Hey Ken. At a talk last night by a functional med/environmental doc, she said that recent research has shown that 21% of the population has MCAS (Mast Cell Activation Syndrome). Apparently, she said, MCAS is finally being recognised by the medical profession. She went on to say that if someone with MCAS gets Covid, they almost always get Long COVID. Can you draw any conclusions between the microbiome and MCAS as you have with other conditions, and maybe relate it to your other research into Long Covid?
The joy of a citizen science site with lots of contributed data is that we can get informal insight. For more information about the probable bacteria involved see Multiple Chemical Sensitivity (MCS) – A Cause Found?
Q: Does 21% of the population has MCAS (Mast Cell Activation Syndrome)?
A: We have 336 samples annotated with MCAS or histamine issues out of 1747 annotated samples. That is 19.2%. Conclusion: We are in agreement with the research.
Q: if someone with MCAS gets COVID, they almost always get Long COVID?
A: This is a bit of a chicken and an egg question. People with CFS/ME gets MCAS. Looking at uploads prior to Long COVID appearing, we actually have 30.5% of all samples with MCS; 16.5% of samples with ME/CFS (104). The incidence of MCAS in this ME/CFS population was 58%.
We have 190 samples annotated with Long COVID but only 13 reporting MCAS. My conclusion is that all of the people she saw with MCAS were borderline ME/CFS or ME/CFS already. A likely correct statement is that someone with ME/CFS and MCAS is likely to get Long COVID. All that COVID is likely to do is to push the person further into the ME/CFS spectrum.We cannot separate Long COVID from ME/CFS.
Doing filtering of people with MCAS without ME/CFS and then Long COVID, we get a 6.4% incident rate. This suggests that MCAS without being comorbid with ME/CFS does not always get Long COVID.
Do you have a blog post where I can learn more about how percentile distribution of a 16s can give statistical insights ? You often mention the concept that a “good” sample has a even distribution…I’m trying to understand why so and what uneven distribution might mean etc
The answer is statistics!!
At each taxonomy level (species, genus, family, etc) we can reasonably assume that the count of each bacteria taxonomy are independent of others of the same rank. There may be a little correlation (if A goes up, B goes up), but in general, not significant.
When we use percentile instead of percentage, we change the information about the bacteria in a uniform distribution. Suppose you have 120 dice. You roll all of them. You expect to have around 20 with 1, 20 with 2, 20 with 3, 20 with 4, 20 with 5 and 20 with 6.
If you get 40 dice with 1 and 2 dice with a 6, you are reasonable to suspect that the dice are biased or loaded.
Instead of a 6 sided die, we use a 10 sided die — 10%ile ranges. If the number in each 10%ile range are the same, then you can assume that the die is fair OR in our case, the microbiome is balanced. If you get a great difference in each 10%ile ranges, you suspect that the die is bias OR the microbiome is unbalanced (as in an unbalance die).
Where there is over or underrepresentation gives us hints as to where there may be an issue. It does not tell us what the issue is. It simply tells us that the microbiome is unbalanced and points us at subsets of bacteria worth examining.
Wait! There is More
A reader sent me this recent paper which appears to emphasis this issue for having a high count in the 0-9%ile for inflammatory conditions.
These observations suggest a general mechanism that underlies changes in diversity in perturbed gut environments and reveal taxon-independent markers of “dysbiosis” that may explain why widespread yet typically low-abundance members of healthy gut microbiomes can dominate under inflammatory conditions without any causal association with disease.
The question of causal association not being found may be a matter of sample size being used and cross-interactions and cooperation between these “minor voices”. The paper data came from Fecal Matter Transplants data and is illuminating on why many FMT fail to persist.
This is a look at Small intestinal bacterial overgrowth (SIBO) from the aspect of the microbiome. Whatever is happening in the small intestine flows out of it and impacts downstream systems. Items that modifies any microbiome abnormalities will likely impact the small intestine.
We have two bacteria that are reported significant in at least 2 of the 3 labs:
Bacteroides caccae (species)
Holdemania (genus)
A total of 31 bacteria (P < 0.001) was flagged as being significant and added to our collection.
We then look at Percentile and found only Bifidobacterium adolescentis showing a significant shift.
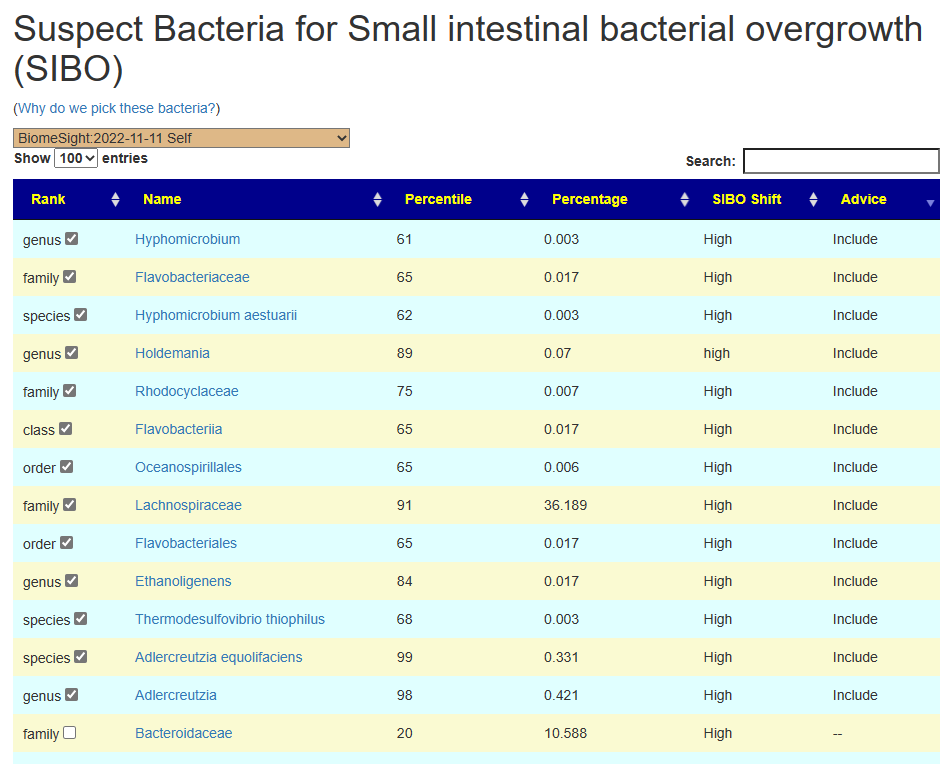
The complete list is below. Note that almost everything is High with SIBO.
ShiftIs
tax_name
tax_rank
High
Flavobacteriia
class
High
Bacteroidia
class
High
Spongiibacteraceae
family
High
Lachnospiraceae
family
High
Bacteroidaceae
family
High
Flavobacteriaceae
family
High
Rhodocyclaceae
family
High
Anaerolinea
genus
High
Ethanoligenens
genus
High
Trabulsiella
genus
High
Bacteroides
genus
High
Hyphomicrobium
genus
High
Myroides
genus
high
Holdemania
genus
High
Pseudoflavonifractor
genus
High
Adlercreutzia
genus
High
Bacteroidales
order
High
Flavobacteriales
order
High
Oceanospirillales
order
High
Nitrosomonadales
order
High
Bifidobacterium thermophilum
species
High
Hyphomicrobium aestuarii
species
High
Anaerolinea thermolimosa
species
High
Thermodesulfovibrio thiophilus
species
High
Bacteroides sp. dnLKV9
species
High
Bacteroides sp. 35AE37
species
High
Bacteroides caccae
species
High
Adlercreutzia equolifaciens
species
High
Blautia obeum
species
High
Pseudoflavonifractor capillosus
species
Low
Bifidobacterium adolescentis
species
We have only one clear agreement with the literature: Bacteroides with a large number of species deemed significant.
Compounds Produced
SIBO is usually detected by breath tests. The question is whether the chemicals detected in the breath is associated with the compounds that bacteria produced. What we found is below. The top 4 product in this list are the likely suspect for the first stage. These likely contributed to the chemicals detected. In particular, N-Acyl-L-homoserine abundance is associated with “Over 50 Gram-negative bacteria species (including several pathogenic species) use AHLs as autoinducers and the means of their communication in Quorum sensing” In other words it is not the source, but sends signals to the source bacteria to release the chemicals detected on the breath.
Trying to “find” the specific bacteria is not practical
📚4543 different bacteria produces Hydrogen (just click to see the list)
📚3817 different bacteria produces Hydrogen Sulfide
After reading your blog for many many years I finally managed to get a microbiome sample done (Biomesight). I suffer from debilitating MCS (multiple chemical sensitivity), mold sensitivity, and associated CFS. I have been isolated at home for almost 20 years now. Pretty much unable to function in any way normally, because of these sensitivities.
I think it all started in early 2000 with food poisoning from a poorly cooked chicken, that had been left out warm for too long. After this chicken meal my body simple went haywire. My gut was so sensitive that even drinking just a glass of water produced something similar to an anaphylactic shock.
It took several months to subside, and for me to completely revamp my diet and figure out what few items I was able to eat.
My body feels toxic. Like I am being constantly poisoned. Main symptoms are severe bloating and gas, extreme irritability and mood changes, brain fog and lethargy, poor blood flow which leads to lactic acid buildup everywhere, narrowing of vision, sleepiness to the point I call it “coma sleep” (I would not wake up from these even if the fire alarm went off). Tinnitus, also have muscle twitches and probably 20 other symptoms I forget.
Fast forward to today, my MCS is so bad that I cannot even read a book because the fumes from printed ink causes a reaction. My body feels toxic. Like I am being constantly poisoned.
Through the years I have spent all my available cash on trying everything I can think of. Herbs, treatments, devices, gadgets. I have found a handful of herbs and supplements that initially gave me relief, but after a few weeks always stop working. Never found a permanent solution. Always temporary, quickly followed by developing resistance.
I’ve been reading your blog for a long time, but because of the mental and physical lethargy, it took me this long to even manage a microbiome analysis.
Do you have any experience with MCS? I am fairly certain this is a microbiome issue, but I have no clue what to do, and all my attempts have been just shooting in the dark trying to see if anything would stick.
Reader in Europe
Analysis
The typical ME/CFS pattern of over representation of 0-9%ile. This is in contrast to MCS where the cause appears to be over population of a few demanding bacteria. A “normal” microbiome will have all of the Percentile ranges being about the same number.
Percentile
Genus
Species
0 – 9
72
97
10 – 19
27
21
20 – 29
13
11
30 – 39
13
15
40 – 49
10
16
50 – 59
19
20
60 – 69
15
19
70 – 79
7
17
80 – 89
11
16
90 – 99
8
13
The likely to be important for the above shift is just a single bacteria family.
And then does a Hand Picked of items deemed important (Roseburia) cited above.
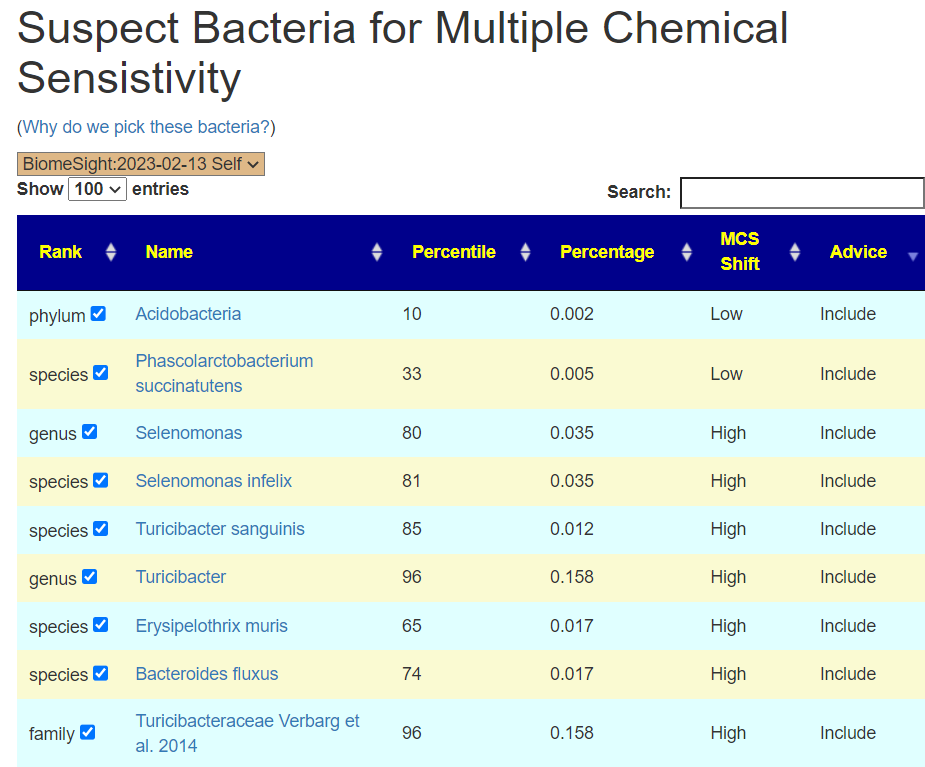
While the MCS associated bacteria above would likely be included by this, we do a fifth set of suggestions by hand picking these and getting those suggestions.
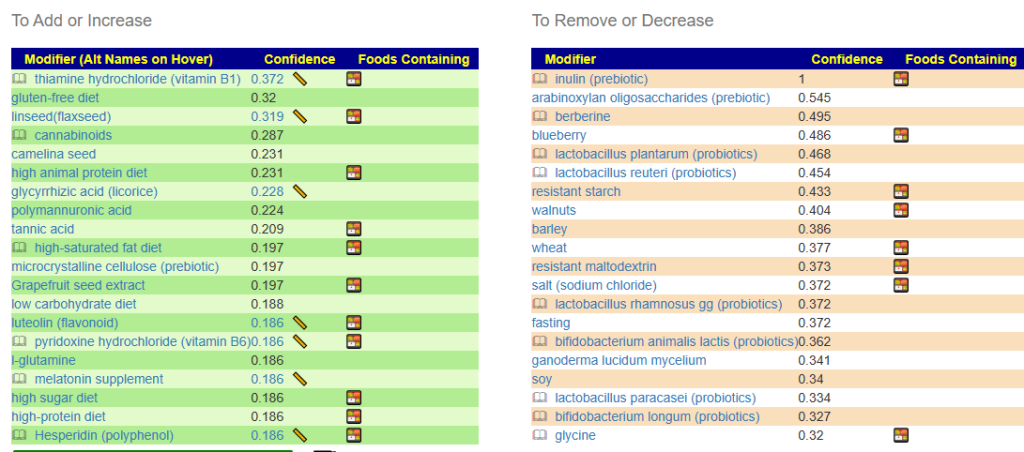
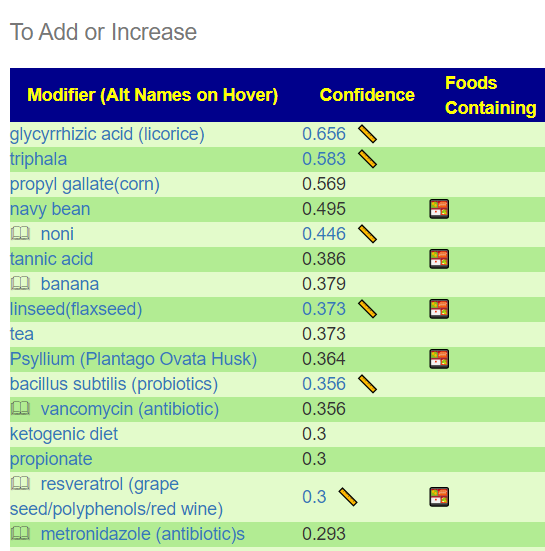
The MCS specific suggestions are below:
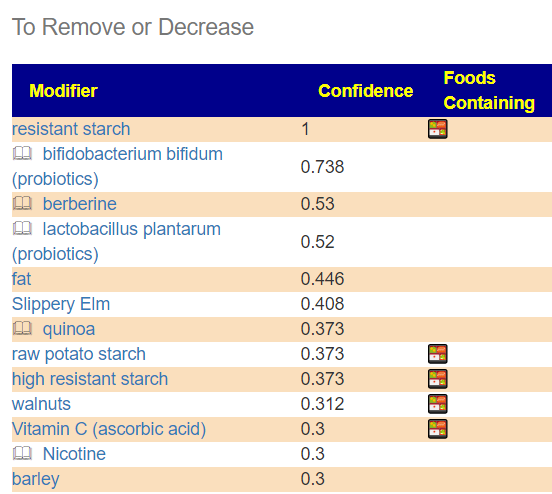
And the avoid:
Going over to Consensus
On that page, we sort by Take Count from highest to lowest. Items with a count of 5 addresses all concerns. The top of the list are:
Hoping for probiotics solutions failed to find any strong candidates. In terms of prescription items, these antibiotics are the top suggestions neomycin and lymecycline . It is interesting to note “Neomycin is not absorbed from the gastrointestinal tract and has been used as a preventive measure”[wikipedia]; so it’s impact is confined to the microbiome. Lymecycline is a tetracycline which also include minocycline and doxycycline — two antibiotics often used by ME/CFS specialists.
Reader Feedback
It looks like there’s not much to do, except perhaps antibiotics.
I was once prescribed ciprofloxacin for a lung infection, and all my symptoms went away for a couple days. They returned after the cipro course was completed. Later I’ve learned this antibiotic is very dangerous. So not very interested to test that particular type again.
Thiamine B1 I’ve found through experimentation that it helps a bit, as well as resveratrol (both listed among the text and images). High protein diet also helps, which was also listed.
A few herbal antibiotics also help, so the killing part does work. In fact the antibiotic route has always produced better results than the nutritional path. Well, at least the antibiotic route produces immediate results. Perhaps the nutritional path produces more sustainable results though, if I could figure it out.
The Lymecycline I would certainly want to test. Have to figure that out also.
It is nice to get feedback that the suggestions and the person’s experience doing multiple random experiments agree. The stated goal of Microbiome Prescription is to give better suggestion than random suggestions off the internet or ad hoc trials suggested by MDs.
As a FYI, I have always been an advocate for Cecile Jadin approach for antibiotics, single course, a break, then a different antibiotic (preferable a different family).
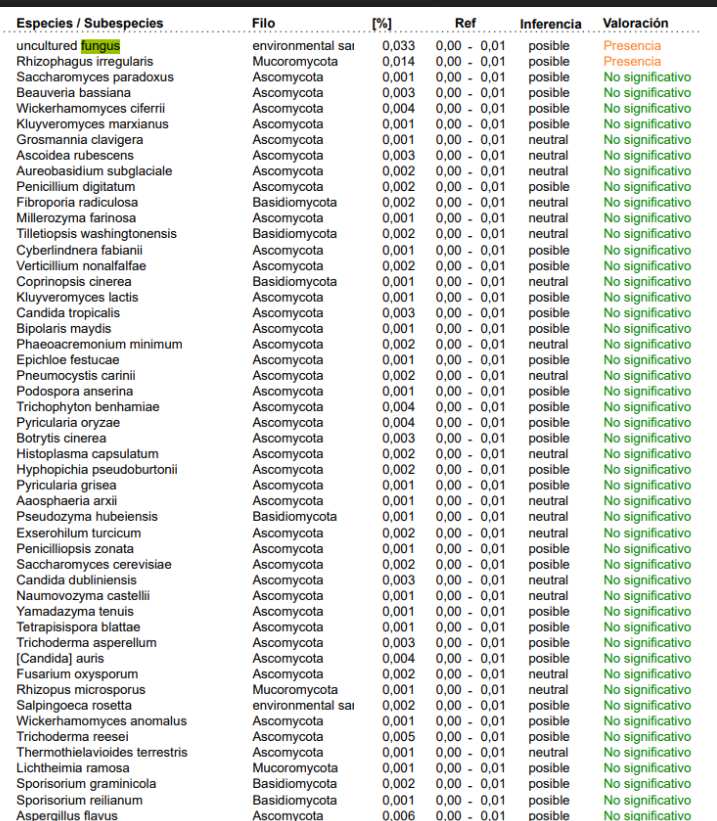
This is what is in their data file for a person (i.e. detected only) "Eukaryota","Fungi","Ascomycota","Dothideomycetes","","","","","","","","","","0.001554","0.00052608","0.0014506","77.3" "Eukaryota","Fungi","Ascomycota","Eurotiomycetes","","","","","","","","","","0.0006793","0.0017786","0.003532","2.5" "Eukaryota","Fungi","Ascomycota","Leotiomycetes","","","","","","","","","","0.0006979","0","0.0003654","90" "Eukaryota","Fungi","Ascomycota","Saccharomycetes","","","","","","","","","","0.01638","0.00071344","0.0019584","99.2" "Eukaryota","Fungi","Ascomycota","Sordariomycetes","","","","","","","","","","0.001107","0.0016878","0.0034788","18.9" "Eukaryota","Fungi","Basidiomycota","Agaricomycetes","","","","","","","","","","0.0003536","0.00054734","0.0017092","17.2" "Eukaryota","Fungi","Basidiomycota","Exobasidiomycetes","","","","","","","","","","0.0001024","0","0.00034712","52.2" "Eukaryota","Fungi","Basidiomycota","Malasseziomycetes","","","","","","","","","","0.0001582","0","0.00010162","73.3" "Eukaryota","Fungi","Basidiomycota","Tremellomycetes","","","","","","","","","","0.0002047","0.00023646","0.000608","17.9" "Eukaryota","Fungi","Basidiomycota","Ustilaginomycetes","","","","","","","","","","0.00008375","","","" "Eukaryota","Metazoa","Chordata","Mammalia","","","","","","","","","","1.985","0.0042838","0.06166","99.5"
A reader request with severe MCS motivated me to revisit Multiple Chemical Sensitivity (MCS) and literature on it. I am first going to recap my memory of what I know, a literature review, Last, analysis using data contributed to Microbiome Prescription – which did not find anything major beyond bacteria shifts that are statistically significant. We explore enzymes, products and substrates with no smoking guns found
There was a processing error — This post was revised
Long weekend tracing issue, made short. Some revisions to reduce running cost had a typo pointing one set of data (Substrate data for Samples) to the wrong lookup table to determine percentile. This has been corrected and the data audited to insure correctness.
I had mild MCS during one flare. It disappeared with remission.
Multiple Chemical Sensitivity (MCS) is not bronchial (breathing). There was a series of studies where the person was wearing a half-face mask breathing compressed air. Bringing a triggered close to the person (blind testing), trigger the response. My own wife lab results leaves a significant scent. She had a complete workup with Dave Berg, Hemex Lab and two weeks later she had a bad MCS reaction. About a week later, new blood work was sent. Everything was the same, except for a marker indicating very active coagulation. The marker had a short half-life around 2 hours. After she fully recovered, same test returned to normal. This hints at coagulation being part of the process. We did find one effective treatment for shortening the duration of a MCS episode: Olestra (as in Olestra chips). This compound sucks chemicals out of tissues [2015] [2014]
– Ken Lassesen
I attended a talk today with the AAAS (I’m a member) and Memory Cells was discuss for some autoimmune conditions. It occurs to me that these are likely a factor. These cells become uber-sensitive to specific chemical compounds and have a lasting memory. In time they may die off, but not quickly.
Caution: this post is subject to revision. The findings to date are so significant that I am posting early.
The Current Literature
First a summary from a 2022 review – it covers a lot of territory… many quotes are below
Multiple Chemical Sensitivity (MCS), a condition also known as Chemical Sensitivity (CS), Chemical Intolerance (CI), Idiopathic Environmental Illness (IEI) and Toxicant Induced Loss of Tolerance (TILT), is an acquired multifactorial syndrome characterized by a recurrent set of debilitating symptoms. The symptoms of this controversial disorder are reported to be induced by environmental chemicals at doses far below those usually harmful to most persons. They involve a large spectrum of organ systems and typically disappear when the environmental chemicals are removed. However, no clear link has emerged among self-reported MCS symptoms and widely accepted objective measures of physiological dysfunction, and no clear dose-response relationship between exposure and symptom reactions has been observed. In addition, the underlying etiology and pathogenic processes of the disorder remain unknown and disputed, although biologic and psychologic hypotheses abound. It is currently debated whether MCS should be considered a clinical entity at all.
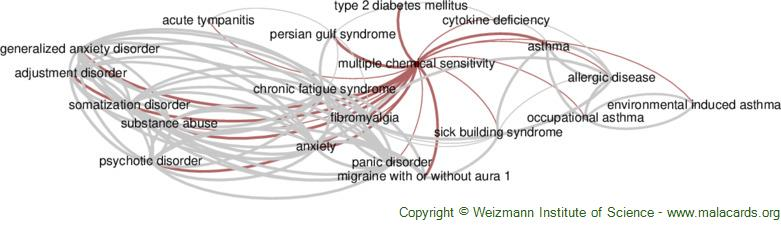
“Not surprising, MCS is often juxtaposed to, and sometimes combined with, other diseases for which definitive diagnoses and explanations are also found wanting, including fibromyalgia (FM), Gulf War syndrome (GWS), chronic fatigue syndrome (CFS), sick building syndrome (SBS), and electromagnetic radiation exposure (ERE) [18,23,24,25,26,27,28,29,30,31,32].”
“An association was documented, however, between MCS and increased nasal airflow resistance, respiration rate, and heart rate.” [2021] Volatile chemicals can not only affect respiration, but can cause laryngeal symptoms which, in the extreme, can induce vocal cord dysfunction [82].
Changes in skin conductance were also seen in MCS patients but not in controls [193].
Compared to younger persons, those 65 years of age and older are less likely to identify themselves as chemically sensitive [88].
In accord with this concept, McKeown-Eyssen et al. [219] found, in a female cohort of 203 MCS cases and 162 controls, that the cases had higher levels of cytochrome P450 CYP2D6 (i.e., one of the most important enzymes involved in the metabolism of xenobiotics in the body) and n-acetyl transferase 2 (NAT2). More possible genes listed here.
Like the sick building syndrome [89], there is a remarkably higher prevalence in women than in men [16,18,21,90,91], with the percentage of women ranging from 60% to 88% [18,57,92,93,94].
Almost every condition in the above chart has microbiome shifts associated with it. Exposure to mold also is known to cause microbiome shifts. There appears to be no published studies exploring this possibility. At this time we have 128 people (7.3%) who have annotated their samples with Multiple Chemical Sensitivity [uBiome: 55, Ombre:39, Biomesight 25] to Microbiome Prescription.A
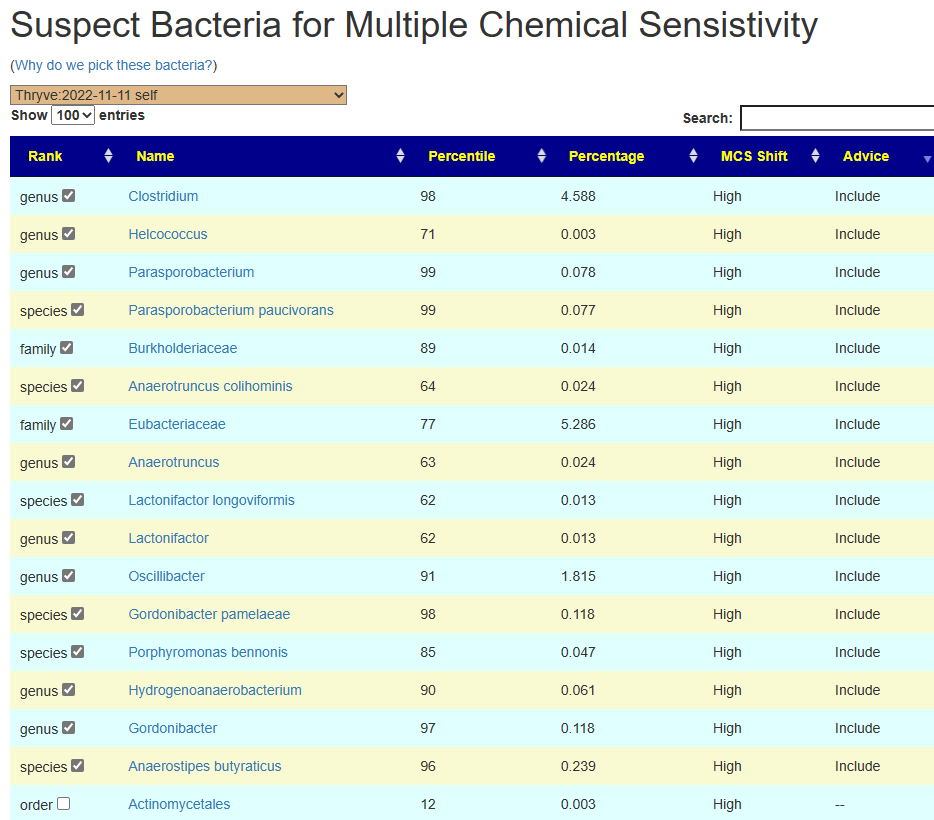
Executing analysis by lab, we found only one taxon reported significant in two labs. Bacteroides clarus where people with MCS had 3x the count of people not reporting MCS [BiomeSight, uBiome]. The top items of significance are shown below. All of them have much higher counts in people with MCS.
Source
probability
Tax_Name
tax_rank
with MCS
without MCS
Obs
BiomeSight
P < 0.001
Anaerotruncus
genus
3356
1834
683
BiomeSight
P < 0.001
Anaerotruncus colihominis
species
3208
1743
683
BiomeSight
P < 0.001
Bacteroides intestinalis
species
28980
2430
396
Thryve
P < 0.001
Prevotella maculosa
species
27399
5733
404
Average Counts out of a million
These have been added to the [Research] tab, as shown below.
Looking at KEGG Enzymes we have the strongest candidates below. Looking for any enzyme that is significant for 2 or more labs, we had only one: 5.3.1.15 D-lyxose aldose-ketose-isomerase (Biomesight and Thryve).
Trying a different approach aggregating all of the data and using percentile ranking. This masks most of the differences between labs and gives us large sample size, We have a very actionable item: increase Bifidobacterium by taking Bifidobacterium probiotics.
tax_name
tax_rank
percentile
Obs
Alistipes indistinctus
species
61.7
61
Anaerobutyricum hallii
species
39.8
41
Bifidobacteriales
order
37.7
106
Bifidobacterium
genus
37.1
122
Oscillospiraceae incertae sedis
norank
63.1
41
Acidobacteria
phylum
33.2
48
Butyricimonas faecihominis
species
61.2
43
Bifidobacteriaceae
family
37.4
122
Collinsella aerofaciens
species
39.1
83
Phascolarctobacterium succinatutens
species
37.3
52
Hungateiclostridiaceae
family
61.4
45
Bacteria where Percentile Average above 60%ile or below 40%ile
KEGG Enzymes
Applying this to KEGG Enzymes, we have just one of concern that is high: EC3.2.1.46 galactosylceramidase, and a big 39 that are low indicating a deficiency of enzymes is likely
Enzymes where Percentile Average above 60%ile or below 40%ile
Compound Produced
This is reflected in compound produced. With D-Galactose being the only high – matching enzyme [3.2.1.46] D-galactosyl-N-acylsphingosine galactohydrolase above,
CPID
Compound
percentile
obs
924
Ferrocytochrome
36.9
63
22336
Reduced hydrogenase
38.3
121
250
Pyridoxal
38.6
98
15767
4-(L-gamma-Glutamylamino)butanoate
38.7
63
16699
2-O-(6-Phospho-alpha-mannosyl)-D-glycerate
38.7
94
1113
D-Galactose 6-phosphate
39.2
118
196
2,3-Dihydroxybenzoate
39.3
73
4575
(4R,5S)-4,5,6-Trihydroxy-2,3-dioxohexanoate
39.5
72
615
Protein histidine
39.6
122
666
LL-2,6-Diaminoheptanedioate
39.7
122
1097
D-Tagatose 6-phosphate
39.8
115
20890
D-Glucaro-1,5-lactone
39.9
61
20889
D-Galactaro-1,5-lactone
39.9
61
124
D-Galactose
63.5
65
Compounds Consumed
As above for production and for bacteria, we have just one item with a high percentile and many with a low percentile.
CompoundName
percentile
Obs
Galactosylceramide
63.9
65
5-Oxoproline
39.9
120
Hydrogen selenide
39.9
122
3-Dehydro-L-gulonate
39.9
72
Reduced riboflavin
39.8
50
Protein N(pi)-phospho-L-histidine
39.6
122
5-Aminopentanoate
39.6
106
[SoxY protein]-S-disulfanyl-L-cysteine
39.6
43
(L-Seryl)adenylate
39.6
60
(2S,3S)-2,3-Dihydro-2,3-dihydroxybenzoate
39.6
73
6-Phospho-beta-D-galactoside
39.5
117
Sucrose
39.4
122
Hippurate
39.4
63
alpha-D-Galactose 1-phosphate
39.4
122
2-Hydroxy-3-keto-5-methylthiopentenyl-1-phosphate
39.4
52
D-Galactose 6-phosphate
39.3
115
4-Aminobutyraldehyde
39.3
47
D-Xylulose 5-phosphate
39.1
122
Benzene-1,2,4-triol
39
43
L-Arabinonate
38.6
52
Pyridoxine
38.6
98
Salicylate
38.3
44
dTDP-4-acetamido-4,6-dideoxy-alpha-D-galactose
38.3
60
Oxidized hydrogenase
38.3
121
3,4-Dihydroxyphenylacetate
38.1
47
Thymine
37.8
45
FMN-N5-peroxide
37.8
45
FMN-N5-oxide
37.8
45
Ferricytochrome
37.4
63
Hexadecenoyl-[acyl-carrier protein]
37.2
47
Protein lysine
37.1
120
2-O-(alpha-D-Glucopyranosyl)-D-glycerate
37.1
54
L-Rhamnonate
36.7
46
Geraniol
36.4
49
4-(L-gamma-Glutamylamino)butanoate
36.3
44
D-Glyceraldehyde
35.6
60
3-Hydroxybenzoate
35.3
41
(2R)-3-Sulfolactate
34.1
43
D-Glucaro-1,4-lactone
33.3
43
D-Galactaro-1,4-lactone
33.3
43
Bottom Line
The is no obvious imbalance between compounds produced and consumed. Thus the best path is to use the bacteria identified at the start. A quick select has been added to the menus.
There are a few things that could be factors, for example D-Galactaro-1,4-lactone is 33.3%ile for consumption and 39.9%ile for production. Unfortunately, the microbiome is not a closed system and whether any surplus accumulates would be too speculative.
Example of the MCS pick page for a person with MCS.
I heard from a group of long covid patients that you’re offering specific recommendations after they provide you results from a microbiome sample analysis. Would you happen to still be offering those?
My partner and I have had covid 8 times, and unfortunately have over 20 cardiovascular, neurological and pulmonological long covid symptoms. I had my sample analyzed through BiomeSight(attached below).
Happy to follow any process that you may have for this.
Posts are done usually on a first come, first serve basis — usually within 2 weeks.
I do not do private consults. I am not licensed to provide medical advice. I am a statistician and Artificial Intelligence engineer.
If you choose to share the post with your Medical Professional and they are interested in discussing the post with me on a zoom or equivalent call, I will make the time. My temperament is to teach and share knowledge.
There is no cost. If the suggestions work, feel free to buy me a coffee as a thank you.
I am doing a more detail analysis first. While similar to other ME/CFS samples (i.e. over representation of bacteria in the 0-9%ile range), we do not have the under representation in the 90-99%ile range.
Percentile
Genus
Species
0 – 9
64
94
10 – 19
6
11
20 – 29
10
15
30 – 39
15
18
40 – 49
15
17
50 – 59
19
20
60 – 69
19
31
70 – 79
19
31
80 – 89
26
39
90 – 99
46
40
The Likely Key Bacteria Causing Above show two genus, both with relatively low importance (Usually there is at least one over 3.5).
Going over to Bacteria deemed Unhealthy, we see a likely why for getting COVID eight times! Two bacteria have been associated with getting COVID from studies. This suggests that the chemicals produced (or consumed) by these bacteria creates a friendly environment for the virus
Looking at Dr. Jason Hawrelak Recommendations, we are at 95.6%ile with almost the not ideal being too low (which is likely caused by Ruminococcus and Oscillospira taking excessive space in the microbiome).
I usually send early and second drafts to readers to improve posts. Some of the questions sent are:
I was incorrectly under the assumption that antibiotics and antivirals will always kill beneficial and detrimental bacteria, until I read your Antibiotics will kill everything — Not article. I have taken azithromycin injections on average 3x a year and 5 courses of 2 month long doxycycline cycles over the past 6 years. My question is, can we infer from the data as to how long one should take antibiotics like doxycycline or azithromycin? My presumption is that regular microbiome samples should be taken 1/mo, ideally 1/week, until bacteria populations affected by these drugs are in optimal ranges. What are your thoughts?
Most antibiotics come from nature and usually from a bacteria that tries to reduce competitors. Usually they are discovered because it is effective against a troublesome bacteria (and ignore side-effects on anything else).
When to stop is a complex question. There are a variety of ways that a bacteria is “gone” but hibernating. My attitude is to take just one course if there is a specific infection. The goal is to knock the bacteria back sufficiently that your natural immune system can take over the fight. For changing a dysfunction microbiome where there could dozens of different bacteria in the cartel, I favor Cecile Jadin approach of alternating types of antibiotics with 7-10 days on and 20 days off between each course. It seems to be more effective against antibiotic resistance that often develops when the same antibiotic is regularly used. I have seen studies on sewerage treatment confirming this.
There is no “optimal range” IMHO, there are “typical ranges” with the problem that different folks will use different methods to determine those. I favor the Kaltoft-Moldrup ranges. See The problem with “official” ranges from labs.
Do you have an article or any other info on the Cold Extremities symptoms caused by particular microbiome signatures? This issue has plagued me all my life and I’d really like to fix it if you have any suggestions on places to look.
I do not recall doing anything specific because there can be multiple paths to this symptoms. Some obvious ones:
Some forms of coagulation or vascular constriction issues that results in slow blood flow. Your saturated Oxygen Levels may be fine, just heat loss from taking too long to reach the extremities. This can also occur with inflammation.
This was the case for me. A genetic defect caused thick blood — my particular defect was easy to compensate for.
Hypothyroidism is another possibility
I am currently taking OMNi-BiOTIC(sold under AllergoSan USA) Stress Release pre and probiotics everyday, alongside a prebiotic called Omni Logic Plus. I saw that your report mentioned “Avoid Probiotic Mixtures”, so I will be reevaluating this strategy. – One scoop of the Omni Logic Plus prebiotic contains 1g of Fructo-Oligosaccharides and 1g of Galacto-Oligosaccharides, and causes me intense, painful symptoms of bloating for 24 hours. -The Simple Suggestions sheet recommends 15gm FOS and 10gm GOS daily. Do you think I should be experiencing bloating alongside these prebiotics, and how should I work up to 15gm/10gm? What exactly is happening in the microbiome when this ramping of prebiotics occurs?
Remember these are suggestions only, many suggestions!! Since it causes painful bloating, I would not do.
The dosages are UPPER LIMITS that are deemed safe (has been used in clinical studies). The purpose is to show what may be therapeutic levels are. See this page. Often people dosages are closer to homeopathic than therapeutic. 🙁 . Then we hear on forums “I tried it and it did nothing”
You may wish to get the Oligosaccharides directly from food and not as supplements. This is always my preference.
Some of these suggestions counteract each other, such as Mutaflor e.coli probiotics (Germany), and doxycyline. Do you recommend prioritizing one or the other first?
See Suggestions Contradictions — Limits of Certainty for why contradictions occur. My usual preference is natural substances over prescription, second item is availability. If you can get a MD to prescribe an antibiotic while you wait for Mutaflor or Symbioflor to arrive — then the sequence resolves itself.
One thing to remember is this: We want to destabilize the bad microbiome. Doing everything at once will likely gain some ground initially but you then get stuck in trench warfare as the other side learns how to respond. I usually suggest breaking suggestions into 4-8 lists of 1-2 weeks duration and just rotate what you take. I refer to this as the resistance approach. It worked for the Americans against England in 1776, French Resistance against Nazi Germany, and Vietnamese (Viet Kong) against Americans in Vietnam, and Afghanistan against the British, Russia and the US. No great victory just constant small ones.
I noticed that you recommend high dose B1 Thiamine at 1.8gm/day and a high protein/low fat diet overall. I understand that there’s a variety of other dietary suggestions here, but would you recommend that a purely carnivore diet be tried? Have you noticed the carnivore diet having any permanent beneficial impact on the microbiome?
Short answer, B-vitamins are often nicknamed “Beef-Vitamins” because that is where most can be sourced from. On the flip side, getting the vitamins out of the beef, depends on stomach acid and what bacteria are there.
You can use the food site, to see how much B12 and B6 are in various foods. 100 grams of beef liver (3-4 oz) gives 0.13 mg of B-12. It is unlikely you will get therapeutic dosages from eating beef.
My usual advice is to do things for 4-8 weeks and then retest. You are sailing your microbiome to safer waters though an archipelago. The winds and the charts will often require many course corrections.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
I have been suffering from fatigue for about 8 months now and would like your advice. I have seen multiple doctors now and they have not been able to figure anything out despite running multiple labs. My fatigue started around August of 2022 when I was put on antibiotics. I had an infected wound from a martial art that got infected. After that, I got c diff from a friend I had been taking care of, so in late August I was put on another course of antibiotics. Then in September I got c diff again and was put on another course of antibiotics. My fatigue became very severe at this point. I could barely make it out of bed, etc. I still have fatigue now. I can walk around but I get tired pretty easily. I still cannot go to the gym or exercise. Just the thought alone of pushing my body seems tiring. Please assist.
Antibiotics can be good or bad. Each type alters the microbiome in different manners. Recently I added a new tool to help people negotiate with their MD to find the best candidate antibiotics that will address the MDs concern while looking at their microbiome impact (which is not an area they are knowledgeable). See this video for more information. What has happened, happened — let us move forward.
The antibiotic given were:
Cephalexin (Keflex, Daxbia) for the wound – which I lack any significant information on
Dificid (A Macrolide, fidaxomicin) for c diff
Analysis
First, we see the type of distribution often seen with Chronic Fatigue Syndrome and Long COVID — two conditions with fatigue being a signature symptom. Many many token genus and species.
Percentile
Genus
Species
0 – 9
77
99
10 – 19
22
27
20 – 29
8
8
30 – 39
13
12
40 – 49
5
10
50 – 59
9
15
60 – 69
6
13
70 – 79
5
15
80 – 89
7
7
90 – 99
3
5
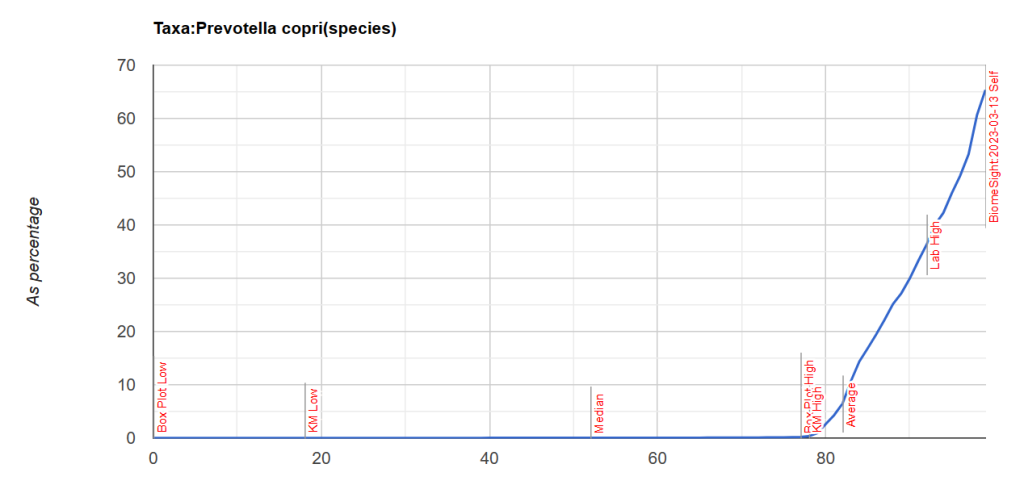
This tool also flags the bacteria that may be causing it. What was flagged is shown below — through the roof on these one bacteria (parent-child), This is known to be a very pro-inflammatory bacteria. It is 61% of the microbiome!! It is strongly associated with rheumatoid arthritis [2013] [2023] [2019]. High levels also may indicate mycotoxin (fungi) is present in the environment (house, places he goes) or person [Citation]. For more information see this excellent summary.
Looking at Potential Medical Conditions Detected, we had 12 items – which is to be expected with this type of shifts, and we will ignore. It is interesting to note that Dr. Jason Hawrelak Recommendations are at the 99.7%ile — with all of the ones with issues being too low which is expected from one bacteria over-whelming the microbiome.
Antibiotics
There is a lovely study from [2013] that reports on antibiotic resistance of Prevotella copri [Table 1]. It states “suggesting that resistance to these antibiotics amongst Prevotella … microbiota is not intrinsic, but selected by previous antibiotic treatment”. Which suggests that the multiple courses in a short period of time contributed. I have no data on the two antibiotics that he took.
This hints that taking additional antibiotics may be ineffectual.
If blood tests for fungi has not been done, it should be suggested to the treating physicians.
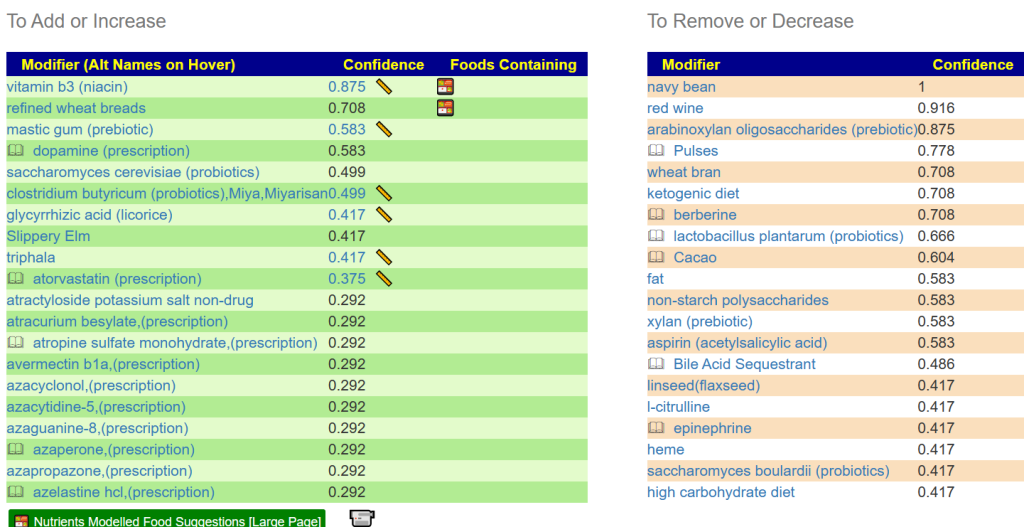
We have an elephant in the Igloo! Let us address this item first. Then retest after a few weeks. I asked for suggestions including antibiotics, shown below.
The top items
A good start would be Vitamin B3 (niacin). Which can cause flushing (i.e. white skin going lobster red), so a low dosage of 100 mg/day and increasing slowly. The other non-prescription items of note are:
.Should I do anything other than add b3, mastic gum, licorice, etc to my diet? Do I need to alter my diet in any way to lower the prevotella copri count? My diet right now is pretty bad. Burgers, pizza, etc. I went keto for a couple weeks a few months back to see if it made a difference and it didn’t so I figured if I was going to be miserable, I might as well enjoy what I eat.
From reader after reviewing above.
First the BAD NEWS, Keto is known to increase Prevotella copri, so the no positive impact is not unexpected. More BAD NEWS – what you are eating (high fat foods) will likely have adverse effects.
Above I focused on the Elephant, let us look at the ants and mice in the igloo. This is very easy to do and I made a video of it below.
Bottom line, cut out beef that are high fat content — lean beef only. Burgers and Pizza both use cheap high fat beef. Shift to rice for your source for starch (There are rice based pizza available). No soft drinks or sweets (cut sugar way down – sugar withdrawal can be rough).
Follow up: I would suggest doing a retest after 6 weeks of trying to alter your microbiome with the above suggestions. This will give us data to do your next “diet correction”. It is usually a multi-leg journey back to health.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
I get a few emails asking about apparent contradictions from Microbiome Prescription AI Engine. With the new “Just give me suggestions!” option, they have been reduced — this post explains the root issue of these conflicts. It does not solve the issue — only time and a lot more published studies will resolve it.
Data From Studies
The data entry attempts to keep true to what is actually reported in the studies on the US National Library of Medicine. A simple example, the following are subjects of different studies:
Grape seed extract
Grape polyphenols
Grape Fiber
Resveratrol
Grapes
Red Wine
Red wine polyphenols
It is human nature to try to consolidate information. There are numerous historic examples where such consolidation failed. A simple one is that all antibiotics are the same. In some nations, antibiotics are over the counter — so if you have an infection like tuberculosis, some people would walk in and buy the cheapest antibiotics expecting it to work. It is no surprise that it would have no effect. “They are almost the same” is not an approach that I subscribe to.
The second aspect of studies is that they report on different levels of the bacteria hierarchy, and rarely report on multiple levels. In some cases, the report is only on the highest levels.
And there are strains below these levels
When looking at your sample. You may be high at the genus level but normal in the family and order levels. So data from studies about what is impacted at the species, family, order or class level may be ignored. Some people, including medical practitioners, may consolidate this information and after reading one study that mentions a genus apply that to all related species, family, order or class — occasionally to the phylum level. The human tendency to consolidate information strikes again.
Last, the study may have been done on people with a specific condition or type of diet. Diet is often based on location in the world: India (many eat no meat), America (lots of junk food), China (high rice content). The shifts seen with some modifiers with different conditions or diets are different and sometimes in opposite directions. We may not get consistent studies. The human tendency to consolidate information by deeming everyone to be the same strikes again.
Below we have seven similar items — but very different information on what the studies report on.
Sum of Count
Column Labels
Row Labels
class
family
genus
norank
phylum
species
subspecies
grape fiber
3
1
grape polyphenols
13
3
grape seed extract
1
8
1
grapes
1
3
9
6
red wine
12
28
1
169
3
red wine polyphenols
5
1
3
resveratrol
40
72
1
6
114
6
Grand Total
2
55
138
3
6
297
9
Pivot Table of current data in the data store with explicit citations
While they are similar, there are difference between them that may be significant. One contains sugars, another contains fiber, another contains alcohol — these minor differences can alter different bacteria significantly.
This is why you may see apparent contradictions in suggestions. We a have a mixture of information about your microbiome and each of the above is a sieve of different mesh and fabric.
I choose not to consolidate information. I keep the information as reported. A medical practitioners is not able to keep all of this information in their head. They will proceed to consolidate, and consolidate and simplify – the art of medicine. The Artificial Intelligence Engine is the result of processing over 41 Gigabytes of information — that is likely far more than any medical practitioners had actually read in their career. Is the detail needed? That’s a personal judgement. I prefer to have it. Using AI, I can work with all of the information available without needing to consolidate or simplify.
When there is a contradiction – which should I choose? My standing answer, is avoid the substance. We do not know with confidence what the outcome may be. On the other hand, I often seen suggestions reinforcing each other — for example Positive: Gluten Free, Negative: Wheats.
We do not want to take gambles with our health — keep to where there is consensus.
“Just give me suggestions”
This picks common items often seen on the internet for a variety of conditions. When there are “similar” items, the one with the most data will usually be selected. It gives higher confidence. These choices are evolving as I review the data.
The intent is avoid showing contradictions, and work where we have the most data. It’s a simple best path forward.
It has been a year since I had Covid-19 I started to deteriorate after it and fell into a limbo of not having the energy to do anything and move on with treatment, I have gave up supplements, antibiotics, probiotics not taking anything, even if I had them in stock, pretty dire, even had very dark thoughts from nowhere that life is not worth living. I got cervical instability diagnosis in 2020 and the Covid-19 infection that made me abandon the microbiome manipulation road, a very bad decision when I look back now. I got diagnosed with a possible mast cell disorder, MCAS is much more worse then CFS, I got a reaction in airport in September 2022 wanted to travel to Italy for a consultation, reacted to fumes in airport was unable to board the plane, almost called the ambulance, the MCAS appeared after Covid-19. I am taking a H1 and H2 for it, and used to take sodium cromoglicate but I got insomnia from it, doctor here told me I am the first patient that has gotten insomnia from sodium cromoglicate. The interesting thing my cognition improved but my physical state deteriorated, I got POTS.
I have also started a YouTube channel to share my story and to keep me motivated to continue:
To recap what Covid-19 in 2022 infection gave me and I still have:
-Insomnia
-Lack of motivation
-POTS
-New food intolerances
-Reaction to the environment(possible MCAS)
-Easy bruising(now afraid to take “thick blood” supplements)
-High cholesterol and triglycerides
From Reader
Questions from Reader
First, the site does not diagnosis — it is based on association. What is association? It just means that two things tend to happen at the same time. Sometimes there is a real connection — other times the connection is due to other factors. For example, the number of children in a family has declined over the last 50 years. The usage of the internet has increased. There is a statistical association between the two but it does not mean that internet use causes less kids, nor does it mean that having less kids mean more internet use (which may actually be true!).
Does it show I have POTS, I attached my CellTrend result which is positive for POTS
You only have a 10% match to bacteria seen in other people who have reported POTS. So, if it is POTS, it is likely atypical POTS.
I do NOT see on the CellTrend results any thing about POTS. Was it a MD’s opinion based on ???
Does it give avoid food all casein and lactose foods and nuts, I have attached my IgG intolerances testing
No, it does not deal will allergies. It suggests food that are likely to positively or negatively impacts the complete microbiome.
Analysis
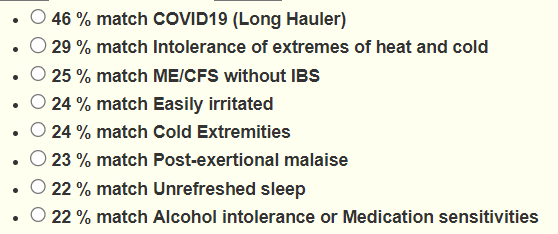
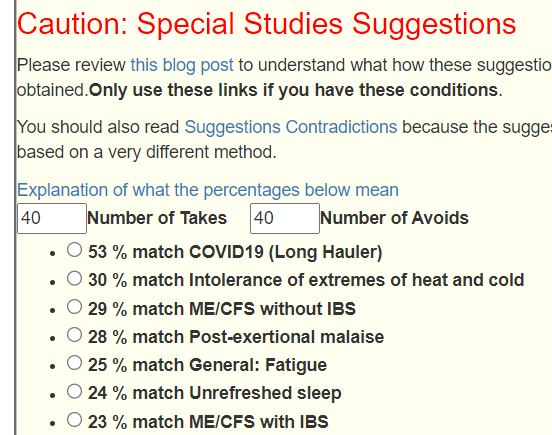
Going over to Special Studies, COVID Long Hauler leaps out!! It is the best description of the current state. This appears to be common pattern of ME/CFS people Post COVID: The signature of Long COVID dominates over ME/CFS. This may be due to the variation of bacteria over time with ME/CFS. With a recent case of COVID, there is much less variation and thus a stronger signature is found.
Looking at the distribution of bacteria by percentile, we do not see the count for each range being close to each other (expected result for a “normal’ microbiome). The 0-9% is only 32% instead of expected 10%, which is less than other samples that I have seen at 60%.
Percentile
Genus
Species
0 – 9
72
79
10 – 19
17
28
20 – 29
14
15
30 – 39
20
32
40 – 49
24
24
50 – 59
20
22
60 – 69
13
20
70 – 79
14
19
80 – 89
9
7
90 – 99
8
12
Below this on the page (added on April 1, 2023) are “Likely Key Bacteria Causing Above”
This now rolled into a single click! “Just give me suggestions” – It results in the short dumb down list with links to the full details. See the video below.
I could start digging into the symptoms and other issues cited above, but with the Long COVID signature being so strong let us not over-engineer. We have a course for the first leg of recovery.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
This is a change from the usual microbiome. The microbiome has impact on getting cancers and on the effectiveness of various treatments. A little bit of recent literature is below.
Colorectal cancer (CRC) is associated with gut microbiota dysbiosis. [2022]
The role of the bacterial microbiome in the treatment of cancer [2021]
This person is atypical — they find the markers for cancer, but cannot locate where it is. We see a large number of bacteria with only token representation (0-9 Percentile). Statistically, you would expect each of the ranges below to have similar numbers.
Percentile
Genus
Species
0 – 9
73
91
10 – 19
16
14
20 – 29
14
21
30 – 39
19
20
40 – 49
12
21
50 – 59
16
18
60 – 69
8
23
70 – 79
11
27
80 – 89
33
20
90 – 99
22
32
The new feature “Likely Key Bacteria Causing Above’ show items of concern:
From the Potential Medical Conditions Detected, we see gut disturbances (Gastroesophageal reflux disease (Gerd) including Barrett’s esophagus, Histamine Issues,Mast Cell Issue, DAO Insufficiency) as well as neurological impacts (Brain Trauma, Epilepsy).
Looking at Bacteria deemed Unhealthy, we have the following with significant counts and percentiles.
Remember they are suggestions — just pick items that you can afford, can get, and that you are happy taking.
The list of items to take was actually surprising. It was a large list with all 4 sets of suggestions saying take (over 110!) . The top items are below
foeniculum vulgare (Fennel)
Curcumin
Vitamin B-12
syzygium aromaticum (clove)
Hesperidin (polyphenol)
garlic (allium sativum)
nigella sativa seed (black cumin)
Caffeine
thiamine hydrochloride (vitamin B1)
oregano (origanum vulgare, oil)
Arbutin (polyphenol)
diosmin,(polyphenol)
pyridoxine hydrochloride (vitamin B6)
retinoic acid,(Vitamin A derivative)
thyme (thymol, thyme oil)
luteolin (flavonoid)
kefe cumin (laser trilobum l.)
neem
On the avoid list we have many items which for other people tend to be on their take list
Going over to the Food site, we see the following items near the top: Kidney, marmite, Cream of Wheat. The main reason is that they are high in B vitamins.
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
Recent Comments