This post is intended for researchers by pointing to bacteria whose genetics are likely significant for long COVID. The raw data is below. Preliminary z-scores indicated that they are significant (Pr < 0.01) and no filtering has occurred for False Detection Rate. Users are advised to perform their own statistics.
Note: These results are lab-specific, using the data provided by BiomeSight.
The reference site for the study is: http://longcovid.microbiomeprescription.com/, the raw data is available at: http://citizenscience.microbiomeprescription.com/
| Symptom Obs | No Symptom Obs | Lab | SymptomName |
| 152 | 998 | biomesight | Official Diagnosis: COVID19 (Long Hauler |
| Bacteria | tax_rank | No Symptom Count | Symptom Count | No Symptom Frequency % | Symptom Frequency % |
| Lactococcus | genus | 620 | 136 | 62.1 | 89.5 |
| Negativicoccus | genus | 461 | 86 | 46.2 | 56.6 |
| Pedobacter kwangyangensis | species | 354 | 76 | 35.5 | 50 |
| Hydrogenophilaceae | family | 480 | 90 | 48.1 | 59.2 |
| Nostoc | genus | 344 | 68 | 34.5 | 44.7 |
| Veillonella montpellierensis | species | 517 | 94 | 51.8 | 61.8 |
| Rhodothermales | order | 24 | 36 | 2.4 | 23.7 |
| Gillisia limnaea | species | 586 | 114 | 58.7 | 75 |
| Tetragenococcus | genus | 601 | 107 | 60.2 | 70.4 |
| Gillisia | genus | 592 | 114 | 59.3 | 75 |
| Paenibacillaceae | family | 771 | 133 | 77.3 | 87.5 |
| Tetragenococcus halophilus | species | 101 | 55 | 10.1 | 36.2 |
| Rhodothermia | class | 24 | 36 | 2.4 | 23.7 |
| Hydrogenophilalia | class | 479 | 90 | 48 | 59.2 |
| Bifidobacterium breve | species | 431 | 82 | 43.2 | 53.9 |
| Thermosediminibacterales | order | 72 | 55 | 7.2 | 36.2 |
| Bifidobacterium choerinum | species | 654 | 117 | 65.5 | 77 |
| Bifidobacterium longum | species | 715 | 129 | 71.6 | 84.9 |
| Hydrogenophilales | order | 480 | 90 | 48.1 | 59.2 |
| Hydrogenophilus | genus | 430 | 81 | 43.1 | 53.3 |
| Rhodothermaeota | phylum | 24 | 36 | 2.4 | 23.7 |
| Bacteria | tax_rank | No Symptom Mean | Symptom Mean | No Symptom StdDev | Symptom Std Dev | Symptom Obs | No Symptom Obs |
| Porphyromonas bennonis | species | 317 | 713 | 1435.9 | 2361.1 | 43 | 288 |
| Clostridia | class | 618307 | 487672 | 199278.7 | 150542.1 | 152 | 995 |
| Insolitispirillum peregrinum | species | 8259 | 12198 | 15534.5 | 21217.5 | 96 | 593 |
| Sphingobacterium | genus | 1125 | 1590 | 1432.3 | 1764.9 | 150 | 938 |
| Sphingobacteriia | class | 29634 | 42219 | 29577.8 | 39150.6 | 152 | 995 |
| Lelliottia amnigena | species | 922 | 205 | 2676.6 | 592.2 | 38 | 301 |
| Roseburia faecis | species | 13441 | 7122 | 19243.9 | 8796.5 | 152 | 978 |
| Leptolyngbyaceae | family | 67 | 266 | 152.6 | 1051.5 | 35 | 232 |
| cellular organisms | norank | 994054 | 988395 | 9012.5 | 5355.3 | 152 | 996 |
| Opitutae | class | 142 | 315 | 447.2 | 759.3 | 79 | 604 |
| Caloramator mitchellensis | species | 8162 | 13580 | 19886.9 | 27582.2 | 145 | 925 |
| Leptolyngbya | genus | 67 | 266 | 152.2 | 1051.5 | 35 | 230 |
| Sphingobacteriaceae | family | 25959 | 37362 | 26540.8 | 35832.1 | 152 | 994 |
| Cytophagia | class | 948 | 2232 | 2899 | 11229.4 | 150 | 960 |
| Aphanizomenonaceae | family | 222 | 124 | 374.4 | 152.8 | 108 | 653 |
| Betaproteobacteria | class | 28271 | 21480 | 26518.8 | 17465.6 | 151 | 993 |
| Pseudanabaenales | order | 110 | 230 | 274 | 973.3 | 41 | 297 |
| Pseudanabaenaceae | family | 68 | 230 | 141.9 | 973.4 | 41 | 297 |
| Spirosomaceae | family | 730 | 2282 | 3089.7 | 12178.6 | 127 | 791 |
| Tenericutes | phylum | 2507 | 6395 | 5922.1 | 16841.5 | 147 | 957 |
| Puniceicoccaceae | family | 139 | 301 | 443 | 741.7 | 79 | 599 |
| Sutterella wadsworthensis | species | 6418 | 10491 | 10990.4 | 13485.8 | 108 | 636 |
| Eubacteriales | order | 614586 | 482370 | 199230.3 | 150329.8 | 152 | 995 |
| Dolichospermum | genus | 217 | 125 | 371.1 | 153.2 | 107 | 646 |
| Dialister invisus | species | 4796 | 8035 | 9328.1 | 10909.7 | 105 | 622 |
| Mollicutes | class | 2507 | 6395 | 5922.1 | 16841.5 | 147 | 957 |
| Coprococcus catus | species | 1256 | 868 | 1371 | 850 | 136 | 804 |
| Treponemataceae | family | 1604 | 5448 | 13832.3 | 32843.8 | 37 | 235 |
| Dorea formicigenerans | species | 1434 | 914 | 1591 | 1112.9 | 142 | 902 |
| Bacteroides eggerthii | species | 8545 | 15385 | 21533.5 | 30777.7 | 57 | 394 |
| Cytophagales | order | 948 | 2232 | 2899 | 11229.4 | 150 | 960 |
| Spirochaetales | order | 1551 | 5448 | 13579.1 | 32843.8 | 37 | 244 |
| Terrabacteria group | clade | 721047 | 521084 | 231350.3 | 165314.8 | 152 | 996 |
| Cytophagaceae | family | 785 | 2189 | 2917.9 | 11452.3 | 144 | 907 |
| Caloramator | genus | 8859 | 14126 | 20084.9 | 27641.6 | 151 | 972 |
| Spirochaetes | phylum | 903 | 3743 | 10120 | 27201.3 | 54 | 441 |
| Emticicia | genus | 784 | 2553 | 3286.6 | 12937.6 | 112 | 693 |
| Leptolyngbya laminosa | species | 66 | 266 | 152.8 | 1051.5 | 35 | 228 |
| Burkholderiales | order | 27963 | 21305 | 26363.5 | 17380.9 | 151 | 993 |
| Pedobacter | genus | 8642 | 13041 | 10106 | 17703.6 | 151 | 980 |
| Burkholderiaceae | family | 361 | 197 | 598.7 | 409.8 | 135 | 886 |
| Eubacteriales incertae sedis | norank | 375 | 161 | 837.1 | 256.6 | 139 | 895 |
| Butyrivibrio proteoclasticus | species | 496 | 203 | 1108.1 | 350.5 | 89 | 657 |
| Dolichospermum curvum | species | 201 | 97 | 393.5 | 137.7 | 87 | 505 |
| Desulfovibrio fairfieldensis | species | 720 | 263 | 1789.3 | 508 | 43 | 284 |
| Bacteroidaceae | family | 300654 | 238983 | 181167 | 141573.4 | 152 | 995 |
| Bacteroidia | class | 426327 | 369089 | 188681.8 | 168273.3 | 152 | 995 |
| Acidaminococcus | genus | 984 | 2304 | 4664.6 | 9773.8 | 105 | 707 |
| Bacteroidales | order | 426327 | 369089 | 188681.8 | 168273.3 | 152 | 995 |
| Spirochaetaceae | family | 1598 | 5448 | 13805.7 | 32843.8 | 37 | 236 |
| Porphyromonas asaccharolytica | species | 314 | 1553 | 970.4 | 8744.8 | 43 | 238 |
| Erysipelotrichaceae | family | 6385 | 3475 | 10831.8 | 4414.9 | 152 | 993 |
| Roseburia | genus | 30033 | 19201 | 34050.4 | 17905.1 | 152 | 991 |
| FCB group | clade | 448905 | 391426 | 199421.4 | 186334 | 152 | 996 |
| Dialister | genus | 4668 | 7912 | 9234.3 | 10868.1 | 107 | 646 |
| Lachnospiraceae | family | 219269 | 176420 | 109155.3 | 81234.8 | 152 | 995 |
| Cerasicoccus | genus | 249 | 650 | 650.7 | 1037.4 | 34 | 250 |
| Sphingobacteriales | order | 29634 | 42219 | 29577.8 | 39150.6 | 152 | 995 |
| Eubacteriaceae | family | 3543 | 1555 | 7588.1 | 4328.8 | 152 | 989 |
| Synechococcaceae | family | 68 | 230 | 141.6 | 973.4 | 41 | 299 |
| Acidaminococcus intestini | species | 300 | 799 | 1051.3 | 2292.1 | 37 | 222 |
| Acholeplasma hippikon | species | 426 | 812 | 1052.5 | 2058.9 | 35 | 260 |
| Treponema | genus | 1604 | 5448 | 13832.3 | 32843.8 | 37 | 235 |
| Firmicutes | phylum | 657764 | 502820 | 205065.5 | 155846.7 | 152 | 997 |
| Caloramator indicus | species | 373 | 1065 | 2091.5 | 3540.5 | 44 | 373 |
| Faecalibacterium prausnitzii | species | 100109 | 141766 | 77192.1 | 87778 | 152 | 986 |
| Spirochaetia | class | 903 | 3743 | 10119.8 | 27201.3 | 54 | 441 |
| Prevotella stercorea | species | 5077 | 10010 | 18648.5 | 25185.5 | 54 | 406 |
| Insolitispirillum | genus | 8259 | 12198 | 15534.5 | 21217.5 | 96 | 593 |
| Emticicia oligotrophica | species | 785 | 2553 | 3291.1 | 12937.7 | 112 | 691 |
| Lelliottia | genus | 922 | 205 | 2676.6 | 592.2 | 38 | 301 |
| Sphingobacterium bambusae | species | 316 | 506 | 452.1 | 1018.8 | 140 | 825 |
%7D%7BN%7D%7D%7D&bg=ffffff&fg=000000&s=0)

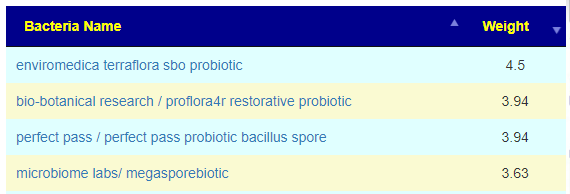

 Have you seen it anywhere? Also how would one figure out the dose for gut bacteria shifting?
Have you seen it anywhere? Also how would one figure out the dose for gut bacteria shifting? …I also have prescript on hand BUT that has a lot of other SBO strains. Would you stuck to TERRAflora for now?
…I also have prescript on hand BUT that has a lot of other SBO strains. Would you stuck to TERRAflora for now? 
Recent Comments