In general, I avoid comparing opinions/suggestions from different microbiome resources. Like my earlier The taxonomy nightmare before Christmas… post; some resources may be sufficient/adequate for some people; for others it is not. My criteria for both tends to be simple:
More data, and more complete data, tends to better results
For the Microbiome it means that Shotgun Analysis where the data is uploadable, complete (often 5000+ items) and has percentile ranking is my preference
For the Analysis it means how many substances are considered (MP: 2065), are all interactions considered (MP: 2.5 million), how many different ways of doing analysis are offered (MP: lots).
Whatever you are using may be sufficient. If it is not, then read on.
This person asked for my help on Facebook explicitly and to properly answer, I need to do some comparison of analysis, interpretations and suggestions.
ME/CFS for 9 years. LC from vax injury 2.5 years.
I’ve been following the biomesight recommendations for 18 months and my gut has improved massively. I’ve just completed my third biomesight test and results are in. I have been experimenting with nicotine patches for 6 months now and my fatigue and pem symptoms have improved massively.
However, my most recent results are back and they have never been worse! Do you think Nicotine has a really negative impact on our guts? I can’t explain why everything is soo much worse.
For info: my gut doesn’t actually feel worse, but the results are terrible .
From a facebook User
Analysis
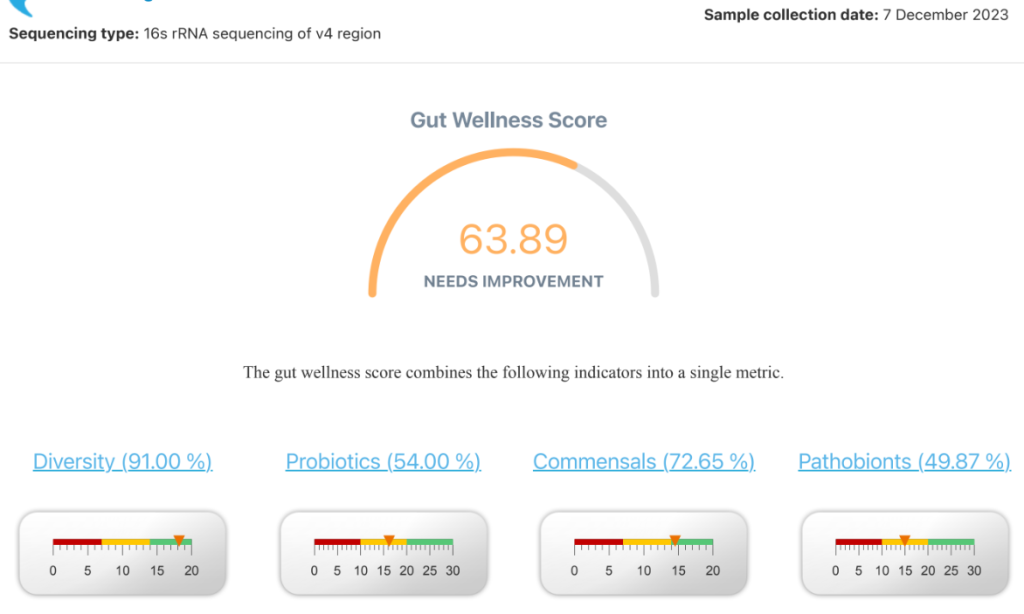
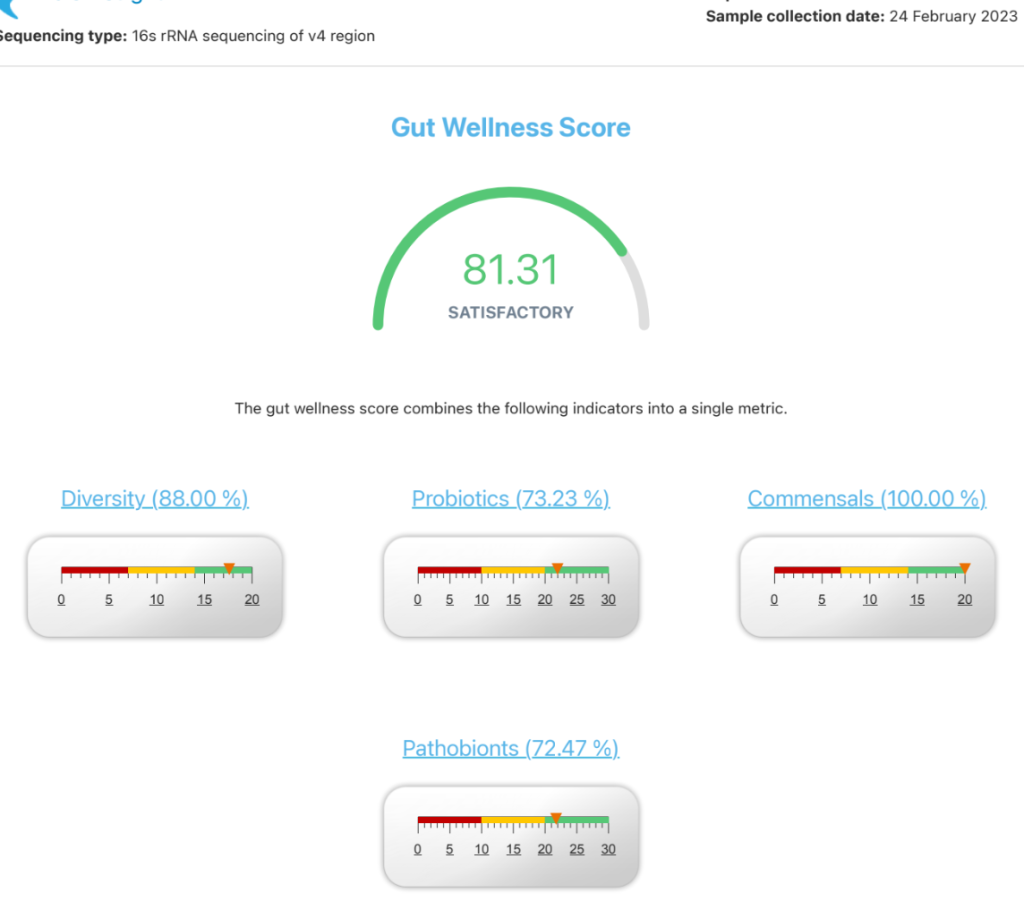
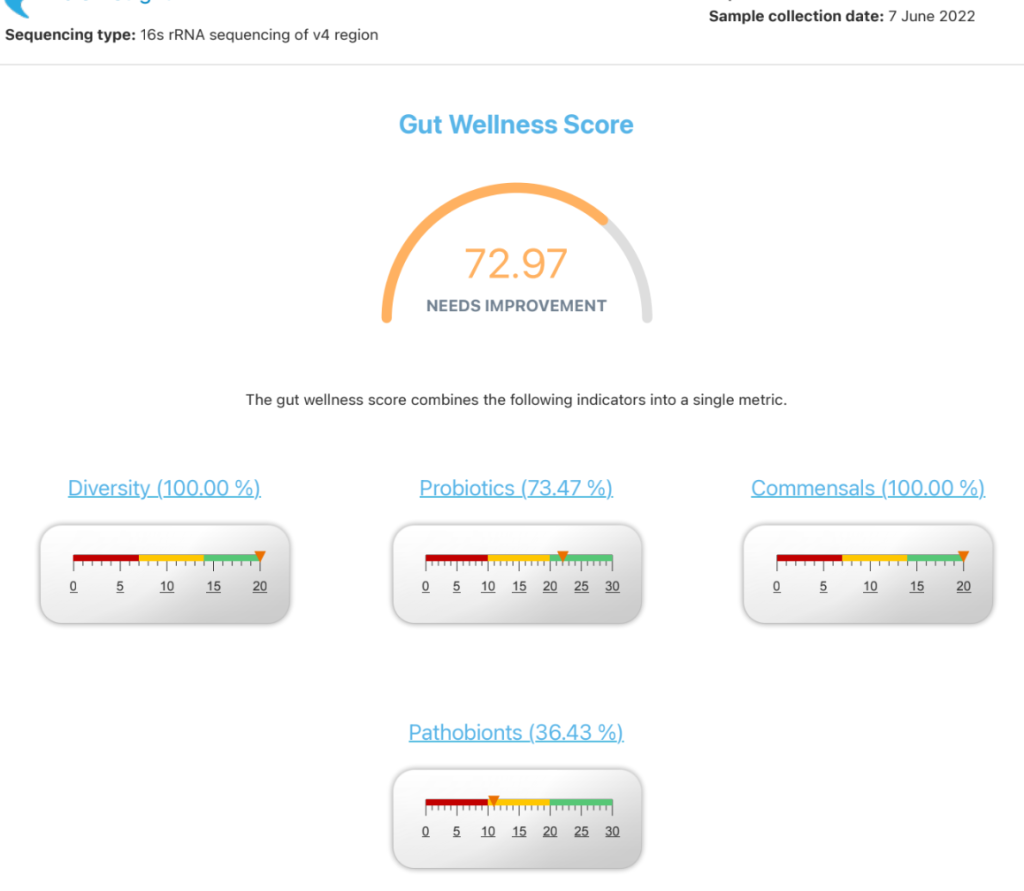
The reader is relying on BiomeSight evaluation. IMHO there is no single magical number or formula but many features that needs to be examined. Below is a table of the three test results meta-information. Remember that I am use the same measurement of bacteria data as Biomesight.
My general impressions is improvement is continuing despite Biomesight indicating not. Why?
Shannon, Simpson and Chao1 Diversity Percentileall moved towards 50%ile from extremes, a good sign.
Biomesight Diversity score started at 100% (ideal) and went downwards; completely opposite read to mine.
Outside Kaltoft-Møldrup are the ranges that I have the most confidence in, and they continued to drop
Criteria
12/7/2023
2/24/2203
6/7/2022
Lab Read Quality
4.4
7.3
10.3
Lab Quality Adjustment Percentage
79.7
89.7
100
Outside Range from JasonH
6
7
7
Outside Range from Medivere
13
17
17
Outside Range from Metagenomics
7
9
9
Outside Range from MyBioma
4
4
4
Outside Range from Nirvana/CosmosId
23
17
17
Outside Range from XenoGene
41
40
40
Outside Lab Range (+/- 1.96SD)
23
16
24
Outside Box-Plot-Whiskers
79
61
120
Outside Kaltoft-Møldrup
53
115
120
Bacteria Reported By Lab
677
709
866
Bacteria Over 90%ile
51
32
86
Bacteria Under 10%ile
56
263
244
Shannon Diversity Index
1.723
1.959
1.914
Simpson Diversity Index
0.068
0.046
0.026
Chao1 Index
13468
14912
20849
Shannon Diversity Percentile
64.4
91.8
87.9
Simpson Diversity Percentile
64.6
43.4
18.2
Chao1 Percentile
72.5
80.4
93.8
Lab: BiomeSight
Pathogens
37
31
37
Condition Est. Over 90%ile
0
1
4
Biomesight (BS) and Microbiome Prescription (MP) appear to be using different list of pathobionts
7 Dec 2023: MP reported 37, BS cites 49%
24 Feb 2023: MP reported 31, BS cites 72%
7 Jun 2022: MP reported 37, BS cites 36%
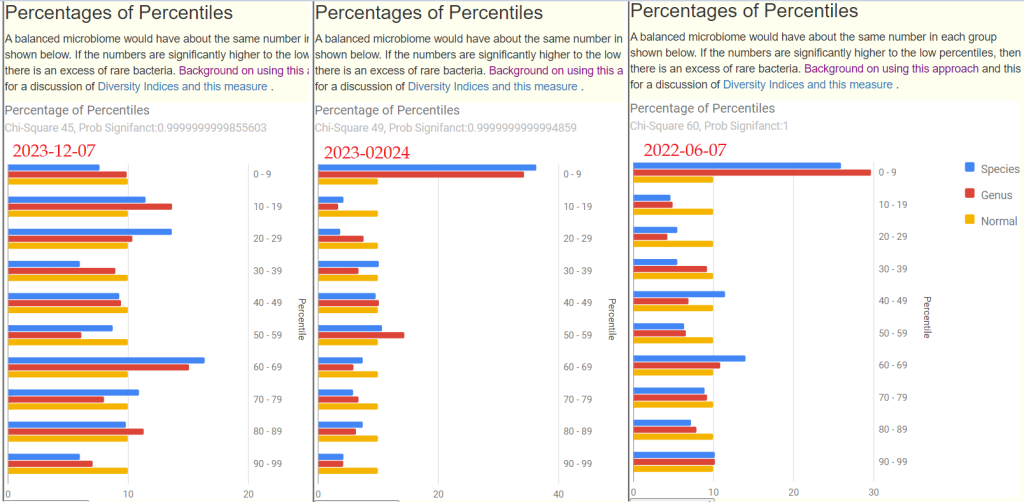
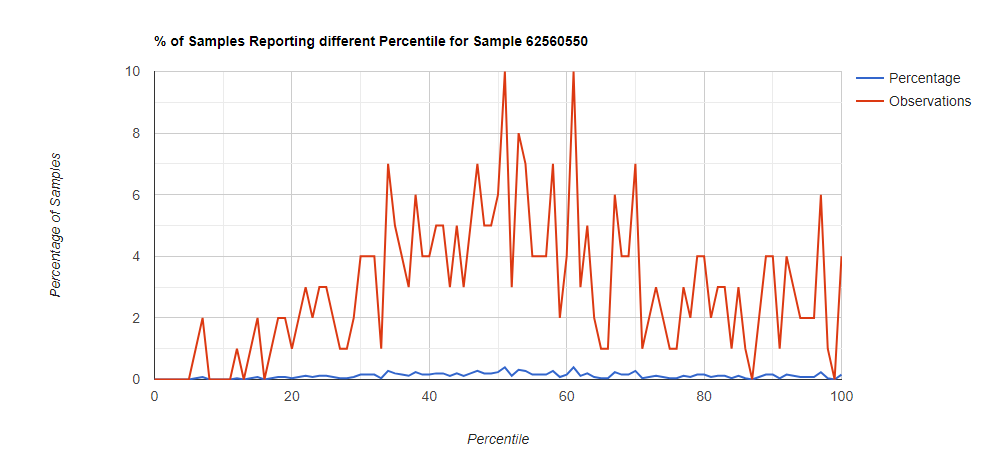
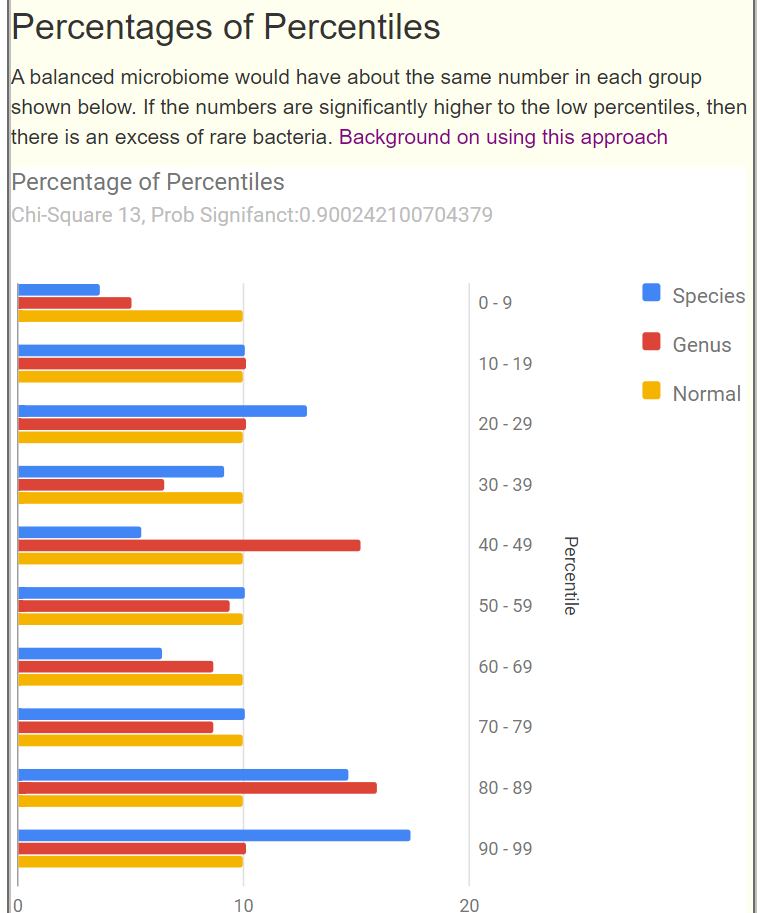
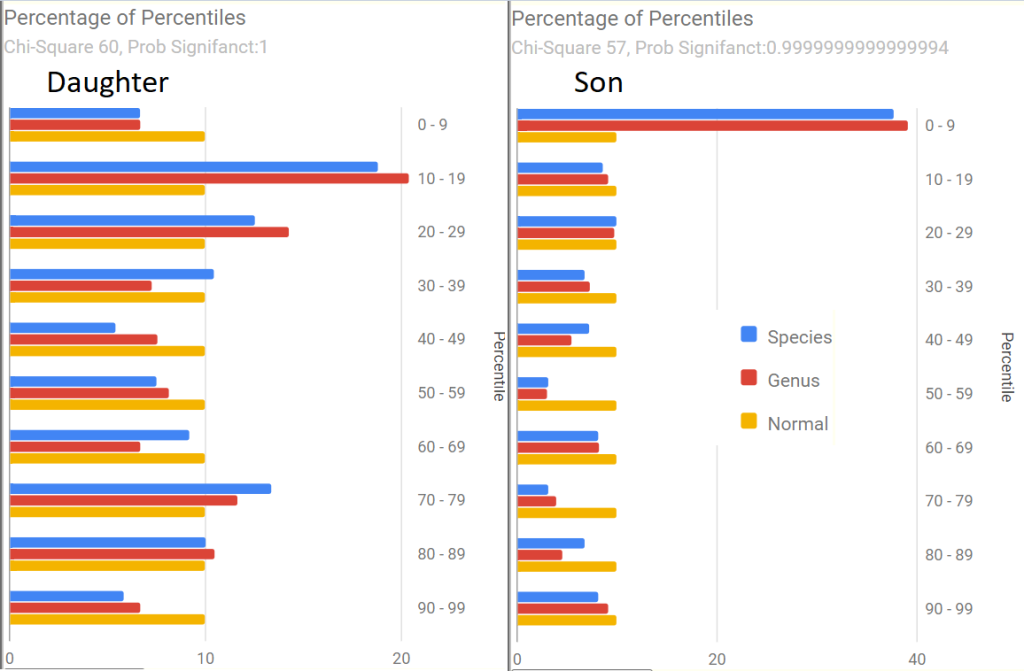
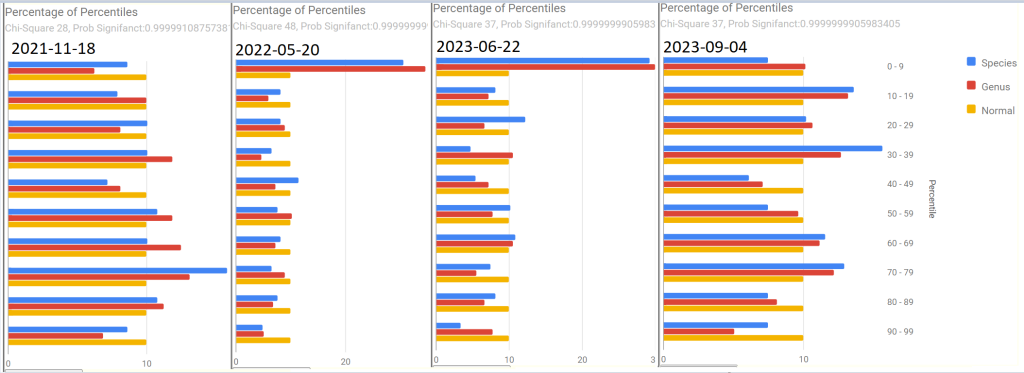
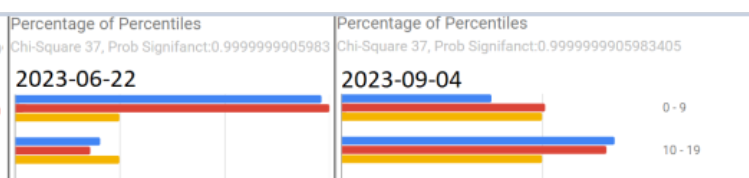
The Percentage of Percentiles
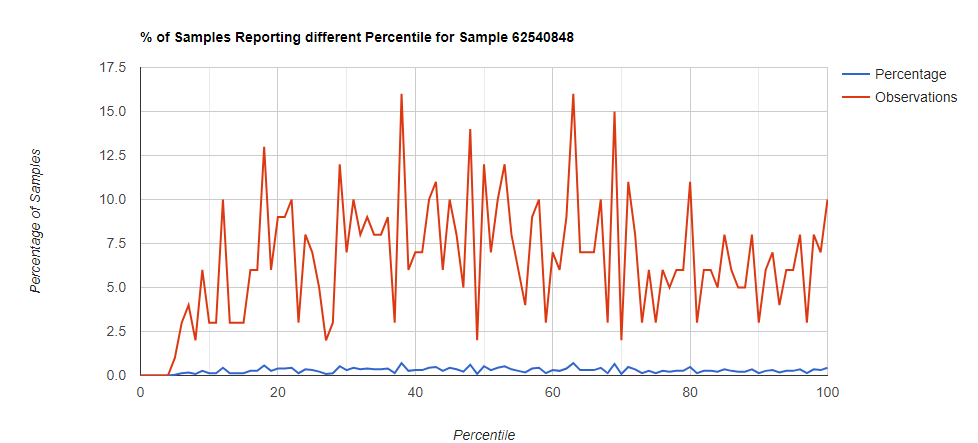
The charts are below — we see in the older samples that the 0-9%ile spike that is typical of ME/CFS has disappeared in the latest sample. My preferred single measure of gut health, Chi2 has moved from 60 to 49 to 45. Significant improvement.
Conclusion: Biomesight simple evaluation of overall health may be misleading because it is too simple an algorithm.
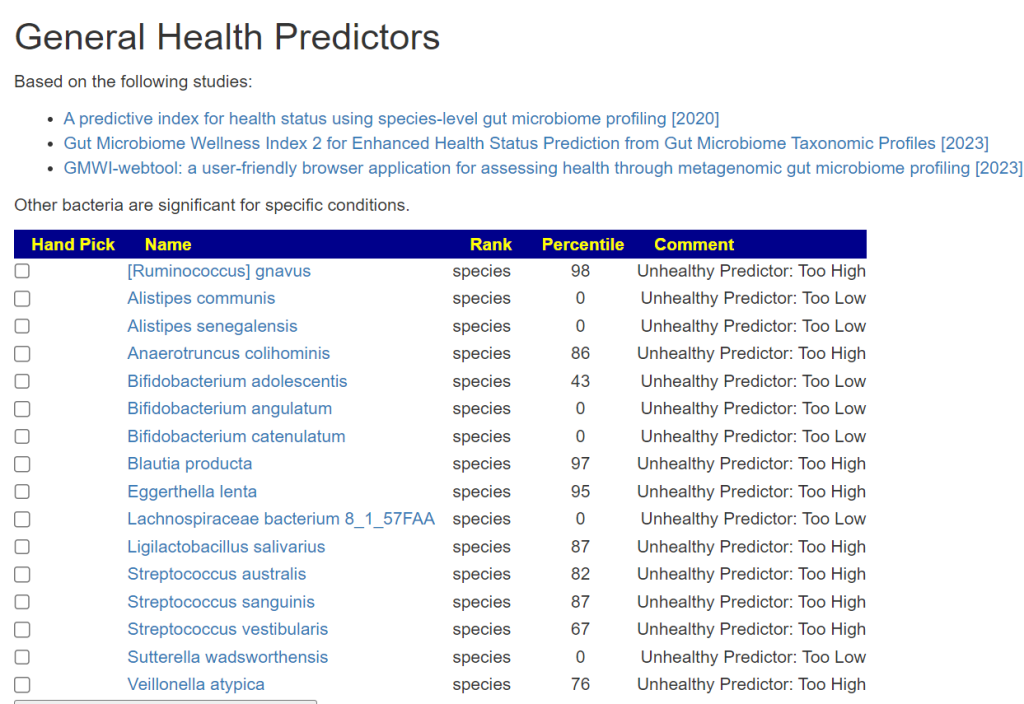
Health Analysis
General Health Predictors (based on various studies) No significant changes
Nicotine is one of the modifiers consider by Microbiome Prescription Expert systems.
2022-06-07: Nicotine patch was a low positive
2023-02-24: Nicotine patch was a positive, 5x higher than above
2023-12-07: Nicotine patch was a positive, less than above but 3x the first value.
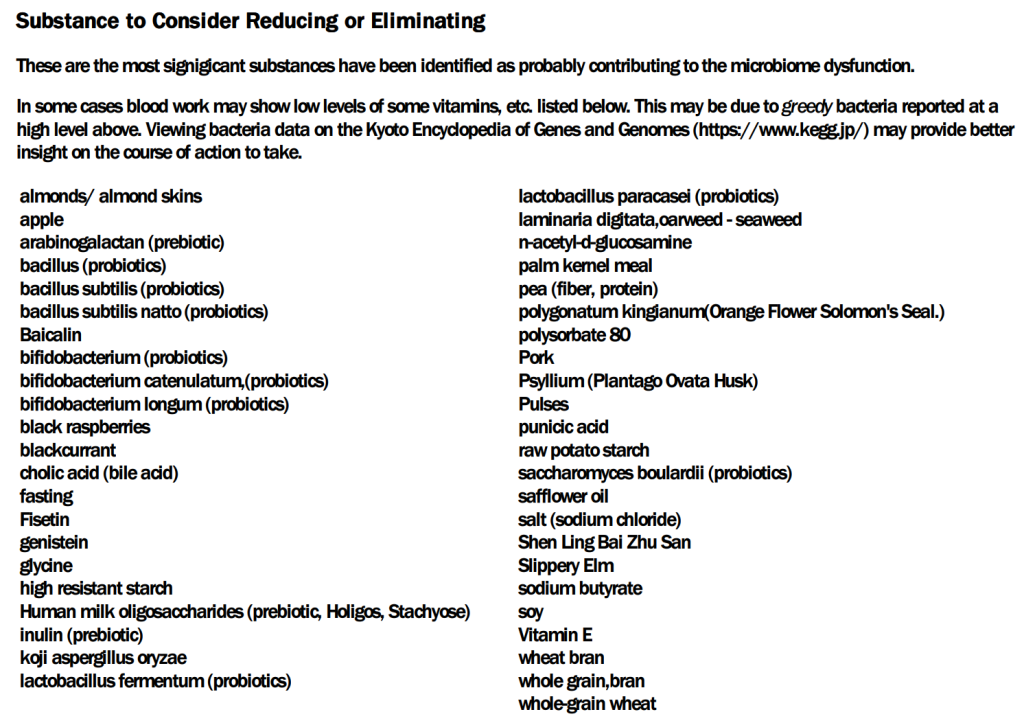
Suggestions Comparisons
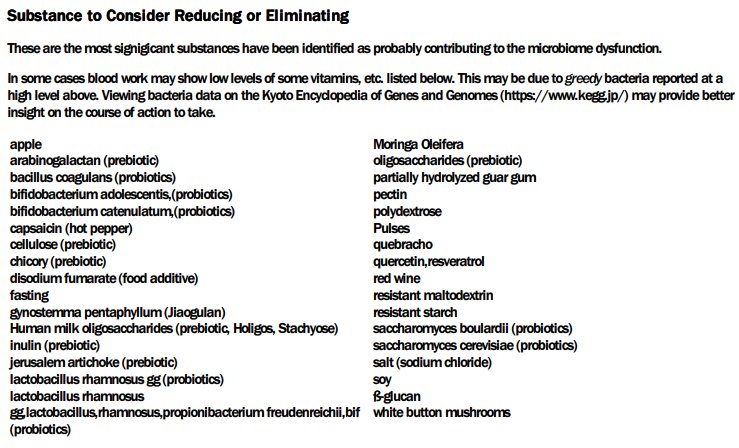
Biomesight just gives suggestions without any attempt to prioritize them. Looking at the suggestions from the latest sample(reader sent the PDF); we list them below. The highest Priority from Microbiome Prescription was 927 and lowest was -906.
Below are Biomesight suggestions followed by how Microbiome Prescription ranks them.
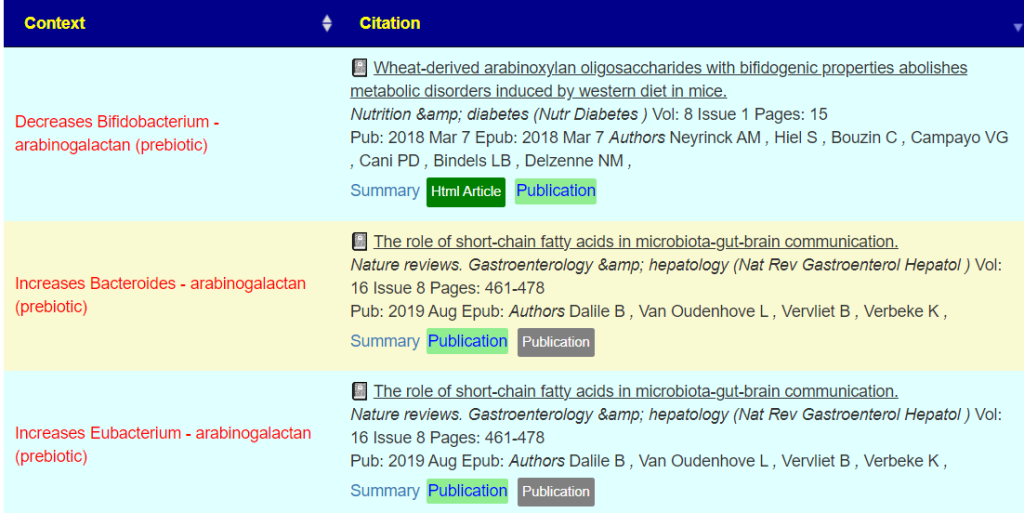
Prebiotics
Arabinogalactan: Massive Avoid: -906 (based on 331 interactions)
So we have a few agreements but a lot of disagreements. It may be just “the change of microbiome environment shock” with either sets of suggestions is causing improvement.
Microbiome Prescription does a holistic approach for suggestions. It looks at the known impact on every bacteria being targeted for a modifier and makes the full details available to review (Click on the ?). People have been double checking these citations. The decision on Arabinogalactan was based on considering 311 interactions, a few are shown below.
Another difference is that the bacteria selected is based on using 4 different algorithms to select what is of concern and then we do a Monte Carlo simulation on the suggestions.
My impression is that Biomesight considers one bacteria at a time and does not use that many studies to base a recommendation on. I do not know what extent BS consider the complexities of interactions. Biomesight would be the source of information to get better clarity on this.
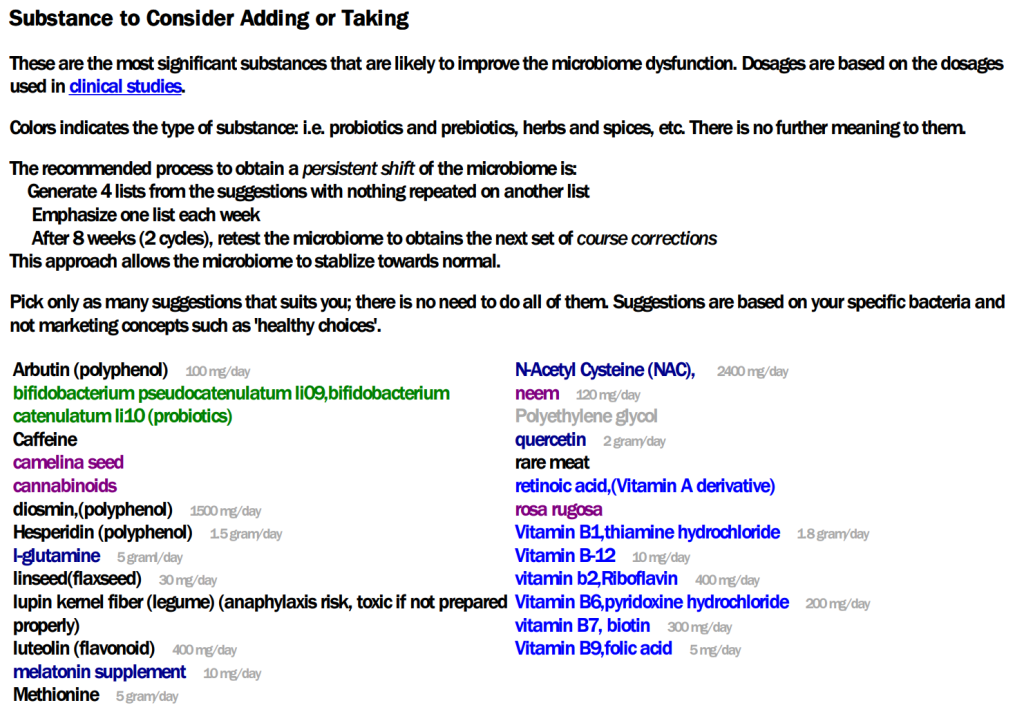
So what are Microbiome Prescription Top Suggestions
I have placed a ? besides those that are common suggestions
This person has ME/CFS and it is extremely well documented that B-Vitamins moderates those symptoms. Microbiome Prescription shouts out that they should be taken. Biomesight only cites one B-Vitamin (with no indication of importance). Some ME/CFS studies on the top suggested B-Vitamin ( Vitamin B1, thiamine ) suggested by Microbiome Prescription are shown below.
IMHO, there is no right answer. Go with Biomesight, Go with what a medical practitioner suggests. Go with whatever you see next in an influencer YouTube.
My best answer is above, it uses a massive amount of data to compute suggestions with a complete evidence trail for people to openly challenge. I have worked professionally as an information auditor and made sure auditability was build into the expert system. I have tuned the expert system to produce good results by doing cross-validation – i.e. 80-90% of suggestions for tested conditions are known to improve that condition from independent clinical studies. In this case, the top suggestions are in agreement with what has been known to help with his specific condition: ME/CFS. MP suggestions are not random shots in the dark but heavily data driven.
It is your choice — just don’t “mix and match” suggestions from different sources.
REMEMBER: Going Biomesight and transferring data to MicrobiomePrescription gives two analysis that you can compare and potentially ask the provider for the basis of their suggestions.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide information on rotations etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
For a while I have been using a variation of this concept for 16s samples that I have reviewed. The concept is very simple to a statistician:
Percentiles is converting data into a native uniform distribution. If you sample for 1000 boxes where each box has 100 balls numbered 1-100, then you expect the distribution of the balls samples to be uniform. It they are not, then something is definitely unfair.
Concept
With the microbiome things are a little more complex because a high in a single strain may push it species into high and thus the genus into high. We could do independent levels, for example species only or genus only. The problem is that the population size starts to drop and thus the sensitivity decreases as a result.
I happen to have a small collection of shotgun samples processed through CosmosID. Their report give percentile for most of what they measure. Getting accurate percentiles requires large sample sizes.
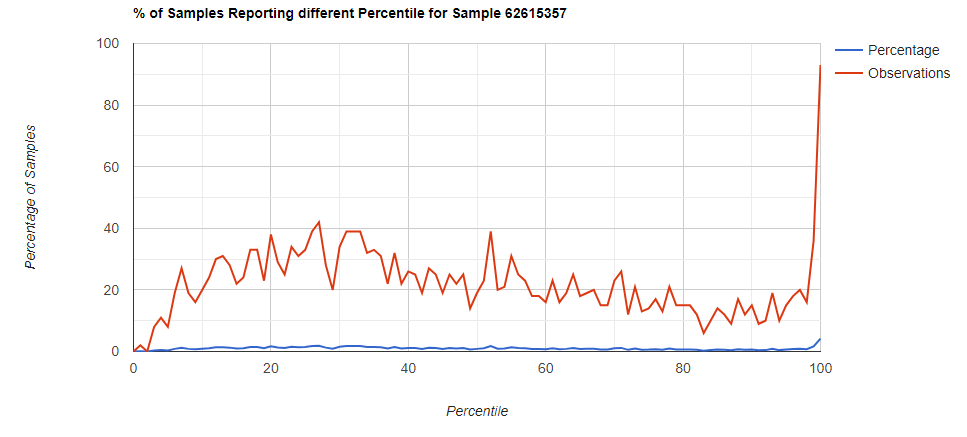
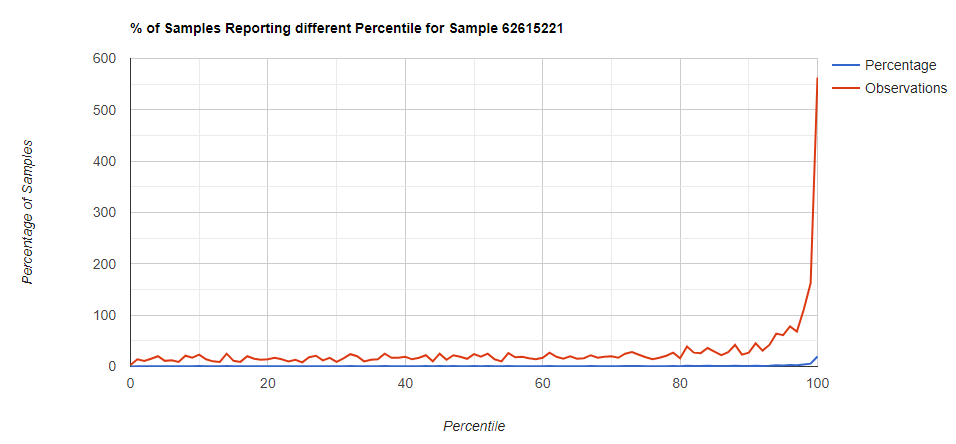
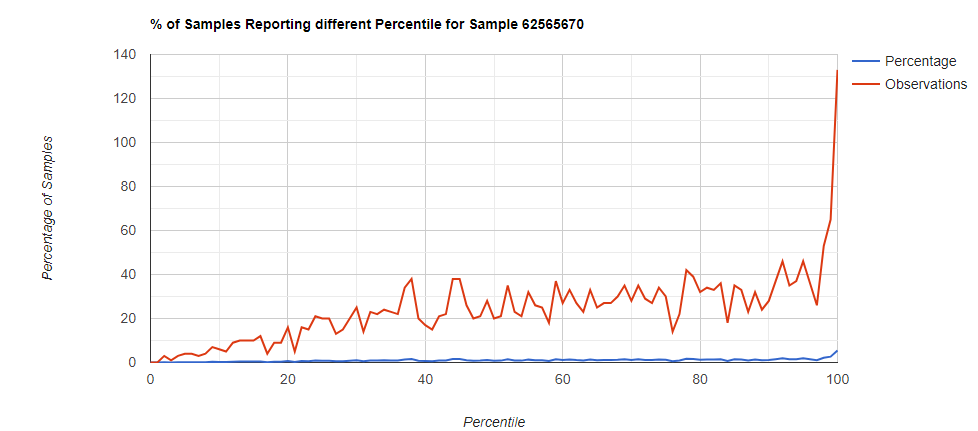
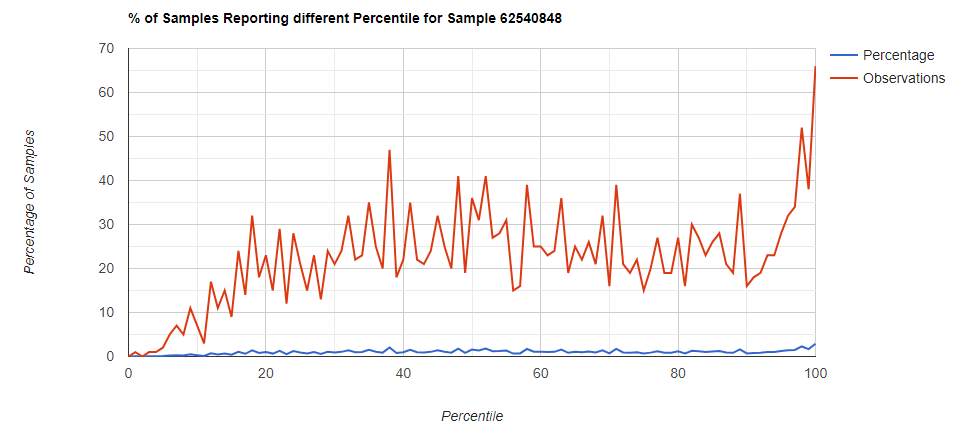
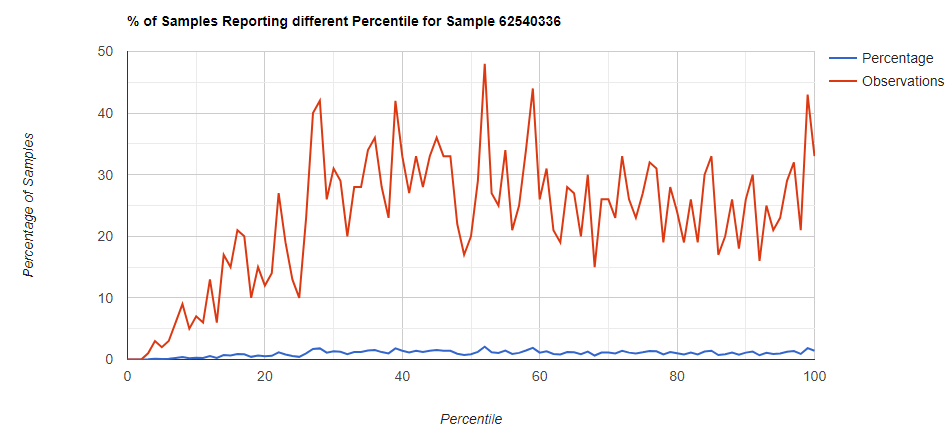
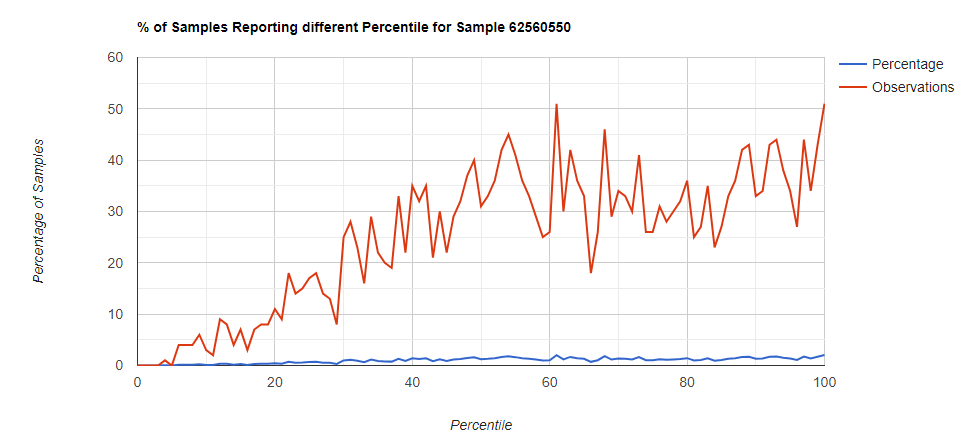
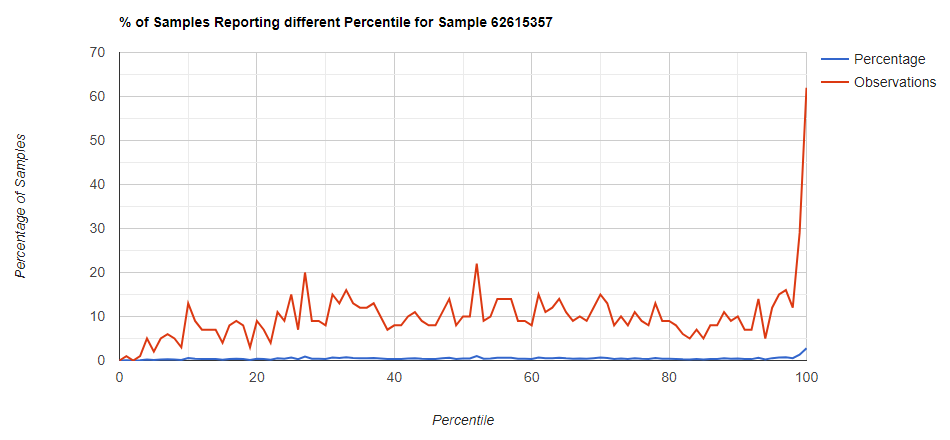
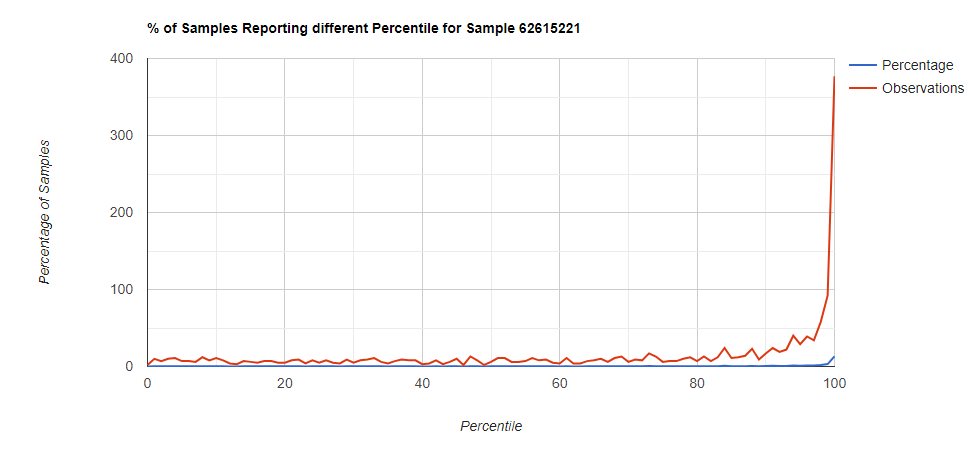
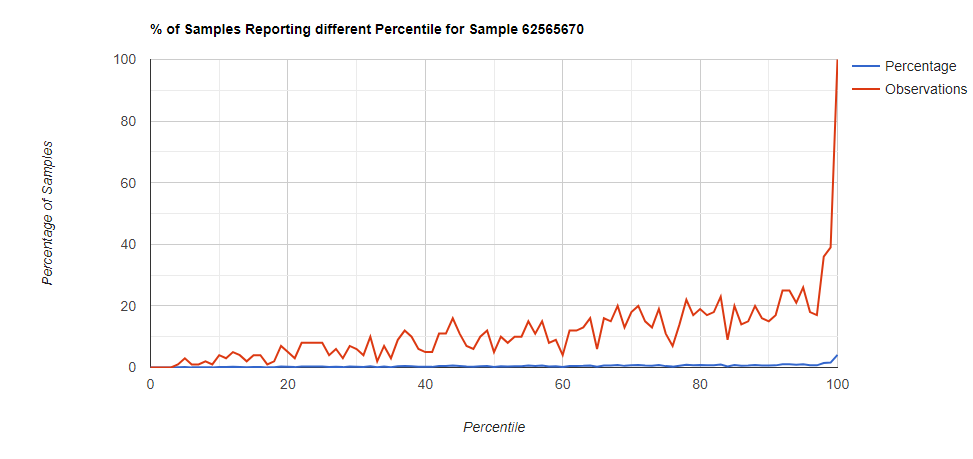
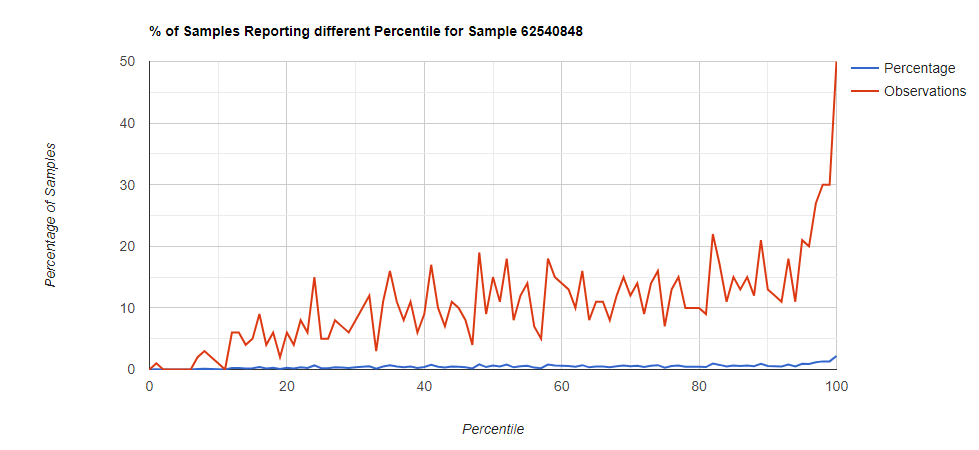
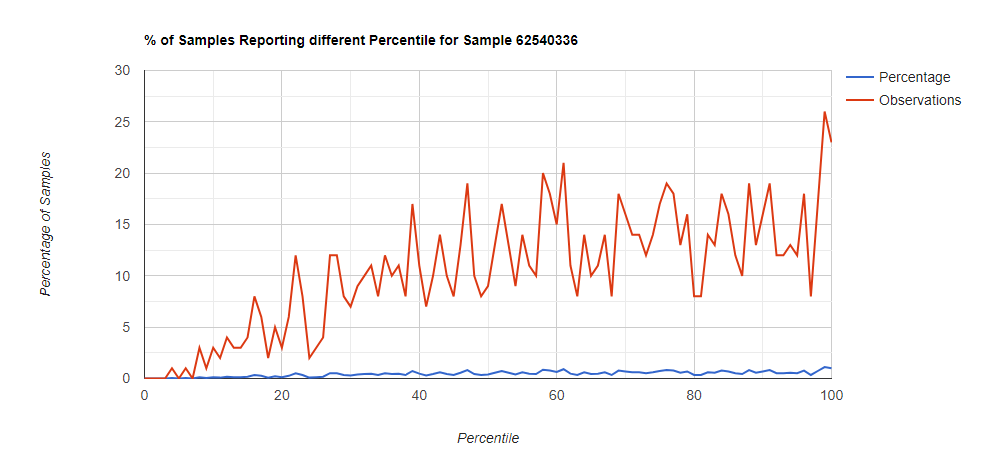
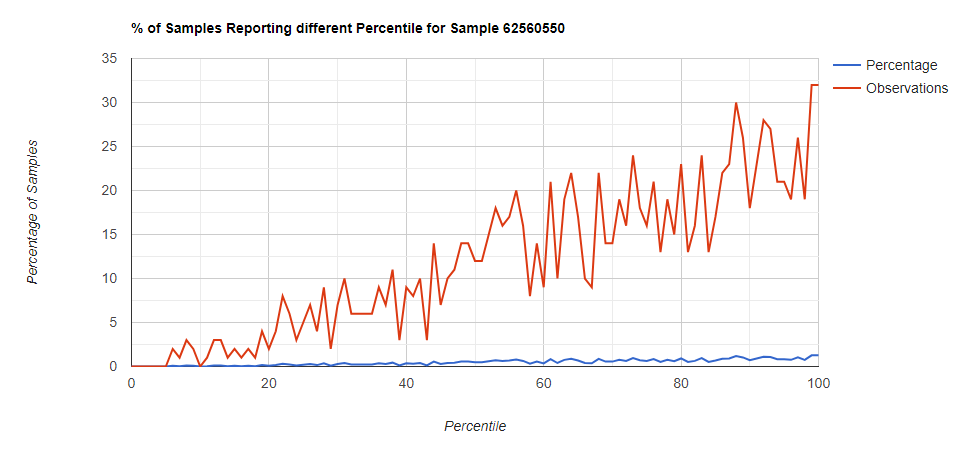
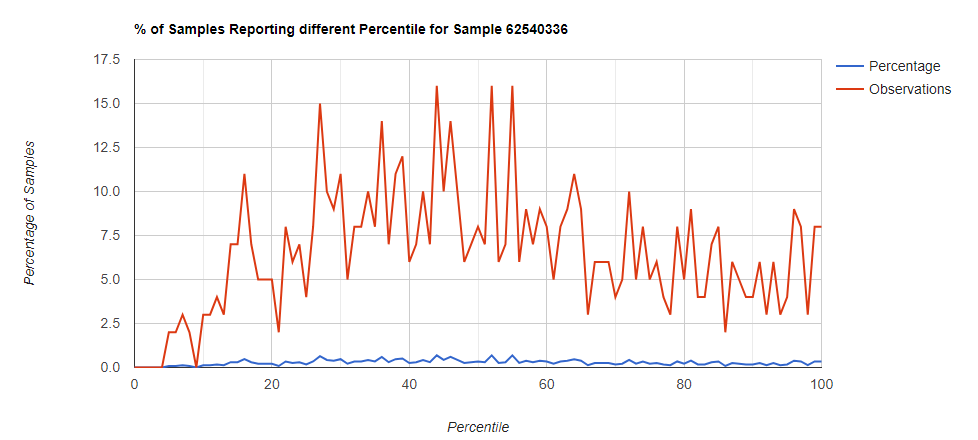
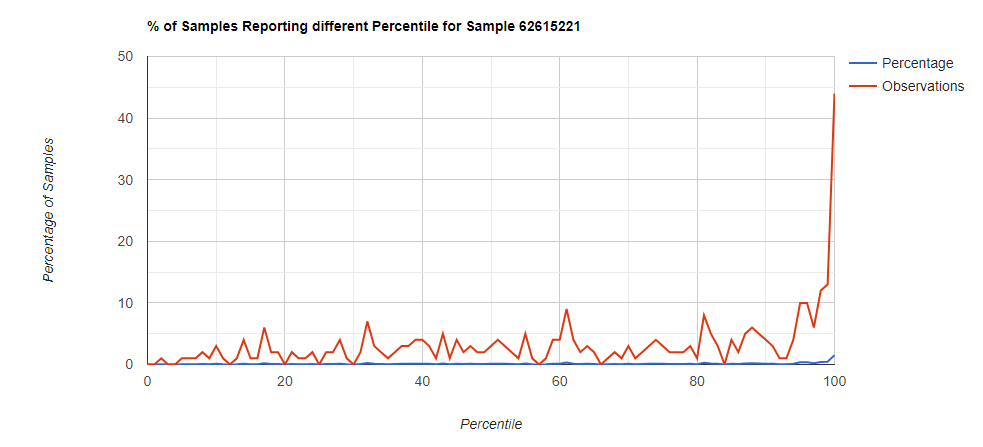
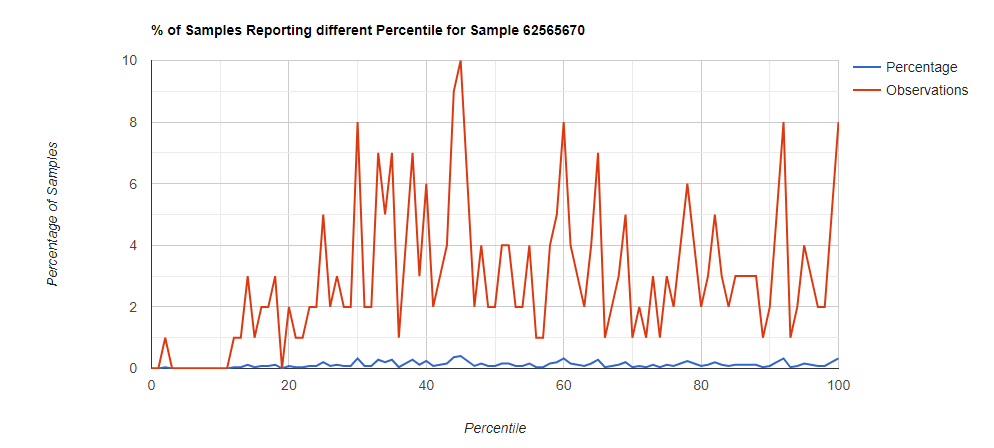
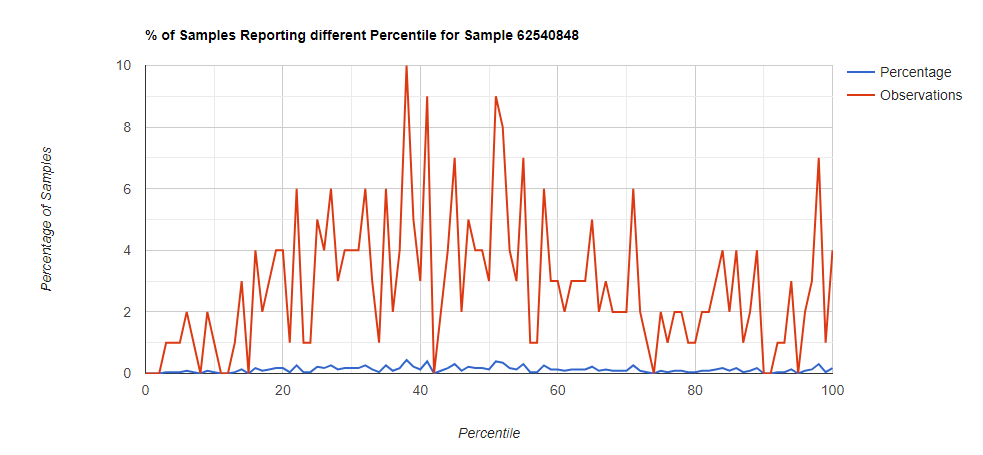
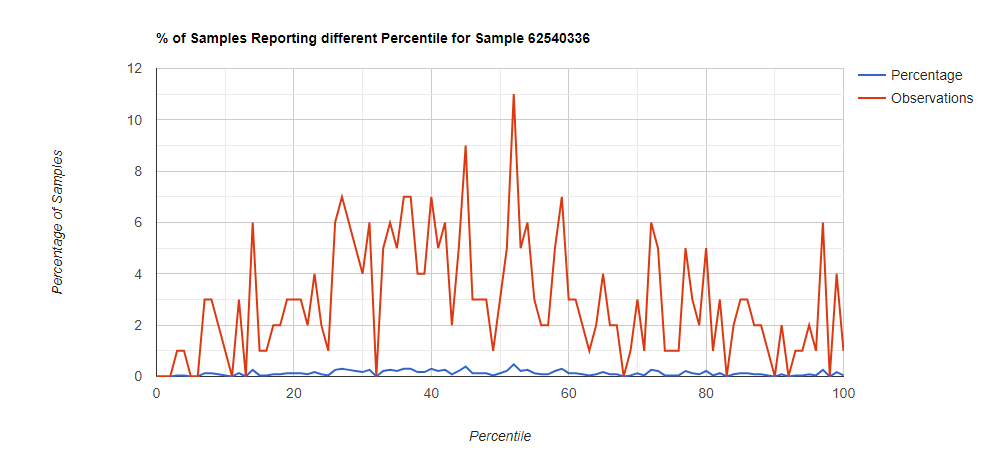
Below I have charted the results with single percentile ranges from reports that have between 2000 and 5000 different biological units reported. I have charted using different approach (the kitchen sink and then select taxological levels).
All of these samples are from people with health issues. Note that the numbers come from rounding so 100% is just 99.5 to 100 (and not 99.5 to 100.5) so the spikes at 100 is likely twice as high.
Kitchen Sink
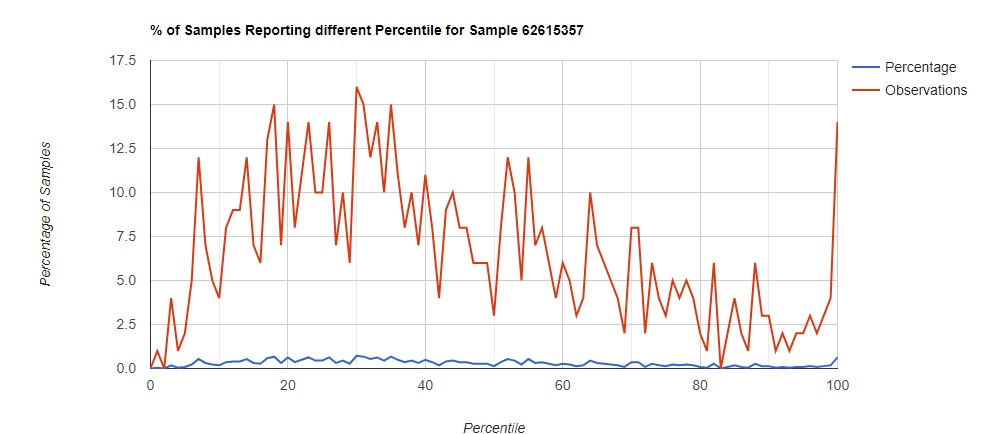
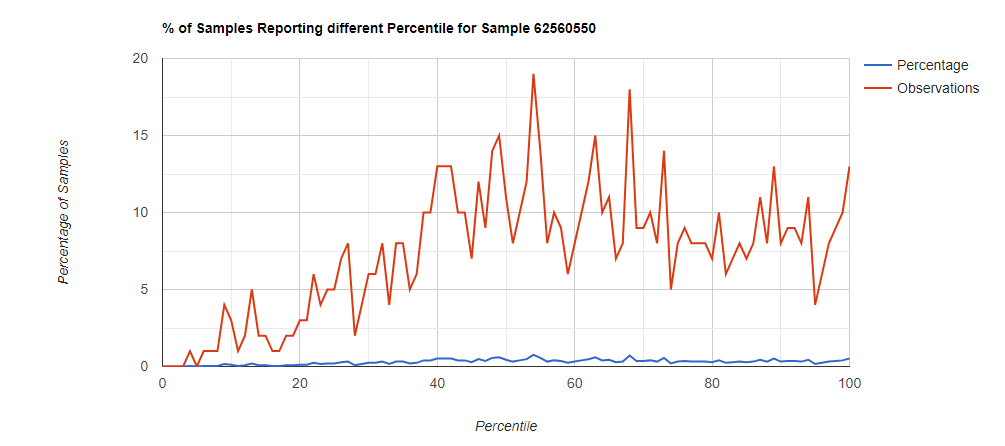
Filter to Species Only
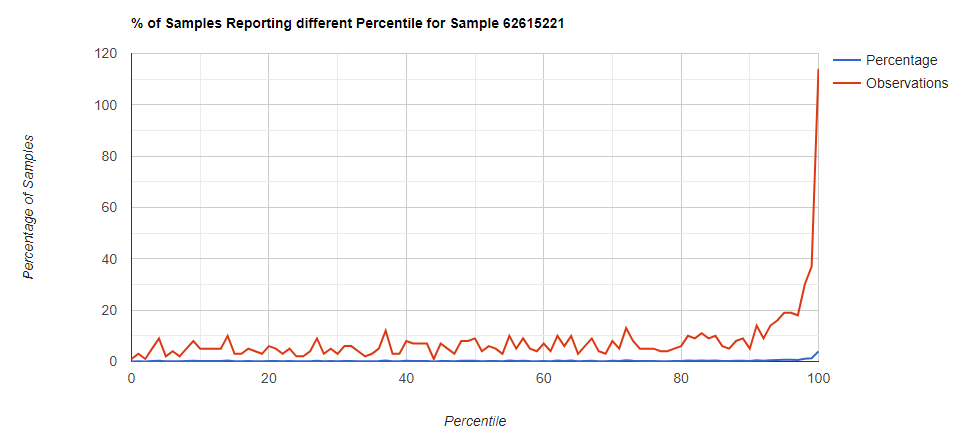
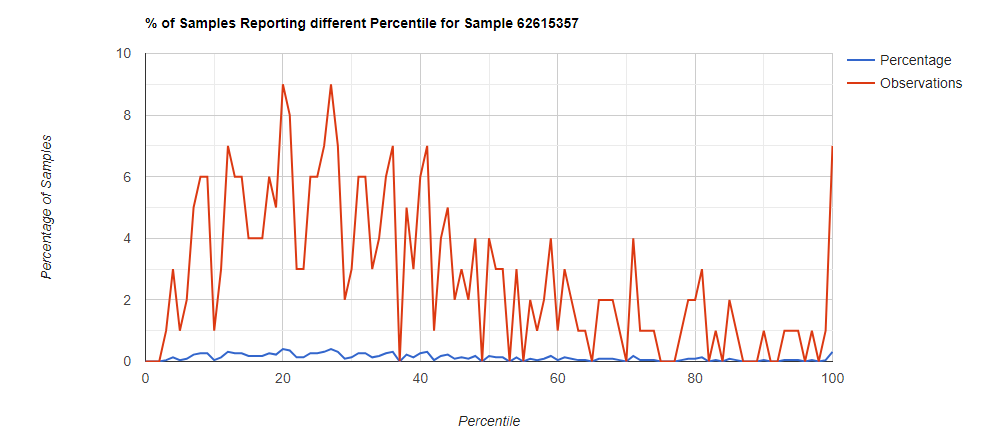
Genus Level
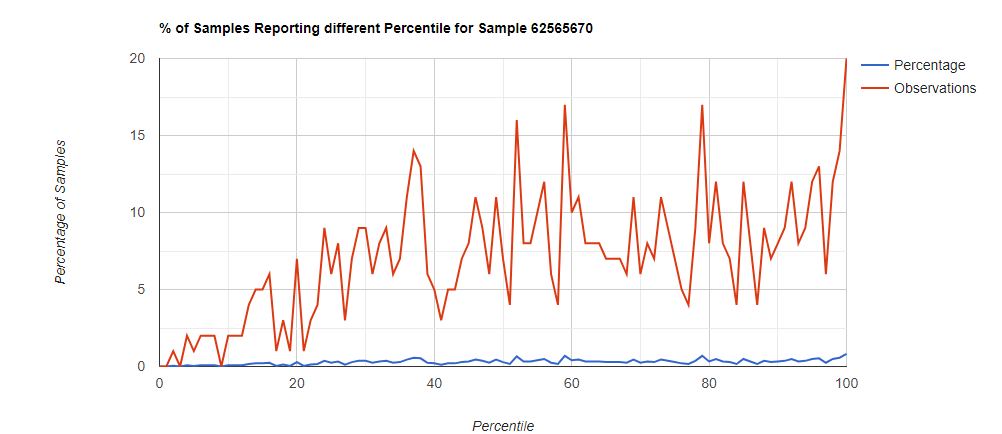
Family Level
Bottom Line
Comparing different levels can be informative, to illustrate, we have species below with good uniformity until we hit the high levels.
Looking at the genus level for the same sample, the pattern is very different.
In this case, we drilled down into these high species and got a predominance of Corynebacterium species that fell into our 100% range (99.5-100 percentiles).
Taxonomy Name
Abundance
Anaerococcus mediterraneensis
0.005611
Anaerococcus prevotii
0.006486
Bacteroides rodentium
0.001238
Corynebacteriaceae bacterium ‘ARUP UnID 227’
0.000437
Corynebacterium ammoniagenes
0.000586
Corynebacterium aurimucosum
0.1573
Corynebacterium callunae
0.00013
Corynebacterium camporealensis
0.002243
Corynebacterium casei
0.000726
Corynebacterium comes
0.000391
Corynebacterium diphtheriae
0.0755
Corynebacterium endometrii
0.001051
Corynebacterium flavescens
0.001684
Corynebacterium humireducens
0.00053
Corynebacterium imitans
0.001024
Corynebacterium jeikeium
0.01813
Corynebacterium lactis
0.000437
Corynebacterium liangguodongii
0.000558
Corynebacterium minutissimum
0.03511
Corynebacterium phocae
0.000865
Corynebacterium pseudotuberculosis
0.000233
Corynebacterium renale
0.000493
Corynebacterium resistens
0.001182
Corynebacterium riegelii
0.001321
Corynebacterium segmentosum
0.007016
Corynebacterium simulans
0.3615
Corynebacterium singulare
0.01858
Corynebacterium sp. NML 98-0116
0.001024
Corynebacterium stationis
0.000577
Corynebacterium striatum
0.04709
Corynebacterium timonense
0.001321
Corynebacterium urealyticum
0.00107
Corynebacterium uterequi
0.000642
Corynebacterium yudongzhengii
0.000689
Cutibacterium acnes
0.002298
Dehalococcoides mccartyi
0.006123
Dermabacter jinjuensis
0.01404
Dermabacter vaginalis
0.001265
Fastidiosipila sanguinis
0.003536
Finegoldia magna
0.06368
Helcococcus kunzii
0.00014
Homo sapiens
1.985
Lawsonella clevelandensis
0.003154
Mycobacterium gallinarum
0.000261
Mycobacterium sp. DL592
0.00013
Mycobacterium sp. ELW1
0.001107
Mycobacterium sp. EPa45
0.002298
Mycobacterium sp. PYR15
0.008328
Mycolicibacterium aichiense
0.000223
Negativicoccus massiliensis
0.001935
Peptoniphilus harei
0.04272
Peptoniphilus sp. ING2-D1G
0.000893
Porphyromonas asaccharolytica
0.06443
Porphyromonas bennonis
0.000521
Propionibacterium freudenreichii
0.000465
Schaalia radingae
0.001089
Streptococcus pyogenes
0.00241
Streptococcus sp. NCTC 11567
0.000149
Sutterella stercoricanis
0.000149
Tessaracoccus timonensis
0.00094
uncultured Chroococcidiopsis sp.
0.000242
uncultured Rhizobium sp.
0.000772
We could also produce single value statistical measures — for example Chi2. We have an a priori expected value of 1% in each bucket.
IMHO, percentages of percentiles is likely more effective in evaluating an individual person’s gut microbiome. It seems to be able to separate the noise from what is significant, for example Corynebacterium cited above where the cause is a proliferation of species and not dominance of one species.
In 1983 or 1984 I suffered from EBV (mononucleosis)
In 1984 or 1985 – I had appendix removed
In 1991 I had a resurgence of fatigue like EBV reactivation, plus apparition of anxiety
In 2004, I was bitten by a tick, I thought at the time that it was a spider. Few weeks after the bite, I had flu symptoms who last very long, like months, and some intermittent fever. When I talked about my intermittent fever to doctors, they where looking at me as if I was crazy. Later I learnt that Lyme was in the area.
Between 2004 and 2007, lots of weird symptoms appeared. Doctors were saying it was in my head
In 2007, I had an urinary tract infection. I took Cipro, and all my little weird symptoms that I had notice for couple of years, have worsened. I started to have mood change, internal tremors.
Between 2007 and 2011 -I’ve met 3 neurologists, they said I maybe have multiple sclerosis, even if my MRI at this time were clear.
In 2015, another urinary tract infection, Cipro again, symptoms once again worsened.
In 2016, I received Multiple sclerosis, (MS), diagnosis.
I saw a naturopath. She run urinary test to see organic acid. And she build a protocol. I follow this protocol for 3 months, with no change.
I went to see a LLMD in USA for a year with some improvement.
Between 2007 and 2011 -I’ve met 3 neurologists, they said I maybe have multiple sclerosis, even if my MRI at this time were clear. They said that I have to wait for another crisis to confirm. But they gave me
I now have dysautomia, probably MCAS and SIBO. I also feel sick in transports. I do have intolerance to heat and cold. I have had big constipation problems for years.
I started to take Mutaflor[E.Coli Nissle 1917] for constipation. It’s helping.
I also started Akkermansia about 1 month ago.
B1 (1000mg/day)
We have two test results available: Biomesight and Genova test.
Analysis
The Percentage of Percentiles showed no statistically significant pattern with significance at 0.90 (we look for above .99) to be concerned.
Looking at the Health Analysis,
Bacteroides/Clostridium Ratio is very high (97%ile_
Anti inflammatory Bacteria Score is high (94%ile)
Butyrate is low (1.2%ile)
D-Lactic Acid is low [GOOD THING, high levels often are seen with brain fog and cognitive issues)
Dopamine, Serotonin are both high (97%ile) – may account for mood issues
Hydrogen, Hydrogen sulfide (H2S), Methane are all low with Methane being the highest (46%ile), so traditional SIBO is unlikely.
Potential Medical Conditions Detected
The following were flagged in agreement with her history:
ME/CFS without IBS
Fibromyalgia
Mood Disorders
COVID-19
And last, Intelligence at 91%ile which agrees with details from emails.
And for Bacteria deemed Unhealthy we have quite a few.
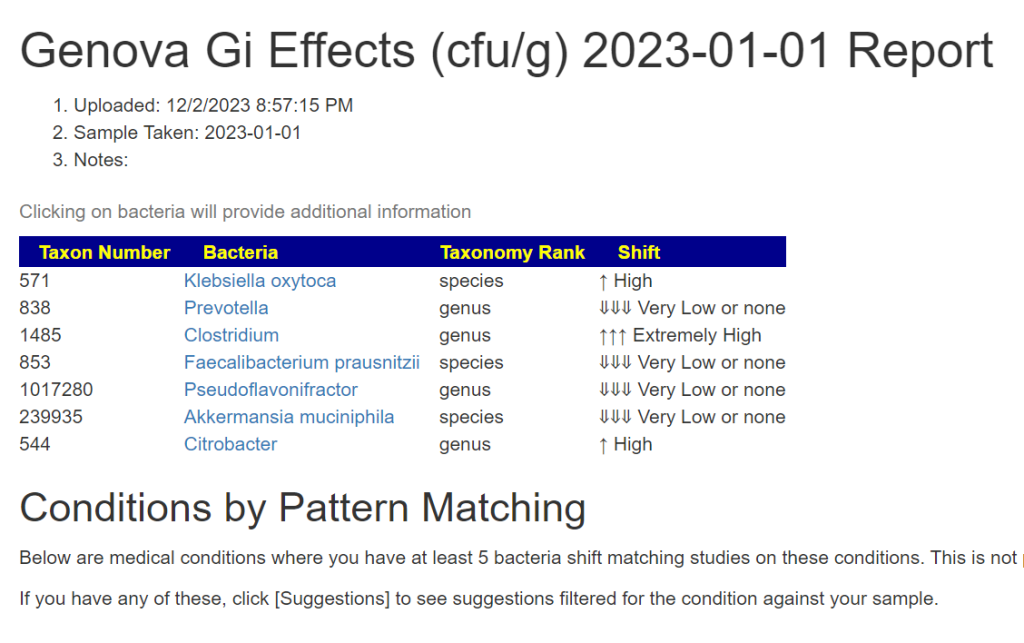
I looked at her GI Effects test with the new Conditions matching (See this post) and nothing was identified by pattern matching.
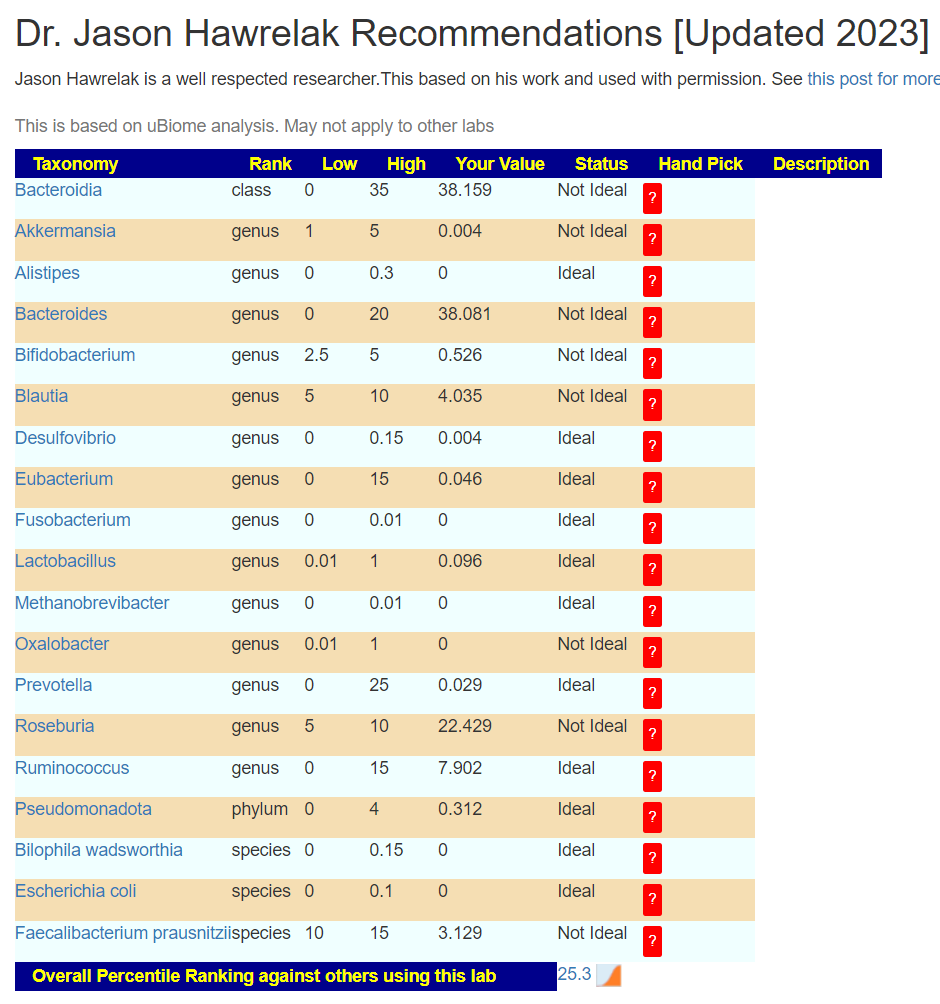
Using Jason’s criteria, we see that there is a long way from health improvement.
Going Forward
With a diagnosis of Multiple sclerosis, I was curious to see the degree of pattern matching to published studies. She is at the 88%ile (i.e. her pattern the reported pattern better then 9 out of 10 people).
While it appears that Lyme played a role, the literature is very sparse on Lyme and she has no matches
Strategy
I will do the usual “Just give me suggestions’ (4 ways of picking bacteria) and then add in:
Multiple Sclerosis
Mood Disorders
This gives us 6 algorithms to build suggestions from. To which we add the new one to hand pick and then process. So we have 7 algorithms being used.
Review of Suggestions
My first curiosity is where does Cipro (Ciprofloxacin) set in suggestions. It is at a positive 275 our of 494. The top antibiotic is amoxicillin which is used for both ME/CFS and Lyme disease.
“use of penicillins(includes amoxicillin) in the 3 years before the index date decreased the risk of developing a first attack of multiple sclerosis (odds ratio = 0.5, 95% confidence interval: 0.3, 0.9 for those who used penicillins for ≥15 days compared with no use).”
For Cipro, I found no equivalent studies and some social media claiming that Cipro triggered MS in themselves.
No probiotic made it above the threshold except a particular mixture: bifidobacterium pseudocatenulatum li09,bifidobacterium catenulatum li10 (probiotics). I currently know of no retail source for this mixture (but can see a lot of studies). Neither can I locate any retail products with any form of bifidobacterium pseudocatenulatum or bifidobacterium catenulatum.
Questions and Answers
Q: In my history, you don’t seem to take into account the positive tests for borrelia and babesia, but only the diagnosis of multiple sclerosis. Am I mistaken? And is it because there are few studies on Lyme disease in relation to the microbiota?
Correct. I just double checked PubMed and found many articles on the microbiome of the ticks, but nothing useful for a human microbiome after being bitten. I have data on Chronic Lyme, there is not much. One example study if A Distinct Microbiome Signature in Posttreatment Lyme Disease Patients [2020]
Q: There is mention of human milk but nothing about dairy. I’m wondering if goat cheese is ok. I consume goat cheese from time to time and wondered if it’s good or bad.
Human milk contains different sugars than goat or sheep or cow or camel or… I have data on goat and cow. Most studies have been done on using them for yogurts which alters their composition.
Looking at the details (see YouTube video), all dairy are negative (not greatly often, but consistently negative for different dairy products), so reduce or eliminate.
Q: Does acacia fiber is consider oligofructose-enriched inulin ? I’m a bit lost. I bought acacia and wonder if it’s ok.
Acacia fiber (a.k.a. gum) is different. There is a study comparing them, PREBIOTIC EFFECTS OF INULIN AND ACACIA GUM [2015]. Acacia fiber was not in the list for to take or to avoid, so no known harm nor benefit (apart from the usual impact on the pocket book)
Q: In the recommendations, it’s said to avoid whole grain wheat. But does it include einkorn and buckwheat ?
No, buckwheat is not wheat, it is a seed (just like peanut is not a nut) — English can be very misleading at time!!! While it is true that Einkorn is the most primitive form of wheat on Earth, modern wheat (which is what the clinical studies used) is sufficiently different in content. “Einkorn kernels have higher protein, antioxidant (carotenoids and tocols), fructans and monounsaturated fatty acids content” [2013]. Many of those changes will cause a different effect on the microbiome. These are slight negative (see video), I would not be concerned about this.
Q: Alan McDonnald’s work shows that all the patients he tested with a diagnosis of multiple sclerosis were positive for at least one strain of borrelia, in addition to having their EBV reactivated. This is generally the case with Lyme. And since I’m treating Lyme, I have a lot of symptoms who alleviate.
Unfortunately, 16s tests do badly with detecting that bacteria. Shotgun tests are 10 to 40x better at detecting this bacteria. Some level may be present in 30% if the population. See this page
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide information on rotations etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
This post originated from a dialog with a Ph.D. in Molecular Genetics that I often discuss many aspects of microbiome analysis with.
The root of the problem is how many “Reads” from a 16s sample do you deem to be threshold for reliability. A “Read”, “num_hits” or “Count” is the number of matches to specific pattern found in the sample that matches a library. These are “best efforts” identification. Not always correct.
To this end, we processed the biggest collection of samples of one lab with different Read Levels to see what happens. The higher accuracy required to be included that you use, the higher the values.
obs
mean
stddev
median
boxplotlow
boxplothigh
tax_name
rank
Reads
471
386.5
5301.7
30
10
70
Neisseria
genus
1
242
733.6
7387.0
50
10
110
Neisseria
genus
2
136
1275.8
9835.5
70
30
210
Neisseria
genus
3
95
1800.3
11747.6
80
20
300
Neisseria
genus
4
68
2491.2
13853.4
120
0
360
Neisseria
genus
5
55
3059.5
15375.2
160
0
380
Neisseria
genus
6
41
4071.7
17748.5
200
0
500
Neisseria
genus
7
30
5517.0
20650.4
240
0
778
Neisseria
genus
8
21
7825.7
24488.4
350
50
1532
Neisseria
genus
9
Two labs may report different reference ranges for the simple reason that one requires at least 2 reads and the other lab 4 reads. This decision is often well hidden from the consumer. If the reference ranges are based on 4 reads and you apply them to 1 read samples then you will get a lot of false too high and too lows.
For the above example bacteria a 1 read reference range would have 386 being the average, while a 4 read reference range would have the average being 1800. So, a sample with 800 from 2 reads would be 2x the average for one reference range and and 1/2 the average for the other reference range.
This is part of the complexity of doing microbiome analysis and understanding the mechanism involved. Mechanisms that are often not understood by the labs and kit providers.
This is a follow up the earlier blog post: Son and Daughter with Autism Analysis from a year ago. There has been a lot of changes of the site and revisions of algorithms.
Comparing Siblings
We know from studies that members in the same family often share about 27% of the same strains. Unfortunately with 16s tests (Biomesight, Ombre), we do not get strain information just species information.
Using the new refactor citizen science symptoms (see New Special Studies on Symptoms ), we are presently surprised! We have many forecast symptoms being the same which supports the observation cited above of share taxa, likely at the strain level.
It does hint that less time with each other and a lot more time with other (ideally normal) children may have benefits to the microbiome. Some of the changes may be connected to gender:
About twice as many women as men experience depression [Mayo]
Increased inflammation is seen in the periphery in both depression and fatigue. [2019] which agrees with the daughter having a lower Anti inflammatory Bacteria Score
Measure
Daughter
Son
Anti inflammatory Bacteria Score
25.6%ile
89%ile
Buytrate Bacteria Score
95.9%ile
78%ile
Histamine Producers
21.8%ile
15.3%
Autism From PubMed
53/97 (1%ile) Prior: 54/97 (1%ile)
73/97 (11%ile) Prior: 53/97 (1%ile)
Forecast Symptoms
Official Diagnosis: Depression 28 % match on 7 taxa
DePaul University Fatigue Questionnaire : Blurred Vision 25 % match on 8 taxa
Neurological-Sleep: Inability for deep (delta) sleep 23 % match on 13 taxa
Age: 10-20 17 % match on 23 taxa
DePaul University Fatigue Questionnaire : Forgetting what you are trying to say 16 % match on 31 taxa
Next looking at Percentages of Percentiles, we see significant differences. Unfortunately, we do not have gender and age reference tables, so interpretation is fuzzy.
Potential Medical Conditions Detected had nothing significant for either child. Both are at 95.6%ile on Dr. Jason Hawrelak Recommendations (they were 98.9 and 99.7%iles before) .
The thing that stands out is that the Son has a lot more Enzymes out of range (with the resulting substrates(consumers) and products also being out of range).
KEGG Suggested supplements has nothing significant for the daughter, but for the son we have the following being very significant:
Serine
Threonine
Glutamine
Cysteine
Arginine
A complex amino-acid supplement may be worth an experiment.
As an experiment (and trying to avoid two different kid diet), I did an uber-consensus from each child’s with tons of prescription medication but only one thing above my usual 50% of highest value.
We can see the spike in low percentile bacteria. This raises the question, has he had COVID (or a COVID vaccine) prior to the sample being done. These spikes show themselves also via Kaltoft-Møldrup and Box-Plot-Whiskers which are both sensitive to this pattern.
Criteria
Current Sample
Old Sample
Lab Read Quality
10.9
4.4
Outside Range from JasonH
4
4
Outside Range from Medivere
17
17
Outside Range from Metagenomics
10
10
Outside Range from MyBioma
13
13
Outside Range from Nirvana/CosmosId
27
27
Outside Range from XenoGene
49
49
Outside Lab Range (+/- 1.96SD)
22
22
Outside Box-Plot-Whiskers
76
100
Outside Kaltoft-Møldrup
248
89
Bacteria Reported By Lab
757
708
Bacteria Over 90%ile
61
82
Bacteria Under 10%ile
285
26
Shannon Diversity Index
2.807
2.451
Simpson Diversity Index
0.088
0.15
Chao1 Index
24924
19183
Lab: Thryve
Pathogens
35
30
Condition Est. Over 90%ile
2
0
Kegg Compounds Low
1001
1048
Kegg Compounds High
162
132
Kegg Enzymes Low
265
115
Kegg Enzymes High
381
296
Kegg Products Low
152
74
Kegg Products High
209
191
Kegg Substrates Low
148
69
Kegg Substrates High
229
212
Anti inflammatory Bacteria Score
89.2%ile
83.2%ile
Buytrate Bacteria Score
77.9%ile
90.2%ile
Histamine Producers
15.3%ile
38.2%ile
Histamine dropping is usually a good sign
From this weekend update of special studies, we can get a count of bacteria shifts strongly associated to symptoms.
Old Sample: 32 taxa
Latest Sample: 60 taxa
Daughter Compared to Prior Sample
First the numbers which are usually similar to the prior sample.
Criteria
Current Sample
Old Sample
Lab Read Quality
6.7
3.1
Outside Range from JasonH
6
6
Outside Range from Medivere
19
19
Outside Range from Metagenomics
7
7
Outside Range from MyBioma
12
12
Outside Range from Nirvana/CosmosId
26
26
Outside Range from XenoGene
47
47
Outside Lab Range (+/- 1.96SD)
11
61
Outside Box-Plot-Whiskers
98
203
Outside Kaltoft-Møldrup
132
134
Bacteria Reported By Lab
842
852
Bacteria Over 90%ile
66
202
Bacteria Under 10%ile
66
10
Shannon Diversity Index
3.064
3.411
Simpson Diversity Index
0.07
0.028
Chao1 Index
29791
35210
Lab: Thryve
Pathogens
36
35
Condition Est. Over 90%ile
0
0
Kegg Compounds Low
973
1027
Kegg Compounds High
43
80
Kegg Enzymes Low
89
44
Kegg Enzymes High
98
171
Kegg Products Low
55
29
Kegg Products High
52
86
Kegg Substrates Low
46
26
Kegg Substrates High
58
111
Anti inflammatory Bacteria Score
25.5%ile
28%ile
Buytrate Bacteria Score
95.9%ile
74.5%ile
Histamine Producers
21.7%ile
28.7%ile
From this weekend update of special studies, we can get a count of bacteria shifts strongly associated to symptoms.
Old Sample 53
Latest Sample: 39
Out of curiosity, I compared the symptom associated outliers. We found 3 are matches (of these 39) and one not matches for the taxa reported for each. That is close to the expected percentage of the same strains for people in the same house.
Autism has challenges because of its complex nature. This is compounded by a low number of samples to work from for Citizen Science analysis. The shifts reported from PubMed have a high pattern match with people who do not have autism.
I am going to try building a consensus for each by doing two itemsL
“Just give Me Suggestions”
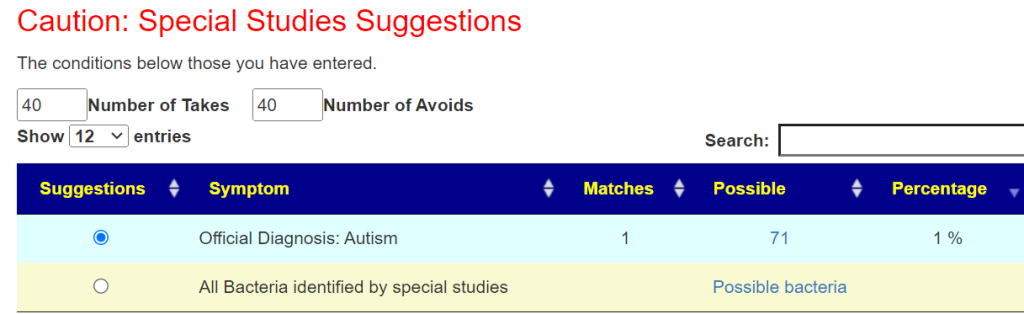
Doing PubMed Autism on [Changing Microbiome]
[All Bacteria identified by special studies]
The rationale is that the last one identify the bacteria that appears to be symptom causing in many people. We have a very poor match from what we do have a match for. This is not surprising because autism is a very wide spectrum.
We then see six sets of suggestion
Son
When I look at the details we have over 150 items with 6 recommended take (i.e. everyone agrees)
The probiotics that have no known adverse risk for any bacteria is below. The high value is 510.
When I look at the details we have just 15 items with 6 recommended take (i.e. everyone agrees)
The probiotics that have no known adverse risk for any bacteria are low in computed benefit, so I would ignore them.
Their values are low: 16/31 out of a high value of 301
Bottom Line
The failure to find significant matching patterns is a bit of a frustration to me. What we did find had very good agree for the son with 150+ items having each of the size suggestion set agreeing for the take. For the daughter, it was not as strong: 15 for 6 sets being in agreement, and 50 with 5 sets being in agreement.
Questions
I assume higher anti-inflammatory score is better – Daughter was 25% and Son was 89%
Deep Sleep with Son – 23% match that he has deep sleep issues is pretty strong?
Does not jump out, but indicates that microbiome is playing a role.
Son – lot more missed enzymes – what is that do you believe and probiotics help with that?
I avoid the word “believe”. A rational assumption is that disruption of enzymes compare to others impacts how the cells (including brain cells) react.
Spike in low percentage bacteria – likely long Covid for Son means he has less good bacteria now?
I avoid the words “good” or “bad” bacteria. Any bacteria far enough from typical values become bad; disruption to the microbiome and the body. Theses spikes are typically seen (pattern matching) with two conditions: Long COVID and ME/CFS. A common symptom of these two issues are cognitive issues – for example: memory, ability to learn, etc.
Histamine – Higher percentage is worse correct? Daughter was 21% and son was 15%
The intent of this site to assist people with health issues that are, or could be, microbiome connected. There are MANY conditions known to have the severity being a function of the microbiome dysfunction, including Autism, Alzheimer’s, Anxiety and Depression. See this list of studies from the US National Library of Medicine. Individual symptoms like brain fog, anxiety and depression have strong statistical association to the microbiome. A few of them are listed here.
The base rule of the site is to avoid speculation, keep to facts from published studies and to facts from statistical analysis(with the source data available for those wish to replicate the results). Internet hearsay is avoid like the plague it is.
I would say some small subjective improvements since last time, but no major changes. Reminder: I have a friendly MD in terms of antibiotics.
Metronidazole was on top in the last samples, I did it back then.
Comment: Metronidazole is no longer at the top but dropped down to 16% of the highest value. It appears to have done its magic in reducing the bacteria pointing to it as a tool..
Base Analysis
When people have multiple samples, I like to do side-by-side comparisons, especially when someone has been doing some of the suggestions suggested. The suggestions are computed and may not always work. Expert Systems and AI are not perfect; they typically do better than a person with only a few years of experience that has training in the discipline (better consistency, remember more facts, etc). How are we doing objectively?
Scores
We see two positive shifts in the latest sample: Increase of Anti inflammatory Bacteria Score and decrease of Histamine Producers.
Percentages of Percentiles
We see a lot of bouncing around between samples. The middle two images matches the typical pattern seen with ME/CFS and Long COVID. Those shifts have faded over the last 3 months with a different pattern appearing indicating a different dialect of gut dysfunction.
Multi-Vector Comparison
The main numbers are below. The take away, less bacteria that are in the high percentile range (at 95%ile, 10 -> 28 -> 23 -> 8). The numbers bounce around with the middle two being similar and the other two also similar. There are no really clear shift in these measures.
Criteria
11/18/2021
5/20/2022
6/22/2023
9/4/2023
Lab Read Quality
8.1
5.5
4.7
7.2
Outside Range from JasonH
6
6
9
9
Outside Range from Medivere
16
16
15
15
Outside Range from Metagenomics
8
8
7
7
Outside Range from MyBioma
5
5
6
6
Outside Range from Nirvana/CosmosId
20
20
23
23
Outside Range from XenoGene
29
29
35
35
Outside Lab Range (+/- 1.96SD)
7
6
17
3
Outside Box-Plot-Whiskers
36
69
54
38
Outside Kaltoft-Møldrup
93
48
47
88
Bacteria Reported By Lab
652
508
542
558
Bacteria Over 99%ile
7
4
6
2
Bacteria Over 95%ile
10
28
23
8
Bacteria Over 90%ile
29
42
36
22
Bacteria Under 10%ile
208
41
50
175
Bacteria Under 5%ile
180
19
8
157
Shannon Diversity Index
1.853
1.826
1.272
1.556
Simpson Diversity Index
0.056
0.038
0.087
0.09
Rarely Seen 1%
2
2
7
1
Rarely Seen 5%
14
5
21
8
Pathogens
41
24
29
36
From Special Studies
The top match was the same on all of the samples, with an increase when there was actually COVID.
Criteria
11/18/2021
5/20/2022
6/22/2023
9/4/2023
COVID19 (Long Hauler)
28%ile
33%ile
41%ile
28%ile
Next one:
15%ile
26%ile
20%ile
13%ile
The “next one” dropping implies some reduction of dysbiosis
Health Analysis
Using Dr. Jason Hawrelak Recommendations, there are many items on the edge of being in range with some items of interest (I strike out those that are unlikely to be of great concern):
Faecalibacterium prausnitzii at 27% of the microbiome or 96%ile
Faecalibacterium prausnitzii at 27% of the microbiome or 96%ile
I would suggest a test for candida to be safe. The data suggests a risk. If confirmed, candida would contribute significantly to gut dysbiosis [The interplay between gut bacteria and the yeast Candida albicans[2021]). I did a “back-flip” check of the top prescription items, and all of them reduces Candida (studies cited below).
Addendum – Predicted Symptoms
This was just added to the site today as a further refactor based on New Special Studies on Symptoms data. These are from [My Profile Tab]
Criteria
11/18/2021
5/20/2022
6/22/2023
9/4/2023
Forecast Major Symptoms
Neurological: Cognitive/Sensory Overload 40 % match on 25 taxa
DePaul University Fatigue Questionnaire : Racing heart 38 % match on 13 taxa
DePaul University Fatigue Questionnaire : Difficulty falling asleep 37 % match on 27 taxa
DePaul University Fatigue Questionnaire : Difficulty finding the right word 35 % match on 20 taxa
Autonomic Manifestations: urinary frequency dysfunction 66 % match on 6 taxa Immune Manifestations: Bloating 37 % match on 45 taxa
Neurological-Audio: hypersensitivity to noise 35 % match on 28 taxa
None
Neurological-Sleep: Chaotic diurnal sleep rhythms (Erratic Sleep) 50 % match on 18 taxa
Neurological: Spatial instability and disorientation 37 % match on 16 taxa
This can be helpful for judging possible severity (and potential improvement of some symptoms), for example: Neurological: Cognitive/Sensory Overload. See [Special Studies] tab.
2021 – 40% matches
2022- 24% matches
6/22/23 – 16% matches
9/4/2023 – 4% matches
Going Forward
COVID has had quite an impact on this microbiome. I am going to just go with the “Just Give Me Suggestions” option with the addition of what matched his diagnosis:
To explain a bit more. First I click the button below
And then click I could click the consensus report to see what the top items are:
Which are shown below.
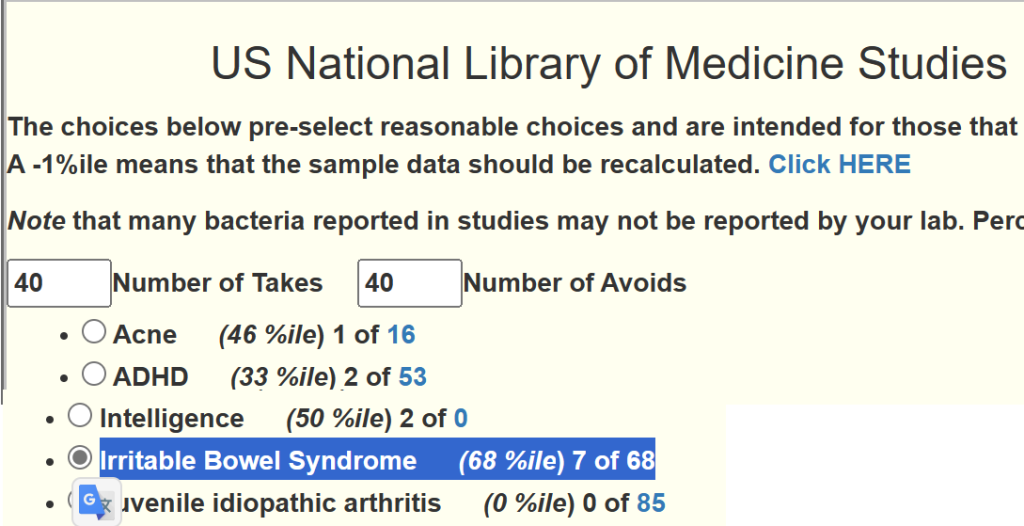
In this case, I want to add Irritable Bowel Syndrome suggestions (on the Changing Microbiome Tab)
Instead of the usual 4 packages of suggestions, we have 5
When we look at the consensus report we see the same items there, but the values have increased.
The intent is put a little bias on the numbers towards specific conditions of greatest concern.
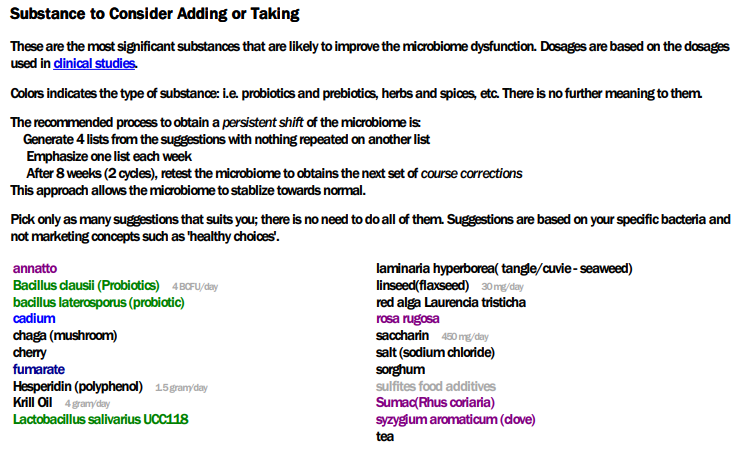
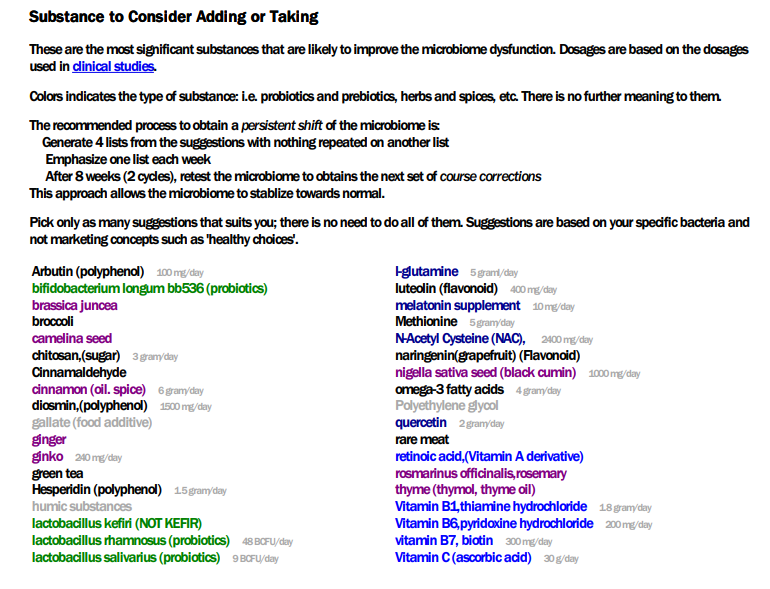
PDF Suggestions
I tend to favor the PDF suggestions because it simplifies things for many readers. Also the PDF gives a good list of citations (never complete) used to make the citations to persuade MDs to see that the suggestions are based on studies — a lot of studies.
The PDF suggestions are below (using the consensus view is another option for those more technically orientated). I clip from the PDF to keep the blog simpler for the typical reader.
This is a little longer list than usual, so I went to the consensus report to get priority data. Top value was 618, so 309 is the 50% threshold.
Minor note: quercetin with resveratrol is an avoid, quercetin is a take. resveratrol by itself is a negative (-113). At times, you need to look at the technical details/consensus to clarify things; the data we are using is incomplete and sparse…. If clearly contradictory suggestions appear, then don’t do them (thing an abundance of caution).
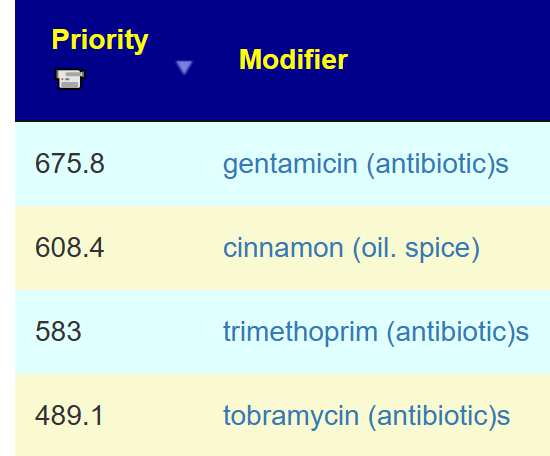
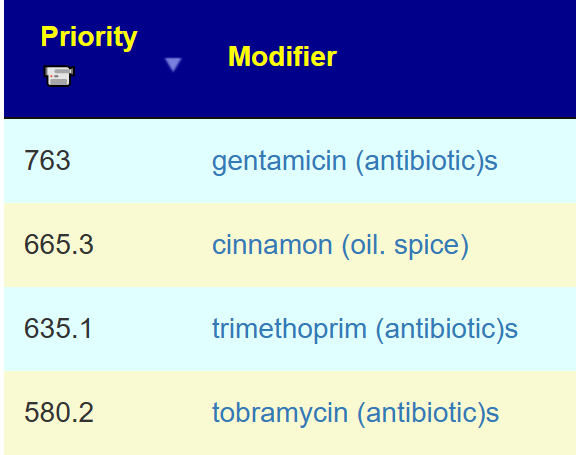
Because he has an antibiotic friendly MD, the following are the TOP antibiotics with notes:
“Since gentamicin has minimal gastrointestinal absorption,…it has applications in several clinical scenarios, such as bacterial septicemia, meningitis, urinary tract infections, gastrointestinal tract (including peritonitis), and soft tissue infection,” NIH StatPearls
“The FDA-Approved indications include acute infective exacerbation of chronic bronchitis, otitis media in pediatrics only, travelers diarrhea for treatment and prophylaxis, urinary tract infections, shigellosis, pneumocystis jirovecii, pneumonia/pneumocystis carinii pneumonia (PJP/PCP), and toxoplasmosis, both as prophylaxis and treatment. ” NIH StatPearlls
CFS Antibiotics are also above the threshold. Since the prior sample had a strong Long COVID or ME/CFS Profile, I would be inclined to include one of those below in the antibiotic rotation. The microbiome cannot make a diagnosis of most things, with most ME/CFS microbiomes there is a particular pattern which you had in your last sample but which has disappeared from your current sample which looks more like your first sample. I read this as recovering from ME/CFS…. in likely a fragile state since relapse is very common with ME/CFS.
My own experience is that it is better to overcure ME/CFS and when there are signs of recovery…. no backflips of joy or running marathons; keep doing slow walks that becomes a bit further each week for 6-12 months. Your microbiome is fragile and can quickly slip back.
I prefer to use the strategy of going for prescription items that are both suggested from the microbiome and been shown to help with one or more of the diagnosis conditions. This usually encounter low resistance from physicians — they are clueless for the microbiome, but very accepting of published studies. An antibiotic that is used as a prophylaxis usually encounter little resistance.
KEGG Suggestions
This is done by using information from the bacteria found with some fudge factors. I am in discussion with some Ph.D. candidates to build this concept directly from the FASTQ files and will hopefully have this as an added feature next year.
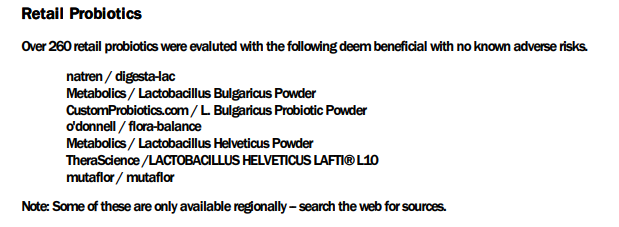
The KEGG probiotics is the usual pattern for ME/CFS and Long COVID with the top one being the usual, with the top reasonably available ones for other families shown below. I usually like to compare the values with those from consensus to minimum risk (i.e. two thumbs up, we do; mixed, we skipped)
The suggestions should be thought as influencers. The human population is often a good analogy or parable for the microbiome population. Each influencer shifts the population in the desired direction. Based on Cecile Jadin’s work and several studies, I am a firm believer in short duration (1-2 weeks) of each influencers. Just as with human influencers, people stop listening if the same person just keeps droning on and on. If a different person starts speaking, you get persuaded more. If a mob start to shout, yet a different human behavior will occur. In terms of the microbiome, “stop listening” means mutations that are resistant to the item will start to increase. Items line vitamins and minerals can be taken continuously; items that are likely to have bacteria resistance developed should be taken for a week and then another item replace it.
Herbs and spices: cinnamon, ginger, black cumin, thyme, rosemary, quercetin (suggests just before each antibiotic with a few days of overlap because it has potential synergistic activity with antibiotics [2020], [2016],[2018] )
Remember our goal is to destabilize a stable microbiome dysfunction.
Questions and Answers
While there has not been significant changes in many of the vectors between this sample and the prior sample from a few months earlier, there has been two significant objective changes:
Significant improvement of Anti inflammatory Bacteria Score (higher) and Histamine Producers (Lower).
The lost of the ME/CFS – Long COVID spike in the 0-9%ile
Q: Do you/should I use the colored list now instead of the consensus list?
Either are fine, the color list (from PDF) is what I tend to use in post because it is easier for new readers to understand (and automatically sent on new uploads). The consensus page is more complex but allows people to apply their own logic and priorities.
Q: “Quercetin (suggests just before each antibiotic with a few days of overlap because it has potential synergistic activity with antibiotics”
Q: I just did Mutaflor for 8 days and felt really tired all the time (but in the end I also got a flu/cold, so maybe that was the reason and not mutaflor). Nevertheless, if it was a herx reaction, I wonder if I should have taken it for longer until the reaction disappeared? (I stopped it 4 days ago.) Not sure if this question even makes sense.
My personal choice would be to keep taking it for at least a week (perhaps 2). Remember that the traditional pattern for a herx is feeling bad for X hours and then things get better. The duration of the feeling bad usually decrease from day to day. Catching a cold makes interpretation challenging.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide information on rotations etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
In reviewing many papers with the microbiome I noticed that often the researchers restrict their examinations to the taxa that is reported in all samples. I suspect this is due to a lack of sufficient statistical training and/or not understanding the natures of the microbiome.
Recently I came across these papers that uses an approach that I often have used, working off relative frequency of detection a.k.a. prevalence.
This post is going to use samples available at Microbiome Prescription Citizen Science site. We are going to restrict to one lab source and divide the data into two groups based on their self-declare symptoms and diagnosis.
Patients with Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) declared [Obs: 271]
Patients without Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) declared and other status declared (for example: “Asymptomatic” [Obs:569]
Naive First Pass
We are going to take the average count for each group ignoring no values reported. We are going to restrict it to taxa where we have at least 30 non-zero values [1,564 taxa]. We found some 77 taxa with a t-score over 2.81 (p < 0.005)
taxa name
taxa rank
Shift
T_score
Prevotella copri
species
low in ME/CFS
-5.27
Prevotella
genus
low in ME/CFS
-4.52
Sporolactobacillaceae
family
low in ME/CFS
-4.2
Sporolactobacillus putidus
species
low in ME/CFS
-4.19
Sporolactobacillus
genus
low in ME/CFS
-4.19
Prevotellaceae
family
low in ME/CFS
-4.1
Firmicutes
phylum
high in ME/CFS
3.94
Blautia
genus
high in ME/CFS
3.91
Cetobacterium ceti
species
high in ME/CFS
3.89
Cetobacterium
genus
high in ME/CFS
3.84
Deeming Not Reported to be Zero
In this case we have 78 taxa with a t-score over 2.81 with slight changes of t-scores.
taxa name
taxa rank
Shift
T_score
Prevotella copri
species
low in ME/CFS
-5.31
Sporolactobacillaceae
family
low in ME/CFS
-4.63
Sporolactobacillus putidus
species
low in ME/CFS
-4.62
Sporolactobacillus
genus
low in ME/CFS
-4.62
Prevotella
genus
low in ME/CFS
-4.5
Prevotella oulorum
species
low in ME/CFS
-4.35
Prevotellaceae
family
low in ME/CFS
-4.08
Bifidobacterium gallicum
species
low in ME/CFS
-3.97
Firmicutes
phylum
high in ME/CFS
3.94
Blautia
genus
high in ME/CFS
3.91
Prevalence
We followed the same process as above and limited things to a Chi-2 probability of < 0.005 (as used above) We ended up with 65 taxa.
tax_Name
Tax_Rank
Prevalence in MECFS %
Prevalence Control %
Difference
Chi2
FoldChange
Deferribacteres
phylum
33.6
20
13.5
14
1.7
Erysipelothrix inopinata
species
21
10.7
10.3
14
2
Deferribacterales
order
33.6
20
13.5
14
1.7
Deferribacteraceae
family
33.6
20
13.5
14
1.7
Deferribacteres
class
33.6
20
13.5
14
1.7
Mogibacterium vescum
species
27.7
15.8
11.9
13
1.8
Haploplasma cavigenitalium
species
8.5
2.8
5.7
13
3
Haploplasma
genus
8.5
2.8
5.7
13
3
Gluconobacter
genus
15.1
6.9
8.3
13
2.2
Prosthecobacter fluviatilis
species
7.7
2.5
5.3
12
3.1
Comparing these two lists, we found only 6 taxa in common
Bifidobacterium angulatum
Propionigenium modestum
Pseudomonas viridiflava
Cetobacterium ceti
Cetobacterium
Propionigenium
The next result is that we have 78+65 – 6 = 137 statistically significant bacteria with p < 0.005.
Bottom Line
There are at least two different statistical ways of determining significance. IMHO, the prevalence approach is likely to be a superior tool for diagnosis purposes because it is possible to compute the probability of a match to the above patterns despite some bacteria not being reported.
A reader raised a valid question which actually triggers other related questions.
You seem to like the “percentage of percentiles” measurement, but I’m not convinced it’s being analyzed appropriately. As I understand it, you first convert to percentiles, getting numbers in [0, 100]. I think this is fine. Then you histogram these percentiles. Because each lab will perform the same measurements every time, I think this is also fine. However, the result is compositional data in the sense of Aitchison, and it should be analyzed in a manner consistent with that. For compositional data, a chi^2 test is inappropriate because it relies on the number of species (or genera) measured.
My suggestion is to apply a centered logratio transform to each person’s percentages and fit a normal distribution to the transformed data. To determine whether someone’s microbiome deviates significantly, calculate a multivariate normal tail probability. Beware that the covariance matrix will be rank deficient (you’re in a ten-dimensional space, but there are only nine parameters because percentages sum to 100). You may want a robust fit because it’s reasonable to expect that the microbiome of someone ill might be an outlier.
For more information about compositional data, see Aitchison, J., “The Statistical Analysis of Compositional Data,” Journal of the Royal Statistical Society. Series B (Methodological) Vol. 44, No. 2 (1982), pp. 139-177; Aitchison, J., “The Statistical Analysis of Compositional Data,” Chapman & Hall, London, 1986; and Aitchison, J. “A Concise Guide to Compositional Data Analysis,” unpublished manuscript, 2005, available online (just Google). For other approaches to compositional data analysis, see Greenacre, Michael; Grunsky, Eric; Bacon-Shone, John; Erb, Ionas; Quinn, Thomas, “Aitchison’s Compositional Data Analysis 40 Years On: A Reappraisal,” arXiv:2201.05197, 13 Jan 2022, to appear in Statistical Science.
What is the statistical basis for other Diversity Indices?
How to calculate these numbers is well determined — they seem to be brilliant ideas tossed out there that seems to fit the data for some study. For some background, see this page. The problem is a lack of rigor, especially statistical rigor.
Diversity indices, particularly the Shannon-Wiener index, have extensively been used in analyzing patterns of diversity at different geographic and ecological scales. These indices have serious conceptual and statistical problems which make comparisons of species richness or species abundances across communities nearly impossible.
The problem is an absence of a native statistical model. For example, it does not fit the usual ones.
Normal distribution – “The distribution that shall rule them all” because that is what is always assumed and what is usually taught outside of mathematics department (who knows better)
The key question is simple, what is the distribution underlying diversity Indices? We read ” In the literature of biodiversity, according to Ricotta (2005), there are a “jungle” of biological measures of diversity.”[2017]. Zheng’s A new diversity estimator[2017] in Journal of Statistical Distributions and Applications where he states “There are many other open problems built on this connection between birthday problem and diversity measures. ” The problem is this, the birthday problems deals with 366 discrete well defined boxes that are well defined. Dealing with the microbiome, we lack these boxes. Consider a measure of a microbiome sample in 2000, there are a large number of different bacteria species in Lactobacillus. Today, we have these species no longer placed in 1 genus, but 25 genus [2020] including:
Acetilactobacillus,
Agrilactobacillus,
Amylolactobacillus,
Apilactobacillus,
Bombilactobacillus,
Companilactobacillus,
Dellaglioa,
Fructilactobacillus,
Furfurilactobacillus,
Holzapfelia,
Lacticaseibacillus,
Lactiplantibacillus,
Lapidilactobacillus,
Latilactobacillus,
Lentilactobacillus,
Levilactobacillus,
Ligilactobacillus,
Limosilactobacillus,
Liquorilactobacillus,
Loigolactobacilus,
Paucilactobacillus,
Schleiferilactobacillus,
Secundilactobacillus.
With the same strains/species, our diversity indices will be very different because our boxes are arbitrary and “soft” unlike the days of the year or the roll of a dice.
Back to percentage of percentiles
While I show genus and species in the table for ease of understanding of the typical reader, I originally did it solely with the lowest identifiable levels (the “atoms” or the microbiome) – species. At the species level, it is not compositional. There is no composition! Looking at the data that was actually received, I noticed many genus had no species listed. In some cases, the genus had species, but none of the known ones were detected. In other cases, the test did not report any species in over 3000 test results.
On this basis I decided to use try using both species and genus. I soon discovered that they almost always exhibit a similar pattern and chi^2. At this point, I opted for benefiting my readers and not as much rigor as some would like. We could do the lowest taxonomical level reporting across the hierarchy as one solution.
This approach ends up with us side-stepping the classification issues cited above. We are dealing with distinctive, non-overlapping events (a bacteria being identified) and then convert them to percentile giving use a continuous uniform distribution for each of these independent events. IMHO, at this point we have a good model to chi^2 test. We are not dealing with measuring a population, just a sample.
In answer to “a chi^2 test is inappropriate because it relies on the number of species (or genera) measured.” is missing the point. If I get two bags of coins from the bank and then flip them to determine if they are biased — whether the bags contains 1000 or 100,000 coins is significant only on the ability to determine the margin of error. The number of species/genus is only significant in that sense. If there is a strong bias with a small number, then having more will not change the bias.
For samples coming from uBiome, Ombre/Thryve and Biomesight there are two important numbers reported. [Count] and [Count_Norm].
[Count] is the number coming from the lab equipment, the bacteria detected.
[Count_Norm] is the above number scaled to be out of one million (1,000,000)
The question arises, if you have low lab quality and the number of bad bacteria also dropped: Is this an actual improvement or a false improvement due to low lab quality?
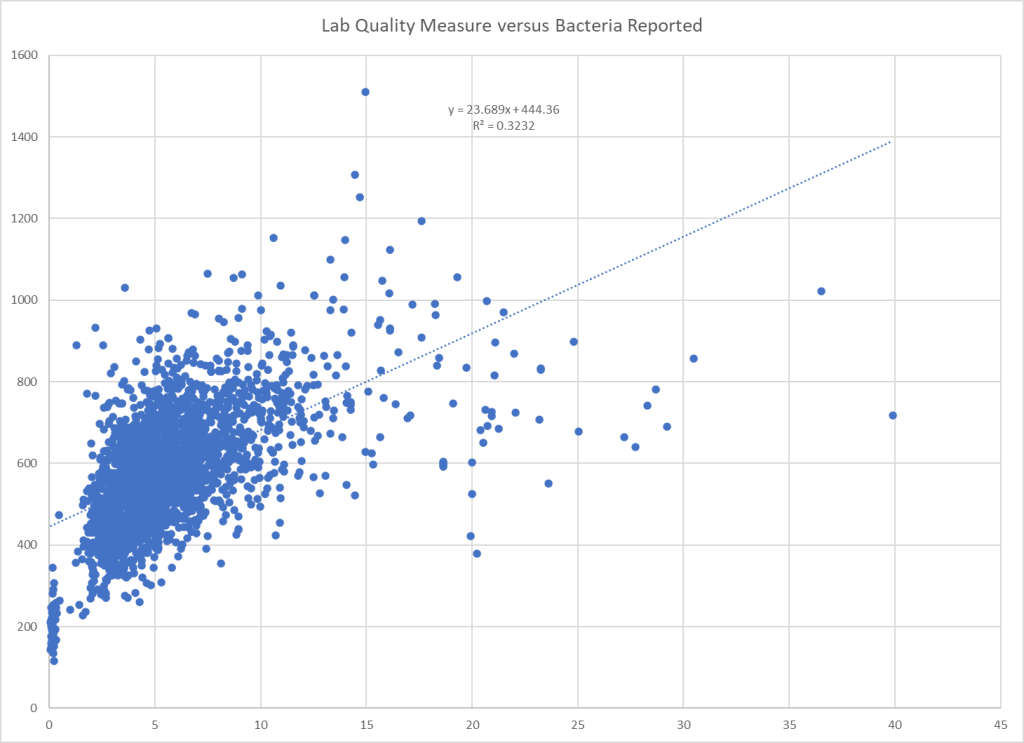
To partially answer that question, I pulled biomesight samples (biggest collection) and plotted the data. Shown below:
Vertical axis is number of bacteria reported
Horizontal axis is lab quality measure
As is shown, there is a relationship.
Using this data and sample values of 4.3 and 8.4, we compute 546 and 643 for expected bacteria (just use the formula on the chart). This means that with 4.3 we expect only 85% (546/643 * 100) of the count seen with 8.4.
So we see the changes below are likely true improvements: (Left is 4.3, right is 8.4)
For bacteria reported by lab, the numbers suggests the left column has less odd bacteria and the gut microbiome may becoming more uniform.
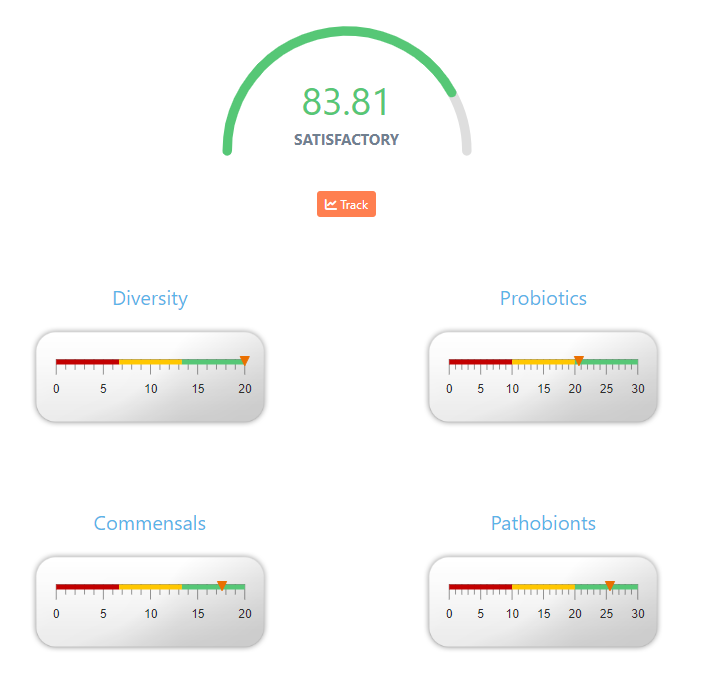
Today I was asked if the numbers shown on various sights like the one below, ” if this result is correlated with the severity of the patient?”. The answer is No. The usual reason that such numbers appear on sites is to satisfy customers asking for such numbers. Simple, easy to understand number.
Businesses want to make customers happy — so they literally cook-up a number to show on their reports. There is no research supporting any of the magical numbers that I have seen. Some one put together some numeric formula to generate the numbers.
For Biomesight, the logic is shown on the page with the right display
If you sum up the values for each dial, you get the total. When you view the percentage, it is not so obvious: 100%, 69%, 88%, 85% looks like a complex formula is being used.
Analogy: Give me a Health Measure for a Person
The microbiome is very much like a person. How would you create a single value for a person?
Probiotics –> Income
Commensals –> Savings
Pathobionts –> Debts
Diversity –> Health?
Married and marriage status
Chronic Conditions
Health Status
Height
Weight
Gender
etc
Would a person with no debt, good savings, a low income and married with 5 kids be a higher or lower measure than someone with moderate debt, high income, small savings and no relationships?
Are there any studies?
What about the ratios used in the literature?
Bacteroides/Bifidobacterium Ratio
Bacteroides/Clostridium Ratio
Blautia/Bacteroides Ratio
Firmicutes/Bacteroidetes Ratio
Prevotella/Bacteroides Ratio
Well, the sample that I am looking at have 43%ile, 98%ile, 7.2%ile, 58%ile and 19%ile. The numbers are all over the place!
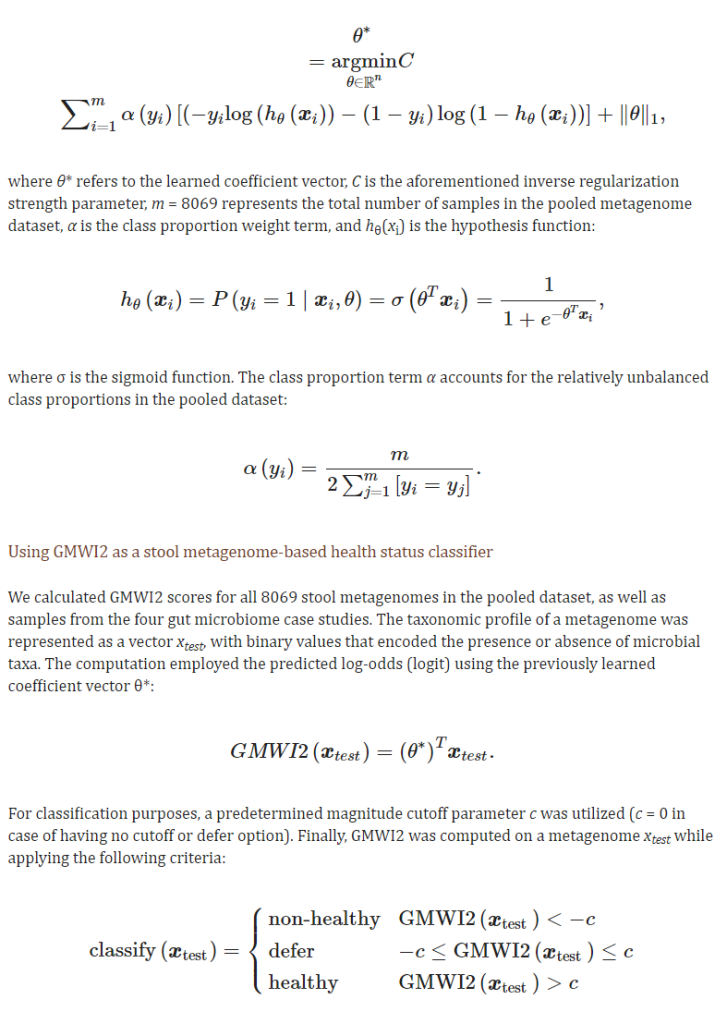
Their latest study states: ” accuracy of 80% in distinguishing healthy (no disease) from non-healthy (diseased)” So 1 in five times, they will misclassify a healthy person as having a disease.
An example of the algorithm being used is below.
This is just trying to determine if the person is healthy or not — nothing about severity.
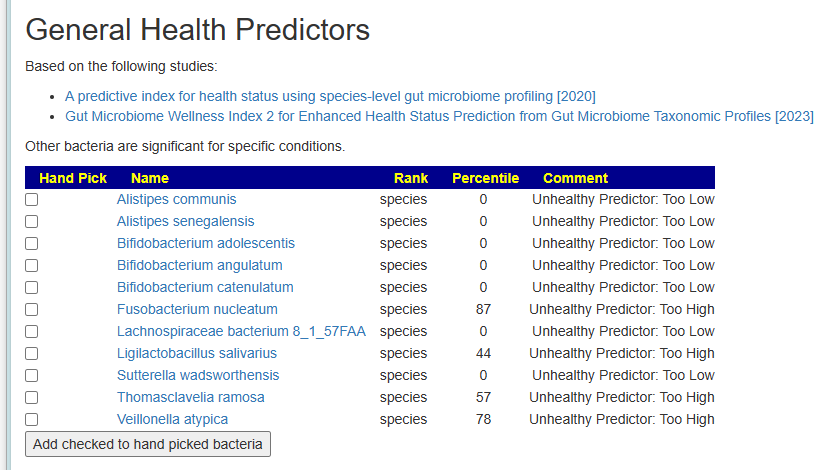
My approach is simple, I simply flagged the bacteria deemed to be unhealthy. Just list them.
Latest microbiome results are in. Seems like my microbiome is stubborn and stuck these last few tests. Wondering if I should just use this test suggestions exclusively or combine with my prior Thorne test
We have two sample – one via BiomeSight and one via Thorne. This post is going to do two things:
Look at Suggestions – by combining both sets of suggestions using the Uber Consensus
Look at the differences between the reports.
We also review “which is better”. My focus is clinical application to individuals — not research papers; answer at bottom.
Uber Consensus
The process has become very simple — “Just give me Suggestions!” on both samples and then going to uber consensus as illustrated by the video below.
The result was excellent agreement on suggestion between each set of results. The CSV files are attached below.
Items less than 100 should be ignored (accuracy of measurement limits). There are a few dramatic differences.
Bacteria Name
Thorne Count
BiomeSight Count
Firmicutes
396799
529540
Actinobacteria
60610
2100
Bacteroidetes
461289
448230
Proteobacteria
6095
18150
Chlorobi
36
429
Acidobacteria
35
100
Cyanobacteria
83
20
Spirochaetes
85
30
Verrucomicrobia
59
10
Chloroflexi
77
50
Tenericutes
54
30
Deinococcus-Thermus
48
30
Fibrobacteres
4
10
Synergistetes
17
20
By Count
Looking at Percentiles next
Bacteria Name
Thorne %ile
BiomeSight %ile
Chlorobi
25
84
Actinobacteria
85
33
Acidobacteria
34
81
Spirochaetes
81
36
Cyanobacteria
31
1
Deinococcus-Thermus
55
29
Firmicutes
14
37
Chloroflexi
67
50
Verrucomicrobia
14
1
Tenericutes
13
2
Proteobacteria
10
18
Synergistetes
6
4
Bacteroidetes
55
56
Fibrobacteres
1
0
By Percentile ranking
We have Bacteroidetes in agreement with both — but for the rest…
At the genus level
Bacteria Name
Thorne Count
BiomeSight Count
Bacteroides
180054
397640
Blautia
16470
107220
Roseburia
16793
73640
Faecalibacterium
109196
152890
Corynebacterium
43413
820
Ruminococcus
9177
44170
Phocaeicola
223209
199669
Parabacteroides
11855
31940
Phascolarctobacterium
6101
23980
Dorea
36
13000
Sutterella
16
11339
Oscillospira
0
8250
Coprococcus
6120
12589
Eggerthella
6491
760
Pseudobutyrivibrio
149
5790
Lachnospira
11593
6230
Prevotella
954
4260
Anaerostipes
9303
6310
Clostridium
2039
4960
Pedobacter
46
2410
Odoribacter
4077
2060
Bifidobacterium
2783
1019
Escherichia
75
1610
Porphyromonas
1372
150
Mediterraneibacter
14831
13629
Bilophila
6
1110
Veillonella
75
1160
Desulfovibrio
1900
1250
Streptococcus
1477
840
Acetivibrio
33
470
Chlorobaculum
6
429
Finegoldia
1339
920
Gemella
17
400
Enterococcus
585
220
Paenibacillus
376
20
Mogibacterium
39
370
Acetobacterium
15
340
Serratia
47
350
Eubacterium
517
240
Megasphaera
35
290
Selenomonas
52
290
Bacillus
248
10
Caldicellulosiruptor
11
240
Campylobacter
235
10
Slackia
16
240
Sphingobacterium
48
270
Caloramator
10
190
Staphylococcus
181
10
Hathewaya
8
170
Peptoniphilus
656
800
Peptostreptococcus
6
150
Microbacterium
125
10
Adlercreutzia
525
620
Rhodothermus
6
90
Erysipelothrix
12
90
Acidaminococcus
12
90
Hymenobacter
80
10
Negativicoccus
115
50
Collinsella
74
10
Rhodococcus
67
10
Dialister
25
80
Anaerococcus
336
390
Pseudoclostridium
8
60
Moorella
9
60
Vibrio
60
10
Caldilinea
1
50
Brochothrix
2
50
Mycobacterium
67
20
Neisseria
57
10
Pectinatus
7
50
Thermoclostridium
16
50
Alkaliphilus
9
40
Shewanella
31
60
Lactobacillus
57
30
Leptospira
4
30
Deinococcus
35
10
Tetragenococcus
5
30
Ethanoligenens
34
10
Weissella
10
30
Gulosibacter
1
20
Pseudoclavibacter
2
20
Kocuria
28
10
Meiothermus
2
20
Stenotrophomonas
28
10
Symbiobacterium
3
20
Devosia
4
20
Dysgonomonas
34
20
Azoarcus
21
10
Leuconostoc
9
20
Glaciecola
1
10
Turicibacter
21
30
Pelotomaculum
1
10
Parascardovia
2
10
Lentibacillus
2
10
Actinopolyspora
2
10
Kitasatospora
2
10
MLOs
3
10
Ochrobactrum
3
10
Rickettsia
3
10
Luteibacter
3
10
Fibrobacter
4
10
Pediococcus
14
20
Halanaerobium
6
10
Dyadobacter
14
10
Mycoplasma
17
20
Thauera
9
10
Lysobacter
11
10
By Counts
Looking at the percentile rankings — the absolute numbers may vary greatly, but what about relative percentiles?
Bacteria Name
Thorne %ile
Biomesight %ile
Ochrobactrum
2
2
Actinopolyspora
1
1
Halanaerobium
1
1
MLOs
1
1
Glaciecola
1
1
Lentibacillus
1
1
Pelotomaculum
1
1
Parascardovia
1
1
Luteibacter
1
1
Phocaeicola
89
89
Rickettsia
1
0
Pediococcus
10
9
Fibrobacter
2
0
Mycoplasma
5
3
Alkaliphilus
1
3
Finegoldia
85
88
Kitasatospora
3
0
Thauera
5
1
Streptococcus
55
50
Turicibacter
12
17
Peptoniphilus
64
58
Hathewaya
1
8
Clostridium
18
11
Desulfovibrio
61
69
Eubacterium
38
46
Symbiobacterium
1
9
Enterococcus
88
79
Sphingobacterium
13
23
Pseudoclavibacter
1
11
Anaerococcus
72
83
Eggerthella
98
86
Gulosibacter
0
12
Lactobacillus
23
11
Bifidobacterium
55
43
Leuconostoc
2
14
Shewanella
35
47
Prevotella
50
63
Corynebacterium
99
86
Collinsella
13
0
Oscillospira
0
16
Faecalibacterium
49
65
Meiothermus
1
17
Caloramator
1
19
Coprococcus
39
57
Lysobacter
18
0
Odoribacter
81
63
Adlercreutzia
63
81
Pedobacter
13
31
Dyadobacter
20
1
Dysgonomonas
24
4
Mediterraneibacter
69
90
Devosia
1
22
Acetivibrio
5
27
Thermoclostridium
9
32
Ethanoligenens
25
1
Dialister
11
35
Veillonella
16
41
Pectinatus
1
27
Porphyromonas
88
62
Moorella
1
28
Negativicoccus
66
39
Lachnospira
51
21
Rhodothermus
1
32
Tetragenococcus
1
32
Acetobacterium
3
34
Anaerostipes
65
96
Bilophila
1
33
Ruminococcus
14
47
Weissella
2
35
Parabacteroides
42
75
Acidaminococcus
4
39
Pseudoclostridium
1
37
Leptospira
1
42
Serratia
34
75
Slackia
4
45
Phascolarctobacterium
56
97
Erysipelothrix
4
46
Sutterella
1
46
Bacteroides
39
87
Roseburia
43
91
Escherichia
28
77
Selenomonas
21
73
Deinococcus
54
1
Megasphaera
18
72
Brochothrix
1
56
Kocuria
58
2
Mogibacterium
17
74
Stenotrophomonas
63
3
Azoarcus
61
0
Caldilinea
0
61
Caldicellulosiruptor
2
64
Mycobacterium
87
24
Hymenobacter
68
1
Blautia
5
73
Paenibacillus
87
19
Neisseria
69
0
Pseudobutyrivibrio
25
95
Campylobacter
75
1
Gemella
4
82
Peptostreptococcus
1
81
Chlorobaculum
1
84
Staphylococcus
85
0
Vibrio
91
2
Bacillus
92
1
Rhodococcus
91
0
Dorea
1
93
Microbacterium
94
1
By Percentile
Bottom Line
I have never had much belief in the absolute accuracy of the bacteria named or the count. Why? Simple, I understand the statistical process being used and its weakness. I will leave arguments over “which is better” and “which is accurate” to others.
My focus and concern is to improve the microbiome. With sparse data and the great complexity involved, I am actually very pleased that the suggestions are in agreement. The suggestions are computed using fuzzy logic expert systems. The noise in the data and the statistical processes involved seem to be smoothed out by this Artificial Intelligence engine approach.
Score: Labs: -2, Microbiome Prescription 2
Which is better?. My focus is clinical application to individuals, both give similar suggestions using the Fuzzy Logic Expert System. There is no difference in that sense.
.







Recent Comments