I suspect that they were contracted out to a dietician and had no or poor quality control/review.
The videos below shows how you can see the evidence for the suggestions on Microbiome Prescription.
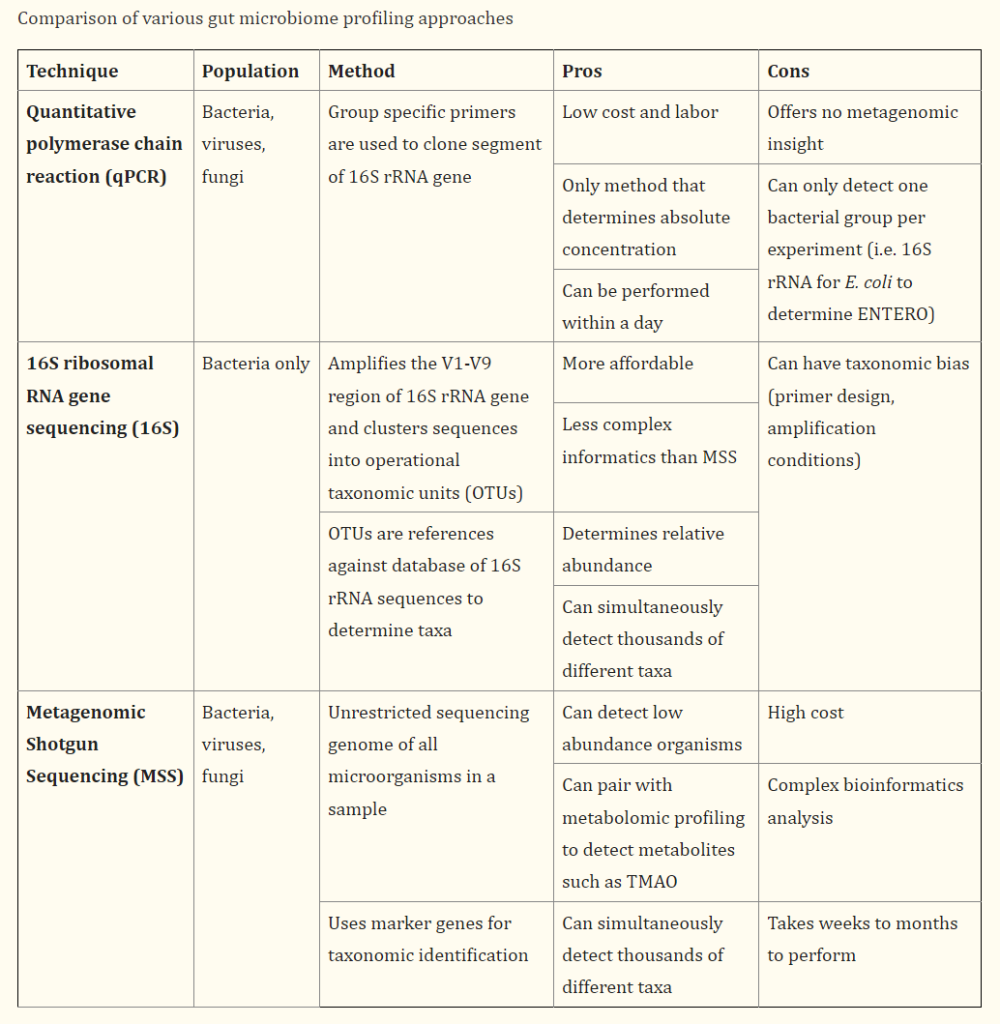
A reader did Ombre and Thorne from the same physical sample and then processed the Ombre results via Biomeisght resulting in three different reports on the same shit. That is:
Ombre (16s) – same digital data used
Biomesight (16s) – same digital data used
Thorne (MSS)
This is the first of two parts — the bacteria numbers as percentiles and percentages, The second part will look at suggestions from each (and provided documentation for why it was suggested when available).
My intent is not to suggest/render judgements on the different test results, just show the differences. It should be noted that most studies are done with 16s and not MSS. Conclusions from one study may not be reproduceable using a different lab/software (even with the same digital data).
Pass #1: Percentile Rankings
These are the most likely to be similar between samples. I only looked at those bacteria reported by all three samples.
phylum
Thryve
BiomeSight
Thorne
Acidobacteria
76
10
52
Actinobacteria
38
46
65
Bacteroidetes
16
6
79
Chloroflexi
99
88
88
Cyanobacteria
96
96
56
Firmicutes
72
86
6
Fusobacteria
14
10
78
Proteobacteria
27
14
29
Synergistetes
46
5
42
Tenericutes
77
61
37
Verrucomicrobia
81
83
64
class
Thryve
BiomeSight
Thorne
Actinomycetia
46
54
62
Alphaproteobacteria
35
52
58
Anaerolineae
33
84
53
Bacilli
84
62
58
Bacteroidia
16
6
80
Betaproteobacteria
24
13
15
Caldilineae
100
79
1
Clostridia
63
90
7
Coriobacteriia
76
81
73
Cytophagia
20
58
77
Deltaproteobacteria
81
78
81
Epsilonproteobacteria
68
71
95
Erysipelotrichia
18
28
36
Fusobacteriia
14
10
78
Gammaproteobacteria
47
39
60
Mollicutes
78
61
35
Negativicutes
90
88
3
Opitutae
59
78
60
Synergistia
46
5
42
Tissierellia
96
99
88
Verrucomicrobiae
81
81
63
order
Thryve
BiomeSight
Thorne
Acholeplasmatales
77
62
4
Acidaminococcales
20
21
17
Actinomycetales
93
95
45
Alteromonadales
16
95
86
Anaerolineales
33
26
61
Bacillales
90
47
75
Bacteroidales
16
6
80
Bifidobacteriales
30
25
37
Burkholderiales
24
13
14
Caldilineales
100
79
1
Campylobacterales
68
71
96
Chromatiales
45
92
72
Coriobacteriales
47
84
11
Corynebacteriales
91
94
96
Cytophagales
21
58
77
Desulfovibrionales
81
78
80
Eggerthellales
92
94
96
Enterobacterales
29
22
67
Erysipelotrichales
18
28
36
Eubacteriales
64
89
7
Fusobacteriales
14
10
78
Halanaerobiales
94
100
67
Hyphomicrobiales
18
74
94
Lactobacillales
83
67
61
Micrococcales
39
9
92
Micromonosporales
74
19
85
Mycoplasmatales
87
86
54
Nostocales
72
97
25
Oceanospirillales
57
10
89
Oscillatoriales
95
80
28
Puniceicoccales
62
16
1
Rhodospirillales
8
50
41
Rickettsiales
29
10
49
Selenomonadales
85
86
29
Streptosporangiales
56
78
76
Synergistales
47
5
42
Thermoanaerobacterales
22
18
48
Tissierellales
95
99
82
Veillonellales
96
92
10
Verrucomicrobiales
81
81
63
family
Thryve
BiomeSight
Thorne
Acholeplasmataceae
77
62
4
Acidaminococcaceae
21
21
17
Actinomycetaceae
93
95
66
Aerococcaceae
92
98
60
Akkermansiaceae
82
85
69
Anaerolineaceae
35
26
61
Atopobiaceae
90
16
71
Bacillaceae
76
98
97
Bacteroidaceae
23
15
55
Bifidobacteriaceae
32
25
41
Bradyrhizobiaceae
34
25
81
Caldilineaceae
100
79
1
Campylobacteraceae
68
66
95
Carnobacteriaceae
52
10
67
Clostridiaceae
87
94
12
Coprobacillaceae Verbarg et al. 2014
76
42
1
Coriobacteriaceae
18
84
7
Corynebacteriaceae
90
92
95
Desulfovibrionaceae
83
78
80
Dysgonomonadaceae
60
4
79
Eggerthellaceae
92
94
96
Enterobacteriaceae
58
23
67
Enterococcaceae
60
62
89
Erysipelotrichaceae
19
25
39
Eubacteriaceae
92
77
29
Eubacteriales Family XIII. Incertae Sedis
95
96
66
Lachnospiraceae
80
93
26
Lactobacillaceae
89
74
64
Micrococcaceae
16
13
91
Microcoleaceae
91
77
1
Micromonosporaceae
74
20
85
Mycoplasmataceae
87
86
54
Odoribacteraceae
97
94
77
Oscillospiraceae
34
54
17
Paenibacillaceae
95
47
96
Peptococcaceae
98
90
39
Peptoniphilaceae
95
99
82
Peptostreptococcaceae
47
84
83
Planococcaceae
30
80
78
Porphyromonadaceae
55
27
36
Prevotellaceae
58
52
50
Puniceicoccaceae
63
58
1
Rhodospirillaceae
10
48
35
Rickettsiaceae
35
13
38
Selenomonadaceae
81
87
26
Sporomusaceae
86
38
46
Streptococcaceae
55
66
73
Streptosporangiaceae
68
20
52
Sutterellaceae
24
14
9
Syntrophomonadaceae
96
58
6
Tannerellaceae
29
20
76
Thermoactinomycetaceae
85
88
43
Turicibacteraceae Verbarg et al. 2014
26
27
22
Veillonellaceae
96
92
10
genus
Thryve
BiomeSight
Thorne
Acetivibrio
66
86
14
Acetobacterium
98
85
13
Acholeplasma
77
48
6
Actinobaculum
38
83
3
Actinomyces
74
79
53
Actinotignum
51
71
62
Akkermansia
82
85
69
Alloscardovia
93
93
1
Anaerococcus
94
96
81
Anaerostipes
90
73
41
Arcanobacterium
97
97
5
Bacillus
21
93
96
Bacteroides
26
16
71
Bifidobacterium
19
18
44
Bilophila
59
61
2
Blautia
84
94
4
Brevibacillus
41
85
87
Butyricimonas
73
56
82
Butyrivibrio
94
87
74
Caloramator
65
60
7
Campylobacter
67
67
96
Clostridium
78
87
16
Coprobacillus
87
49
1
Coprococcus
27
4
22
Corynebacterium
90
92
95
Desulfotomaculum
82
75
60
Desulfovibrio
69
84
87
Dialister
97
93
45
Dorea
90
69
1
Dysgonomonas
60
4
40
Eggerthella
75
78
86
Enterococcus
26
67
88
Erysipelothrix
76
67
17
Escherichia
72
32
52
Ethanoligenens
99
37
47
Eubacterium
92
54
38
Faecalibacterium
33
32
21
Filifactor
78
97
50
Finegoldia
90
84
75
Gemella
65
97
18
Hathewaya
88
77
1
Helcococcus
99
87
6
Lachnospira
5
93
88
Lactobacillus
89
60
64
Ligilactobacillus
58
15
81
Limosilactobacillus
24
23
49
Mediterraneibacter
86
81
46
Megasphaera
91
97
41
Mobiluncus
18
16
3
Mogibacterium
98
96
31
Mycoplasma
88
86
47
Mycoplasmopsis
35
94
0
Negativicoccus
75
92
24
Odoribacter
98
98
58
Paenibacillus
95
99
96
Parabacteroides
29
20
76
Pectinatus
23
19
2
Peptococcus
82
90
1
Peptoniphilus
95
99
69
Phocaeicola
3
25
55
Porphyromonas
94
95
97
Prevotella
67
64
58
Pseudobutyrivibrio
40
43
28
Roseburia
69
60
63
Ruminiclostridium
76
46
5
Ruminococcus
91
84
8
Schaalia
36
10
26
Slackia
37
81
10
Streptococcus
56
70
75
Sutterella
46
14
16
Syntrophomonas
97
20
2
Thermoclostridium
60
38
34
Turicibacter
26
27
22
Varibaculum
86
86
2
Veillonella
60
84
20
Weissella
87
13
31
Pass #2: Percentage
phylum
Thryve
BiomeSight
Thorne
Acidobacteria
0.011
0.002
0.005
Actinobacteria
0.652
0.364
2.117
Bacteroidetes
12.526
12.633
60.723
Chloroflexi
0.183
0.02
0.02
Cyanobacteria
0.123
0.374
0.024
Firmicutes
82.61
82.717
27.458
Fusobacteria
0.002
0.002
0.02
Proteobacteria
1.163
1.502
1.894
Synergistetes
0.004
0.002
0.005
Tenericutes
0.049
0.048
0.015
Verrucomicrobia
1.994
1.954
0.627
class
Thryve
BiomeSight
Thorne
Actinomycetia
0.641
0.351
1.093
Alphaproteobacteria
0.013
0.085
0.171
Anaerolineae
0.002
0.011
0.003
Bacilli
2.931
0.729
0.765
Bacteroidia
12.522
10.238
60.036
Betaproteobacteria
0.266
0.263
0.175
Caldilineae
0.182
0.009
0.001
Clostridia
73.508
81.689
25.405
Coriobacteriia
0.665
0.527
0.989
Cytophagia
0.004
0.036
0.047
Deltaproteobacteria
0.723
0.735
0.875
Epsilonproteobacteria
0.011
0.009
0.275
Erysipelotrichia
0.281
0.191
0.336
Fusobacteriia
0.002
0.002
0.02
Gammaproteobacteria
0.152
0.198
0.359
Mollicutes
0.049
0.048
0.013
Negativicutes
3.839
3.4
0.069
Opitutae
0.004
0.008
0.004
Synergistia
0.004
0.002
0.005
Tissierellia
1.468
3.352
0.386
Verrucomicrobiae
1.993
1.946
0.621
order
Thryve
BiomeSight
Thorne
Acholeplasmatales
0.023
0.033
0.002
Acidaminococcales
0.008
0.007
0.007
Actinomycetales
0.092
0.321
0.021
Alteromonadales
0.002
0.065
0.021
Anaerolineales
0.002
0.002
0.003
Bacillales
0.231
0.147
0.233
Bacteroidales
12.567
10.238
60.01
Bifidobacteriales
0.164
0.03
0.123
Burkholderiales
0.267
0.259
0.127
Caldilineales
0.182
0.009
0.001
Campylobacterales
0.011
0.009
0.273
Chromatiales
0.004
0.03
0.013
Coriobacteriales
0.143
0.527
0.025
Corynebacteriales
0.196
0.202
0.81
Cytophagales
0.004
0.036
0.047
Desulfovibrionales
0.716
0.727
0.825
Eggerthellales
0.517
0.525
0.963
Enterobacterales
0.011
0.012
0.157
Erysipelotrichales
0.282
0.191
0.336
Eubacteriales
73.717
80.554
25.38
Fusobacteriales
0.002
0.002
0.02
Halanaerobiales
0.013
0.239
0.004
Hyphomicrobiales
0.002
0.008
0.07
Lactobacillales
2.71
0.388
0.525
Micrococcales
0.006
0.002
0.063
Micromonosporales
0.004
0.002
0.006
Mycoplasmatales
0.021
0.015
0.007
Nostocales
0.006
0.357
0.005
Oceanospirillales
0.008
0.002
0.02
Oscillatoriales
0.117
0.009
0.002
Puniceicoccales
0.004
0.002
0
Rhodospirillales
0.002
0.069
0.021
Rickettsiales
0.002
0.002
0.004
Selenomonadales
0.096
0.392
0.02
Streptosporangiales
0.004
0.008
0.007
Synergistales
0.004
0.002
0.005
Thermoanaerobacterales
0.002
0.007
0.019
Tissierellales
0.99
3.424
0.267
Veillonellales
3.749
3.4
0.041
Verrucomicrobiales
2
1.946
0.621
family
Thryve
BiomeSight
Thorne
Acholeplasmataceae
0.023
0.033
0.002
Acidaminococcaceae
0.008
0.007
0.007
Actinomycetaceae
0.096
0.086
0.021
Aerococcaceae
0.096
0.084
0.007
Akkermansiaceae
2.07
1.903
0.616
Anaerolineaceae
0.002
0.002
0.003
Atopobiaceae
0.141
0.002
0.018
Bacillaceae
0.014
0.07
0.085
Bacteroidaceae
8.206
7.869
30.336
Bifidobacteriaceae
0.17
0.03
0.123
Bradyrhizobiaceae
0.002
0.002
0.011
Caldilineaceae
0.189
0.009
0.001
Campylobacteraceae
0.012
0.009
0.267
Carnobacteriaceae
0.004
0.002
0.007
Clostridiaceae
2.456
11.827
0.304
Coprobacillaceae Verbarg et al. 2014
0.051
0.138
0
Coriobacteriaceae
0.006
0.527
0.007
Corynebacteriaceae
0.195
0.192
0.776
Desulfovibrionaceae
0.743
0.721
0.822
Dysgonomonadaceae
0.006
0.002
0.023
Eggerthellaceae
0.537
0.525
0.963
Enterobacteriaceae
0.012
0.012
0.117
Enterococcaceae
0.004
0.015
0.06
Erysipelotrichaceae
0.293
0.138
0.336
Eubacteriaceae
8.637
0.25
0.054
Eubacteriales Family XIII. Incertae Sedis
0.377
0.188
0.047
Lachnospiraceae
35.558
38.817
15.522
Lactobacillaceae
2.488
0.047
0.09
Micrococcaceae
0.002
0.002
0.027
Microcoleaceae
0.121
0.007
0.001
Micromonosporaceae
0.004
0.002
0.006
Mycoplasmataceae
0.022
0.015
0.006
Odoribacteraceae
1.028
0.955
0.588
Oscillospiraceae
1.604
21.973
5.153
Paenibacillaceae
0.105
0.007
0.085
Peptococcaceae
0.295
0.178
0.03
Peptoniphilaceae
1.028
3.413
0.261
Peptostreptococcaceae
0.162
0.047
0.81
Planococcaceae
0.006
0.006
0.015
Porphyromonadaceae
1.701
0.886
1.001
Prevotellaceae
0.654
0.507
0.285
Puniceicoccaceae
0.004
0.004
0
Rhodospirillaceae
0.002
0.065
0.012
Rickettsiaceae
0.002
0.002
0.002
Selenomonadaceae
0.078
0.388
0.016
Sporomusaceae
0.022
0.004
0.004
Streptococcaceae
0.18
0.165
0.344
Streptosporangiaceae
0.004
0.002
0.003
Sutterellaceae
0.277
0.255
0.028
Syntrophomonadaceae
0.016
0.034
0.001
Tannerellaceae
0.389
0.545
2.972
Thermoactinomycetaceae
0.01
0.015
0.004
Turicibacteraceae Verbarg et al. 2014
0.004
0.004
0.004
Veillonellaceae
3.892
3.4
0.041
genus
Thryve
BiomeSight
Thorne
Acetivibrio
0.019
0.473
0.007
Acetobacterium
0.015
0.196
0.003
Acholeplasma
0.023
0.007
0.001
Actinobaculum
0.002
0.006
0
Actinomyces
0.015
0.014
0.009
Actinotignum
0.004
0.004
0.005
Akkermansia
1.995
1.903
0.616
Alloscardovia
0.009
0.009
0
Anaerococcus
0.414
0.407
0.073
Anaerostipes
4.839
0.144
0.173
Arcanobacterium
0.03
0.03
0.001
Bacillus
0.002
0.019
0.052
Bacteroides
7.908
7.869
30.336
Bifidobacterium
0.017
0.019
0.121
Bilophila
0.295
0.292
0.002
Blautia
13.004
18.727
1.315
Brevibacillus
0.002
0.004
0.004
Butyricimonas
0.147
0.142
0.374
Butyrivibrio
0.276
0.108
0.066
Caloramator
0.023
0.241
0.003
Campylobacter
0.011
0.009
0.263
Clostridium
1.006
3.204
0.188
Coprobacillus
0.051
0.138
0
Coprococcus
0.196
0.035
0.277
Corynebacterium
0.188
0.192
0.761
Desulfotomaculum
0.017
0.007
0.006
Desulfovibrio
0.414
0.429
0.813
Dialister
2.448
2.075
0.019
Dorea
1.94
0.535
0.001
Dysgonomonas
0.006
0.002
0.006
Eggerthella
0.077
0.046
0.139
Enterococcus
0.002
0.013
0.056
Erysipelothrix
0.008
0.019
0.003
Escherichia
0.011
0.01
0.03
Ethanoligenens
0.756
0.004
0.007
Eubacterium
8.214
0.039
0.051
Faecalibacterium
6.494
8.261
4.065
Filifactor
0.008
0.043
0.004
Finegoldia
0.154
0.054
0.041
Gemella
0.006
0.099
0.003
Hathewaya
0.013
0.349
0.001
Helcococcus
0.024
0.006
0.001
Lachnospira
0.004
7.122
4.473
Lactobacillus
2.397
0.017
0.043
Ligilactobacillus
0.006
0.002
0.029
Limosilactobacillus
0.002
0.002
0.003
Mediterraneibacter
5.661
0.813
0.456
Megasphaera
0.036
0.196
0.009
Mobiluncus
0.002
0.002
0.001
Mogibacterium
0.143
0.188
0.007
Mycoplasma
0.021
0.015
0.006
Mycoplasmopsis
0.002
0.015
0
Negativicoccus
0.008
0.06
0.002
Odoribacter
0.844
0.813
0.202
Paenibacillus
0.098
0.017
0.072
Parabacteroides
0.389
0.545
2.955
Pectinatus
0.002
0.004
0.001
Peptococcus
0.019
0.145
0.001
Peptoniphilus
0.395
2.946
0.09
Phocaeicola
0.002
3.922
10.611
Porphyromonas
0.352
0.335
1.001
Prevotella
0.63
0.507
0.158
Pseudobutyrivibrio
0.004
0.076
0.022
Roseburia
2.675
2.71
3.37
Ruminiclostridium
1.995
0.008
0.002
Ruminococcus
8.972
9.736
0.374
Schaalia
0.004
0.002
0.003
Slackia
0.008
0.107
0.003
Streptococcus
0.171
0.165
0.34
Sutterella
0.211
0.255
0.028
Syntrophomonas
0.015
0.002
0
Thermoclostridium
0.004
0.006
0.004
Turicibacter
0.004
0.004
0.004
Varibaculum
0.036
0.034
0.001
Veillonella
0.023
0.556
0.01
Weissella
0.017
0.002
0.003
Bottom Line….
For some bacteria we have the numbers being close, and for others very, very different. Often we see percentage being 10x different between tests! For Percentile, we see one test reforming 91%ile and a different test reporting 1%.
A human analogy: You pick a person off the street and ask “What is this person?” A Canadian? A Swede?
There is usually no clear answer —
Their name may indicate Iceland — GuðrúnJónsdóttir
Their passport may indicate that they are a Canadian Citizen
Their skin color may indicate that they are from Africa
Their nose may suggest that are from the Mediterranean
Their DNA may suggest that they are part Nigerian, Finnish, Thai, Irish
They are mitochondrial Haplogroup K, very common among Jewish People
Their eating habits suggests they may be Hindu
The way they speak English suggests that they are Haida Gwaii (native tribe on Canada’s west coast)
Their music preference (opera) suggests Italian
Bacteria exchange RNA etc constantly — just like our humans! We may want to have definitive answers — we should fix ourselves before complaining about bacteria! ;-). Different tests use different characteristics to give a bacteria a name.
What I am curious about is whether these changes make dramatic changes in suggestions.
These are notes in progress. Use them at your own risk
In terms of KEGG data, one enzyme stands out: ATP:L-threonine O3-phosphotransferase (2.7.1.177). This is referred to as L-threonine in simpler terms. The people with this sensitivity has 10% of the levels of people not reporting it and there is a value for almost every sample.
This lead to this interest quote (dealing with plants)
“Salicylic acid[SA] .. in the rhizosphere may be strongly reduced, or completely abolished, due to the presence of histidine and threonine in the root exudates.” [2014] in other threonine may be a key chemical is processing SA.
There are no probiotics that produces it. It is available as a supplement, with WebMd suggests this dosage of “Early research suggests that taking 1.5 grams to 2 grams of threonine by mouththree times daily might improve some symptoms in people with familial spastic paraparesis. But the improvement does not seem to be very significant.”
I was unable to find anyone trying this for Salicylate Sensitivity (Hint: any volunteers?)
Salicylate Issues
I did an analysis looking at the frequency percentage of a bacteria being found for Biomesight samples (the largest collection). The key items are below. The higher the Chi2 value, the more likely it is.
I did an analysis looking at the frequency percentage of a bacteria being found for Biomesight samples (the largest collection). The statistically significant items are below, with 1 overgrowth “Streptococcus oralis” and the rest as undergrowth . The higher the Chi2 value, the more likely it is.
This is a hot new area is a speculation, first suggested in Postbiotics: what else?[2013] which states “Recent work on relevant probiotic strains has also led to the isolation and characterization of certain probiotic-produced, soluble factors, here called postbiotics, which were sufficient to elicit the desired response.”. To translate, culture probiotic and separate out the chemicals they produce (for example, lactic acid for lactobacillus cultures), you do not alter their composition. It appears that marketing types are using the same term for something different that they are trying to sell.
There are just two clinical studies in progress. All from 2022 or later, a few examples:
Lysate Probiotics: See Lysis – Wikipedia. This is caused by gently breaking down a bacteria (probiotic) often using bacteriophages. It keeps all of the components intact, but the cell is no longer alive. This has had clinical studies, for example
Bacterial lysates in food allergy prevention [2013] “heat-killed Bifidobacterium breve and Streptococcus thermophilus; … food allergy prevalence could not be reduced by these interventions.”
Sterilized: This is cooking the bacteria to kill it. It changes the factors or metabolites that would be there if the bacteria had been killed by a bacteriophages.
The new Snake Oil
A reader asked me about one new product, Thaenabiotic being pushed by Flora Medicine in Portland, OR. This is described as:
ThaenaBiotic® is a fecal-derived, sterilized, full-spectrum postbiotic that contains metabolites from a unique, healthy ecosystem of microbes originating from special, hand-picked donors.
https://www.floramedicine.com/thaenabiotic
This is the second time in a month that I have been asked about sterilized fecal matter postbiotics (or similar names). I roll my eyes for several reasons:
Being sterilized means “He’s dead Jim”. Not just changed but well cooked (perhaps very char-boiled!). This is a clever way to attempt to get around the FDA limits on the matter of Fecal Matter Transplants — it’s dead material!
Even if some metabolites survives, whether it has any results beyond placebo effects is very questionable. At best, the effect may last one or two days — hence you will need to keep reordering! An excellent business model!
The metabolites may cause effects, but the persistence of the effects is the key question. With appropriate living probiotics (or live FMT), sufficient bacteria takes up residence — not possible with killed bacteria.
“This suggests that it is the host response to probiotics, rather than microbial metabolism that facilitates the molecular changes in the brain and downstream behaviours.”
This is being run out of a Naturopath office with the three sole people that can “prescribe” appearing to be members of that same office. You must pay for a consult with them before you can order.
“Fecal Matter Transplants” and “Post-Biotics” are hot words in trade magazines. If you want to make money fast, you create a product wrapped in those words without needing any evidence that they work or are safe. It will be at least two years before the FDA will shut you down.
And not surprising, they are looking for investors and venture capitalists. To paraphrase John Paul Jones, “Give me Research or Give me Money”
P.S. I have emailed them asking for “Can you provide published clinical studies on the use of your ThaenaBiotic product? As well as details on the composition… which metabolites and chemicals are in it and the amount of each.” – I expect stonewalling or no answer back.
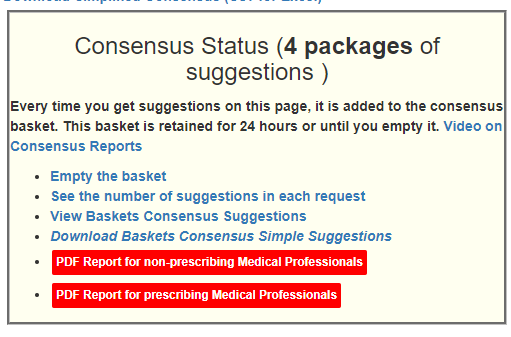
As a result of some readers asking for a PDF that they could shared with their medical professional I have created two reports and deployed the first versions today. The readers requested these features:
Simplify the suggestions into shorter list without extra data like Priority.
Provide some of the literature used to generate the suggestions
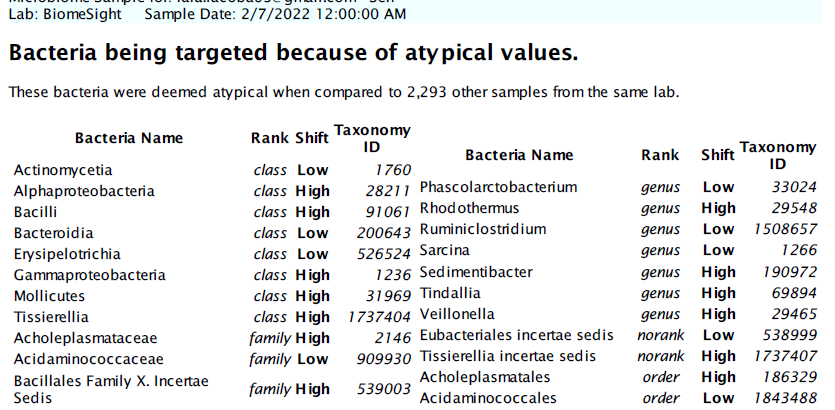
Provide the bacteria being targeted.
The reports are based on the consensus reports (so you can build them as you like).
For the automatic emailing of the PDF, we run “Just Give Me Suggestions” — which executes 4 different algorithms (Mean +/- 2 Standard Deviation, Box-Whiskers, Kaltoft-Moltrup and top/bottom 5%ile) and to obtain a consensus report. From the consensus report, we pick those that are at least 50% of the highest value to take, and below 50% of the lowest value to avoid. We then sort the items alphabetically for the lists.
The suggestions are from Microbiome Prescription and may disagree with suggestions from the lab used. To see how we get suggestions (tracing back to source studies), see this video. You will need to ask the lab how they do theirs — in some cases, it is opinion from a dietician.
Links are on various pages, for example, changing Microbiome tab.
First Page is an introduction to what the report is
Second Page is the bacteria being targeted, group by taxonomy rank
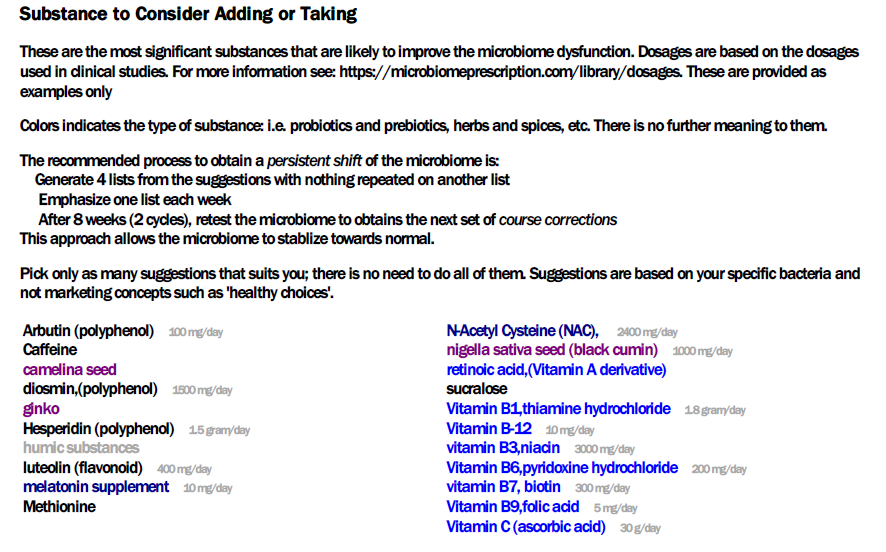
Third page are suggestions to take. Where dosages from clinical studies are available, they are shown
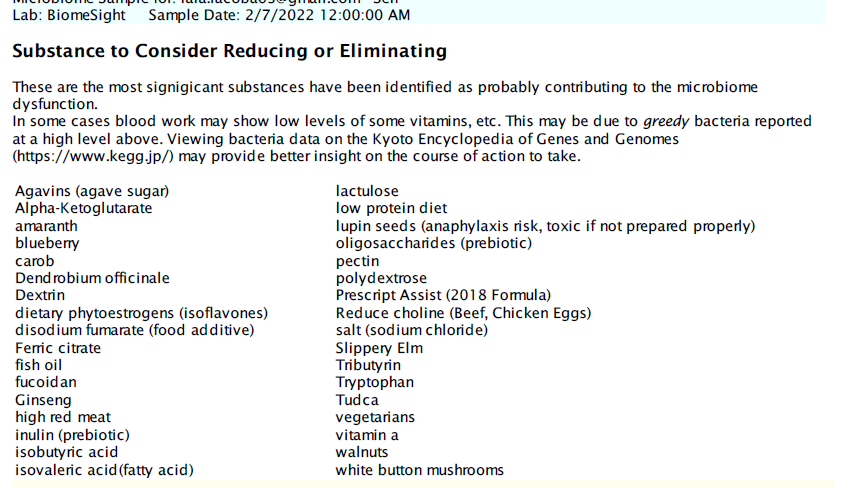
The next page are things to avoid
The last page are a partial listing of citations explicitly used. The newest studies are listed first to pre-emptively answer the question about how old the data being used is.
This is in Beta Testing Mode
Open for suggestions and improvements. Remember this is targeted for the typical medical professional with limited knowledge and understanding of the microbiome.


Recent Comments