Backstory
Hello, I’m sorry to message you privately, but I’m reaching out for help regarding my 15-year-old daughter, who has been homebound with ME/CFS for 2.5 years since contracting COVID in 2022. I came across your story on Facebook, and I felt truly inspired by how you managed to overcome ME/CFS by working with your microbiome. We are currently trying to follow a similar path.
We’ve recently done a Biomesight 16S test for her. As expected, it showed typical deficiencies, like a lack of Lactobacillus bacteria, along with an overgrowth of sulfate-reducing bacteria (possibly SIBO). Since we’re unsure how best to approach this dysbiosis, we sought the help of a microbiome specialist through Viola Sampson in the UK. She recommended lactulose, Lactobacillus reuteri, Lactobacillus rhamnosus, Lactobacillus plantarum, Bifidobacterium breve, along with Allicin and Goulds tincture from Australia. We’re just beginning this treatment, so it’s hard to say much about progress yet. We’ve started with Lactobacillus rhamnosus, plantarum, and breve, and she’s doing well with these so far.Honestly, I’m a bit concerned about these Lactobacillus bacteria because I read somewhere that all people with ME/CFS have some degree of lactic acidosis, so I’m worried that these probiotics might produce even more lactic acid. When I brought this up with my practitioner, she wasn’t aware of it.
I also uploaded a Biomesight test of my daughter to your Microbiome Prescription page, but I noticed that your site has somewhat opposite recommendations for her microbiome, such as advising against lactulose. To be honest, I’m struggling to navigate your page, and it’s a shame because I truly want to follow the recommendations accurately. I was hoping to identify which specific antibiotics or probiotics might be the best fit for my daughter’s case, but I’m not sure how to interpret that information from your site.
Currently, my daughter is mainly dealing with POTS (Postural Orthostatic Tachycardia), histamine intolerance, chronic fatigue, anxiety and panic attacks, and digestive issues. She’s become highly sensitive to various foods and medications, and it all points towards dysautonomia. Although she’s taking many supplements, she reacts to some, like iron supplements, which I suspect might be due to certain bacteria that feed on iron. She has many vitamin deficiencies, yet we can’t supplement effectively due to these reactions. It’s so difficult to manage.
I apologize for the long message, but I wanted to be as clear as possible about her situation. I’d be incredibly grateful if you could review her Microbiome Prescription and offer any insights on what stands out in her microbiome and where we might start. I’m also curious about any thoughts on the potential use of antibiotics or probiotics, as our microbiome practitioner is generally against antibiotics, though I know some people with ME/CFS have found success with a well-planned antibiotic approach.
Here, I am including the link to our microbiome analysis from Microbiome Prescription.

Analysis
First, disagreement between sites is well known and explained here: Why sites suggestions disagree on the same data. Microbiome Prescription tuned it’s advice by doing cross-validation for several conditions, for example: Cross Validation of AI Suggestions for Nonalcoholic Fatty Liver Disease. ME/CFS was the first explicit studies done. To the best of my knowledge, no other microbiome site has done cross-validations of their suggestions and been public in showing results.
Individual practitioners are hard to evaluate because they often find patterns that works for some people by trial and error. It is a rare practitioners that can provide documentation on their suggestions.
Quick boot strap
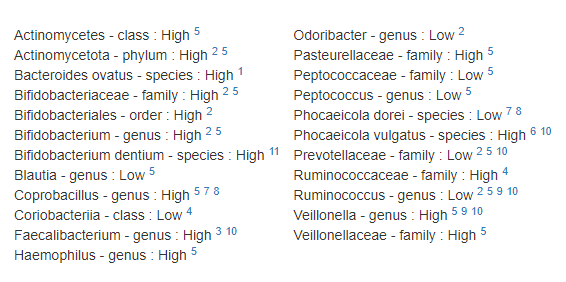
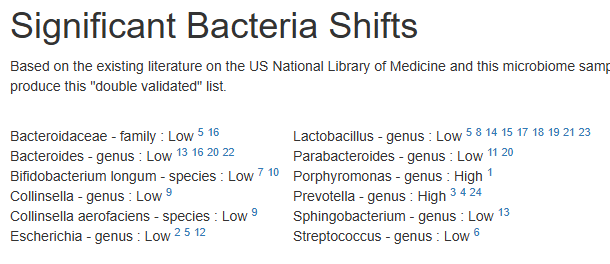
Long COVID is one condition that has a built in cross validation list of suggestions. This is on [Old Ui] / [Changing Microbiome]. POTS is not currently on the list because of insufficient studies.
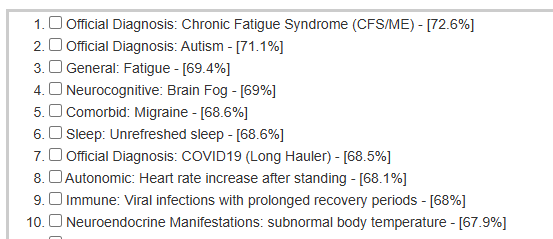
This identified the following bacteria as being probable according to the published literature. The number of cross reference numbers after each item, indicate the number of studies For example Ruminococcus – genus : Low was reported in 4 studies.
The suggestions (based on microbiome shifts cross reference with substance that improved ME/CFS from studies are below. The number of cross reference numbers after each item, indicate the number of studies – as above. This leads to the best suggestions being the ones with the most cross reference. Thus:
- Magnesium supplements – 6 studies
- Vitamin B9 – 6 studies
- Coenzyme Q10 – 6 studies
- Far infrared Sauna – 4 studies — as a personal note, we purchased a small one at Costco and use it regularly as preventative.
- Vitamin B1 – 3 studies
- Omega-3 – 3 studies
- Ribose – 3 studies
- licorice – 3 studies — we usually use Spezzatina and just suck on them
- carnitine Amino Acid – 3 studies
- Melatonin – 3 studies
- Selenium supplement – 3 studies
This is a significant list and I noticed that none of these were suggested by Viola Sampson despite published literature saying they help.
My suggestion would be to add one of these every three days, noting any changes that results. For dosages see Dosages for Supplements, start low and work up. The above will take a little over a month. All of these items can be taken continuously and together.
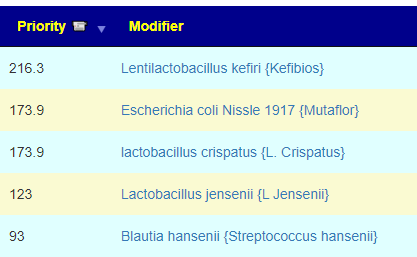
Probiotics
Probiotics are a popular “cure-all” which in some cases help and in other cases hurt. For example, lactobacillus probiotics often will increase brain fog.
Looking at probiotic with positive values, most are actually hard to obtain. For example Kefibios is only sold in Italy. Mutaflor in only a few countries. Of the choices, I would try Mutaflor after adding in the items above — but be warned, it may trigger severe die-off.
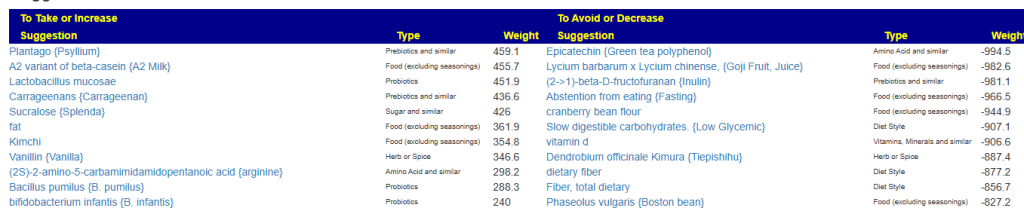
Top items
The list below are other things that likely have never been studied for ME/CFS but should have significant impact on the bacteria shifts.
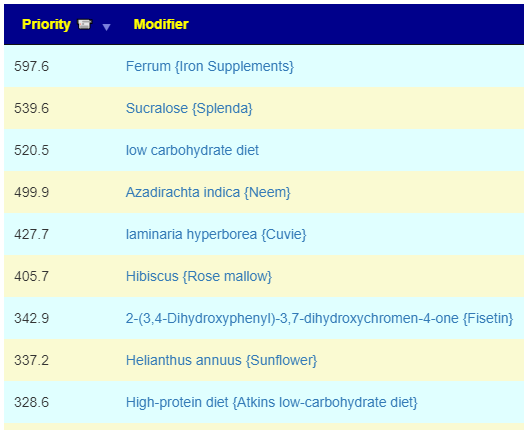
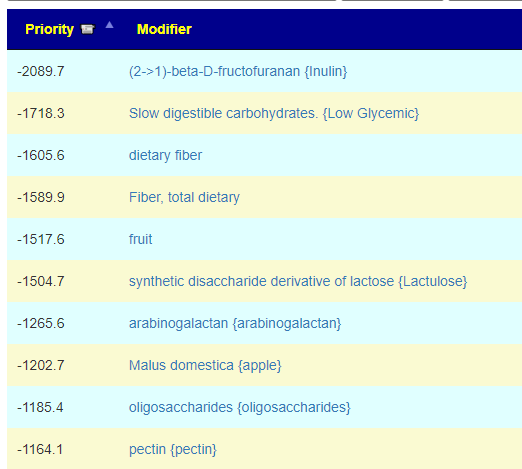
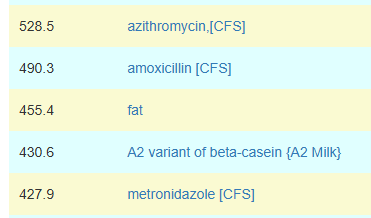
On the other side, the following should be avoided:
Food Site
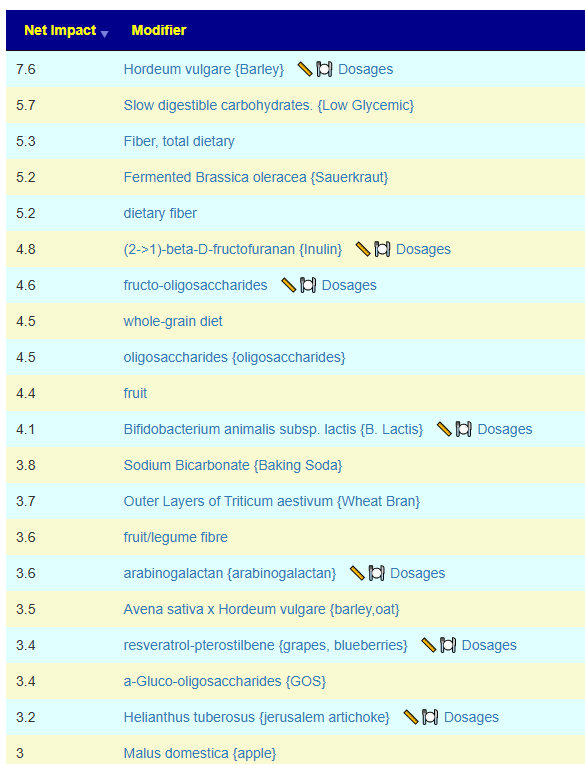
Going to https://food.microbiomeprescription.com/ and entering your login token will show the nutrients computed to help most. Iron supplements or food high in iron is at the top; for example thyme, basil, and my favorite Caterpillar, roasted ;-). Both herbs have positive recommendations.
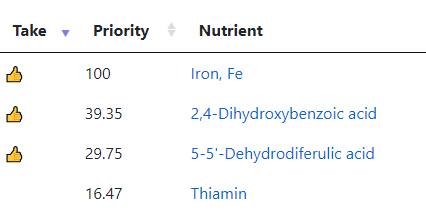
The second one is found in cranberry (a suitable seasonal food) and raw Olive. The third one is found in maize, rye and Hard wheat, semolina. HOWEVER, none of these are recommended in the list of suggestions. I usually cross reference the two for safety.
Next Steps
I would continue with additional suggestions (1 and 2 studies) at the same pace. Two weeks after the last one was added, do another microbiome test (same firm of course) and get back to me for a follow up analysis if needed.
Postscript and Reminder
As a statistician with relevant degrees and professional memberships, I present data and statistical models for evaluation by medical professionals. I am not a licensed medical practitioner and must adhere to strict laws regarding the appearance of practicing medicine. My work focuses on academic models and scientific language, particularly statistics. I cannot provide direct medical advice or tell individuals what to take or avoid.My analyses aim to inform about items that statistically show better odds of improving the microbiome. All suggestions should be reviewed by a qualified medical professional before implementation. The information provided describes my logic and thinking and is not intended as personal medical advice. Always consult with your knowledgeable healthcare provider.
Implementation Strategies
- Rotate bacteria inhibitors (antibiotics, herbs, probiotics) every 1-2 weeks
- Some herbs/spices are compatible with probiotics (e.g., Wormwood with Bifidobacteria)
- Verify dosages against reliable sources or research studies, not commercial product labels. This Dosages page may help.
- There are 3 suppliers of probiotics that I prefer: Custom Probiotics , Maple Life Science™, Bulk Probiotics: see Probiotics post for why
Professional Medical Review Recommended
Individual health conditions may make some suggestions inappropriate. Mind Mood Microbes outlines some of what her consultation service considers:
A comprehensive medical assessment should consider:
- Terrain-related data
- Signs of low stomach acid, pancreatic function, bile production, etc.
- Detailed health history
- Specific symptom characteristics (e.g., type and location of bloating)
- Potential underlying conditions (e.g., H-pylori, carbohydrate digestion issues)
- Individual susceptibility to specific probiotics
- Nature of symptoms (e.g., headache type – pressure, cluster, or migraine)
- Possible histamine issues
- Colon acidity levels
- SCFA production and acidification needs
A knowledgeable medical professional can help tailor recommendations to your specific health needs and conditions.









Recent Comments