This is an update Jason Hawrelak Criteria for Healthy Gut. His criteria is based on percentages and used by medical practitioners around the world. I have three significant collections of samples and decided to find out how these percentages translate to percentile for each lab.
They are similar and not similar. For example 50% of people will have low Akkermansia using uBiome while Biomesight increases it to 77%. Alistipes — are never out of range for Biomesight while 90% of people using uBiome would be too high.
Taxa Name
Taxa Rank
Percentage
uBiome Percentile
Ombre Percentile
Biomesight Percentile
Akkermansia
genus
1 – 5
48 – 80
71 – 91
77 – 93
Alistipes
genus
0 – 0.3
0 – 10
0 – 33
0 – 100
Bacteroides
genus
0 – 20
0 – 32
0 – 48
0 – 45
Bacteroidia
class
0 – 35
0 – 24
0 – 40
0 – 45
Bifidobacterium
genus
2.5 – 5
78 – 91
78 – 87
90 – 95
Bilophila wadsworthia
species
0 – 0.15
0 – 32
0 – 43
0 – 44
Blautia
genus
5 – 10
15 – 60
32 – 72
24 – 69
Desulfovibrio
genus
0 – 0.15
0 – 46
0 – 42
0 – 72
Escherichia coli
species
0 – 0.1
0 – 100
0 – 75
0 – 88
Eubacterium
genus
0 – 15
0 – 100
0 – 99
0 – 100
Faecalibacterium prausnitzii
species
10 – 15
80 – 95
50 – 69
46 – 69
Fusobacterium
genus
0 – 0.01
0 – 40
0 – 66
0 – 72
Lactobacillus
genus
0.01 – 1
23 – 93
9 – 75
46 – 99
Methanobrevibacter
genus
0 – 0.01
0 – 7
0 – 33
0 – 33
Oxalobacter
genus
0.01 – 1
0 – 100
38 – 100
35 – 100
Prevotella
genus
0 – 25
0 – 100
0 – 89
0 – 88
Pseudomonadota
phylum
0 – 4
0 – 52
0 – 76
0 – 54
Roseburia
genus
5 – 10
51 – 86
85 – 96
81 – 95
Ruminococcus
genus
0 – 15
0 – 100
0 – 98
10- 95
This post is intended to illustrate that percentages cannot be determined by one lab and applied to another. Percentile appears to be more robust.
There are generations of approaches. Often limited to the knowledge available at the time
Generation #1: Eat Fermented Foods as a Cure All
This dates back millennium in the east and the west. It helps some, and thus is validated as working (for some at least). For example, Garum in ancient Greece
Generation #2: Yogurt and Probiotics
In western culture, The Russian biologist and Nobel laureateIlya Mechnikov, from the Institut Pasteur in Paris, was influenced by Grigorov’s work and hypothesized that regular consumption of yogurt was responsible for the unusually long lifespans of Bulgarian peasants.[25] Believing Lactobacillus to be essential for good health, Mechnikov worked to popularize yogurt as a foodstuff throughout Europe. [Wikipedia]
There are several generation of technology involved here.
“A significant difference in gut microbial composition between SARS-CoV-2 positive and negative samples was observed, with Klebsiella and Agathobacter being enriched in the positive cohort.”
These studies indicates an increase or decrease in the average for populations. There is no thresholds where the odds change nor relative magnitude. This is further complicated by non-replication by other researchers — the reason is often because on non-standardization of microbiome analysis
Generation #4: Lab Specific Shifts with critical levels and contributions
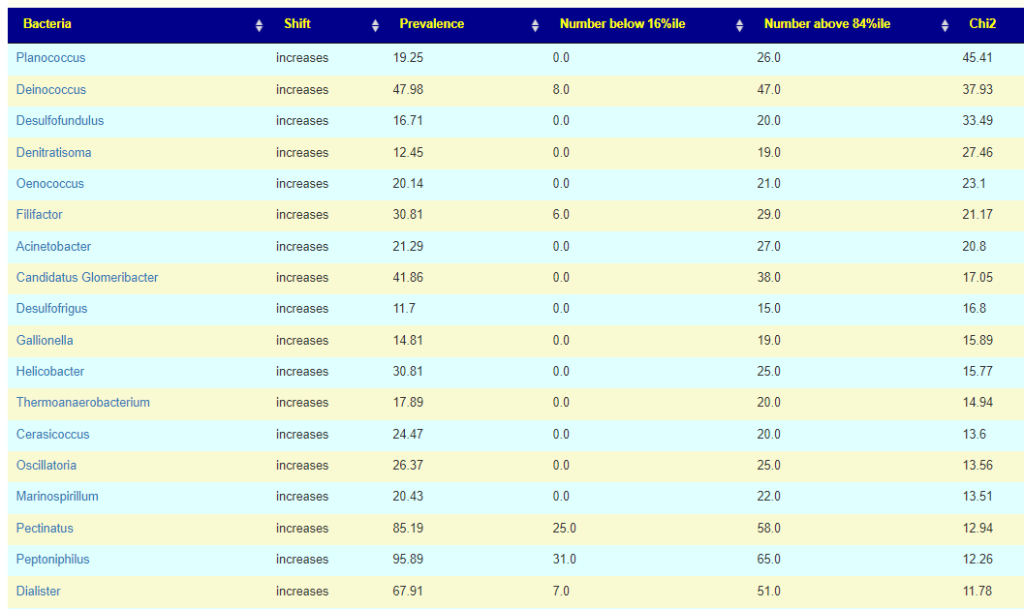
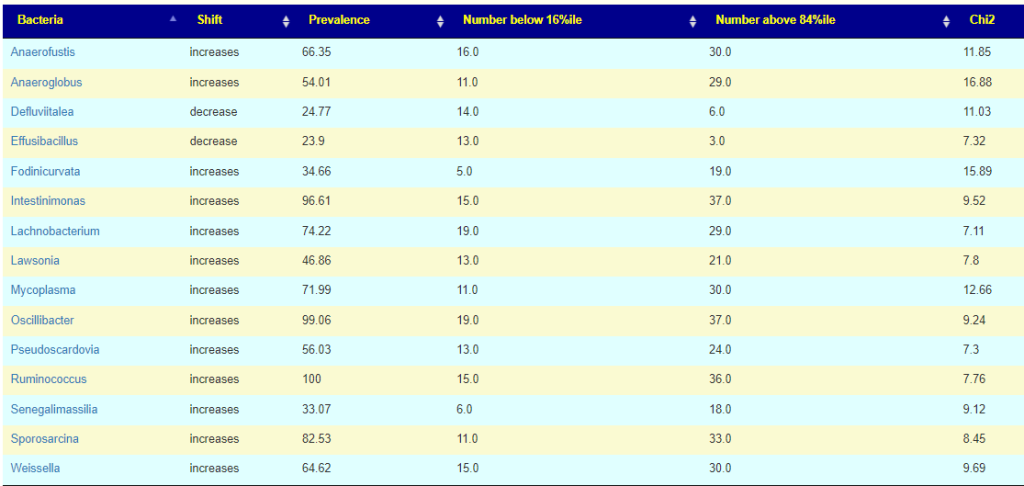
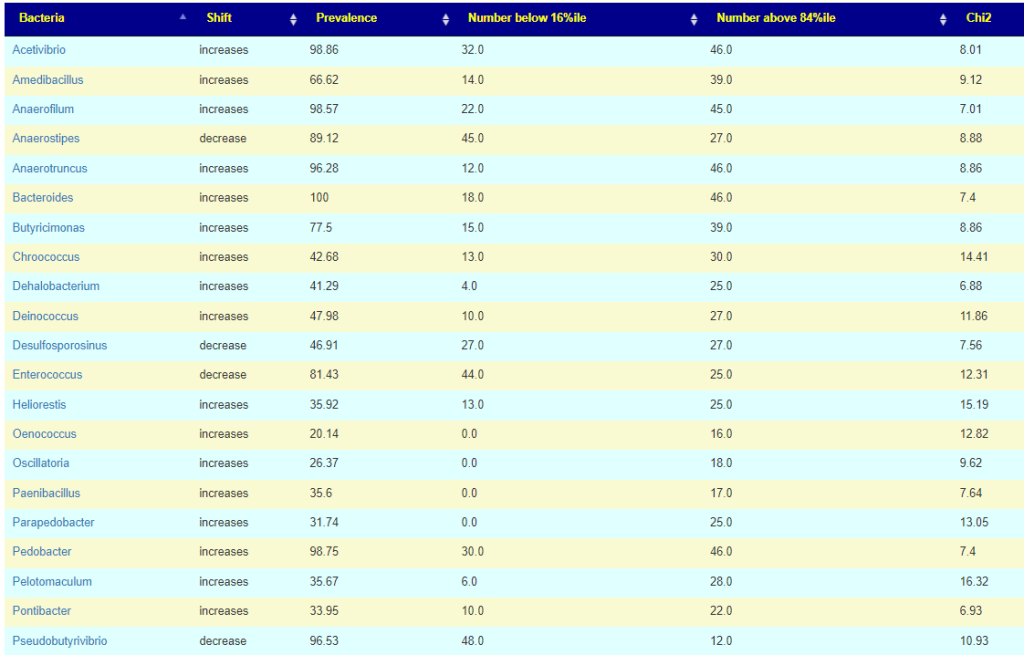
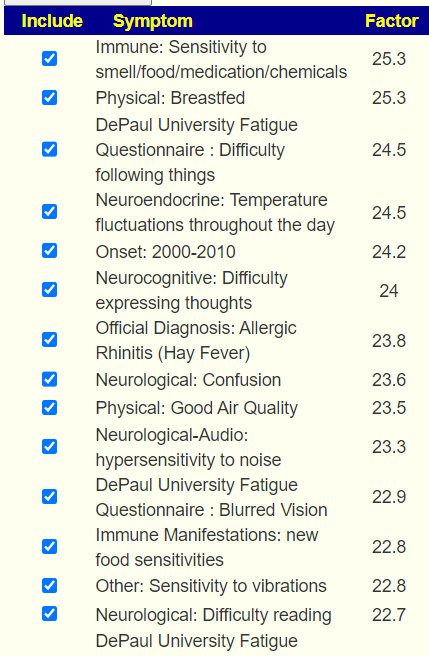
Using large dataset and techniques such as those described in Symptoms with Ability to Predict from Microbiome Results. We have the ability to set threshold and determine the relative importance. The table below is for Long COVID based on one lab’s pipeline. We can easy see the pattern — often, it is a relatively rare bacteria(low prevalence) that is seen in significant levels in Long COVID patients
This allows identification of the genus (or other ranks) that may be ascribe to the condition if over the 84%ile. It also allows the relative importance of each to be evaluated since there may be multiple targeted bacteria. Chi2 value is a reasonable proxy for importance.
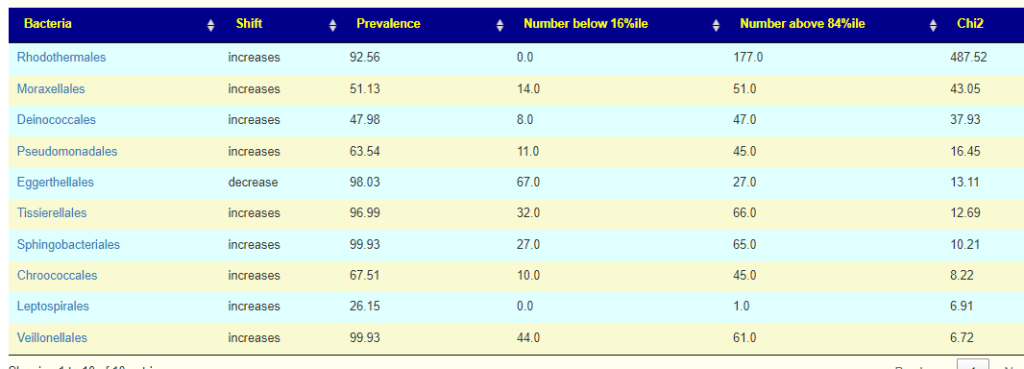
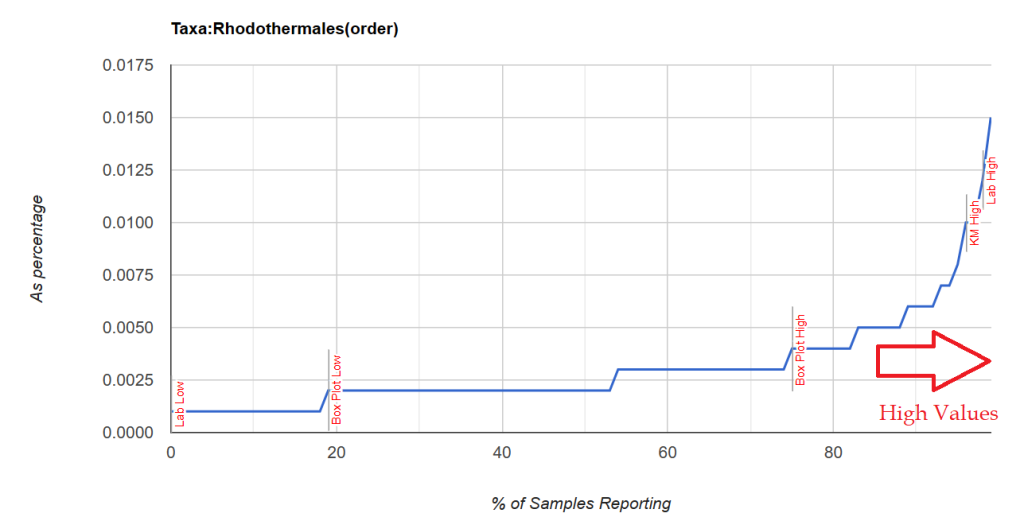
Moving up the taxonomical rank, we see at the ORDER level that one order is really significant.
Bottom Line
IMHO, this last method allows superior identification of bacteria involved with conditions and symptoms using two simple cutoff points: <= 16%ile and >=84%ile. Other cutoff points are possible, We can then look at a patient’s microbiome (assuming suitable lab-pipeline) and identify with statistical accuracy which bacteria are involved. Not only can we identify the bacteria — we can determine the relative importance of each bacteria.
This week I refactor the genus association algorithm resulting in clearer results. I also change it so the common person can understand what is being reported.
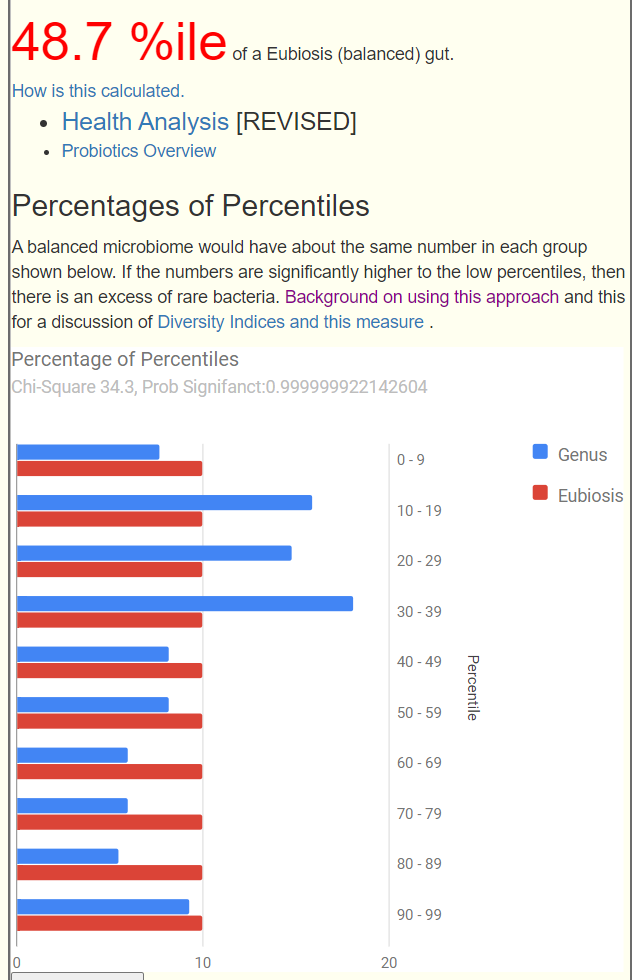
The core is that once we convert percentage to percentiles, we end up with a “flat” or uniform distribution. For any genus, we have the same number in 0-10%ile, 50-60%ile and 90-100%. If there is no association, we should see the same number in the 0-16%ile and 84-100%ile. If there are not, we can compute the statistical significance (I picked p < 0.01 or one chance in 100 of not being a true association).
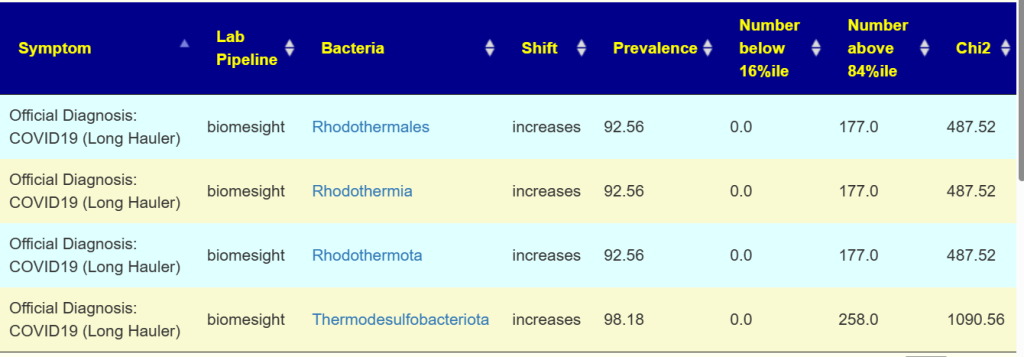
Processing without considering genus (i.e. all tax ranks) The following association occurs with extremely high statistical associations to many conditions.
This does not mean that it is a cause, but may indicate these bacteria prosper with the disruption associated with the condition. An example is below
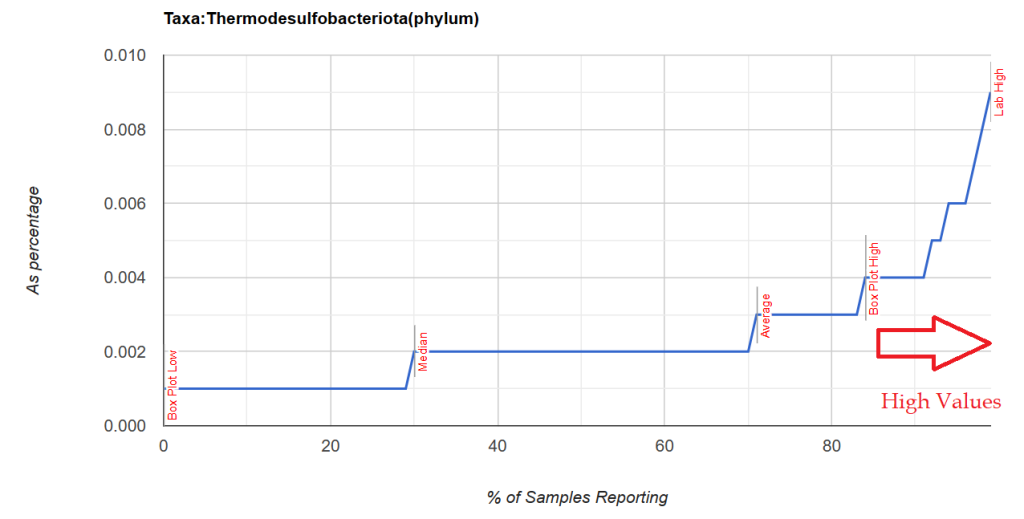
Note that these are almost always present, it is when the percentile ranking exceeds 84%ile that we have a strong indicator which is illustrated below with two distributions. Note that the amount is small.
Unfortunately, restricting to genus level resulted in nothing.
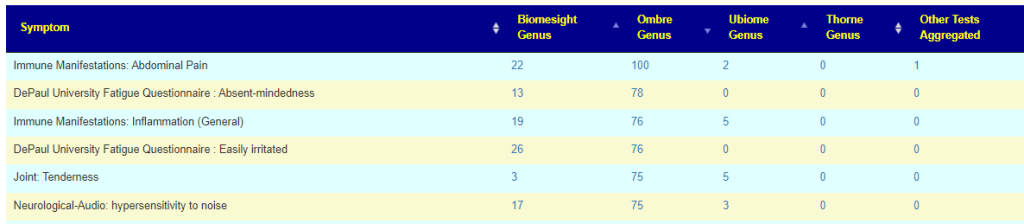
Overview by symptom
This lists all of the symptoms found significant in various lab processing pipeline. The number depends on the number of samples contributed and the number of samples annotated with symptoms. This page is recomputed and updated on the 2nd of each month; more data means more associations.
Note Taxa identification is fuzzy and should never be assumed to be “correct”. The same FASTQ file processed thru ubiome, Ombre, Biomesight and Sequentia biotech; resulted in different genus being reported with different amounts. Clearly, the associations is processing pipeline dependent.
Genus identification
Looking at Immune Manifestations: Constipation we can compare results across different tests
We see the 3 are in consensus for Butyricimonas being increased and one is silent. We see 2 are in consensus for Lachnobacterium being increased, and two are silent (at the moment, waiting for more data). Two are in consensus for Desulfosporosinus being decreased with two silent.
The lab processing pipeline is very significant for detection rate (for Butyricimonas , one detects it 57% or the time and another lab 77% of the time) and the amount reported.
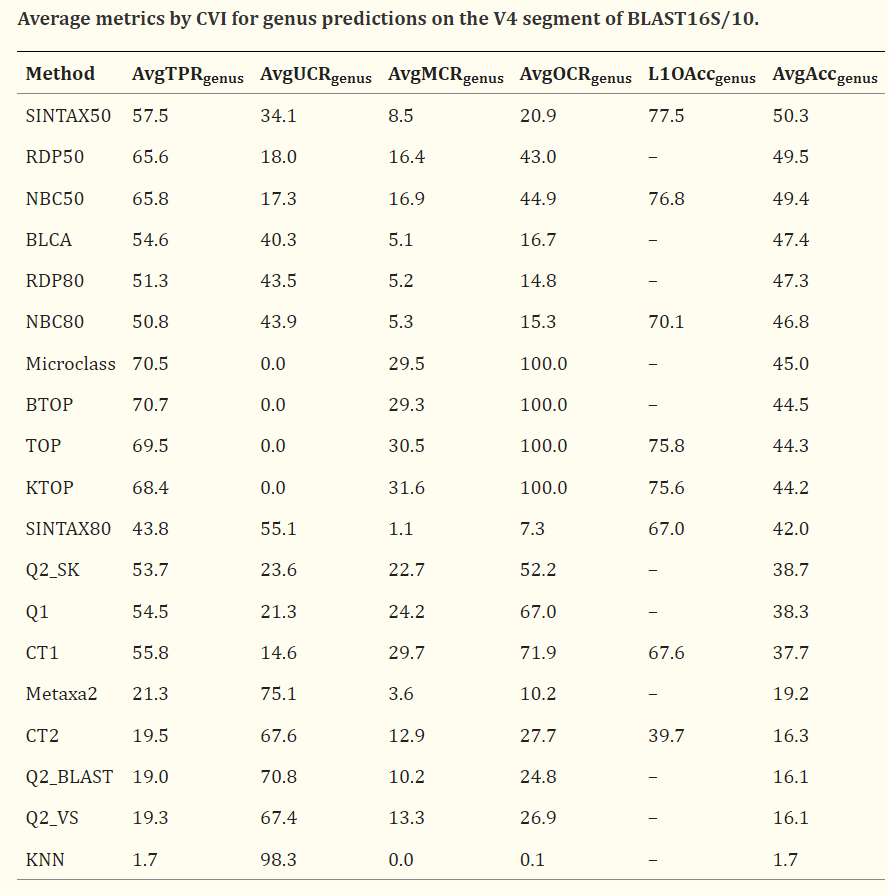
While this paper is dealing with fungi the tables can be eye opening for some people. A suitable quote from the paper “When the accuracy of genus predictions was averaged over a representative range of identities with the reference database (100%, 99%, 97%, 95% and 90%), all tested methods had ≤50% accuracy on the currently-popular V4 region of 16S rRNA.“
My expertise is in statistics, operational research and artificial intelligence, with good expertise in reading medical studies; so I asked a colleague who has a Ph.D. in Molecular Genetics. His casual comments were:
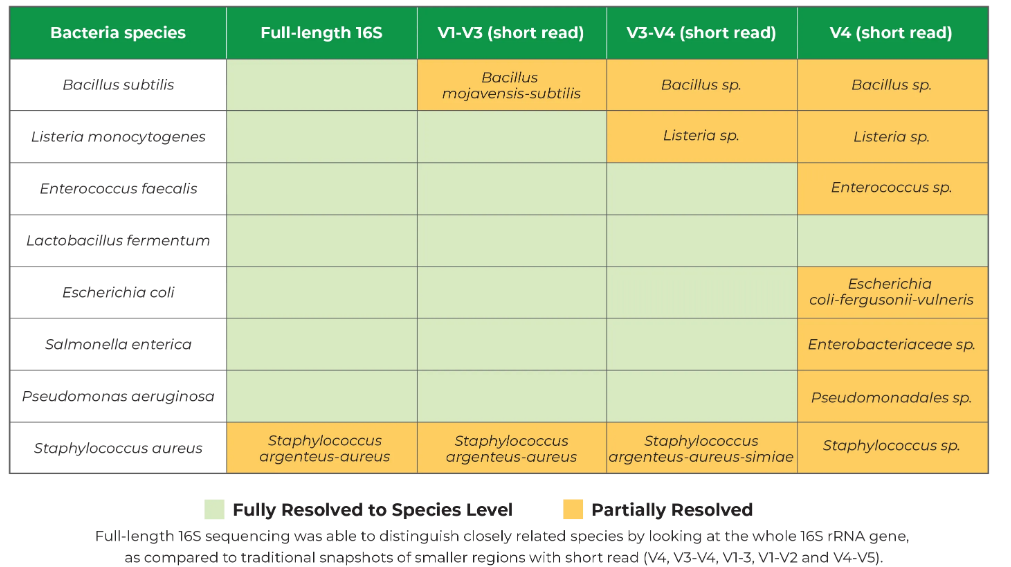
There are several studies with ASVs out there. Especially the recent ones. Clustering pipeline is what matters here. But I agree that full length gives better taxonomic assignment. Problem is full length is twice as expensive. So my point is when using V4, you will achieve incredibly better taxonomic assignments with ASV vs OTU. However, full length or V3-V5 gives a better resolution.
He also shared this graphic from Zymo Research. The V4 often cost around $50 and the full length can be 3-4x more.
What is ASV?
ASV stands for amplicon sequence variants.
OTU stands for operational taxonomic units
ChatGPT gives a good common man explanation:
Both methods aim to characterize and quantify the diversity of microorganisms in a given sample, but they differ in their underlying algorithms and conceptual frameworks.
Amplicon Sequence Variants (ASVs):
ASVs are derived from high-throughput sequencing data by clustering sequences that differ by as little as a single nucleotide. This means that ASVs are defined at a very fine level of sequence resolution.
The goal of ASVs is to represent individual unique sequences within a dataset, thereby capturing the most detailed information about the microbial community present in a sample.
ASVs are typically generated using algorithms like DADA2 (Divisive Amplicon Denoising Algorithm 2), which infer exact sequence variants and correct sequencing errors.
ASVs are considered more accurate in capturing true biological diversity but may be more sensitive to sequencing errors.
Operational Taxonomic Units (OTUs):
OTUs are clusters of similar sequences that are defined based on a chosen sequence similarity threshold (commonly 97% similarity for bacterial 16S rRNA gene sequences).
The 97% similarity threshold is often used to group sequences into OTUs to approximate the species level, although this can vary depending on the marker gene and research goals.
OTUs are generated using methods such as UCLUST, UPARSE, or others that involve sequence clustering. The resulting OTUs represent a consensus sequence for each cluster.
OTUs are considered more tolerant to sequencing errors, but they may group together closely related species or strains into the same cluster.
In summary, the main difference lies in the level of sequence resolution. ASVs aim for the highest possible resolution by identifying unique sequences, while OTUs represent clusters of similar sequences based on a chosen threshold. The choice between ASVs and OTUs depends on the specific research goals, the desired level of taxonomic resolution, and considerations related to sequencing error handling and computational resources.
To translate into human terms: ASV identifies criminals by fingerprints or DNA, while OTU identifies by the image from a security camera.
A Dilemma for Direct-To-Retail Tests
My colleague words makes the points clearly: Problem is full length is twice as expensive. Consumers are not knowledgeable about the differences but are very cost aware. The cheapest and least reliable way is often the norm. A direct to retail test costing less than $400 is likely to use the more inaccurate processes.
This means that many studies published before 2021 may have correctly identified the bacteria impacted as little as 50% of the time. So, does Barley increases or decreases Bifidobacterium?
In addition to possible confounders with selection of control and subjects in the study, we must now consider the possibility of misidentification of the bacteria. For myself and microbiome prescription’s expert system, this is not a major issue because we are using a fuzzy logic expert system.Suggestions are based on most probable given the data available.
Many medical practitioners (MDs and naturopaths) are not trained in this area and resort to a naïve deterministic approach.
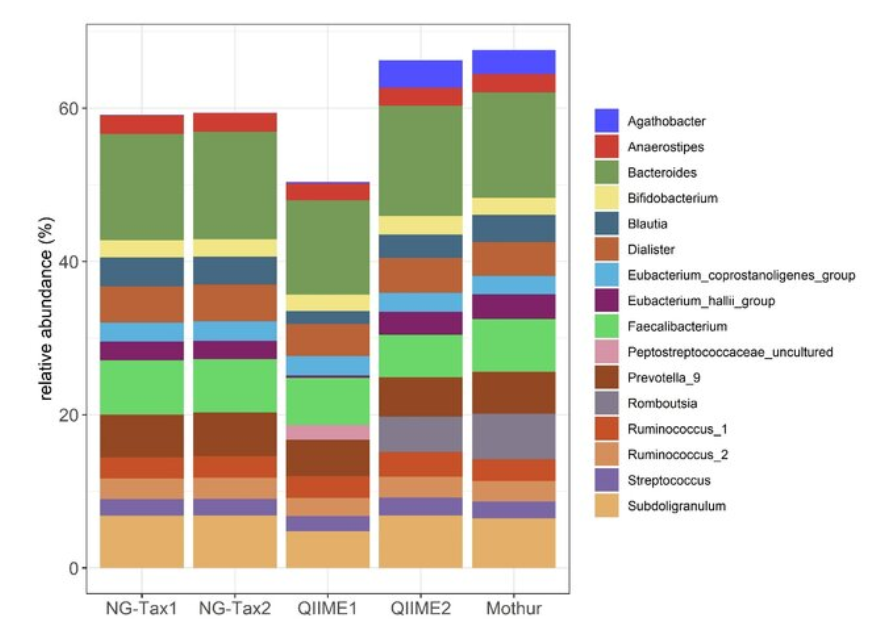
The differences of the same sample, Bacterial genera profile. Top 10 most abundant bacterial genera per pipeline resulted in a total of 16 unique genera.
Based on mock communities, ASV-based approaches had a higher sensitivity in detecting the bacterial strains present, sometimes at the expense of specificity [17–20]
OTUs detected much higher amounts of Verrucomicrobiae in the seston and sediment samples than were detected by the ASV approach. These differences are surprising given that both OTU and ASV approaches classified sequences to the same database.
Bottom Line
In dealing with microbiomes in a clinical setting, we have multiple fuzziness:
The actual bacteria being reported (and the amount) is not reliable (in the common sense of that word), it is probable.
When trying to modify the microbiome, the impact on the reported bacteria is not reliable (in the common sense of that word), it is probable.
This means using a single study has significant risk. With a diverse collections of studies and facts, then a fuzzy logic expert system results in significantly reduced risk and a higher probability of successful manipulation. It also illustrates why the Large Language Model (i.e. ChatGPT style) is very inappropriate. and likely machine learning also.
As of this writing, Microbiome Prescription has 10,390 Citations from US National Library of Medicine resulting in 2,415,340 facts in it’s expert system.
brompheniramine (Dimetappm, Dimetapp, Bromfenex, Dimetane, and Lodrane)
dimenhydrinate (Dramamine or Gravol) Dimenhydrinate is marketed under many brand names: in the U.S., Mexico, Turkey and Thailand as Dramamine; in Serbia as Dimigal; in Ukraine as Driminate; in Canada, Costa Rica, and India as Gravol; in Iceland as Gravamin; in Russia and Croatia as Dramina; in South Africa and Germany as Vomex; in Australia and Austria as Vertirosan; in Brazil as Dramin; in Colombia as Mareol; in Ecuador as Anautin; in Hungary as Daedalon; in Indonesia as Antimo; in Italy as Xamamina or Valontan; in Peru as Gravicoll; in Poland and Slovakia as Aviomarin;[18] in Portugal as Viabom, Vomidrine, and Enjomin; in Spain as Biodramina; in Israel as Travamin; and in Pakistan as Gravinate.[19]
Which Bacteria may be causing the Cognitive Declines?
Many of the drugs above are in the Microbiome Prescription database. Many of them impacts the same bacteria [ DECREASING] — implying that the cognitive loss may be connected with microbiome alteration.
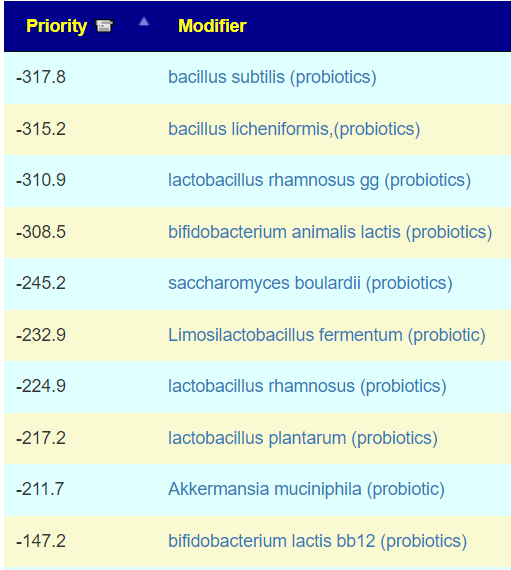
The obvious way to improve recovery appears to be the following probiotics:
A comment on this post wrote “I take Huperzine A and always wonder if that helps me out a little. (I can’t take any of those strong central anticholinergics anyway though!)“.
Huperzine A, the active ingredient derived from the traditional Chinese herb, is an efficacious, selective, and reversible acetylcholinesterase inhibitor (AChEI)
So, does it impact cognitive issues in these groups? There is no clear evidence (mixed results in most reviews)
To this I should add, the goal is to disrupt dysbiosis. Keeping the same items allows the dysbiosis to adapt. So, Keto for no more than 6 weeks, gluten free (if you tolerate gluten) for no more than 6 weeks, etc. Sticking religiously to a “cure-all diet” rarely ends well.
Once the dysbiosis is resolved, then the approach below should be considered.
I have been asked this often. My answer is extremely logical but not what you will get from most health experts (and unfortunately, may not be easy to determine for some).
The Diet….
Very simple — the type of diet that your ancestors ate 300+ years ago! Diet changes gene expression, i.e. microbiome AND dna adapts.
Last year, researchers discovered that these kinds of environmental genetic changes can be passed down for a whopping 14 generations in an animal – the largest span ever observed in a creature, in this case being a dynasty of C. elegans nematodes (roundworms)…. Usually, environmental changes to genetic expression only last a few generations. … studies have shown that both the children and grandchildren of women who survived the Dutch famine of 1944-45 were found to have increased glucose intolerance in adulthood.Scientists Have Observed Epigenetic Memories Being Passed Down For 14 Generations
From a post that I did three years ago:
Some nuggets that I found in a Christmas Present…
My wife gave me “Danish Cookbooks” by Carol Gold. This is NOT a cook book, but rather an academic study of cookbooks published in Denmark. I’m 100% Danish and very interested in history.
I have always been inclined towards going for ancestral diet patterns, and did Paleo for a while. My problem with Paleo is that it is more idealogical based than actual (scientific) archeologically based. It is also trying to jump the diet back thousands of years which effectively ignores how our bacteria evolved to meet our changes of diet.
A diet based on typical diet of your ancestors 400 – 1400 years ago is likely a better choice. You avoid the newly introduced foods, for example, potatoes. You also avoid process foods and modern additives. On the plus side, your gut bacteria is likely closer to the optimized bacteria your ancestors evolved from eating the same food for a thousand years.
In this book, I found two gems from the historical records:
We have decreased the use of spice considerably — in 1600, the common spices were:
“The issue here is … the use of seasonings in general slackens” p.47
Many of these spices (like wormwood and ginger) have strong antibacterial characteristics which would have kept some gut bacteria families in control well.
“Their most common food was meat” p. 122
White (wheat) bread was very uncommon, expensive, and typically seen only in upper class homes on special occasions(not as part of the regular menus). It appears that most of the carbohydrates came from Rye Bread.
I am sure that some readers who favor a diet that is vegan or vegetarian on ideological grounds would object to these suggestions. My response is simple, if your ancestors were vegetarians for centuries or millenniums (as some friends who were born in India can validly claim), then that is the right diet without any doubts.
Evidence shows that gut bacteria is inherited through generations — hence it is good to know what your ancestors ate because your gut bacteria have likely adapted to that diet.Given my heritage (which likely applies to people from the UK, Poland, northern France and Germany etc), this boils down to:
Rye Bread without any wheat flour
Meat and Fish (especially since the family seemed to always been within 5 miles of the coast back to 1500..)
No potatoes — they really did not enter my ancestor dies until the early 1800’s – after one of my great-grandfathers was born. Little or no sugar (“Worldwide through the end of the medieval period, sugar was very expensive[1] and was considered a “fine spice“,[2] but from about the year 1500, technological improvements and New World sources began turning it into a much cheaper bulk commodity.” – Wikipedia)
The last item needs to be taken with a touch of salt and sung: “A spoonful of soil helps the microbiome recover!” We have become hyper-hygienic. See the Hygiene hypothesis. This comes from a post in 2016:
“The Amish and Hutterites are U.S. agricultural populations whose lifestyles are remarkably similar in many respects but whose farming practices, in particular, are distinct; the former follow traditional farming practices whereas the latter use industrialized farming practices….Despite the similar genetic ancestries and lifestyles of Amish and Hutterite children, the prevalence of asthma and allergic sensitization was 4 and 6 times as low in the Amish” – i.e. industrialized farming practices resulted in six times (600%) the rate of asthma and allergies. See Innate Immunity and Asthma Risk in Amish and Hutterite Farm Children(2016). This is also echoed in their farm products!!! Amish and Hutterite Environmental Farm Products Have Opposite Effects on Experimental Models of Asthma [2016]. Given a choice of buying groceries from a Hutterite farm or a Amish farm, buy the Amish (non industrialized) groceries!!!!
So I advocate not a Paleo diet, but a regional medieval-food diet (modified for modern nutritional needs). No prepared foods (talk about being extremely unnatural!), so food prepared from scratch — ideally organic with heritage seeds.
A summary of his seven results are below. The Lab Read Quality bounces around, and with that, other values may echo these shifts (i.e. up to 20% shifts for some measures). A low read quality means less bacteria are reported, for example, when it was low, the Outside Kaltoft-Moldrup has low, when it was high, the value became high.
Another way to view it is this: If 10% are out of range and 400 are reported then we have 40. If we have 660 in another report then we would expect 66. This could be misread as a 66/40 or a 65% increase in out of range bacteria when the same percentage is out of range. Technically, it is more complicated but that should explain the problem.
Looking only at high read quality ( 1/22/2024, 2/22/2023, 8/31/2021) we see improvements where there are 🙂 below. This is an unfortunate aspect of 16s tests.
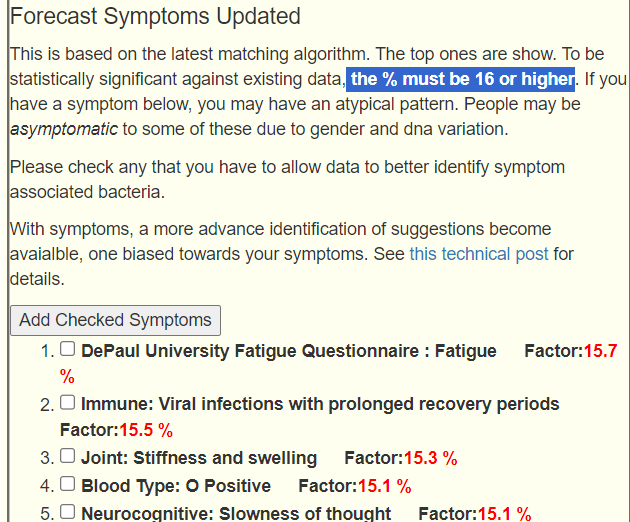
I have added at the bottom Forecast Symptoms compared to actual.
Criteria
1/22/2024
9/12/2023
2/22/2023
8/11/2022
3/25/2022
12/3/2021
8/31/2021
Eubiosis
56.4
100
37
100
100
68.1
67.4
Lab Read Quality
7.9
3.5
9.7
5.5
6.2
3.6
7.8
Outside Range from GanzImmun Diagostics
16
16
15
15
17
17
20
Outside Range from JasonH
7
7
7
7
4
4
6
Outside Range from Lab Teletest
20 🙂
20
24
24
22
22
25
Outside Range from Medivere
16
16
15
15
15
15
19
Outside Range from Metagenomics
7
7
9
9
7
7
8
Outside Range from Microba Co-Biome
2
2
7
7
1
1
1
Outside Range from MyBioma
5 🙂
5
7
7
7
7
8
Outside Range from Nirvana/CosmosId
20
20
23
23
18
18
21
Outside Range from Thorne (20/80%ile)
198 🙂
198
223
223
217
217
246
Outside Range from XenoGene
24 🙂
24
32
32
36
36
39
Outside Lab Range (+/- 1.96SD)
5 🙂
15
10
11
9
9
14
Outside Box-Plot-Whiskers
54
56
42
36
42
59
42
Outside Kaltoft-Moldrup
123 🙂
70
139
56
78
59
140
Bacteria Reported By Lab
511
399
666
478
613
456
572
Bacteria Over 90%ile
20 🙂
54
26
24
26
57
46
Bacteria Under 10%ile
108
41
82
48
44
29
99
Shannon Diversity Index
1.368
1.18
1.038
1.287
1.561
0.895
0.903
Simpson Diversity Index
0.115
0.063
0.05
0.042
0.058
0.022
0.02
Chao1 Index
7603
5057
12534
8053
13234
5563
9209
Pathogens
26 🙂
25
30
23
39
24
30
Condition Est. Over 90%ile
0
0
0
0
0
0
0
Actual Symptoms in top 10 Forecasted
5
8
10
8
8
10
9
Max Forecast Symptom Factor
38.5
22.3
25.3
16.9
15.8
26.4
33.1
Explaining the new Symptom Forecast Algorithm
This algorithm is similar to the Eubiosis algorithm. We compute the expected number of matches to bacteria shifts associated with the symptoms. The expected theoretical threshold by randomness is 16%. A higher number indicate increased odds, a lower number decreased odds. This is based on the existing annotated samples uploaded. It is not definitive and often there can be multiple subsets of bacteria associated with a symptom. The match is on too much or too few of a collection of bacteria
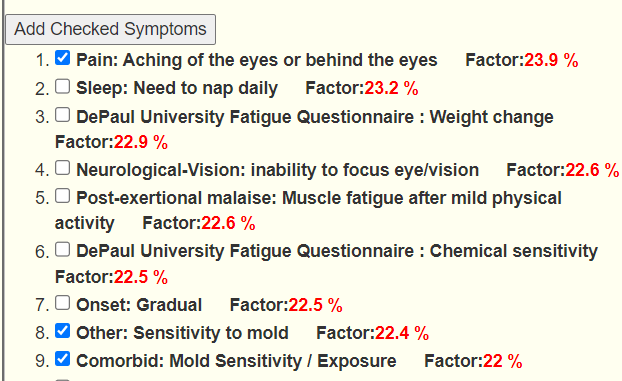
The checkmarks are the entered symptoms, the list are the predictions from most likely to lesser.
This data actually clarifies that the ideal 16+ for a factor is dependent on the Lab Read Quality and that 16 may apply to shotgun results but for 16s results, some flexibility with the 16 is warranted.
As a general FYI, hitting 80-100% correct prediction of symptoms implies that the algorithm performs well and the change of algorithm was appropriate.
It also implies that we are successfully identifying the bacteria associated with the symptoms..
The drop of matches with this sample is difficult to clearly interpret. It was not intended to be an indicator but a tool to correctly identify the bacteria of concern. Getting suggestions solely from the symptoms have been added. See the video below.
Going Forward
Again, using Just give me suggestions include Symptoms is how we are going to proceed. And then add in the two Special Studies. This results in 7 packages of suggestions.
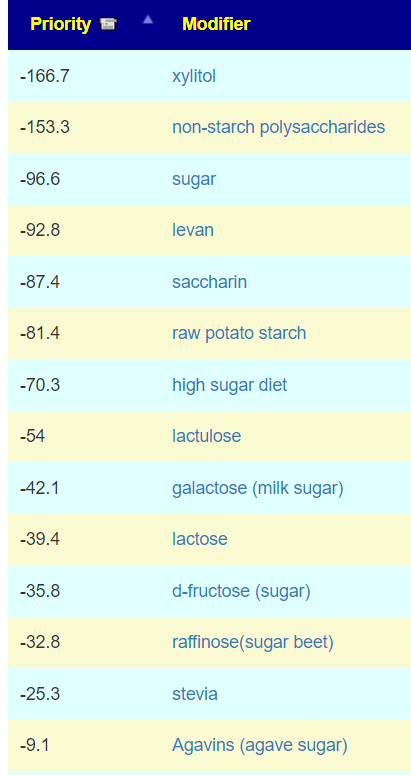
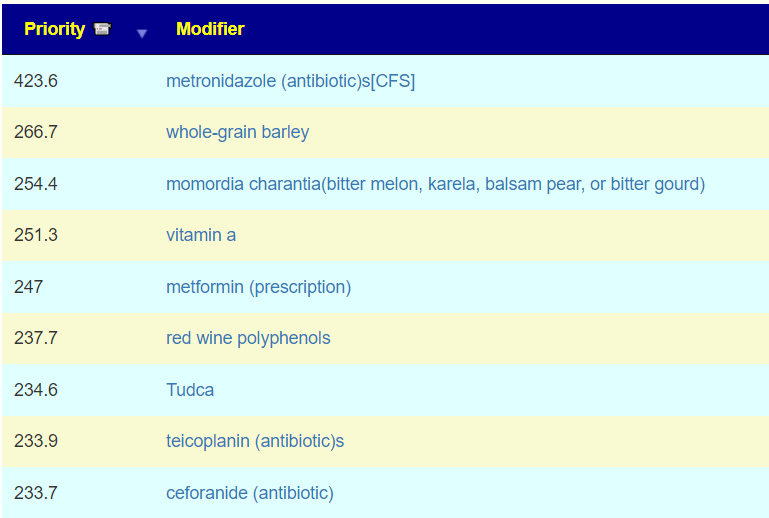
Thresholds: High is 524 thus 260 or higher, Low is -346 this -170 or lower
For our first pass, we are going to look items that all 7 agrees upon, the list is very short
For myself, I would try to obtain and rotate the antibiotics listed above and use Splenda where practical.
Bottom Line
This analysis has been both challenging and informative. We see that 16s Lab Read Quality can confuse analysis because it will alter many measures significantly. Care must be taken when comparing two or more samples with different Read Quality. Additionally, having the top suggestions full of prescription items means that we needed to adjust the threshold based on the top non-prescription item.
On the positive side, we see that the revised symptom forecasts appear to perform well, actually better than I was expecting.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a result on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or anyone. Always review with your knowledgeable medical professional.
This is the son of a person with issues: Bad Diet and Antibiotics? ME/CFS like symptoms. As I have often cautioned, young people’s and children’s microbiomes are different than adults and we do not have appropriate reference ranges. We will do best efforts.
Tired all the time
Cannot gain weight (very skinny)
Diagnosed with Marfan syndrome (a genetic disease he has since birth) [editor] About 1 in 5,000 people have Marfan syndrome
Stomach pain
Disgestion issues (yellow stool and fat in stool)
Joint and Muscle pain
Dark circles around the eyes
Analysis
There is no available literature on microbiome shifts with Marfan syndrome. Marfan syndrome (MFS) results from heterozygous mutations in the fibrillin-1 gene (FBN1; OMIM #134797), located on chromosome 15 at band q21.1 (15q21.1), which encodes for the glycoprotein fibrillin. [MedScape]. Coagulation plays a major role in Marfan syndrome. Both procoagulation and bleeding disorders participate in the disease. Platelet function abnormalities, compatible with von Willebrand syndrome or congenital thrombocytopathies, have been identified in 29% of patients. [2014].
FBN1 is the causative gene for Marfan syndrome, an inherited disorder of connective tissue whose major features include tall stature and arachnodactyly, ectopia lentis, and thoracic aortic aneurysm and dissection. More than one thousand individual mutations in FBN1 are associated with Marfan syndrome, making genotype-phenotype correlations difficult. [2016]
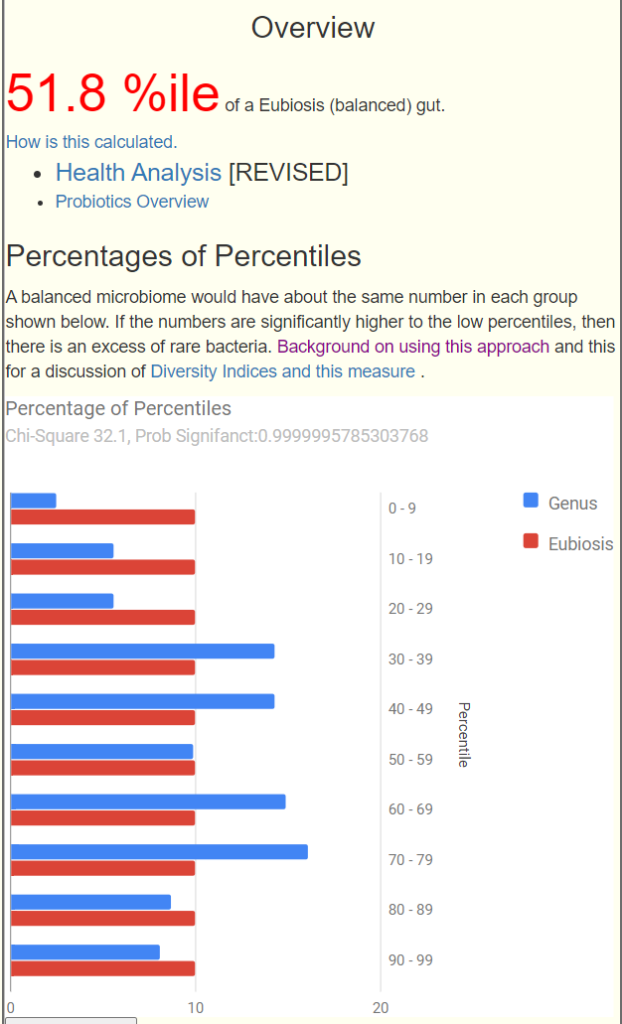
At a high level we see potential issues. [NOTE: The Eubiosis value changed for many people after a defect was detected in how percentile was computed for some bacteria – often 100% dropped, which how agrees with people symptoms ].
However, there were no statistically significant matches (this page was just updated to use the latest algorithm). This algorithm is similar to the Eubiosis algorithm. We compute the expected number of matches to bacteria shifts associated with the symptoms. The expected number by randomness is 16%. A higher number indicate increased odds, a lower number decreased odds. This is based on the existing annotated samples uploaded data. It is not definitive and often there can be multiple subsets of bacteria associated with a symptom. The match is on too much or too few of a collection of bacteria associated to symptoms.
We will still check the matching symptoms. The top one is a match for symptoms but not a match for the typical bacteria seen for this symptom. We have to hope that there is sufficient matches to be worth while.
First, looking at all of the common, popular measuring sticks –
General Health Predictors has a low number (just 8) with only one of possible concern: Veillonella atypica
All of the usual ratios are between 20%ile and 80%ile
Anti inflammatory Bacteria Score is at 89%ile — very good
Dr. Jason Hawrelak Recommended Levels came in at 94%ile
So, everything looks like a reasonably healthy person.
Going Forward
With no clear issue associations, we are going to do two runs: One with symptoms and one without.. Using the standard ‘Just give me Suggestions’ The list below are for the items at a priority of 50% or more of the highest priority [506] [Symptoms: 440]. This limit has no rationale apart from reducing the volume of suggestions.
At this point, I attempted to do cross validation: Are there any literature of items suggested (or avoid) on improving Marfan syndrome. This is done to test the suggestions – for other conditions with lots of literature, we have usually seen 90-95% agreement. For ME/CFS, I know the literature well — for this condition, not. I found only symptom treatment (Mayo, NHS). Since this is a DNA condition and I know DNA can influence the microbiome (and the reverse), then trying to improve towards typical this youth’s microbiome is a reasonable (and low risk) approach.
Because of the platelet function abnormalities that could be present, as well as thick blood (procoagulation) — both areas that I am familiar with from ME/CFS. I checked suggestions for possible items that could be related to coagulation:
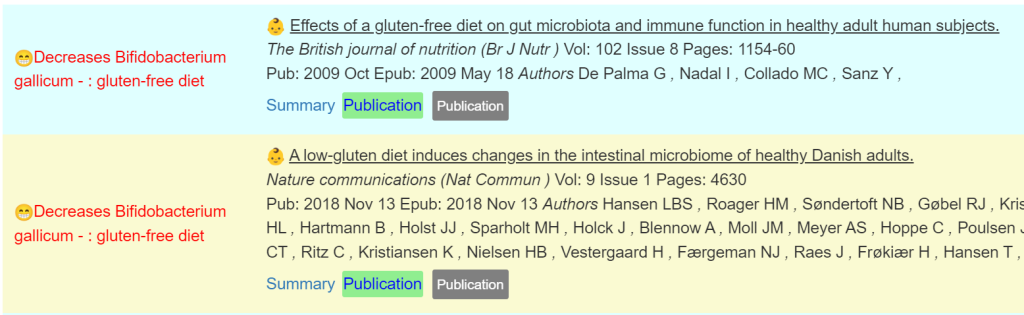
Q: Do you know why it suggest gluten Free diet? Could he have gluten intolerence/celiac maybe?
The why is because of that type of diet impacts on bacteria that are off balance. We cannot detect gluten intolerance/celiac. Only the impact of that type of diet on different bacteria. Some source papers to illustrate:
Bottom Line
The thing that strikes me most about the suggestions, the items to avoid are prebiotics and probiotics; the opposite of common advice for anyone with health issue, especially digestive issues. There are no studies on PubMed for probiotics and this condition which infers to me (given the popularity of trying probiotics) that there were studies with no effect or negative effect.In the sparse literature, we did have one of the take suggestions computing matching the literature.
If this was my own child, I would likely follow the items in suggestions above. There is low risk in following them and one suggestion does cross-validate with the available literature (which has almost nothing published in this area).
I work off the axiom that a disease or conditions modifies the microbiome to be favorable to the condition. Undoing those shifts have a reasonable change of slowing, and in some cases, reversing the condition. I have had antidotal reports of this approach speeding cancer treatment.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a result on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or anyone. Always review with your knowledgeable medical professional.
I am contacting you as you may provide a microbiome analysis for you has cfs – long Covid 19. I have been struggling for years with cfs-me. I also have Covid 3 times (the last one was in December 2023). When I did the test, I just had few days before a food poisoning that led me to ER. I did a GI map last year because I wanted to have more information after failing to cure a methane SIBO with herbs. I have a very bad infection (enterohemorrhagic e choli). I was suggested by the functional doctor whom I ordered the test some thyme and probiotics but obviously it had no impact. I redid a stool test (biomesight) but I am really overwhelmed by the results.
Would you mind give me some insight on those tests ?
joint pain, neck pain, TMJ, migraines
hypothyroidy, insulin resistance, low cortisol,
possibly Lyme (low nk57 but negative test)
possibly mold intoxication
heavy metal intoxication
brain fog
Attention-Deficit/Hyperactivity Disorder (ADHD)
skin issues on the face and eczema on my hand
Analysis
We have some dysbiosis (i.e. Eubiosis is not 100).
Looking at reported symptoms, we see a number of matches to reported symptoms over 16%ile, with one of the unchecked, inability to focus eye/vision , being a potential missed item. There are 67 symptoms entered with 58 of them above 16% (the threshold)
Explaining the new Algorithm
This algorithm is similar to the Eubiosis algorithm. We compute the expected number of matches to bacteria shifts associated with the symptoms. The expected number by randomness is 16%. A higher number indicate increased odds, a lower number decreased odds. This is based on the existing annotated samples uploaded. It is not definitive and often there can be multiple subsets of bacteria associated with a symptom. The match is on too much or too few of a collection of bacteria
Looking at Health Indicators
General Health Predictors: 11 items, with Veillonella atypica being the greatest concern
Potential Medical Conditions Detected: None. I double checked, and there were no significant matches.
Dr. Jason Hawrelak Recommendations: 94%ile
Going Forward
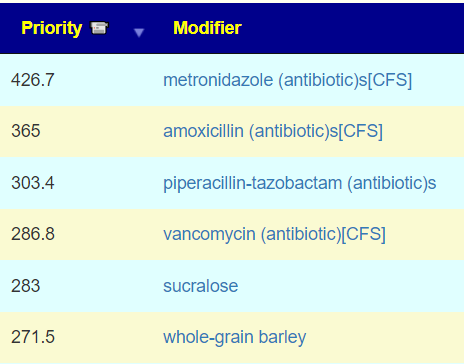
Doing just give me suggestion with symptoms gives the following suggestions for items to add (50% of 516 or hgh
Two items were border-line: whole-grain barley and gluten-free diet. These are not exact contradictions, the gluten in barley is different than the gluten in common gluten foods
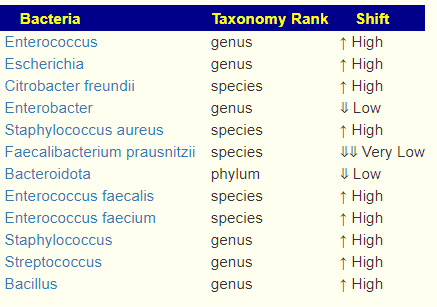
The data transcribed is below. Our consensus report above picked 67 bacteria of concern
As expected (See this post) there was agreement and disagreements between these reports on what is high or low, and some agreements. For example, Faecalibacterium prausnitzii was at the 81%ile on Biomesight data and very low above.
Suggestions will always be different because of the much smaller set of bacteria being used. We do note the following agreement in suggestions:
Q: Another question about the antibiotics protocol for me/cfs (in case I succeed to convince my GP). Dr Jardin suggests : 1 week on with one antibiotics then 3 weeks off, then another cycle with another antibiotics. Is it right ?
Correct for Jadin. One week on and 3 weeks off… and then change antibiotics. This comes from old clinical experience at the Pasteur Institute. I have read studies dealing with sewage plants that found this pattern works better.
Q: On your blog, it also says to pick one of the 4 suggestions of supplements and switch every week during 8 weeks and retest. Does it mean I must choose 4 supplements, take 1 supplement during 1 week then switch to another 8 times and so on. Am I right ? (I am not English fluent so I struggle a little to understand everything)
4 SETS of supplements…. so each week you change sets. This again is suggested to prevent dysbiosis adapting. I have too often heard “It works for 3 months and then stopped working” . As an analogy, think of cops setting up cameras to stop people speeding, their existence improves traffic — but once people learn that they are always at the same place … bad behavior returns.
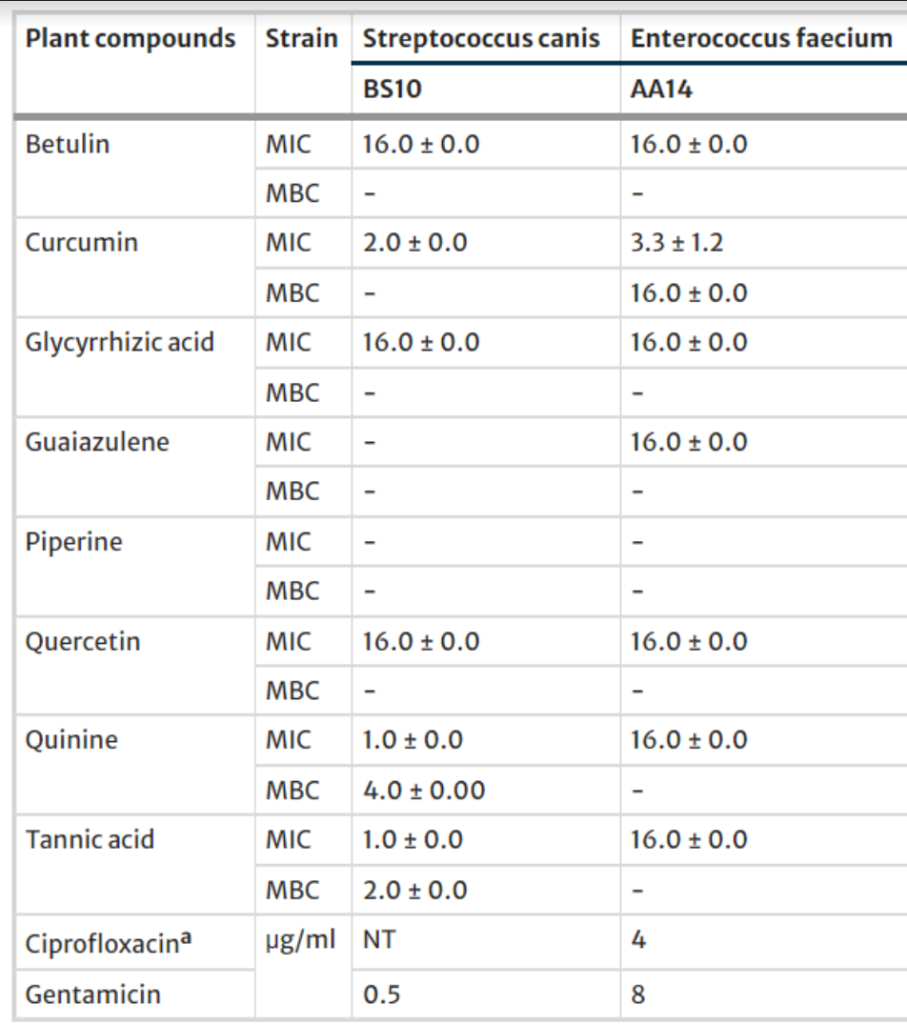
Q: Last question : could symbioflor1 help for my enterrococcus faecalis overgrowth? Or is it the opposite?
There is nothing that I could find for symbioflor1 impact on enterrococcus faecalis overgrowth in the 13 studies I have processed. So we are again into the “fuzzy knowledge area”, in general (especially the EU), probiotics are not troubles strains and thus can be used to shift related bacteria.
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
This is one of two set of ongoing samples from readers that “have appeared to almost stalled”. The other reader sent me this note at the same time (and another sample) “I have to say, symptoms are pretty dead on accurate to what I’m experiencing like all but one box. PEM is my highest ,”
This implies strongly that the association between symptoms and bacteria shifts are strong. The microbiome is just stubborn.
Feedback
He has 49 different symptoms checked and unusually, have a friendly MD in terms of antibiotics.
I would say some small subjective improvements since last time, but no major changes. Also I increased squats from 14 to 15 and push-ups from 9 to 10 at the time of the sample. (I also increased walking distance a little, but only after the sample was taken. I probably could have increased them by more, but I wanted to start really slowly with increasing those things.)
Between the last test and this sample, Amoxicillin was the only antibiotic I did. I also did some of the top herbs and probiotics (B. infantis, Mutaflor and L. Kefiri).
Also anxiety is a bit of a problem, but only sometimes, not every day. I’m not really sure what the cause is. I think it might be connected with winter, cold, rarely seeing the sun, maybe piracetame, people around me coming to me with suggestions on what I should do, maybe noise. (Noise has been a problem for me since the beginning of CFS. I really can’t endure noise well.) But those all don’t have to be the cause, they can also just be triggers or be connected to it. (Eating might also be connected to it. It seems to me that on the days I eat bacon for breakfast and a large portion of potatoes and beef for lunch (like once a week), it is better. On the days I eat sth. made from corn flour for breakfast (like every four days), it is worse. But I cannot eat the same things multiple days in a row because I quickly develop food intolerances if I do that, so I have to eat alternating things that I tolerate.) I am just wondering whether something can be done to help with that (anxiety).
Analysis
The eubiosis index is a recent addition and I am curious on how it behaves compared to other measures. Having a magic number to indicate health is an ideological goal, my gut feeling is that there is no such magic — rather many aspects need to be examined.
Sample
Eubiosis (balanced) gut.
Unhealthy Bacteria
2021-11-18
99.6
8
2022-05-20
48.5
12
2023-06-22
38.5
12
2023-09-04
100
12
2023-11-23
100
12
The traditional analysis
Criteria
11/23/2023
9/4/2023
6/22/2023
5/20/2022
11/18/2021
Lab Read Quality
5.4
4.7
7.2
8.1
5.5
Outside Range from GanzImmun Diagostics
12
11
11
15
15
Outside Ran ge from JasonH
7
9
9
6
6
Outside Range from Lab Teletest
25
22
22
20
20
Outside Range from Medivere
11
15
15
16
16
Outside Range from Metagenomics
8
7
7
9
9
Outside Range from Microba Co-Biome
3
3
3
1
1
Outside Range from MyBioma
6
6
6
5
5
Outside Range from Nirvana/CosmosId
22
23
23
20
20
Outside Range from Thorne (20/80%ile)
235
241
241
231
231
Outside Range from XenoGene
33
35
35
29
29
Outside Lab Range (+/- 1.96SD)
2 🙂
21
7
8
6
Outside Box-Plot-Whiskers
31 🙂
58
42
37
69
Outside Kaltoft-Moldrup
47 🙂
51
92
94
48
Bacteria Reported By Lab
508
568
582
674
527
Bacteria Over 90%ile
17 🙂
41
24
38
52
Bacteria Under 10%ile
83
50
147
177
36
Shannon Diversity Index
1.59
1.272
1.556
1.853
1.826
Simpson Diversity Index
0.047
0.087
0.09
0.056
0.038
Chao1 Index
6986
10061
9016
14744
7390
Shannon Diversity Percentile
43.8
12.7
40
81.8
78.2
Simpson Diversity Percentile
45.3
77.5
78.6
54.8
33.6
Chao1 Percentile
25
48.9
41.4
79.4
27.8
Pathogens
22
23
29
32
20
Condition Est. Over 90%ile
5
0
9
3
4
At first look, there seem to be little change. Looking at specific items, there is improvement (highlighted in red above), namely less bacteria with extremes levels. For all of the reference ranges from 3rd party labs, there is no effective change.
Going Forward
Since symptoms were also entered, we proceeded with [Just give me Suggestions Include Symptoms]. The results surprised me a little; the top items were CFS antibiotics and whole-grain barley (likely a proxy for beta glucan — see this post: Beta-Glucan: The Microbiome Fixer; ß-glucan is on the to take list). The following was sorted by Take Count descending (which means that all five sets agreed)
Personally, given the slow progress, I would be inclined to try talking a medical professional into prescribing one of these.
Let us do the usual breakdown by types, most are below 1/2 of the highest value.
Vitamins: B1, B2, B3,B6, B7, B9, B12 are all positive; with Vitamin A being top vitamin.
My prescription model to be discussed with the MD would be:
Week 1:A course of metronidazole with Tudca
Week 2-4: metformin (possibly with Tudca)
Week 5: Teicoplanin with Tudca
Week 6-8: metformin (possibly with Tudca)
At end of week 8 do another sample
Week 9: Ceforanide with Tudca
Week 10- new report: metformin (possibly with Tudca)
Barley porridge and similar alternating with beta-glucan supplements (since food sensitivities appear to develop quickly). Perhaps consider a diabetes-like diet (to keep the natural sugars low).
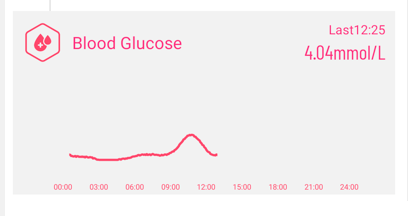
Speculation: monitoring blood glucose levels (like what diabetics do) may be a waste or time OR may provide insight. I have a smart watch that monitors blood glucose ($30 from Banggoods to Temu). There are also more professional monitors.
Question: I ate cornflour for breakfast, which I wrote about in my first mail. On those days anxiety is worse
This is often cited on influencer’s health pages, we have some potential researched supporting it:



Recent Comments