As expected, little agreement with below (see Nightmare for why this often occurs).
Citizen Science Approach
Tinnitus is not usually viewed as a microbiome issue. It was worth checking if it reaches our threshold for inclusion as defined in A new specialized selection of suggestions links. It did, hence this post
Study Populations:
Symptom
Reference
Study
Neurological-Audio:Tinnitus (ringing in ear)
1075
73
Bacteria Detected with z-score > 2.6: found 129 items, highest value was 6.3
Enzymes Detected with z-score > 2.6: found 493 items, highest value was 7.1
Compound Detected with z-score > 2.6: found ZERO items
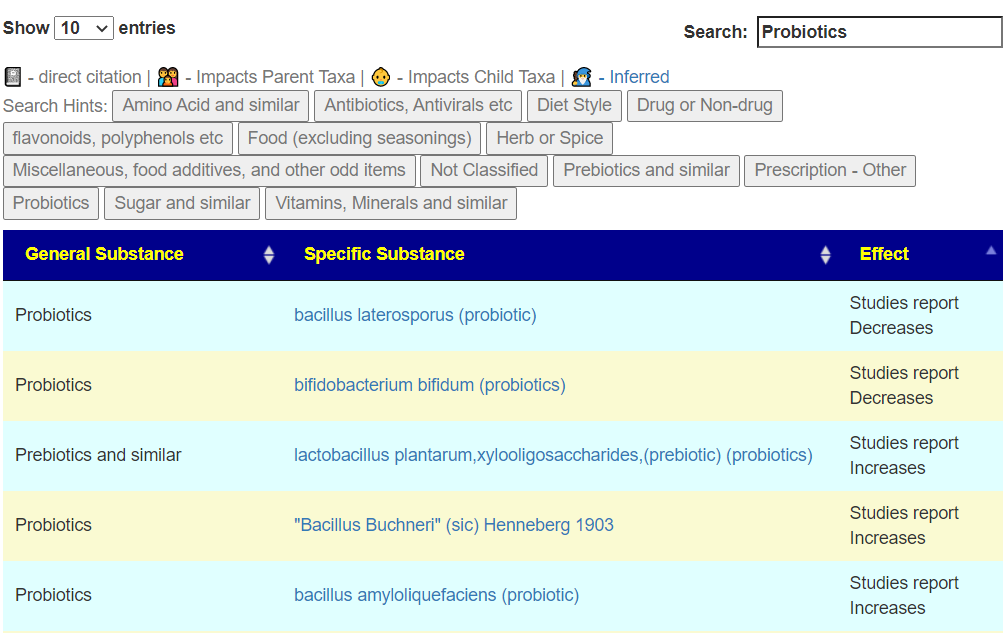
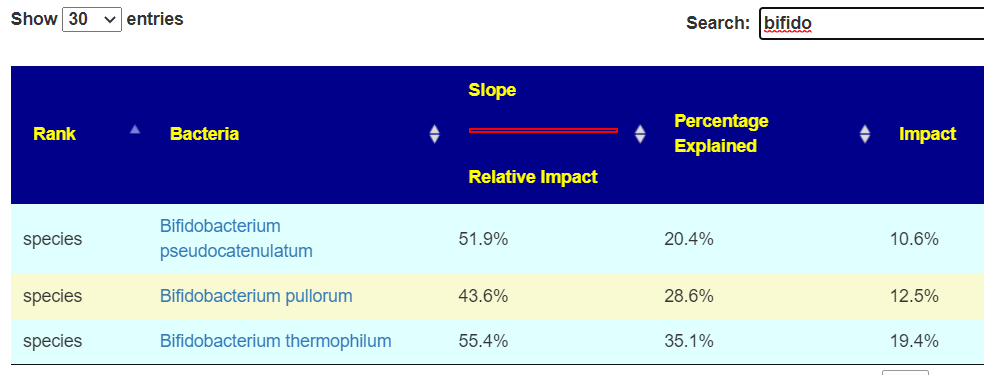
Bifidobacterium probiotics: we have 4 in the top group. Unfortunately none of these species are available at the retail level (that I am aware of). Checking interactions for these 4, there was no significant interactions found with common retail bifidobacterium species, just with the general genus.
As above, all levels that were found significant had too little. I will leave it to the reader to go to Kyoto Encyclopedia of Genes and Genomes to learn about these enzymes (a steep learning curve).
gamma-L-glutamyl-L-cysteinyl-glycine:spermidine ligase (ADP-forming) [spermidine is numbered so that atom N-1 is in the amino group of the aminopropyl part of the molecule] (6.3.1.8)
Nothing was found again!!!! In one sense this was a surprise, in another sense, it hints that the results found significant are not random.
Bottom Line
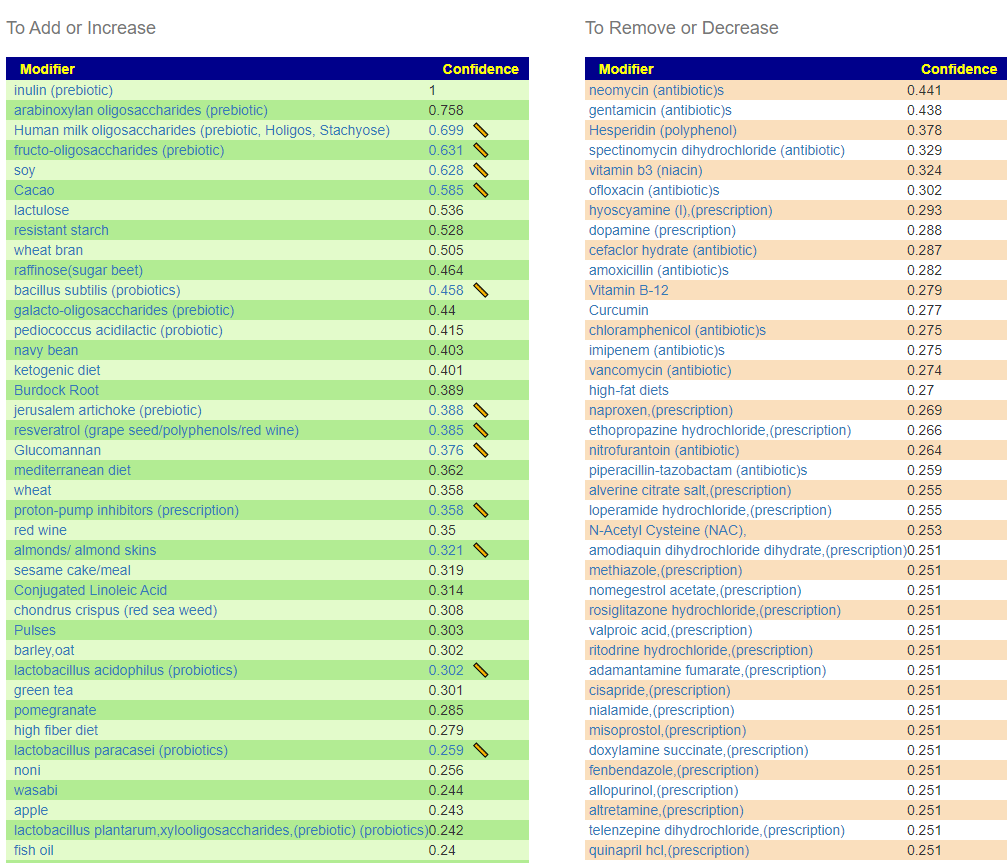
This was an interesting analysis because the dominant deficiencies were in genus that are available as probiotics. In reality, it points to just 3 probiotics: an E.Coli probiotic and two bifidobacterium. Food suggestions will be generated on Microbiome Prescription using an individual’s unique microbiome.
Social Feedback
From The Gut Club: Stool Test Discussion Group
I went and looked at these two in combinations and got a lot of bacteria in common
Suggestions are available on Changing Microbiome tab on https://microbiomeprescription.com/
Study Populations:
Symptom
Reference
Study
Histamine or Mast Cell Issues
1092
56
Bacteria Detected with z-score > 2.6: found 143 items, highest value was 8.5
Enzymes Detected with z-score > 2.6: found 215 items, highest value was 6.1
Compound Detected with z-score > 2.6: found ZERO items
Interesting Significant Bacteria
One of the top items happens to have probiotics that are known to take up residency – are Symbioflor-2 and Mutaflor. . All of these top items are too low levels
Nothing was found!!!! In one sense this was a surprise, in another sense, it hints that the results found significant are not random.
Bottom Line
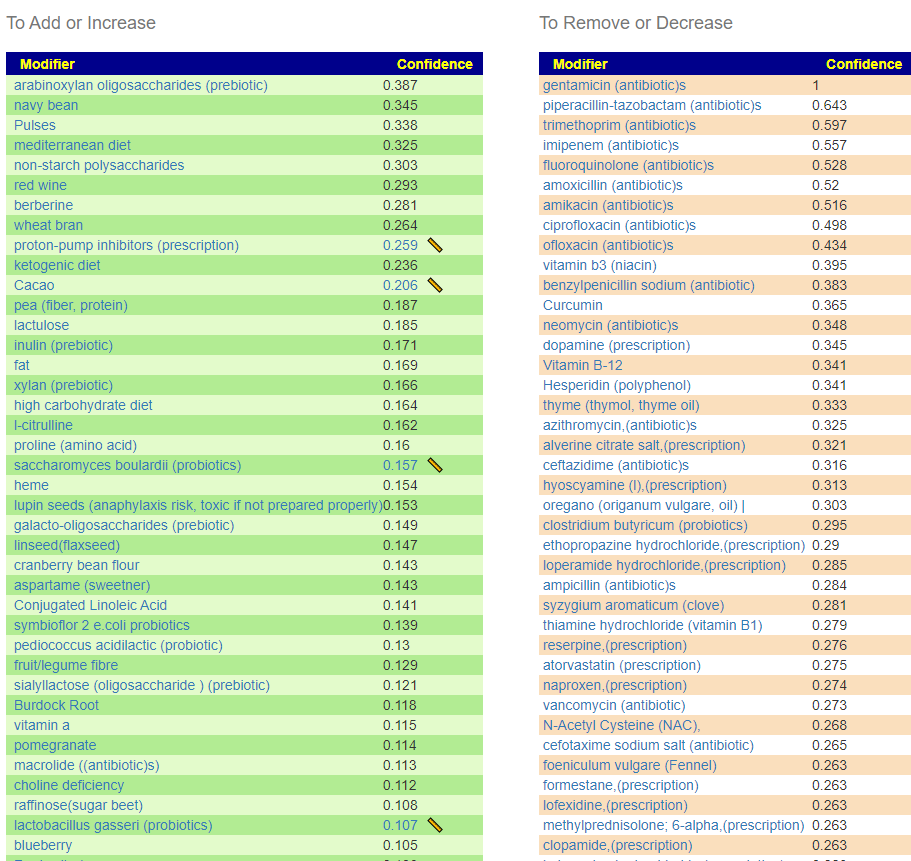
Histamine or Mast Cell Issues appears to a condition of deficiency. Common internet thinking is that it is a condition of a surplus of histamine producing bacteria. It is more likely that the normal histamine consumers are being starvedof enzymes that are needed to stop the accumulation of histamine.
The z-scores for bacteria are lower than Long COVID which reflect the diffusion of bacteria over time. Trying to tackle at the compound or enzyme levels becomes excessively complex. Working at the bacteria level appears viable, but do not expect as many bacteria matches to appear.
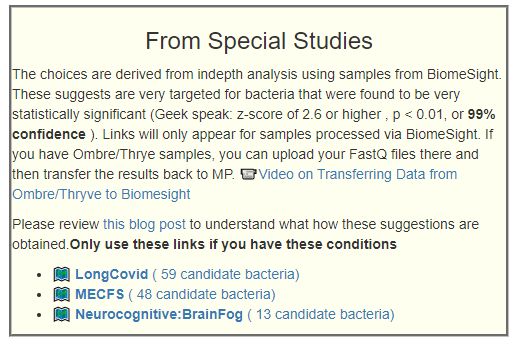
Going to [Changing Microbiome] page you will see a new box appearing. It may or may not contains links to suggestions. It is scoped to BiomeSight interpretation of microbiome data. If you have Ombre/Thryve samples, do not despair, you can move your raw data to BiomeSight and send it to Microbiome Prescription. It is simple and fast as shown in this video ?Video on Transferring Data from Ombre/Thryve to Biomrsight and then to Microbiome Prescription.
Actually, if you have done any of those listed below — you can follow the same process
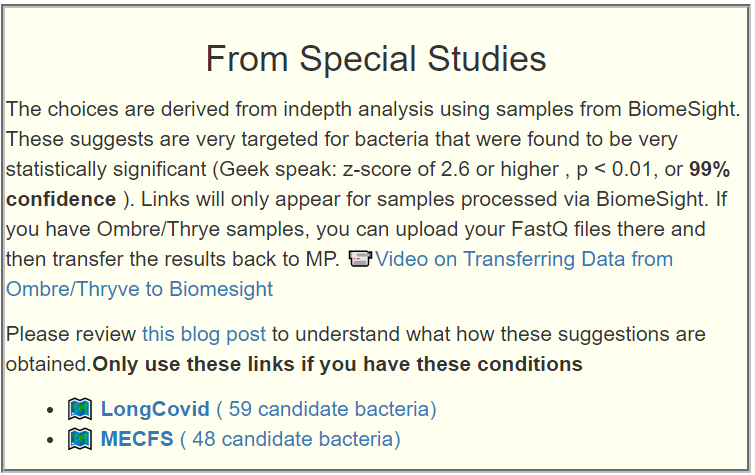
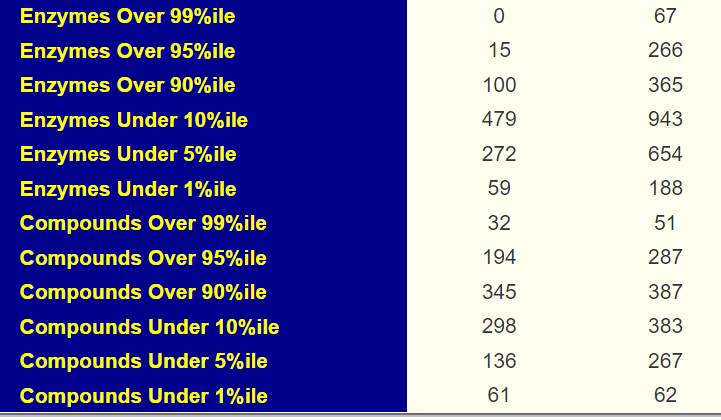
Choices from BiomeSight.comThe counts are the number of matches to the sample currently selected.
What will appear in this list?
First, why Biomesight? — the reason is very simple, there are more samples (20% more at present and increasing then Ombre despite being in business for much less time). The bigger the sample size, the easier it is to find significant shifts.
The criteria is that there must be strong statistical significance for a good number of bacteria. My current threshold is: z-scores must all be 2.6 or higher, that is p <0.01 or 99% confidence. At least 50 bacteria needs to be identified as significant. I will be going thru the symptom list from most frequency reported to less frequently reported. Make sure that you annotate your samples with your symptoms.
NOTE: The numbers below reflect the statistics when various posts were done. The numbers are recomputed at least bi-weekly.
The bigger the z-score (positive or negative), the more significant
I should point out that these bacteria may not be the cause, rather they may be ‘the canaries in the coal mine’ of the microbiome. These studies’ methodology determines association and not causality.
An additional criteria is that they need to be clear abnormalities with the KEGG Enzymes estimate.
I have done two with acceptable results and have made them available. More will be added over time (each one takes a fair amount of time).
US National Library of Medicine Studies are difficult to use
I have their results available and on the site, including as bacteria filters. The problem is that all of those results are very sensitive to the lab being used and the software processing the results. See The taxonomy nightmare before Christmas… for background. In the absence of better information, they are the best we have — until now. With these suggestions, the lab and the software being used are the same and also the one that your results are done by.
Background
Interesting Observation
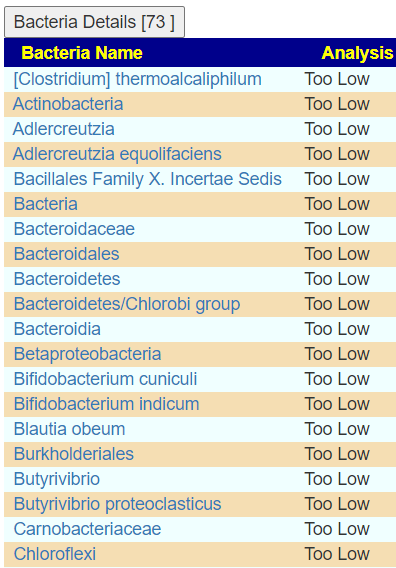
For both of the above, lower levels of a large number of bacteria was the common pattern. These bacteria are not present in all samples, and most of the studies seen on the US National Library of Medicine look only at bacteria found in all samples. That approach will exclude the bacteria that we find are significant.
You may find dozens (in this case 6 dozens!) of bacteria selected
A second item to be aware of is that often those PubMed studies may consist of just 50 people (control and patients). In our analysis, we have 1200+ people with often more then 120 people with a specific condition. Statistically, we are more likely to detect more associations than those studies. It’s a number’s game.
I am still tuning the suggestions engine, so expect reordering of suggestions occasionally. The suggestions pass the reasonableness test.
Quick Cross Validation
I ran the suggestions only for prescription drugs for ME/CFS and the top four suggestions are listed below. Three of the top four are used by ME/CFS physicians such as Dr. Cecile Jadin [Src], Philippe Bottero [src], G. L. Nicolson, M. Y. Nasralla, A. R. Franco, K. De Meirleir, N. L. Nicolson, R. Ngwenya & J. Haier [Src]. These physicians all report various degree of success.
azithromycin,(antibiotic)s
atorvastatin (prescription)
minocycline (antibiotic)s
doxycycline (antibiotic)s
Atorvastatin is an oddity with no studies for its use with ME/CFS. On the flip side, generic statins were high on the avoid list. It would be nice if someone did a clinical trail for this explicit type of statin.
A reader pinged me about new results so I thought it would be good to look at his series of 4 samples from Ombre/Thryve to help people interpret their own results. I am using the tool described in Comparing Samples – Update.
As you can see, the bacteria count do bounce around, with the change from the last sample being a definite improvement
There is a ongoing shift towards overproduction of Enzymes, but this does not cascade into increased compound (Produced – Consumed)
Several of the External Criteria measures showed improvement (2 less) and less showed more (1 more)
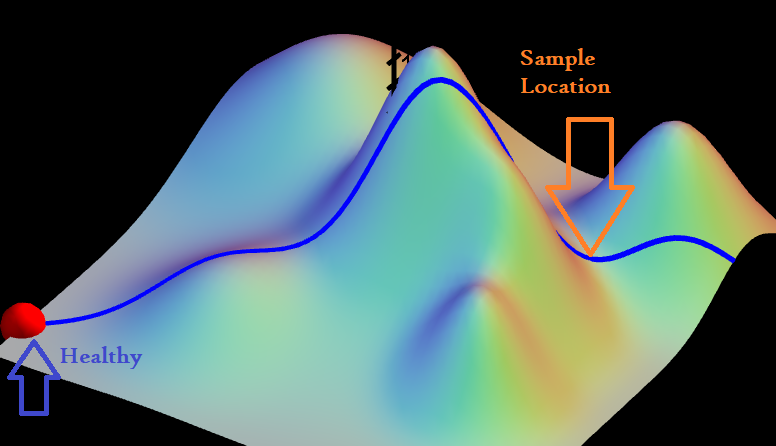
The microbiome is a dynamic system and as shown in the image below, it is not a simple straight path. There is no single measure that indicate the current status of the gut, rather a variety of measures.
The latest sample showed (compare to prior):
Drop in compound extremes
Increase in high Enzyme production — this may hint at the body stocking up on supplies for an attack of troublesome bacteria
A drop of bacteria out of range by both external criteria and Microbiome Prescription Criteria.
Reader’s Comments
This round I restarted the b.lactis by custom probiotics. I did it last test and took a month break and it came up again. 1st round doing it , the herx was kicking my butt and I lasted 10 days. This time around , only did 1 scoop at night and I was still herxing and sleeping 8 hours hard. After day 10 I did half dose mornings and half at mid day or night. Much better tolerance and body seems to respond well. Calmer, better sleep, allergies seem better.
Now also taking rice bran, blue berries, Lactoferrin for iron, and a lot of the other high priority items. I try playing basketball 1 time a week to check my progress. I have plenty of energy to play, but if I play too hard I crash still exactly 5 hours later (impaired sleep, brain fog, fatigue , headache, inflamed stomach lasting exactly 24 hours) . Then back to normal the same day. Tried the symptom /handpick bacteria tool and focused on picking PEM/brain fog/sleep with associations. The top modifier for that was glycemic (licorice root tincture). Added that to the mix this week. Still crash, but notice some weight loss and less belly inflammation after I play. Overall improvement in sleep and anxiety. I am still a work in progress and could be better, but seeing improvement. My post exertion crashes are the thorn in my side I haven’t been able to dent much, no clue why I crash exactly 5 hours after every time but can play and feel find right after. Couple more days of b lactis and I switch to my next probiotic L.gasseri. Then will test again in about 2 weeks!
Mystery of Crash after 5 hours lasting exactly 24 hours
I have a few suggestions to try — looking at possible mechanisms..
At 3 hrs (2 hrs) before crash — take 3 regular aspirins
What this is attempting to test is whether coagulation is a factor
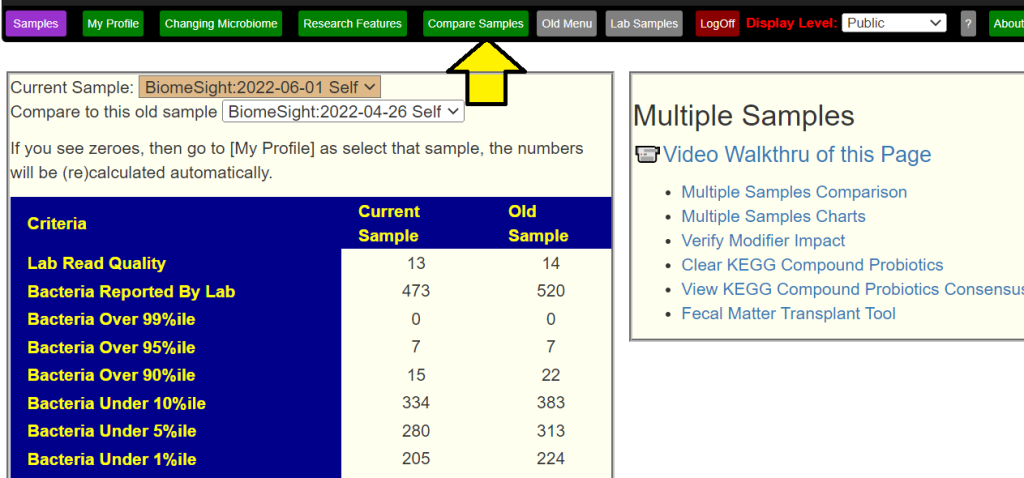
A reader asked me to compared her latest sample to her prior samples. Comparing samples can be time consuming and complex, so I revisited my past comparisons posts and created a table that saves time and add clarity.
Location of the comparison table
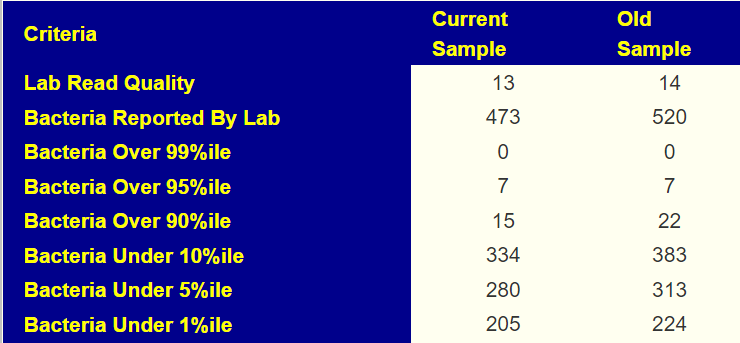
Bacteria Report
Lab Read Quality indicates the numbers of bacteria that the lab obtained. In this case, the quality of the samples were similar
This impacts Bacteria Reported. In this case 1/14 less, and the bacteria count is about 1/14 less. If there was a severe change, then we wish to understand why
Bacteria Over/Under: Between samples we would like them to be reduced (less extremes). If lab quality goes down or up a lot, then the numbers may need to be adjusted for comparison.
We see more than a 1/14 drop, which indicates a better microbiome.
Lab Relatives
If both labs were done with the same provider, then this section will appear. In this case we see that rarely seen bacteria goes down – a good sign.
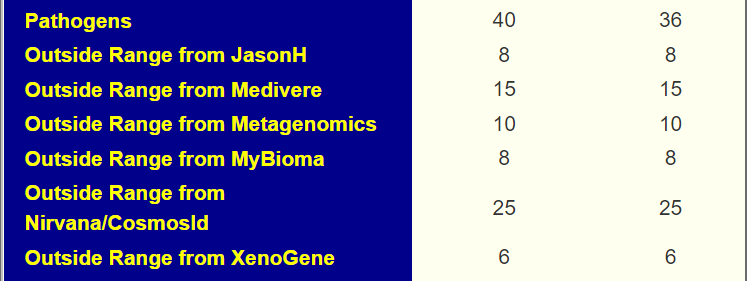
Foreign Criteria
This applies various foreign criteria to the samples. The increase of pathogen is a potential concern. I tend not to focus on pathogens because the source data usually report “higher” or “lower” only.
Microbiome Prescription Criteria
This reports on the main approaches used for generating consensus suggestions. All of them indicate little change except KM which suggests improvement.
PubMed Conditions
This uses the literature from the US National Library of Medicine to estimate likelihood of having various conditions. It is a fuzzy estimate due to the what the studies report. In this case we see good improvement across the board.
KEGG Criteria
As above, we want to reduce extreme values (represented by high and low percentiles). What we see below is very significant improvement across the board.
Bottom Line
The above are the list of my first go-to items comparing samples. If someone has followed the suggestions from Dr.A.I. between samples (or done other things), it give a quantification of the changes that occur across multiple dimensions.
In this case, we see significant improvement over a few months! It should be noted that the various external criteria show no apparent changes, the deeper dive that Microbiome Prescription does show significant positive changes.
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
Dr. A.I. is not a person ,it stands for Artificial Intelligence – a compute program that takes facts (in this case, well over 10 millions) and use logic to come up with suggestions based on probability.
Back Story
I’ve had severe gastric symptoms for about 15 years (unstoppable daily acid reflux, severe bloating and food sensitivities/very reduced diet, upper digestive pain, chronic UTI, chronic tender lymph nodes), and milder related symptoms my whole life (recurrent sore throat, allergies, eczema, psoriasis, vitiligo, depression, anxiety, fatigue ). Since I haven’t been able to fully resolve them, I’ve also developed comorbidities (Hashimoto’s, thyroid microtumor). I’ve found your website and have gotten a bit better and have hope to keep improving. I’m trying to understand your videos and instructions on how to use your AI the best I can.
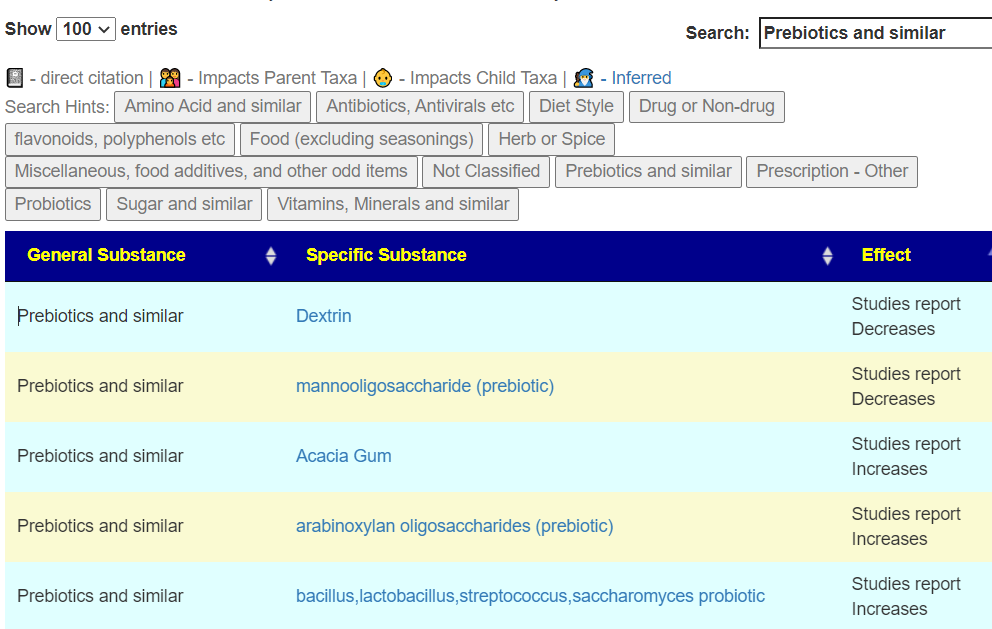
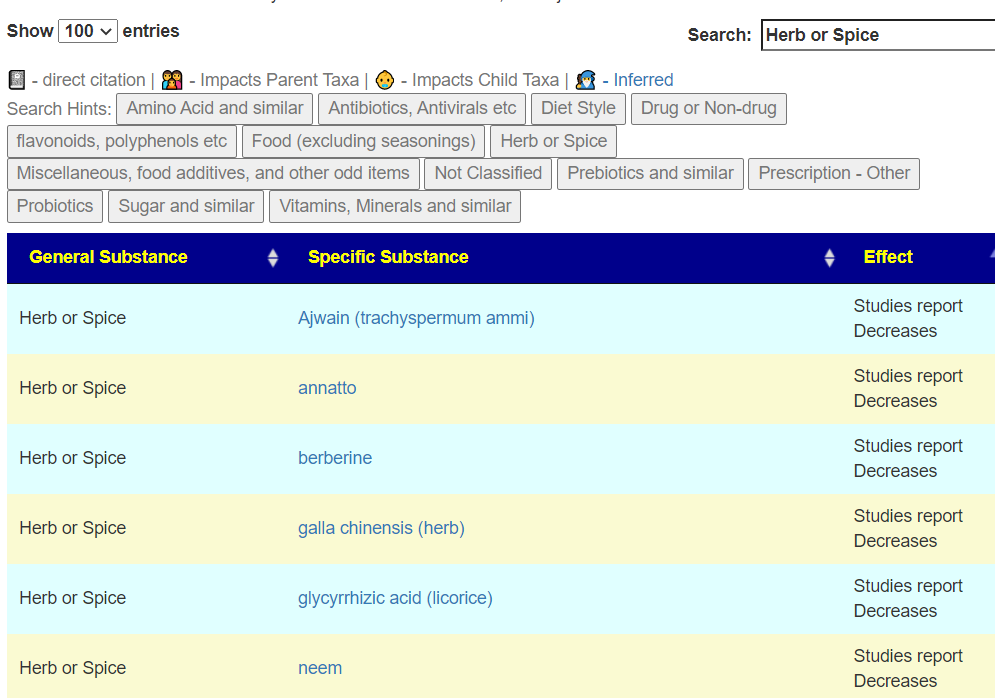
I did a number of Ubiome tests in its day, unfortunately I only downloaded the raw data for two of them, which I uploaded to your website. I am attaching other gastro tests that I believe I cannot upload since there’s no raw data, they may be useless. I also have uploaded my recent thryve test, and I plan on having more tests done to monitor progress. I have been going back and forth with microbiome labs to try to get the raw data, we’ll see. I’m “hooked” to herbals, taking bidens for UTI for years, and tied to foods like cabbage and meat, and my microbiome shows signs that it needs a wider variety of foods as well as a rotation of probiotics, herbal antibiotics, and foods. I react very strongly to prebiotics. I can eat cruciferous veggies, meats, fish, low-carb, low oxalate NO: starches, grains, cereals, fruits, sugars, eggs, milk, legumes. Neem helped a bit with oxalate sensitivities. A few probiotics helped with mood. Then I get stuck in needing these things, the flora develops resistance.
My husband and I are both following your sites. Thank you again for all you do.
Addendum
Sending the first draft results in the following information, see Addendum Discussion at the bottom.
I am thankful you have taken my sample to analyze. This is an incredible amount of work and very illuminating on how you approach the tools on your website. I agree, my situation seems to be a bit contradictory and difficult to approach. Here are some comments and reactions to your ideas—I am not suggesting these should be included or modify your post, that is up to you…
Firstly, I would like to say, that I have already been implementing a few of the top probiotic and flavonoid suggestions for a couple of weeks and I do feel that many of my symptoms have either improved some or changed and are changing, which, for at least a decade seemed unmovable. Other are unchanged. I do not think I mentioned this before, but in general I have less hepatic region/upper digestive discomfort and when I do have some, it’s less aggressive and I recover faster. I have related this symptom in the past to oxalate intolerance. My UTI feels much better, though it is not fully gone and my reflux has more frequently better days, though these come and go. My mood has improved and I tend to be more hopeful. I’m a bit less fatigued.
The things I have so far implemented are:
Before I implemented any of your website suggestions, I used bidens and neem which helped a lot.
When I took the Ombre sample I had been doing high doses of reuteri, plantarum, longum, casei for a couple of weeks… I wonder if these have anything to do with the high Kegg.
I have been taking P. acidilactici as a base…
I did 2 courses of Symbioflor 2 (2 bottles) and Enterogermina, which I think helped. I think some results suggest I may be low in good strep too.
I am now on a run of B. coagulans and Equilibrium (this last one because I test low in alpha diversity)
I am planning a run of L. sakei and Enterogermina again next… The prescript assist folks refuse to share an updated CoA with me.
I am taking artemisia, planning to alternate with neem, bidens, cryptolepis/sida
Regarding dietary recommendations, these are mostly non-negotiable at this point due to intolerances and allergies. One single pistachio a week ago gave me more bloating and worse symptoms for a couple days, so it is unlikely that nuts will be part of the solution initially. Rice bran is a big question, I have been searching for a brand that has low heavy metal analysis, but generally, I do not tolerate prebiotic fibers well at all. This is subject to change, for instance neem did help minimize a bit oxalate intolerance.
I have been using quercetin and I am waiting for a full-spectrum cannabinoid extract to arrive to try. I have had a complicated relationship with licorice in the past, but I am willing to try again.
I do not think I can do oats yet, starches and cereals are too challenging.
The foods I eat that contain choline are salmon (once a week), beef daily and cruciferous vegetables which are the bulk of the veggies I eat because I tolerate them well, probably because of low oxalate content.
I think some killing is necessary along with the rest. The Mircobiome FX people recommended their B. subilis strain for this purpose (in their test C. difficile and B. fragilis were high) but it’s not recommended by the AI.
I will follow up with another Ombre test soon.
Analysis
Comparing results from different labs has risks. In this case, I thought it may be worth it. (I was debating about purging ubiome data since the data is stale and they consume a lot of space — I will keep them available).
I should note that I recently revised the code to use lab specific percentiles for ubiome, ombre and biomesight. This means that the numbers are more accurate despite the oddities of different labs.
05-08 Ubiome06-29 Ubiome2022 Thryve/Ombre
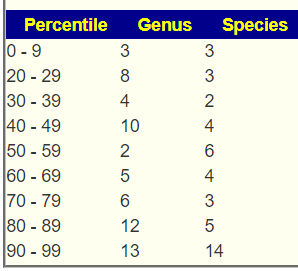
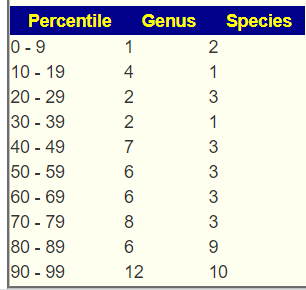
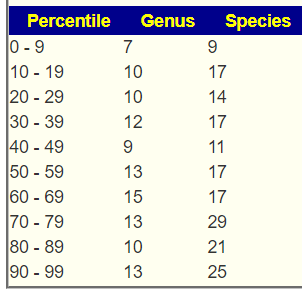
The ubiome samples had a over representation of bacteria that had extreme values (at 90% or higher). The Ombre sample had a better balance, but still with some overrepresentation of bacteria with extreme value.
Dr. Jason Hawrelak
Jason’s criteria was developed using uBiome data. And all of the samples are good. There were no significant potential medical condition on any samples. The same number of bacteria deemed unhealthy were seen on each report.
05-08 – 98.8%ile
06-29 – 95.6%ile
2022 – 95.6%ile
The new Over and Under Population Experimental Feature
With this feature, we see much more difference between samples. The latest sample suggests that the issue may be related to too much being produced.
05-08 ubiome06-29 Ubiome2022
The Road Forward
There are a lot of health issues. The site supports targeting of specific issues (because that is how some people wish to proceed). In general, I have been finding the consensus with perhaps 1 or 2 specialized set of suggestions appearing to give good results. We are dealing with fuzzy data everywhere and should resist temptations to over engineer suggestions.
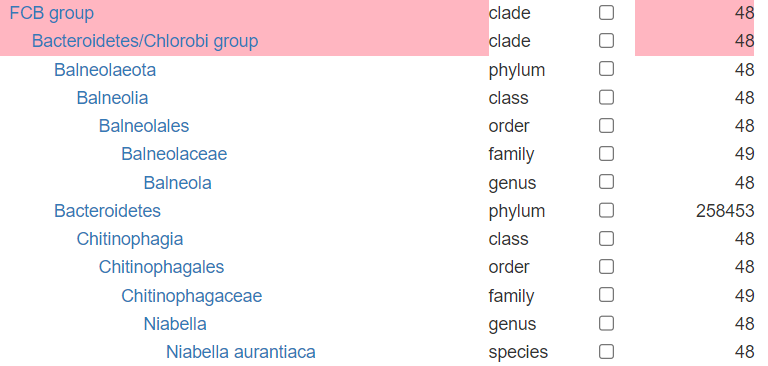
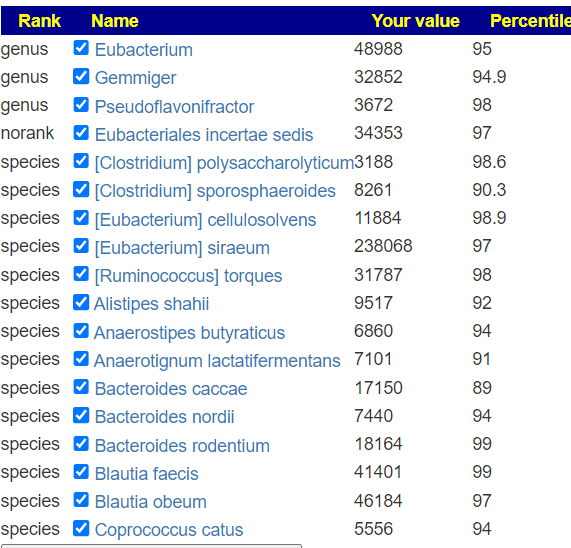
I looked at the Taxon Hierarchy and selected items in Ombre. There was something odd with the data as shown below.
The work around is to keep choices to the family, genus and species level. Picking items with a count of 2000 or more only. The selection is shown below
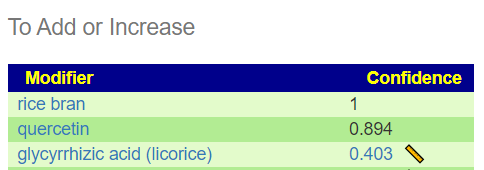
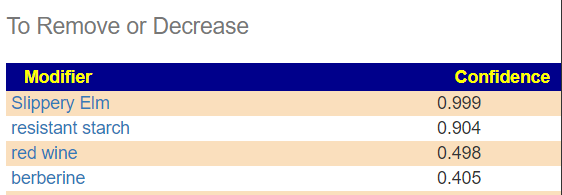
The result of the hand picked is shown below, I usually truncate the list to 0.4 and higher. Both lists are relatively small!
Avoid: Barley, Rye, Wheat (a bit fuzzy, different types are on either side)
Probiotics
The top ones selected using KEGG may be hard to find in many places: enterogermina, Sun Wave Pharma / Spor Sun. The weight give them is light, so likely not much impact would be expected.
This is a sample which I term “on the border of what we have knowledge about”. We can see the issues, but lack studies that we can use to correct the issues. I have encountered one like this before and after doing the first set of suggestions, the microbiome moved into a state where we are able to get a normal number of significant suggestions from. I hope this is the case here. Samples like this are a bit frustrating to me..
I would suggest stocking up on Spezzatina (perhaps even do what we did, buy a whole kilogram (2.2 lbs) of Amarelli Spezzatina [note: no sugar at all!]) and using them through out the day.
We had the space and purchased our own infrared sauna a few years ago (on sale at Costco). If you follow that path, remember lots of water and slowly work up duration. For water in the sauna, we use Gerolsteiner Natural Mineral Water (available from Trader Joe’s) because of it’s high mineral content.
Reduce the foods high in choline in your diet (see the list here)
Keep nuts (Costco/Trader Joe’s?) handy for snacks. Remember peanuts are NOT nuts.
Addendum Discussion
First, and most important: items are suggestions only. People should do only what works for them. Each item increases the odds of a positive shift a little, key word is a little. Occasionally, I will get emails from people who experienced awesome changes from a single item (Neem and Tulsi are often cited). If something is not mentioned and it helps — keep doing it!.
“a complicated relationship with licorice in the past” In follow up email, the cause appeared to be licorice oil being used. For licorice, I strongly favor the Italian Spezzatina. This person had no problem with the Spanish equivalent… when there is an item with a suggestion, before discarding entirely, consider the following:
If in an oil, you may be reacting to the carrier and not the substance. On occasion, it can be preservatives in it. For example Mountain herbs is 35-45% alcohol
The dosage may be too high to start, I always advocate starting low and slowly increasing
We rarely buy prepared capsules, instead we buy organic bulk and make our own capsules. It is both cheaper, organic sourced (very few supplement bottles cite organic) and less likely (but not impossible) to have the issues cited above.
Concerning salmon, etc. Remember everything is odds. Nothing is guaranteed. You want to shift your odds where practical.
One item that may be worth trying is Akkermansia Probiotic (link with 30% discount). Both my wife and I have, and are, using it — it has definitely made changes (I had almost the same amount that he has – 52%ile, and there was a change). The link is for by subscription — of course, once you get your first bottle, you can just suspend the subscription.
A reader asked this question about Lactobacillus Salivarius (NCBI 1624). I am doing it for this single strain — for a mixture, just do each one and consolidate the results.
FIRST, login to access more information. Most of the information below do not require a login.
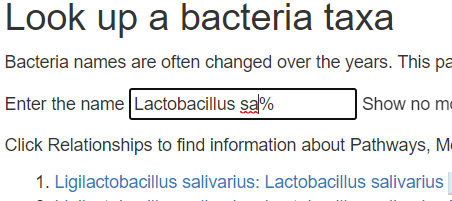
SECOND, look up the species
From https://microbiomeprescription.com/Library/Lookup?name=Lactobacillus+sa%25&top=200
THIRD, click on that link above, this will show what helps or hurts this probiotic. Click on [Probiotics] for a start — you want to make sure that other probiotics you are taking support it. Note that I have gone thru a few retail mixtures and the probiotics fight each other!Buyer beware of mixtures! In this case we have 26 listed. 24 are friendly and 2 are hostile (bacillus laterosporus (probiotic), bifidobacterium bifidum (probiotics)
FOURTH, There is one more source of information, by looking at the associations in microbiome report. On the same page above click the red interactions button.
On the https://microbiomeprescription.com/library/details?taxon=1624 page
This will show a page of bacteria that are associated positively or negatively with this bacteria (i.e. probiotic). You will need to type in the family names:
These have a positive impact (i.e. IMPACT is > 0)Other lactobacillus are friendly
FIFTH, check prebiotics (they are often bunddled in probiotics) — 18 are friendly and two are hostile
SIXTH Check Herbs and Spices, the results here may impact the rotation of herb and spices. You want to take friendly when you are doing the probiotics. Although they will likely not take up residency, the chemicals that they produce while in transit are good… you do not want to reduce the production of those chemicals.
Bottom Line
Doing your homework will get much better results than just tossing them in your mouth with something that will inhibit it!
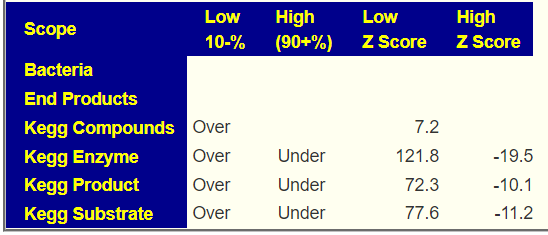
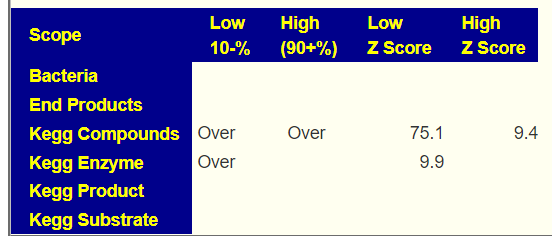
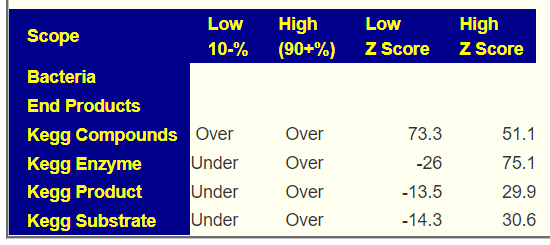
This is using data from the study being done with BiomeSight. We will only use their samples. After the first review, a z-score of 6.4 or higher (or a lots of items) was set as a cutoff point. The following ignore False Detection Rate.
Conclusion: the ENZYME production of the microbiome is by far the strongest indicator.
The reference set consists of 1037 heterogenous samples (i.e. no Long COVID, but a variety of medical conditions) and 154 samples with Long COVID
Taxon Patterns
Care needs to be taken with these numbers because the frequency of reporting on a bacteria is a factor that impacts the z-score. The data for this table is available at Citizen Science site and independent analysis is strongly recommended. This table is a simplified view of very complex data.
tax_name
tax_rank
No Symptom Mean
Symptom Mean
Z-Score
Change
Terrabacteria group
clade
715040
520885
10.4
73%
Firmicutes
phylum
652452
502830
9.0
77%
Tenericutes
phylum
2562
6362
-7.9
248%
Eubacteriales
order
609888
482468
7.9
79%
Mollicutes
class
2562
6362
-7.9
248%
Clostridia
class
613743
487719
7.8
79%
Emticicia oligotrophica
species
769
2553
-6.8
332%
Faecalibacterium prausnitzii
species
100292
142415
-6.7
142%
End Product Patterns
End products only had a single item above our 6.3 z-score threshold with a very small shift.
EndProduct
No Symptom Mean
Symptom Mean
No Symptom StdDev
Change
H2
1329
1307
6.6
98%
KEGG Enzyme Patterns
This is where we see a massive number of patterns(182!!) with very high z-scores (i.e. 6.4 or higher). This hints that the bacteria associated with these enzymes may be a good target to modify.
Products are the output of enzymes. Various enzymes may produce the same product. Our starting assumption was that products would have stronger association than enzymes. That was not shown in the data.
Subtrate are the fuel for enzymes reaction. Various enzymes may consume the same compound. Our starting assumption was that substrate would have stronger association than enzymes. That was not shown in the data.
CompoundName
No Symptom Mean
Symptom Mean
No Symptom StdDev
Change
Dihydrourocanate
38026
55395
-7.8
146%
(S)-3-Hydroxy-3-methylglutaryl-CoA
34820
50269
-7.4
144%
Electron-transferring flavoprotein
106880
149551
-6.9
140%
threo-3-Hydroxy-D-aspartate
760
2532
-6.9
333%
3-(Methylthio)acryloyl-CoA
757
2494
-6.8
329%
3-Hydroxy-3-(methylthio)propanoyl-CoA
757
2494
-6.8
329%
3-Oxopropionyl-CoA
757
2494
-6.8
329%
ADP-sugar
772
2553
-6.8
331%
Aryl dialkyl phosphate
772
2553
-6.8
331%
beta-D-Mannose
772
2553
-6.8
331%
D-erythro-3-Hydroxyaspartate
761
2532
-6.8
333%
Pseudouridine
105195
147050
-6.8
140%
N4-(Acetyl-beta-D-glucosaminyl)asparagine
759
2473
-6.7
326%
Short-chain acyl-CoA
103536
144711
-6.7
140%
(2-Amino-1-hydroxyethyl)phosphonate
752
2431
-6.6
323%
trans-2,3-Dehydroacyl-CoA
68745
95899
-6.6
140%
(S)-4-Hydroxymandelate
113176
152269
-6.5
135%
5-Methylphenazine-1-carboxylate
750
2381
-6.5
317%
Hexadecanoyl-[acp]
1468
4753
-6.5
324%
Kanamycin B
34729
48298
-6.5
139%
Octadecanoyl-[acyl-carrier protein]
734
2376
-6.5
324%
(1E)-4-Oxobut-1-ene-1,2,4-tricarboxylate
739
2338
-6.4
316%
2-Deoxystreptamine antibiotic
35916
49415
-6.4
138%
Adenylated molybdopterin
119083
159672
-6.4
134%
Alditol
763
2429
-6.4
318%
beta-Carotene
720
2314
-6.4
321%
Molybdate
119083
159672
-6.4
134%
Bottom Line
Several years ago, I hypothesized that a symptom or condition is the result of a coming together of many small deviations in individual bacteria representation. There may be 10 different combination of bacteria with none overlapping causing a symptom. The inspiration for this was observing the literature and experience of people with Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) — a sibling condition to Long COVID. This model is contrary to the common belief that there is a single or small number of items that is the cause. My looking at Brain fog (using same technique as above Brain Fog: Microbiome scents…) came up with nothing. That was not desired, but almost expected because that population is very heterogenous for cause with a long time since the triggering event for the microbiome to diverge from each other (often treatment attempts would be a factor). With long COVID, we have a short time since the triggering event and the people tend to be treatment naïve, This makes finding patterns a lot easier (when you look under the right rocks!).
Almost everything is overproduction. This may be caused by the immune system ramping up to provide fuel to fight COVID. The microbiome is stuck in an on-state, likely with cross talk between enzymes keeping it stuck on. The term of the Pasteur Institute for Tropical Medicine, “an occult infection” describes the behavior seen nicely.
Addressing the few microbiome shifts is one approach — but the enzymes dominate in both statistical significance and number of items, It is likely the best path to address the enzymes instead of individual bacteria.
At present in our citizen science database we have samples reporting brain fog for:
Biomesight: 124 samples
Ombre/Thryve: 151 samples
UBiome/Thryve: 170 samples
Results from different labs cannot be safely aggregated, so we will investigate on a lab by lab basis. One lab will read data as bacteria A and a different lab as bacteria B.
Biomesight returned nothing, Ombre just 7 candidates and ubiome 23. There was nothing in common.
KEGG Substrate
Biomesight returned 2 candidates, Ombre returned 42 candidates and ubiome 86. There were a few things in common between Ombre and uBiome. False Detection rate is a risk.
(S)-Ureidoglycolate – much higher consumption
2-O-(alpha-D-Glucopyranosyl)-D-glycerate – much higher consumption
I am disappointed in not finding many associations. I will pass the torch to others to see if there is literature connecting these to coagulation or vascular constriction/dilatation .






Recent Comments