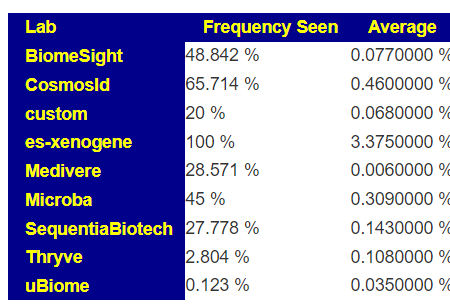
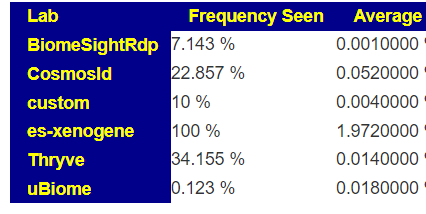
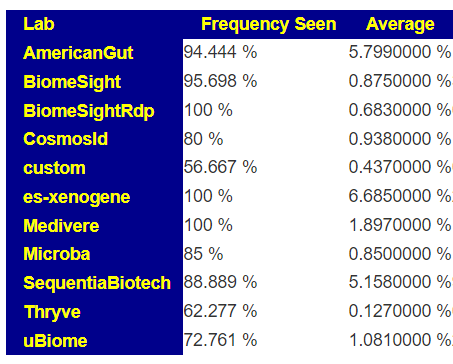
The numbers reported on most tests for these bacteria are extremely questionable. The one exception is Xenogene (based in Spain). This can be seen on these summary pages. These bacteria are grossly under reported on 16s tests.
What does this mean for manipulation? If you take Symbioflor-2 or Mutaflor, you may not see any changes in your tests (or they may become worse), when in reality they have taken up residency and are increasing. Either you go and do tests with Xenogene; or you use subjective measurements. My subjective measurement from Mutaflor was a massive severe herx for the first two weeks.
I got messages as shown below, and thought that I should share my thinking and suggestions.
Hi Ken I needed some help from you on some inputs. My mom she is 63 years old and from past few months she is getting recurrent urinary tract infections and she is been taking antibiotics. She takes one antibiotic for Ecoli UTI and next time urine culture shows Pseudomonas and again she takes another antibiotic and another infection starts.
Do you know any good probiotics which are live and multi strains?
I was thinking about sending my mom suffering with UTIs the below 2
So you need to find ones that have been documented to help, and also persists, and last — be able to get fast delivery so they can be sent to India with a friend that is travelling there.
The ones that you suggest may work — but there is no evidence (peer reviewed studies) for them being either effective for UTI or persists. The three above have the best odds of doing the correction. Enterogermina is antibiotic resistant.
Quantity
I would suggest at least a 90 day supply for all of the above. 30 days may be sufficient, but given the challenges of re-supply, it is likely better to be safe.
This email arrived and contributed in two changes:
Warning on using Special Studies — suggestions can be erratic and should not be used if they conflict with the usual consensus building algorithms.
Adding Modelled Food Suggestions — this should also partially address some challenges doing suggestions in Japan
Back Story
Love your work, I have read many of your posts on CFSremission, and based on that and my own research I think your microbiome-based view of ME/CFS is generally correct.
I have been suffering from cfs since 2009, I did a study abroad in South Korea and had a weird fever there, after that I got tired easily, often felt light-headed, head felt hot, but I was able to mostly live a normal life and actually spent a lot of time in the gym. (I think this supports the microbiome theory, my diet changed radically when I went to Korea)
I dealt with the fatigue with regular consumption of coffee/tea throughout the day, often going out drinking at night. I also used to lift weights in the gym almost every day. Full body lifts like squats, deadlifts, etc. During this time I drank about a quart of milk a day as part of my bodybuilding routine. My sleep always seemed unrefreshing.
Then in late 2019 I got sick with a EBV/Mono-type illness, swollen lymph nodes and tonsils, crushing fatigue, sore throat, that lasted a month. Sore throat resolved, but the tonsils were still a bit swollen and the lymph nodes got smaller but seemed to be permanently hard. I thought I might have thyroid issues or cancer, but multiple screenings ruled that out.
I tried multiple times to go back to the gym, but my workouts were poor and I got hit with what I now understand to be PEM the next day. Eventually I had to stop trying to exercise. I’ve tried various supplements such as methyl-b12, doses of tumeric or curcumin, too many to count, then I discovered your website. I think it lines up with my experience and is a good model to explain the so-called “anomalous” way that some treatments work for some CFS sufferers and not for others.
So I am writing this email to you now hoping I can get some insight. I have read your blog posts about other CFS sufferers analyzing their samples, so I hope you could take a look at mine as well. Feel free to use this or parts of it as a blog post, but don’t use my name or email address obviously.
Some background, I had to get a sample manually added from a lab here in japan, based on those suggestions I took two rounds of miyarisan, (I live in Japan, so it was the most easily obtained of the probiotics suggested) as well as added lots of inulin, oats, whole grains etc. to my diet. Similar to some of your other posts, including the suggestions to avoid Vitamin B supplements (the greedy bacteria taking the B-vitamins!) But, I feel like it made me worse. These days my legs are very heavy and tired.
I had another sample taken between the two rounds of miyarisan which i sent to Biomesight (a much better choice.) It took over a month for the results to get back. When they came back, it suggested a totally different course, putting miyarisan and inulin into the strong-avoid category! With the inulin+oats+miyarisan diet, I am more tired and my libido dropped a lot.
So I made a new analysis based on the national and special studies for unrefreshing sleep, ME/CFS without IBS, cold intolerance, general fatigue, etc.
1. As attached, it suggests “alcoholic beverages” pretty high. How should I interpret this? Beer? Wine? Vodka shots every evening? Is there more context for this?
2. Not many foods with any strong suggestions, what can I eat realistically (here in Japan) off this list of suggestions? It suggests a milk diet, but whole milk is not suggested? Seems to have a lot of contradictory suggestions.
3. I decided to go with national + special studies, but the “general consensus” is totally different. I assume the studies are better for my condition?
Feel free to look at the data of both of my samples, or offer a different way of getting a consensus, I really need some guidance here!
Regards,
From a reader (with permission to post)
Initial Impressions
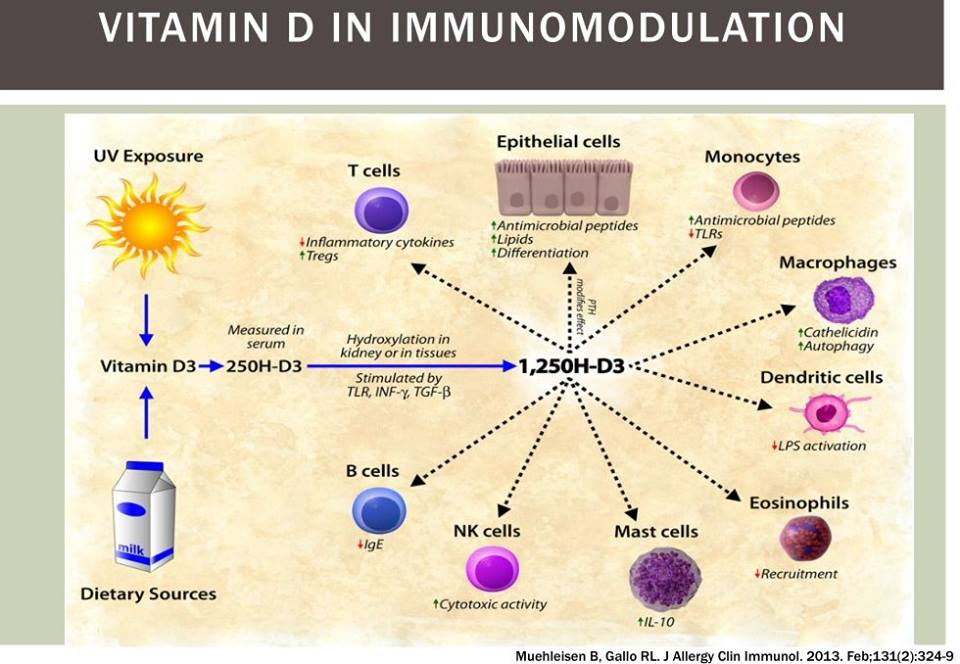
“EBV/Mono-type illness” — EBV, HHV5 and other virus in CFS gives context, but this post, Viral Reactivation and the Microbiome gives context and cites “For EBV, viral load was significantly higher when 25(OH)D levels were low, demonstrating an inverse correlation between 25(OH)D levels and EBV load. ” [2018]. My first step would be to get 25D levels measures (likely low) and 1,25D levels (likely very high). It’s an easy issue to address with Vitamin D3 supplements (likely 20,000 IU/Day may be needed. See the following for more information
My suggestion [2016] for target level is: 90-100 ng/mL (200-250 nmol/L). (of course, to be discussed with your medical professional)
The Key Problem with Suggestions is the picking of bacteria
Suggestions are based on several main factors:
The bacteria you decide to alter (i.e. increase or decrease)
The importance of each (sometimes called weight) when there is a trade off
What substances has had any research. This is a nightmare – between contradictory results, small sample sizes, study done in the context of a specific diseases, etc. This is why I use fuzzy logic.
With the above stated, I walked thru this sample trying to first improve the bacteria selected (using my experience and statistical understanding), and then looking at the suggestions they generate.
This issue can be compounded with the depth of bacteria reported. “The disease is in the small details”. This is why more detailed and comprehensive (i.e. number of bacteria types reported) tests are a better starting point.
Contradictory Suggestions root issue
Facts in the database are based on what is specified in the study. A simple example: one study may use turmeric and a different study used curcumin. Curcumin(diferuloylmethane) is a main component of turmeric, but it also contains two other compounds demethoxycurcumin, and bisdemethoxycurcumin. In addition, volatile oils (tumerone, atlantone, and zingiberene) [Antiinflammatory Herbal Supplements, 2019]. The studies may result in a bacteria increasing in one and decreasing in the other. Both are right! It is the additional components that are significant. The worst case of “fuzziness” is with anything that has the word “diet”. Many people offering advice will deem them to be the same to simplify the facts that they need to remember; Dr. A.I. does not need to simplify — but that comes at a cost of confusion when things seem similar at a high level to the user. Another example: lactate, lactose, versus milk.
Analysis
Going to the My Profile / Health Analysis page, we see the two items that where he is at highest percentile (98%ile and 99%ile) are related and would agree with unrefreshing sleep.
Sleep Apnea
Insomnia
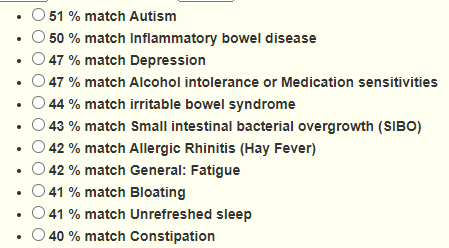
ADHD is high, but that seems common with ME/CFS. Dr. Jason Hawrelak Recommendations come in at the 89%ile. Going over to special studies, we see a lot of matches. The matches are not predictive — there are other factors (like DNA/SNP) before symptoms appear. They indicate simply increased risk.
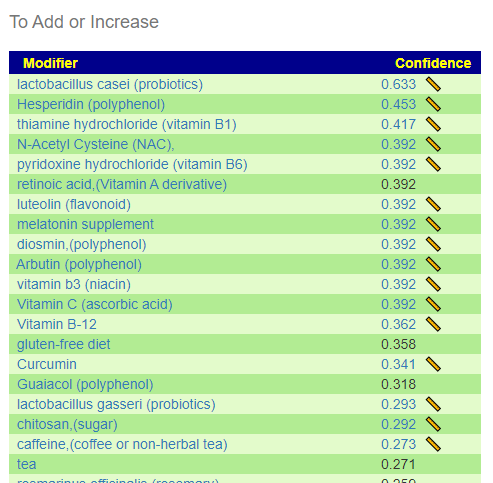
The majority of probiotics are to be avoided (not unusual for ME/CFS). The top suggestion was lactobacillus casei which is an easy one to get in Japan. The well studied one is sold as Yakult. The next ones are: lactobacillus gasseri, bifidobacterium breve. With most of the probiotics being negatives, you do not want to get them in probiotic mixtures.
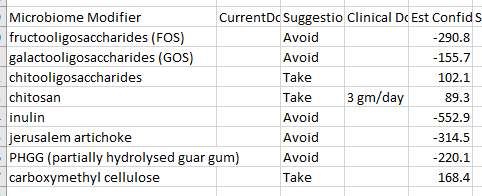
Most pre-biotics are to be avoided.
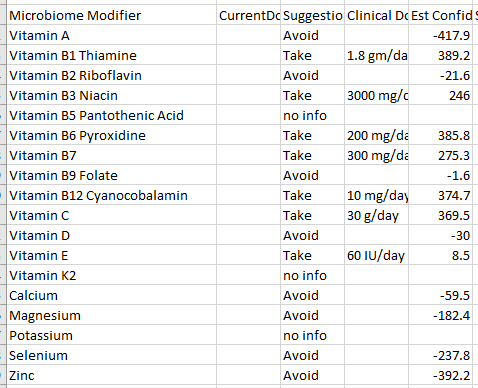
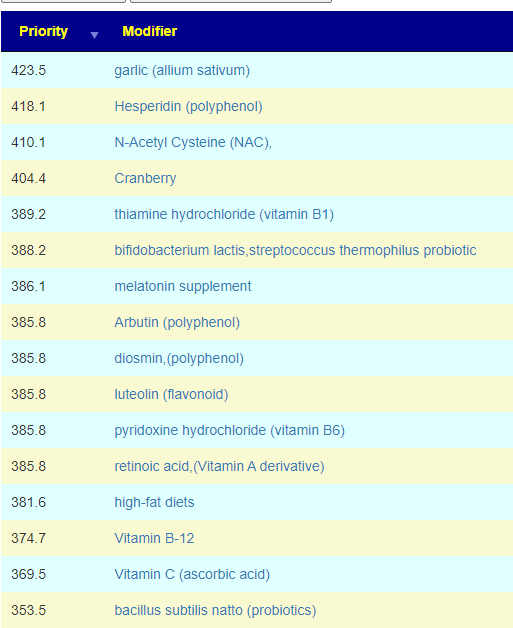
In terms of vitamins, we see most of the B-vitamins are suggested (this is seen in one subset of ME/CFS patients, a different subset has it as an avoid). Vitamin D is a very mild avoid — but given the EBV issue above, I would ignore it and make that judgement call based on blood tests.
This also may apply to B-vitamins — none of the B vitamins are strong avoid, so a B-Complex is fine.
I have filtered the rest of the list to only the to take, coffee is sitting high in the list which appears to agree with “I dealt with the fatigue with regular consumption of coffee/tea throughout the day“. It helps in additional ways on shifting the microbiome.
There are a few items not in the simplified list that are worth calling out:
bacillus subtilis natto (probiotics) – is in the Japanese desert food called Natto. (it is a bit of an acquired taste [I have acquired that taste] and usually found only in some Asian markets in the US). Nattokinease is an extract from it.
ME/CFS without IBS – 7 bacteria matched – We get good agreement with the above
From ME/CFS without IBS
Comparing Suggestions from Special Studies
As a result of this email (and several others received this week), I looked at Special Studies suggestions for some specific people. My expectation when I did special studies was that the suggestions would converge tighter — so some people that is true. For other people, like this person is it false. For more information read the blog post: Caution: Special Studies Suggestions
I noticed that most of the results had inulin, etc – which are to avoid above and appears to make the person worse.
Chronic Fatigue Syndrome (CFS/ME) – 52 bacteria some agreements and some disagreements
Unrefreshed Sleep — 62 bacteria matched
ME/CFS without IBS – 94 bacteria matched
I will be using this person sample to experiment with revised algorithms for Special Studies.
Probiotics
The top probiotic from KEGG data are E.Coli probiotics. Both Mutaflor and Symbioflor-2 (commercial E.Coli probiotics) are on the to take consensus list.
This was an unexpected frustration. I wait back to the algorithm and made it less conservative. By this I mean, not eliminating items where there are contradictory results from studies. This resulted in in more suggestions, some Japan specific [there are 50 items acquired in Japan on the list]
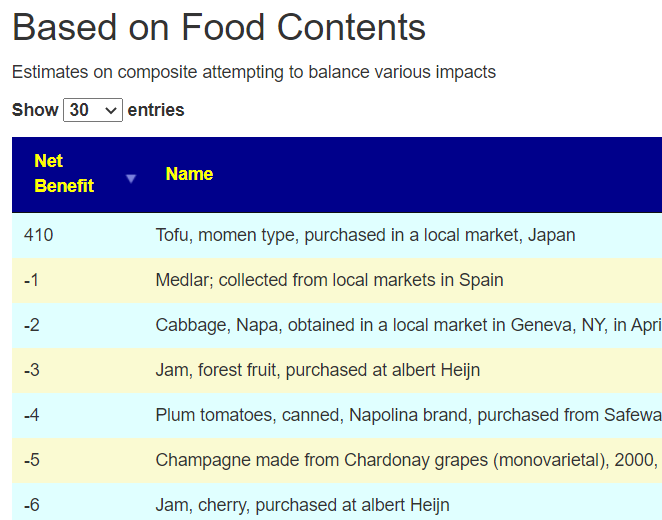
I was going to leave the algorithm with the more relaxed condition. I then did cross-validation with the consensus and found that most of the items appearing as take using the relaxed filter were on the avoid list of the consensus. Tofu, which showed up with the strict criteria, is on the consensus to take list (as in Soy).
Why do we have any disagreements? The root problem is not sufficient studies – often with contradictory results — one may be on people with diabetes and another people with asthma. Existing conditions (and in some cases severity) can result in difference response. The microbiome is not a machine but a complex society that interacts with a lot of things
The Hail Mary Exploration
I redid the consensus and included prescription items. For many people, the pharmaceuticals are way down the to take list. Herbs and probiotic having a higher positive weight often. For this person, this was not the case. What was also unusual was none of the antibiotics that are recommended in other ME/CFS analysis (and which are used for ME/CFS – i.e. cross validation) are anywhere near the top of the list. What I found listed near the top of the pharmaceuticals were:
My immediate, due diligence, suggestion is to get testing for cholesterol, hepatitis and fungal infections. Was the “EBV/Mono-type illness” perhaps hepatitis? Two of these can result in chronic fatigue. In terms of special studies, ME/CFS (three variations) were poor matches (one was the bottom of the list). Using US National Library of Medicine studies, he is at the 29%ile.
What I find interesting is that soy is a recommendation, and we find these studies..
In terms of having the typical microbiome for someone that has a ME/CFS diagnosis — he does not match. He is also at the 0%ile for hypercholesterolemia (High Cholesterol), 8%ile for GERDs (usually common for a subset of ME/CFS).
My gut feeling is that he was not sufficiently tested before the ME/CFS label was slapped on him. His microbiome is not a match. Nothing match his symptoms to the microbiome associated conditions that I have data on.
FEEDBACK FROM READER AFTER READING
Those are very interesting points. Since my initial symptoms in Korea, I was diagnosed with Gilbert’s syndrome, an excess of Bilburin. I did get my liver checked (due to slight yellowing of the eyes) out but they don’t seem to have found anything (Over a decade ago so my memory is pretty spotty.) I think over the years in college I got MRI’s and various bloodtests with obviously no real diagnosis. Even so, my life was very active over that decade. I lived in China for a few years, frequently attended the gym, also did a fair share of partying, have always had a big appetite. Minimal impairment throughout my life overall.
Since getting sick a few years ago in Japan, I got a lot of different tests, including thyroid and diabeties. If I rifle through all the different result sheets (I have quite a few), a few things of note:
Dec. 2020 I was positive for EBVVCA-IgG which my doctor told me meant that I had had EBV in fairly recent past. No treatment was suggested.
Feb.. 2020 I had slightly elevated liver enzymes (ALT, GTP) (Not surprising given my frequent social drinking in my 20s) which persisted until April 2021 and seemed to have resolved. This was explained by lowered alcohol consumption. Never received a suggestion for follow-up or differential diagnosis.
Persistently higher tryclycerides (I have gained some weight since my illness, matches with the atorvastatin suggestion!) and CRP indicating inflammation. Suggested to lose weight and exercise (The latter being somewhat problematic for me.) Back in my weight-lifting days, I drank lots of milk and overall had a high-fat/protein diet. Since I recently stopped drinking so much whole milk, I wonder if that will resolve it or not.
Before I moved recently I had been going to a cfs clinic which conducted sleep studies (of which I have had several over the years, indicating that I do not have sleep apnea, although that was my thought for years.) and did some other tests indicating I had high stress/inflammation. He gave me vitamins, CoQ10 (which I ordered myself) and anti-depressants for sleep. (Interesting I score high for Depression (47%) but up until the last few years I had a very active lifestyle, I don’t think depression fits my physical symptoms at all. I’ve always been very social and generally on the adventurous side. Still am, just don’t have the physical stamina I used to. I requested a prescription for Piracetam (all of the -tams were recently regulated in Japan) and he refused.
I haven’t gone back there since as I felt like the approach he had was very symptoms based and surface level. Reading your recovery stories, I pretty much ruled out getting any kind of prescription anti-biotics or being able to utilize those out here. I don’t know how the legal system works here in Japan, but my own and other anecdotal experience tells me that doctors here don’t enjoy doing things off-label, it’s an extremely by-the-book conservative approach to medicine. Fortunately, if you have a specific, known medical problem, you can get extremely professional and competent care here.
It is very interesting that I do not fit in the ME/CFS microbiome profile. An infection with Hepatitis or a fungus at some point could fit, especially given that I’ve spent time in a variety of different environments. I think I could easily get tested for Hepatitis here, it will just have to wait until next month (Currently very busy as a **** .) As far as fungus goes, usually I hear about “Candida,” any suggestions of what kind of fungus I should perhaps be looking out for would be helpful.
I will have to think about how I will go about getting tested for fungal infections here, it is somewhat difficult to explain my issues to doctors and get them to take it seriously. Definitely a good idea to also pursue a potential alternative diagnosis though, the data certainly doesn’t rule it out.
You have given me a lot to think about, thanks again for all of your consideration!
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that appears to have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
I use modelling and various mathematical technique to estimate forecasts when there is no hard data available.
I have been in dialog with a microbiome testing firm on incorporating my suggestions engine into their site. One of their requests was to provide more information on foods. Of course, if there are no studies than how can you make suggestions?
It is possible to model likely impact of foods by looking at what is in them. That information is available from:
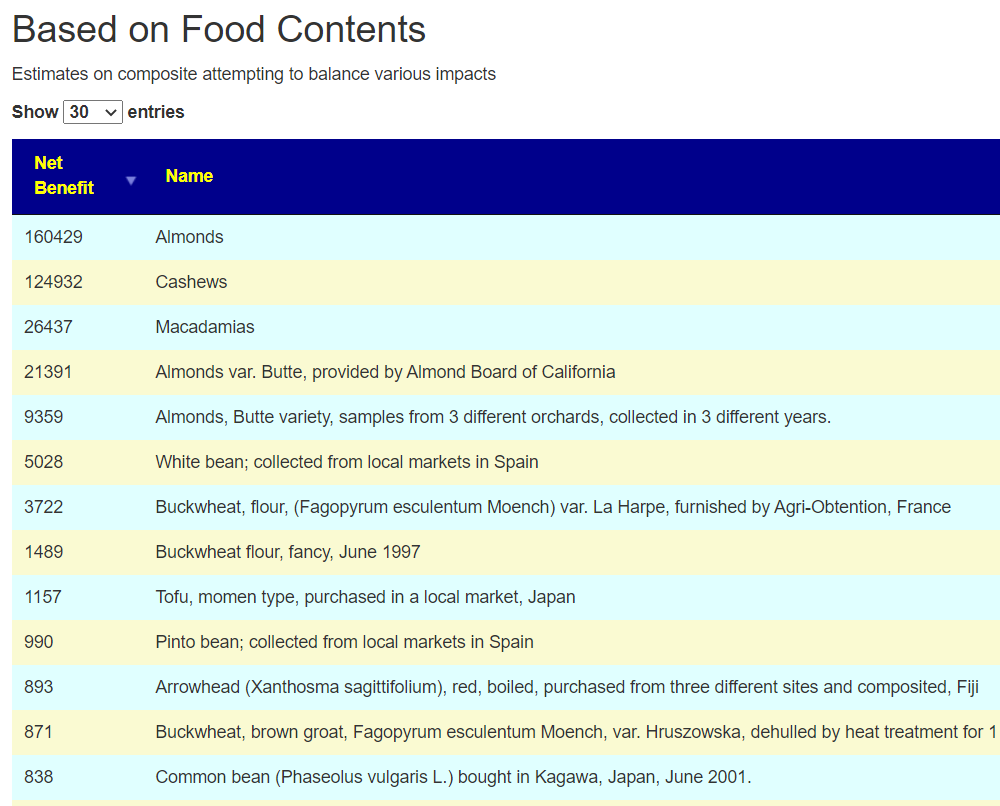
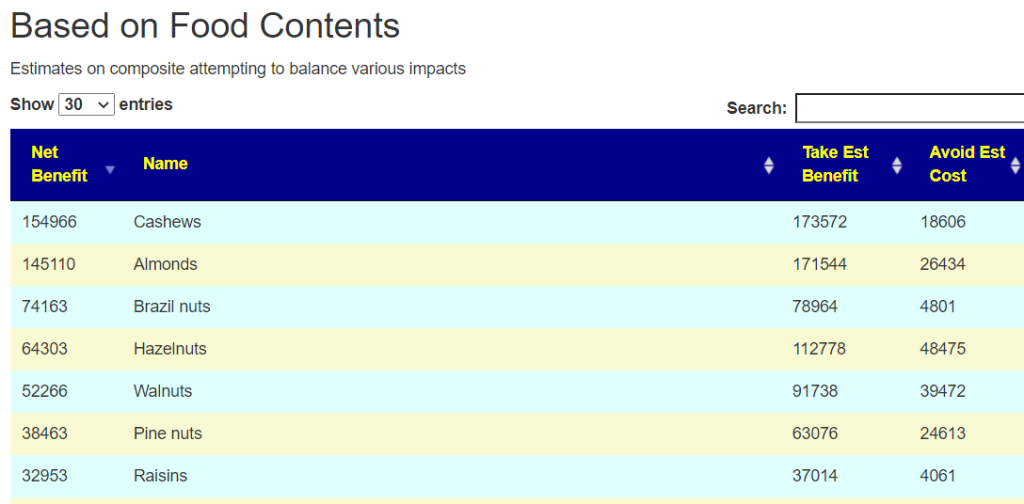
So the process using existing pubmed studies to identify the constituents of the food that impacts certain bacteria and then aggregate these constituents to get a modelled benefit from the food.
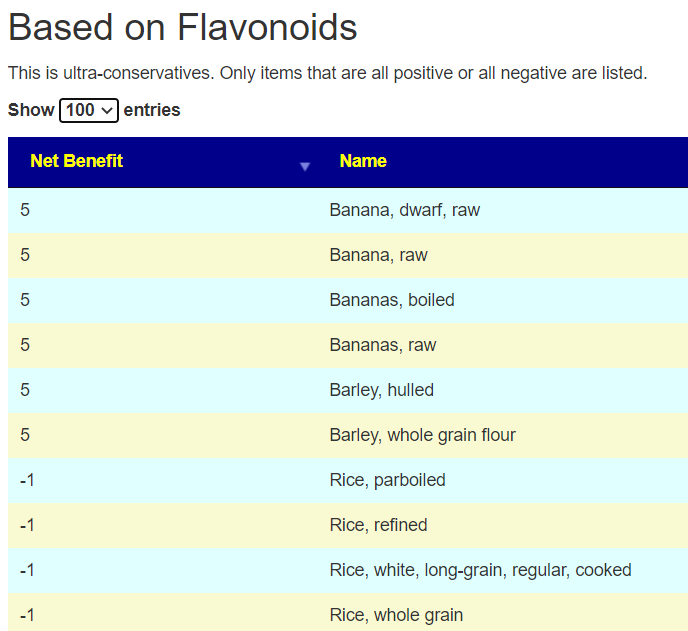
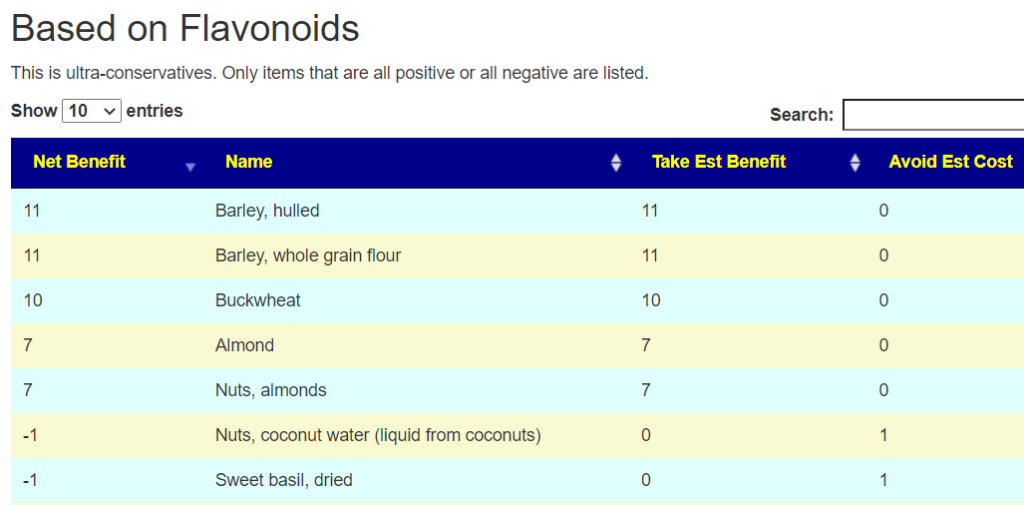
The results are two tables (depending on which decomposition approach is used).
This is on the Changes Tab
This lists only things that are entirely one way or the other.
Appears to Cross Validate
I did some of the other suggestions methods, built a consensus report and then looked for Almonds on the same sample and found agreement. Same with Barley, Basil, and Buckwheat. Some suggestions from the second list have disagreements (not unexpected).
I would suggest that that you see how it works for your samples between these two approaches.
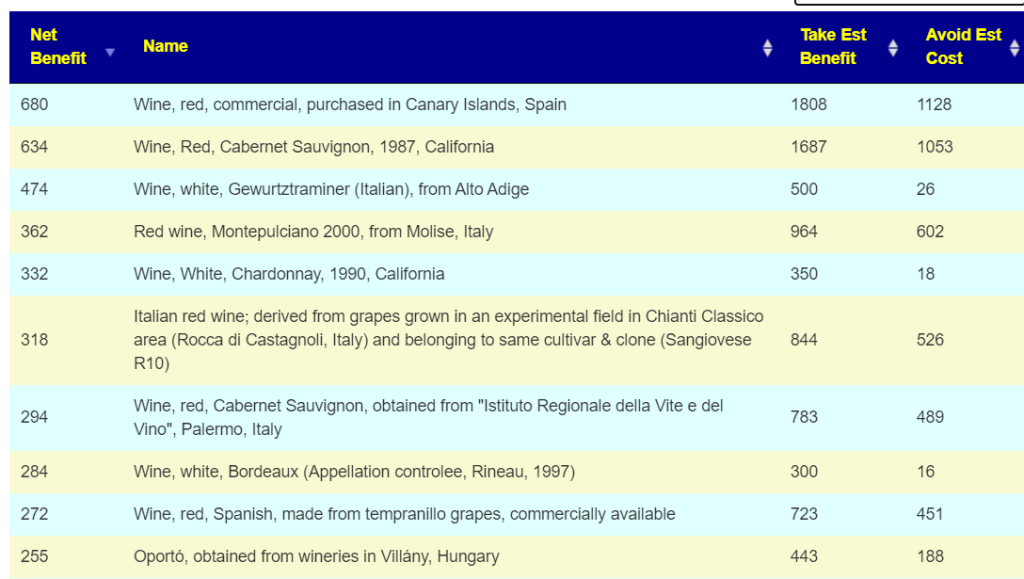
For your amusement, the second list is LONG (typically 800+ items) and for those that drink wine, may be amusing to scan..
Other Labs
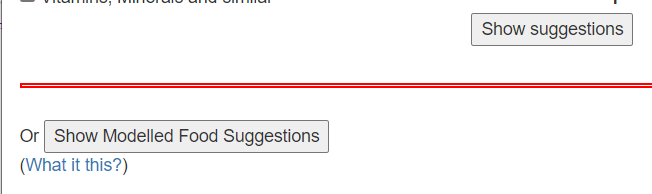
This has been added to the define suggestions page. Both buttons open the suggestions in new windows so it is easy to switch back and forth.
If you have already uploaded a sample, a link has been added there.
Special Studies are a conceptual thought experiment. The logic is simple, identify the bacteria that are have major statistical significance from the reference. Then use these bacteria with the weight that each has being the z-score to generate suggestions.
The first reviews that I did using them had good results and agreement with my preferred trio to build consensus, namely:
This last week I have gotten several emails from people who got counter-indicated suggestions. I have verified that for their samples, it produces contrary suggestions.
Digging into the mathematics and fuzzy logic being used, I see several possible failure points that I want to slowly investigate. The top failure points are:
Using the z-score for the weight to give for each desired shifts. A different formula may resolve it. Two candidate formula are:
z-score * incidence of bacteria being seen
z-score * function(bacteria count) — with many possible functions
The z-score cut off is too low, I am using 5.0 at present, it may need to be raised to a higher value.
The criteria for picking a bacteria to include may not be specific enough, so a lot of bacteria that are fine are included. This can result in excessive noise in the suggestions
The data available for suggestions at the species levels that we are working are insufficient (and in some cases, may not exist). A lot of the species flagged are rarely seen in studies showing changes.
Bottom Line
Use the suggestions generated with great caution. If they compliment the suggestions from the three preferred consensus methods listed above — good. If they contradict, keep to the original consensus method — I have been getting consistent report that they work. The special studies suggestions are getting inconsistent results.
A special study with a z-score below 6.6 is very suspect and should be ignored.
A reader contacted me over a new post on Biomesight – How to reduce brain fog. He was concerned over the content (knowing that I have often researched and posted on brain fog), so I am doing this post to provide some clarity on brain fog. (Bad pun: Remove some fog from brain fog)
What is Brain Fog?
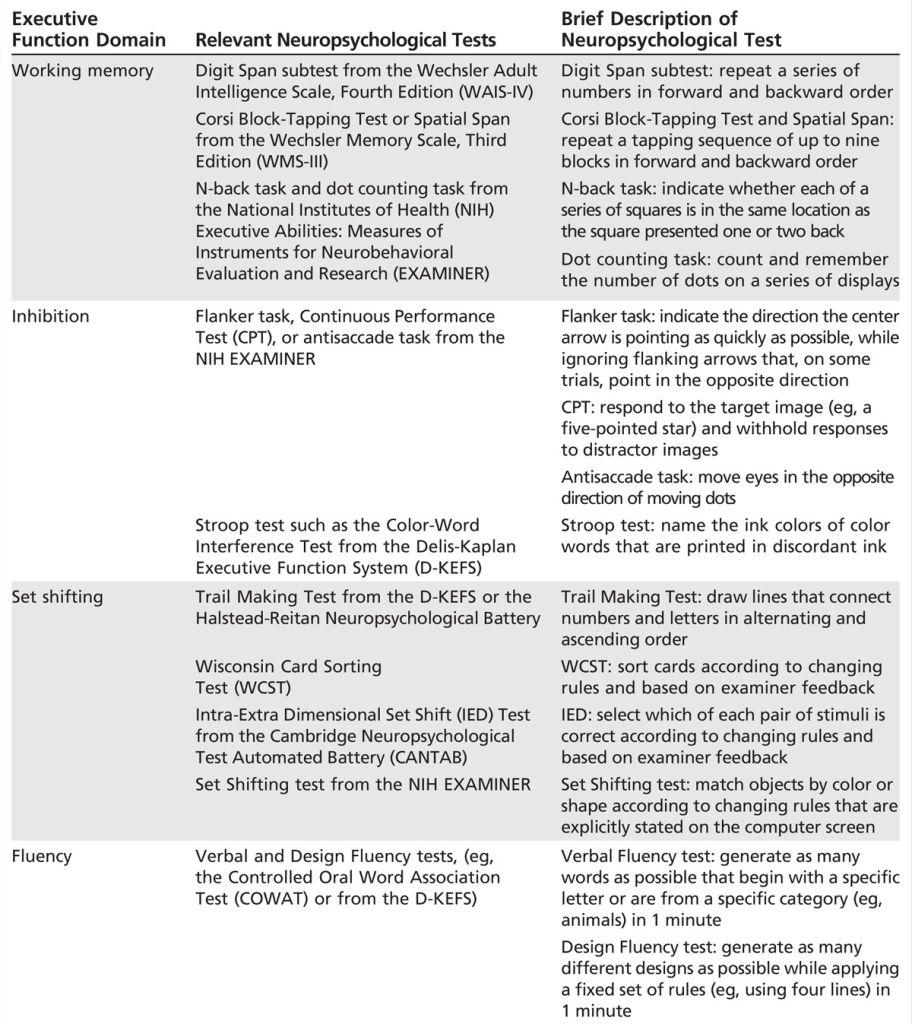
The term brain fog is a vague term that has been defined in the literature as a combination of the following more accurate (and measurable by tests) conditions. A better term is executive dysfunction [2015] or Cognitive Fatigue [2014]. The literature goes back to at least 1989. I know from personal experience, I have taken them from professional psychologist, and other in the family has too.
Some people will perform badly on all tests, other will perform poorly on certain tests only.
IMHO, if you do not have the majority of the above, the term may be misapplied.
For different diseases, what constitues brain fog can vary, for example:
The clinical picture typically affects visuo-spatial immediate memory (g = − 0.55, p = 0.007), reading speed (g = − 0.82, p = 0.0001) and graphics gesture (g = − 0.59, p = 0.0001). Analysis also revealed difficulties in several processes inherent in episodic verbal memory (storage, retrieval, recognition) and visual memory (recovery) and a low efficiency in attentional abilities.
Many of the above have distinct microbiome signatures and thus the hope of getting a universal microbiome signature for brain fog is an ideological belief. This appears to be confirmed in the analysis from Special Studies … Brain fog strongest z-score is just 5.2. This is lowest significance level of 26 items evaluated, the next lowest is General Fatigue. IMHO, there may be no true significance, the z-scores numbers were not adjusted for False discovery rate and incidence of reporting.
Most people will agree that there is no magic cause or microbiome signature for general fatigue — it could be an issue with iron levels, excessive lactic acid (impairment in clearing it), blood circulation issues, respiratory issues etc.
Brain fog could be described as mental fatigue and thus the same wide variety of issues can be involved. For ME/CFS, the dominant causes for brain fog, according to the literature are mentioned in some of my prior posts:
My first concern is simple, the belief of there being a common microbiome pattern is very questionable. There are likely patterns, for example, a microbiome pattern that results in higher d-lactic acid production; a pattern that results in lower d-lactic acid production; a pattern that inhibits one of the many steps in the coagulation cascade; a pattern that overloads one of the many steps in the coagulation cascade; a pattern that causes vascular constriction; a pattern that cause inflammation; a pattern that inhibits the absorption of iron…and on and on. There is not a single pattern that applies to all.
When a statement like this is made “Unsurprisingly, high ethanol producers in the gut based on research findings (separate from what we are seeing from the Biomesight dataset) is associated with brain fog.” I would expect links to these research papers to be included for the reader to follow up. Ethanol is drinking alcohol, booze – which has me very curious about the links and especially if they are seen with many of the conditions cited above.
How does special studies compared to Biomesight post
The table below shows no agreement between my special studies and their findings. We used different statistical process, but finding not a single agreement should be a red flag on relying on the data. While I have a smaller sample (approximately 1/3), the data processing to get the microbiome data was identical.
Bacteria
BiomeSight Post
Special Studies Z-Score
Escherichia coli (species)
5.3
Lactiplantibacillus pentosus (species)
5.1
Shuttleworthia (genus)
5.1
Escherichia (genus)
4.5
Veillonella (genus)
4.4
Veillonella dispar (species)
4.4
Staphylococcus pseudolugdunensis (species)
4.2
Clostridium cellulovorans (species)
4.1
Class Deltaproteobacteria
X
Species Bacteroides uniformis
X
Species Bacteroides cellulosilyticus
X
Species Phascolarctobacterium faecium
X
Genus Bacteroides
X
Species Anaerotruncus colihominis
X
Species Faecalibacterium prausnitzii
X
Genus Prevotella
X
Bottom Line
I do not believe that we can aggregate all microbiome samples reporting brain fog into a single set and find a universal pattern to address a priori. The numbers from Special Study: Neurocognitive: Brain Fog were the weakest of all special studies and, based on some other recent work in progressed, results may be adversely affected by sampling bias, sample quality, and false detection rate.
“Lots of high % potential health stuff. In real time, mother’s very hormone sensitive . Gets like a Premenstrual dysphoric disorder (PMDD) state , feels depressed. Struggles with anxiety and depression in general . Notice she’s been getting allergies. During the birth of 2nd child two years ago; mother had to get vancomycin because she was strep B positive. When the family get sick, the mother gets the sickest of the 4 of us unfortunately. Mother caught COVID in Sep 2022. Mother’s cycles in 2021 started to be heavy where before that never happened. As a kid, mother was on Accutane a lot. When mothers results through biomesight I also got a message that said unusually small file size or something along those lines.”
Foreword – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that appears to have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
Mother Overview
Jason Hawrelak Recommendations – 99.7%ile (better than most), High Roseburia, Blautia. The others are low
Checking on the two studies that I could find Premenstrual dysphoric disorder
This suggests that we have a general match with the literature and should include in our consensus, a hand picked set of suggestions.
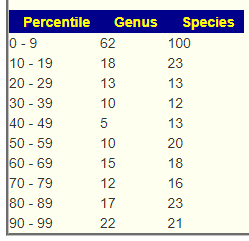
There is an abundance of bacteria which are there, but at low levels.
We have an impressive list of bacteria deemed unhealthy. Note that counts are often small (agreeing with the abundance of bacteria at low levels seen above).
Potential Medical Conditions Detected had at 99%ile, Schizophrenia, which suggests some overlap with PMDD.
Going Forward
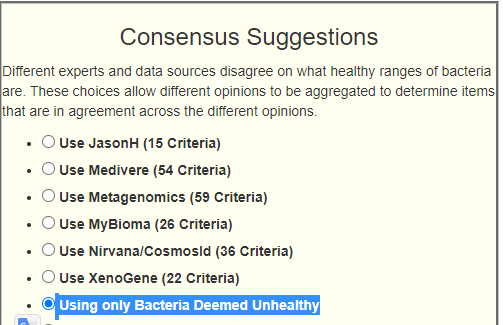
I added a new choice to the site that gets canned suggestions for Bacteria Deemed Unhealthy above because of the large number of bacteria flagged in this sample.
The new option
The suggestions for this person with this new option.
33 bacteria was selected.
Building the Consensus
I am building from:
Hand Picked (see above focused on PMDD) (4 picked)
Unhealthy Suppression – just added (33 picked)
Outside Range from Nirvana/CosmosId (5 picked)
Outside Lab Range (+/- 1.96SD) (6 picked)
Outside Box-Plot-Whiskers (60 picked)
Outside Kaltoft-Moldrup (95 picked)
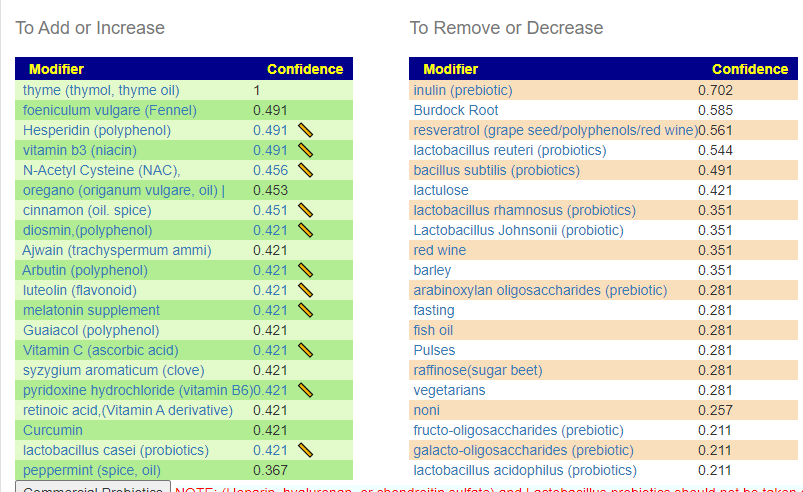
The top items to suggested to take are shown below (meat and B-vitamins are concentric):
I attended this series of talks and for the readers of this blog I link to the videos in terms of my preferences below. The first ones are very technical, Day Three is much easier watching. Unfortunately, they did not post the videos, talk by talks..
Dr. Katherine Amato on Day 3 (hour 3) is likely the best starting one.
Dr. Poyet Day 3 (hour 1) on Industrialization Microbiome
Dr. Iraola Day 3 (hour 0) – on the Microbiomes of South America etc
Day 3 hour 2 — very interesting on the impact on the microbiome of anal intercourse…. there is significant impact.
This is a summary of items that may be the cause. This assumes that a lack of oxygen getting to tissue (or the brain) is the cause. Note that if the brain is tired(oxygen starved), that there may be false signals saying the body is exhausted because the brain does not have the energy to manage the body. The sources are typically from Chronic Fatigue Syndrome. Some of these may be related to the microbiome (lack of studies). It is suspected that many people are borderline (have no apparent issues) and then some event pushes them over the edge into fatigue.
This is intended as a checklist to review with your medical professional. Items should be objectively excluded by actual tests and not subjectively excluded (often a response if the professional does not know how to test). See Hypoxia[2022] and Hypoxia (medical)
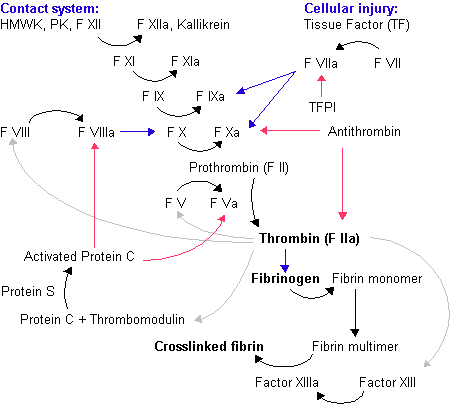
Coagulation Issues
The typical scenario seems to be an inherited or acquired (epigenetic — sometimes from a virus infection) coagulation defect. Some step of the coagulation cascade gets “constipated” with the result being what is often called “sticky blood”. It only takes one step.
If the blood gets thick, it gets slow and hence less oxygen gets to the body and the brain.
Most “blood thinners” only impacts one of these steps (with heparin being the main exception). Taking excessive supplements that impacts the same step may result in long bleeding time or easy bruising.
Note: We are talking about sub-clinical (i.e. not having a stroke or blood clot) levels. The lab levels may not be abnormal, just low (or high).
Low Iron Or Impaired Heme
Hemoglobin is the iron-containing oxygen-transportmetalloprotein in the red blood cells of all vertebrates Hemoglobin in the blood carries oxygen from the respiratory organs (lungs or gills) to the rest of the body (i.e. the tissues). There it releases the oxygen to permit aerobic respiration to provide energy to power the functions of the organism in the process called metabolism. [wikipedia]. Hemogloblin can be inhibited by some chemicals (Carbon Monoxide [2022] and the pH of the blood (Bohr effect [2021]) are the most common. pH is influenced by the microbiome.
It should be noted that SPECT scans show the expected effects of shape- changed, poorly deformable red cells in reducing cerebral blood flow in regions which by chance have smaller than usual capillaries.
Hypoxia and inflammation are frequently co-incidental microenvironmental features of sites of concentrated physiological or pathological immune activity.
Hypoxia activates hypoxia-inducible factor, which is a major regulator of multiple aspects of immune cell function. Consequently, hypoxia plays a key role in the regulation of immunity and inflammation.
The impact of hypoxia on immunity and inflammation is site-specific and cell type-specific.
Pharmacological hydroxylase inhibition, which activates hypoxia-sensitive pathways, is profoundly protective in multiple models of inflammation.
David Bell, M.D. did a study in 1995 (twenty years ago) finding about low blood volume. Cort Johnson has an 2015 update by Dr. Bell that is worth reading. “In contrast, ME patients have a volume that can be as low as 50% of normal.”
Small Heart Size
“A considerable number of CFS patients have a small heart. Small heart syndrome may contribute to the development of CFS as a constitutional factor predisposing to fatigue, and may be included in the genesis of CFS.” [2008]
” Echocardiographic examination revealed that CFS patients with “small heart” had an actually small LV chamber and poor cardiac performance. Cardiac functional changes evaluated by repeated examinations appeared to be directly associated with the severity of their symptoms. Small heart syndrome with impaired cardiac function may contribute to the development of CFS through low cardiac output as a constitutional factor.” [2009]
Enzymes and thus Microbiome
“We’ve discovered that the muscles regulate oxygen consumption in a very precise way using the oxygen-sensitive enzyme FIH,”
” cytochrome P450 (CYP), monoamine oxygenase (MAO), and cyclooxygenase (COX). CYP enzymes are central players.. are important for therapeutic intervention and treatment of neurological and inflammatory diseases”
Note that blood platelets activation is part of the coagulation cascade above.
Snoring, collapse of upper airways and intermittent hypoxia are main causes of smoldering systemic inflammation in patients suffering from obstructive sleep apnea. The systematic inflammation is considered one of the key mechanisms leading to significant cardiovascular complications. Blood platelets, formerly not even recognized as cells, are currently gaining attention as crucial players in the immune continuum. Platelet surface is endowed with receptors characteristic for cells classically belonging to the immune system, which enables them to recognize pathogens, immune complexes, and interact in a homo- and heterotypic aggregates.

Recent Comments