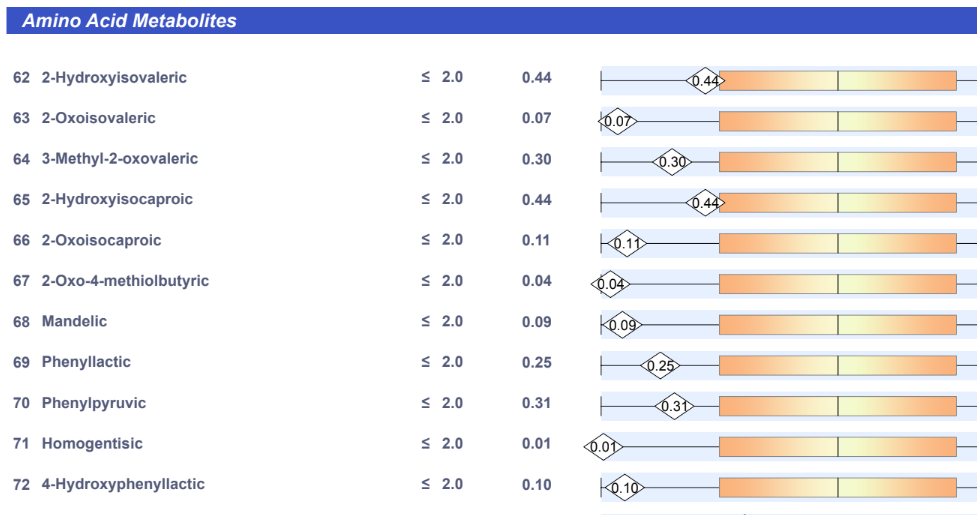
A reader forward this image from BiomeSight to me:
Apart from wording being questionable (former technical writer speaking) because many people will read it as needing to be increased whereas the chart on the right clearly shows that it needs to be decreased.
Same sample on MP reports:
D-Lactic Acid 18%ile. Thus much lower than the mid point! A Contradiction! D-Lactic acid is the bad form of lactic acid. L-Lactic acid is the very good form!
A brief discussion of how metabolites are estimated. There are several approaches used by retail providers:
Based on clinical studies reporting that a certain bacteria produces this compound.
Then just total up the count of all such bacteria
Based on clinical studies reporting that a certain bacteria produces this compound AND the amount that each produces.
Then just total up the count times the amount of all such bacteria
Then just total up the count times the amount of all such bacteria
This is the method that Microbiome Prescription [MP] uses.
There are additional methods but most are significantly more expensive. Working from clinical studies always have the issue of some bacteria not being studies – hence estimates may be off.
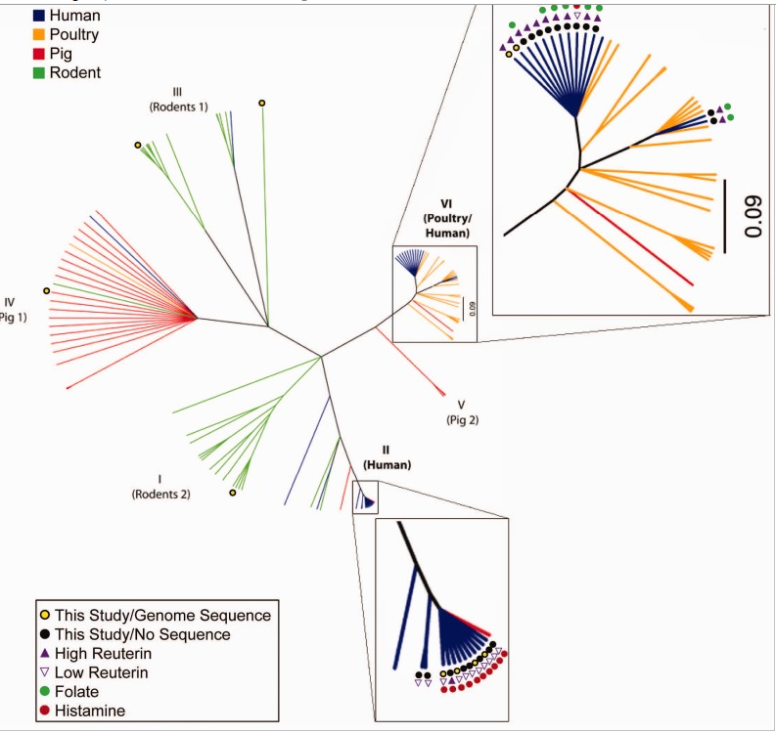
Example of one metabolite (Reuterin) showing different amounts per bacteria according to strains
There is no “right” answer. You should ask the provider of the estimates exactly how are metabolites computed (and data sources). In the case of MP, the source and method are clearly identified above. Additionally, the site should provide some education on the significance of each. Often metabolites are requested by customers and the provider does an “economical” analysis and implementation to satisfy the customer request; the results may be less than ideal or complete.
Often education is needed. The reader that emailed me, asked “should I not stop all lactate/lactic acid producing probiotics“. NO…. because L-Lactic acid is good and inhibits bad bacteria. So I checked L-Lactate (commonly just called Lactate) – see below.
Description on MP of this Metabolite
D-Lactic Acidosis: Elevated levels of D-lactic acid in the blood can lead to a condition known as D-lactic acidosis. This occurs when the body’s ability to metabolize D-lactic acid is impaired or overwhelmed. It’s often associated with specific conditions such as short bowel syndrome (SBS) or other gastrointestinal disorders where there’s an increase in the production and absorption of D-lactic acid.
Neurological Symptoms: D-lactic acidosis can lead to neurological symptoms, including confusion, impaired cognitive function, difficulty concentrating, and altered mental status. Severe cases may even lead to coma.
Gastrointestinal Symptoms: Symptoms such as abdominal pain, diarrhea, and bloating can occur in individuals with D-lactic acidosis. These gastrointestinal symptoms are often related to the underlying conditions causing D-lactic acid accumulation.
Metabolic Acidosis: Elevated D-lactic acid levels can contribute to metabolic acidosis, an imbalance in the body’s acid-base equilibrium, leading to a decrease in blood pH. This can have systemic effects and affect various organs and bodily functions.
Impaired Energy Production: D-lactic acid can interfere with cellular metabolism and energy production, potentially contributing to fatigue and weakness.
Looking up Lactate Value
Clicking on this tab button shows the thousands of metabolites that can be estimated on MP from KEGG data which we can search over.
and we find Lactate (C3H6O3) listed at 27%. IMHO that is low and you want to increase it. The description provided on this is below.
Energy Production: Lactate is produced as a result of the breakdown of glucose during anaerobic metabolism when the body’s demand for energy exceeds its oxygen supply. It serves as an alternative fuel source, particularly for muscles and red blood cells, and can be converted back into glucose (gluconeogenesis) in the liver.
Exercise and Muscle Function: During intense physical activity, the body produces lactate as muscles work vigorously, leading to temporary increases in blood lactate levels. Contrary to earlier beliefs associating lactate with muscle fatigue and soreness, lactate is not the primary cause of muscle fatigue but is rather utilized as a fuel by muscles and other tissues.
Lactate Threshold: The lactate threshold is the exercise intensity at which lactate begins to accumulate in the blood more rapidly than it can be cleared. Athletes often train to improve their lactate threshold, as it correlates with performance and endurance in certain sports.
Clinical Implications: Elevated lactate levels in the blood (lactic acidosis) can occur due to various conditions, such as sepsis, shock, hypoxia, liver disease, certain medications, or metabolic disorders. Severe lactic acidosis can lead to symptoms such as rapid breathing, nausea, abdominal pain, and, in severe cases, it can be life-threatening if left untreated.
Health Conditions: While lactate plays essential roles in energy metabolism, excessive accumulation due to underlying health conditions or imbalances can lead to health issues. Conditions associated with lactic acidosis require proper medical evaluation and treatment.
Diagnostic Tool: Blood lactate levels are sometimes measured in clinical settings to assess tissue oxygenation, especially in emergency and critical care situations, as elevated lactate levels can indicate tissue hypoperfusion and metabolic stress.
This is a follow up to this analysis ME/CFS after trying suggestions from Dr.A.I. from 2 years ago. The goal of MicrobiomePrescription is not to cure any condition — rather to generate suggestions that have a high probability of mitigate a person’s symptoms. Mitigate means reduce severity or eliminate. With some condition, it could result in a technical remission (i.e. no longer matches a diagnostic criteria). The term remission and not cure should be used always — because the microbiome could return to a dark place due to future events or inadequate ongoing care.
Update Story
I’ve been doing MUCH better for the last two years. I feel nowhere near the “normal” levels of energy that a 36 years old man should have and a lot of things are difficult, but I’ve been better and I’m able to work full time as a web developer, remotely. I know live with my significant other, and working + living with someone takes absolutely all of my energy, so I usually have no resources left to meet friends or do extra activities, but the fact of being able to work full time is a huge improvement compared to two years ago. Most of the brain fog has lifted. It comes back on my bad days, but it’s really not as bad as it used to be.
I feel that my energy levels are going worse these days and it’s getting harder to work full time though. That’s why I’ve done another microbiome analysis, and it seems to be even “worse” than 2 years ago, according to Biomesight’s score.
I still have trouble digesting things (even though it’s been a bit better the last two years, it has never been “normal” I think) and get diarrhea quite often. I usually have to go to the toilets 5-6 times a day. I’m still very skinny.
I take much less dietary supplements than I used to, but I’m still taking :
Acetyl L-Carnitine
Ubiquinole
R Lipoic Acid
B12
Vitamin D
Nattokinase
I’ve also done another round of “Spezzata”[Licorice] recently, but it definitely makes my blood pressure go up. I also eat a lot of dark chocolate and drink a lot of coffee.
My diet has changed a bit since I’ve started living with my Significant Other about a year ago. I eat a lot more rice than I used to now.
Analysis
The first thing that I noticed was the lab quality is down a lot. Lower quality means less bacteria types (793 dropped to 334) are identify and the estimated costs have greater uncertainty. On the plus side, all measures are the same or are significantly better.
Criteria
Current Sample 2024
Old Sample 2022
Lab Read Quality
2
5.4
Lab Quality Adjustment Percentage
85.9
100
Outside Range from GanzImmun Diagostics
19
19
Outside Range from Lab Teletest
25
25
Outside Range from Medivere
15
15
Outside Range from Metagenomics
9
9
Outside Range from Microba Co-Biome
6
6
Outside Range from MyBioma
8
8
Outside Range from Nirvana/CosmosId
21
21
Outside Range from Thorne (20/80%ile)
327
327
Outside Range from XenoGene
41
41
Outside Lab Range (+/- 1.96SD)
7
10
Outside Box-Plot-Whiskers
43
118
Outside Kaltoft-Møldrup
24
68
Bacteria Reported By Lab
334
793
Bacteria Over 90%ile
0
99
Bacteria Under 10%ile
0
31
Lab: BiomeSight
Pathogens
16
41
Condition Est. Over 90%ile
0
3
Standard Items
Looking at new features added. Note that the drop in number of bacteria reported impacts many of these values)
Measure
2024
2022
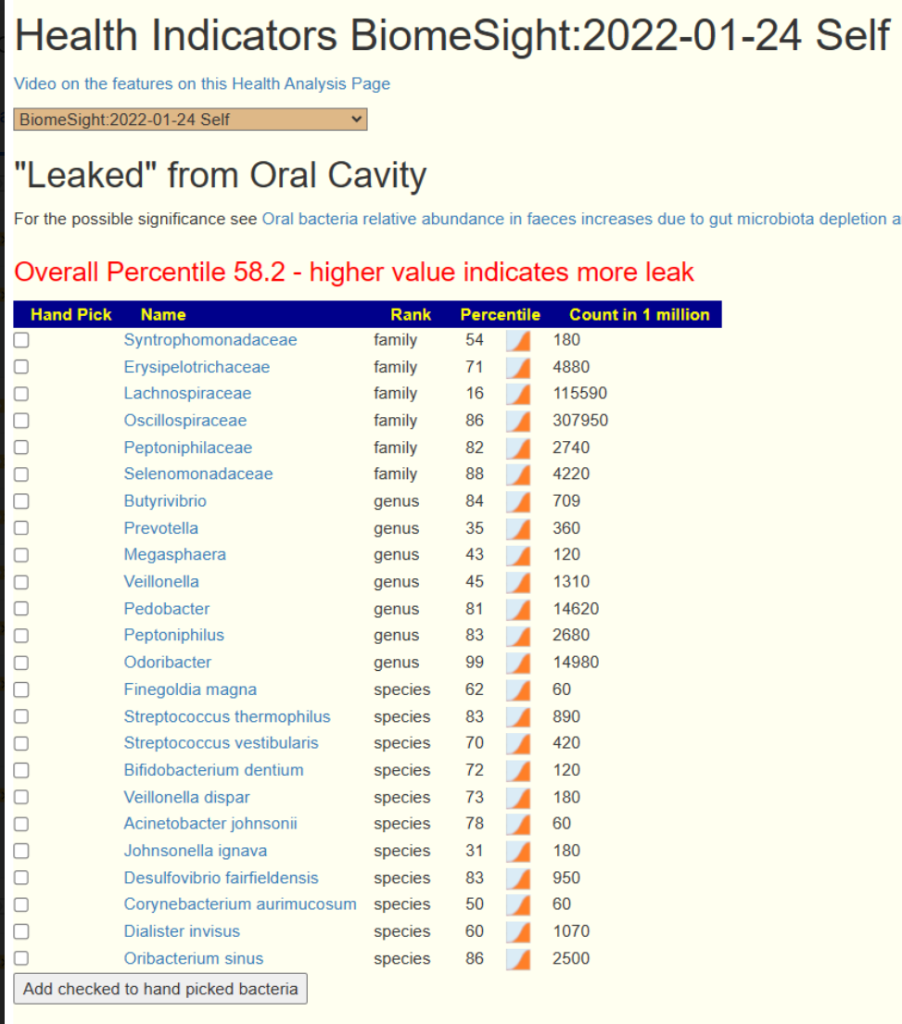
“Leaked” from Oral Cavity [LOW is better]
21.1%ile
65.7%ile
General Health Predictors [More is better]
6
17
Jason Hawrelak Ratio
10%ile
14%ile
Butyrate
9%ile
29%ile
Potential Medical Conditions Detected
0
3
Bacteria deemed Unhealthy
0
31
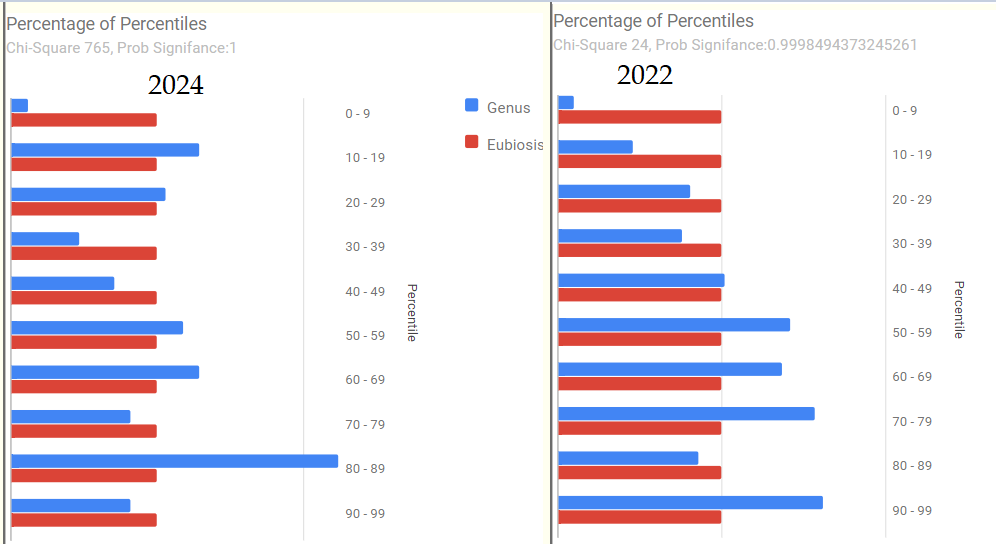
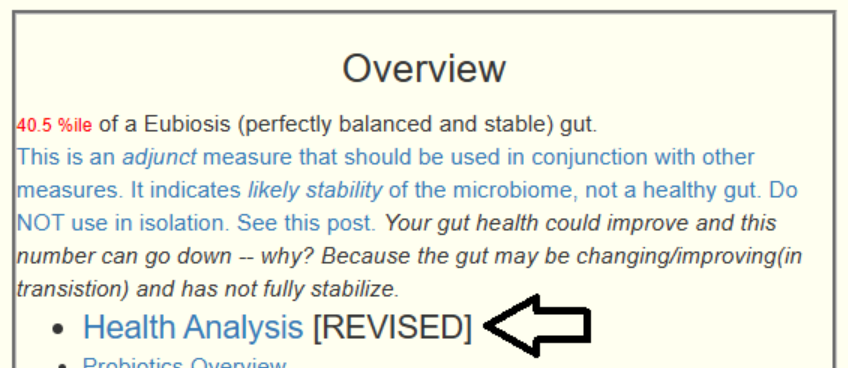
Eubiosis
8%
71.6%ile
The charts show similar patterns but with a group of bacteria dominating (80-90%ile) range
Conclusion: He is better than 2022 in many measures but is worse in a few (especially newer ones).
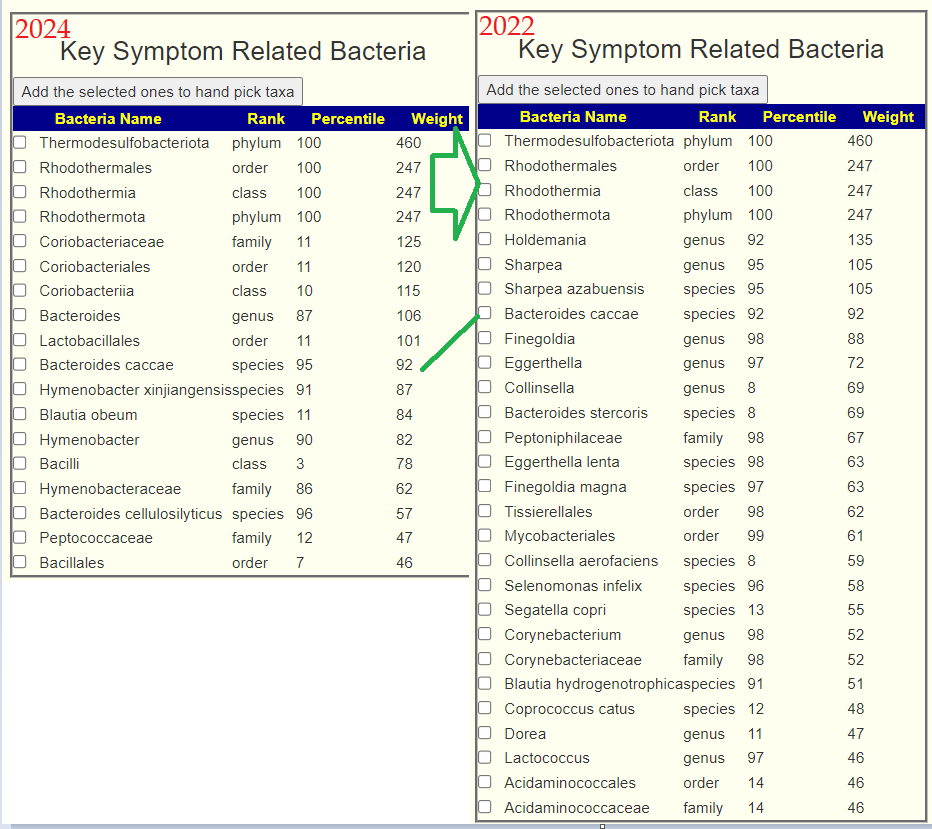
Let us look at some recent feature additions. First key bacteria — we see improvement we a lot of key bacteria dropping down below the threshold. (see Technical Note: Identifying Key Bacteria to Address for background)
As usual, I start with “Just give me Suggestions include Symptoms” with the new refactored algorithm (see Algorithm for “Just Give Me Suggestions”). The items were similar but with just a change of order.
First, let us look at what is currently being take. Microbiome changes over time. The highest for non-prescription items is 327 and lowest -516.
Acetyl L-Carnitine: 152
Ubiquinole: AKA COq 10, Not on current suggestions
None of the above is clearly a bad choice. The worst, vitamin D tend to be a slow acting supplement. This illustrates that doing a retest every 6 months to reset your course to recovery is likely good practice.
Some observations on suggestions:
60% of the top 5 items (all antibiotics) have [CFS], i.e. commonly used by ME/CFS specialists.
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
Hi Ken – I’m attempting to use MBP. I recall you linked (a long time ago) to a section that showed a list of probiotics useful in colitis, with each probiotic having the studies. How would I arrive to that page?
Where do I get the probiotics?
I prefer single species — and where I get mine?
Single species with (almost) no fillers. There are precisely three sources that I use:
Maple Life Science™: No strains yet, but shipments usually have manufactured date within 4 weeks of arrival (i.e. FRESH). Contains FOS
Bulk Probiotics: US based Newbie — but has some species not available at the other two sites. No other ingredients just the bacteria. Specifically, Lactobacillus Jensenii that has great potential for Crohn’s disease.
NOTE: none of these sell though retail outlets. This keeps their costs down and their product fresh.
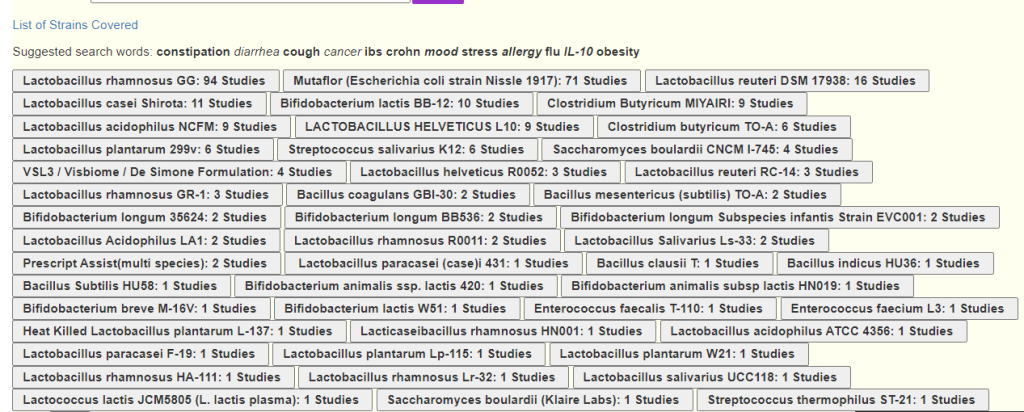
There is a multiple step/layer approach that I would use. The sequence is below:
You will see the list of probiotics with the ones with the most studies listed first.
Below it are the links to the studies. You should read at least some of them – some may report “no effect”. The list is generated by a data gathering algorithm on the species and the condition and the condition may be mentioned in passing and not directly referenced or tested.
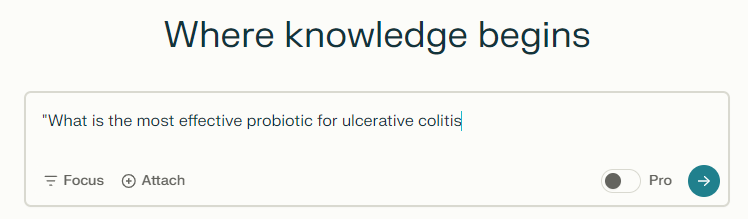
#2 Use Perplexity AI
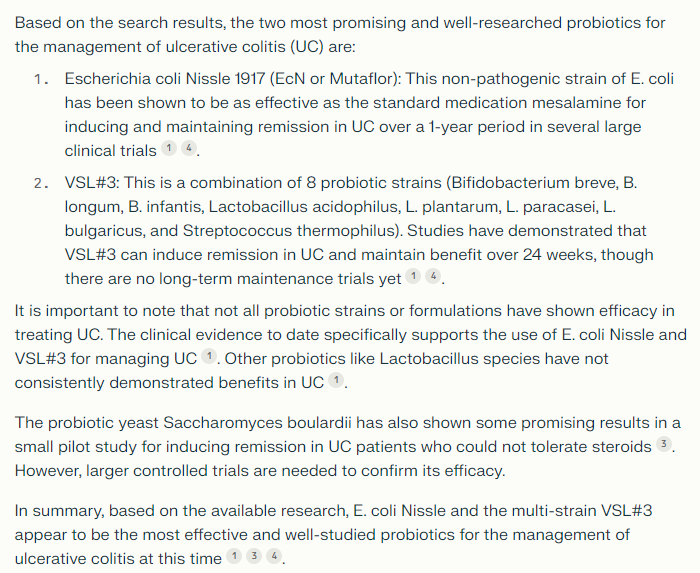
Go to https://www.perplexity.ai and just ask “What is the most effective probiotic for…”. I use this AI because it provided links to data sources so I can verify the response
A typical response is below
#3 Probiotic Via Published Microbiome Shifts
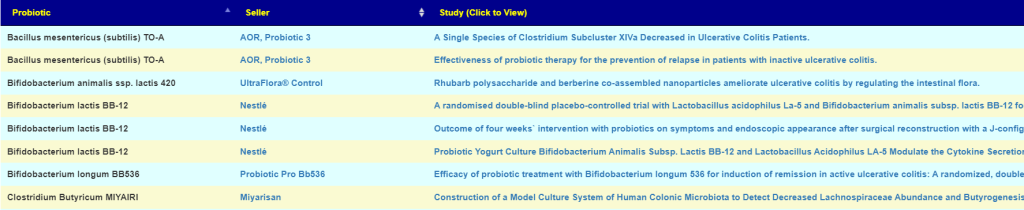
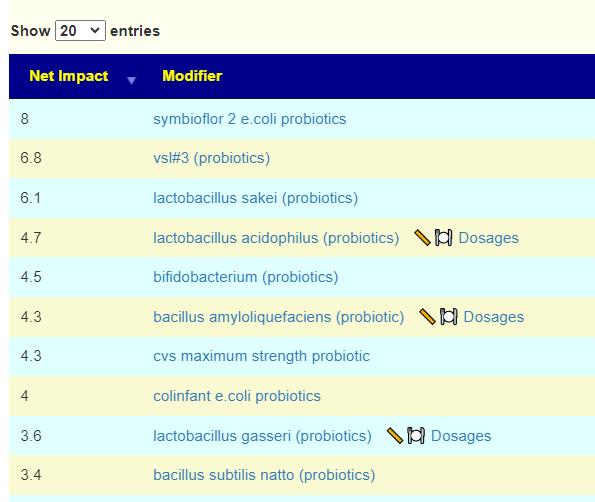
In this case we are using the MP engine to generate suggestions. It is inferior in reliability to the above methods but is a reasonable fall back. Go to Medical Conditions with Microbiome Shifts from US National Library of Medicine ( https://microbiomeprescription.com/Library/PubMed ) and search for the condition
You can click the PDF download (which report TOP items only) or click Candidates (all items)
Surprise, surprise! #1 and #2 agree with Perplexity!!! vsl#3 is not listed because we do not have strain information for this mixture of probiotics. Remember – these are computed SOLELY from the microbiome shifts without reference to any studies on ulcerative colitis!
#4 Probiotic via Citizen Science
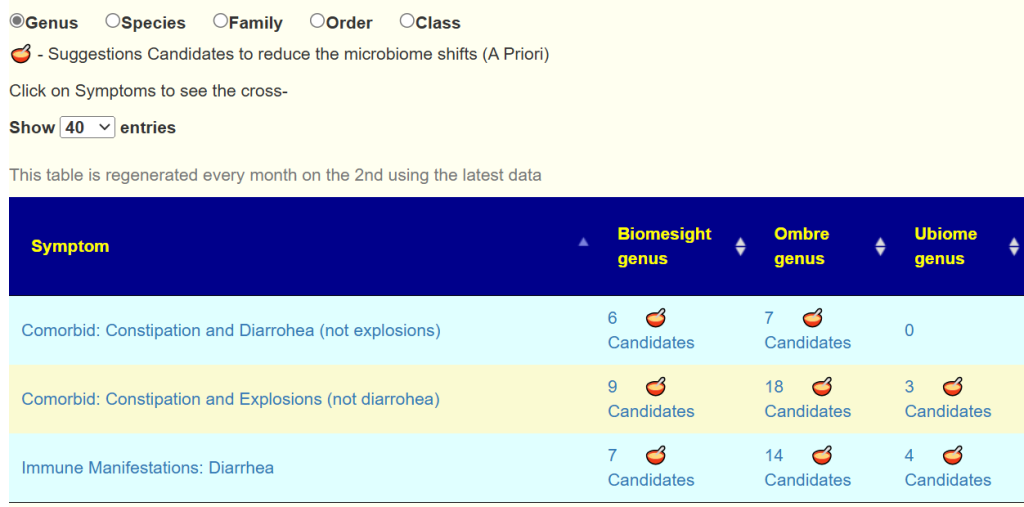
Goto Symptoms associated with conditions reported for Samples https://microbiomeprescription.com/Library/Symptoms Enter the name — in this case it was not found (not enough samples that people have annotated with ulcerative colitis). In that case, you may want to go over to symptoms you have; for example Diarrhea. This data is conditioned on the lab that the contributor was using and layered by taxa level.
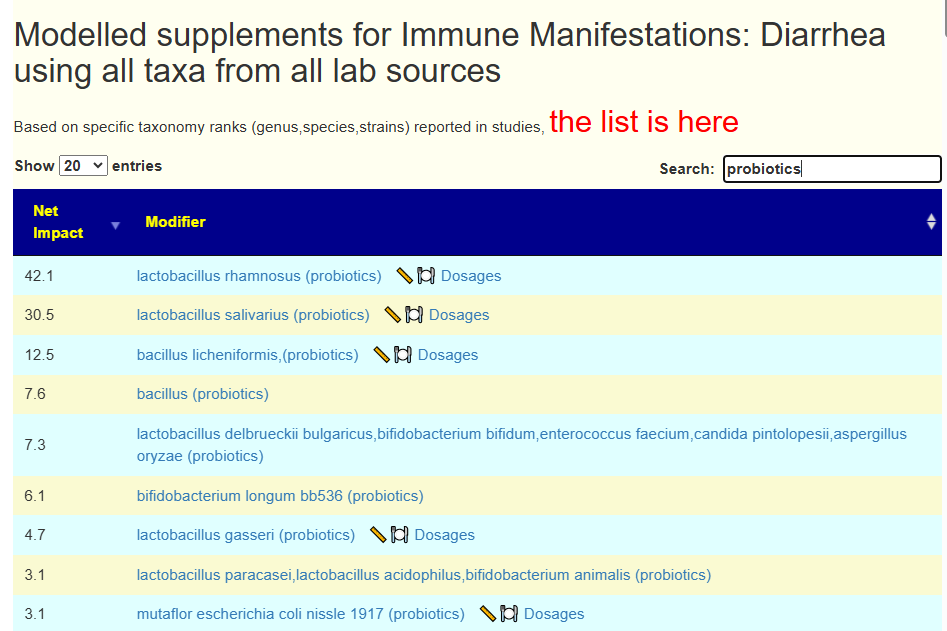
I will be adding a suggestions icon to this page shortly, and you can then review those suggestions. Clicking on the bowl, produces suggestions that can be filtered to probiotics.
#1 and #2 above are #1 and #3 with the most studied one show in above!
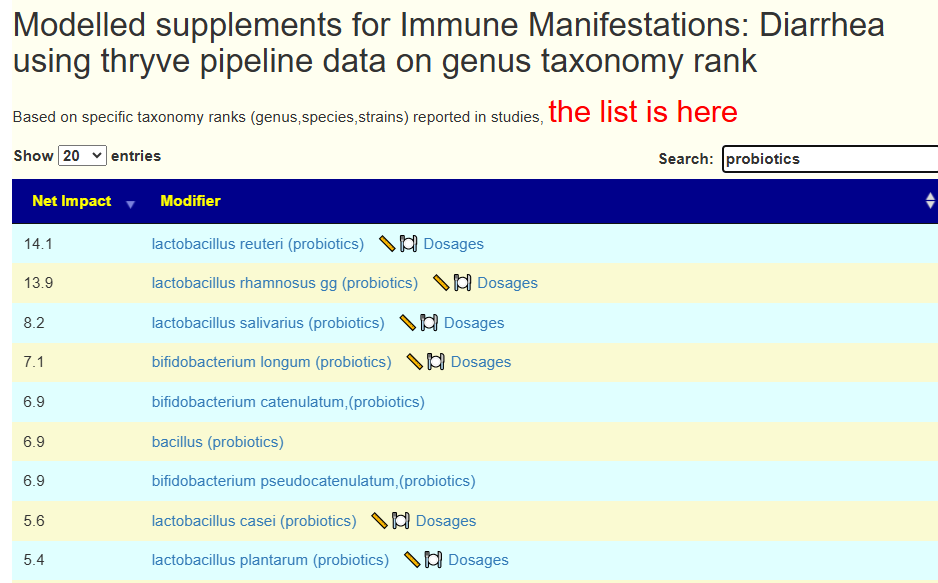
Clicking on the symptom name takes you to the symptom page listing all of the bacteria
This will then use the expert system to generate suggestions which can be filtered to probiotics
This is ranked not by the number of studies published but by the ones with the greatest estimated impact by the expert system. We see Mutaflor, L. rhamnosus – and many familiar ones in the researched strain list.
Bottom Line
We have 4 ways of selecting probiotics. For the specific question asked, all 4 converge to the same items. In terms of clinical use, we see that the suggestions based solely on bacteria shifts going through the expert system appear to be cross-validated. IMHO, this explicit expert system works better than the typical MD would.
I’ve found your work through PR forum and then your website, it’s really interesting reading all that information and feeling so related to the issues.
For the last year I’ve been house bounded and sometimes bed bounded, all coming from ignoring one year of daily sandy-yellowish diarrhea along with a series of chronic sinus infections that one after another left me in a worst health state to finally being isolated fearing further infections.
I’ve been reading and investigating, trying methylation protocols and probiotics. The probiotic I took was fairly simple (bifidobacterium bifidum and lactobacillus acidophilus) but gave me pretty bad reaction which got me thinking about histamine release, one Google search showed me that those strains are not histamine releases but what it does (acidophilus) is increase D-lactic production and what other bacteria could do this? Streptococous, the one which probably caused my chronic sinusitis.
This is how I ended up thinking that I really need to know if I have those kind of bacterial overgrowth in my guts and reading your work thougth that you could have some advice to start learning how to do it.
I looked at “Leaked” from Oral Cavity and while the count places him at 49%ile, the number of bacteria was much longer than usual — a lot of different bacteria at low levels which suggests a new statistics to add in the next revision.
Going Forward
Since symptoms are entered, I am just using the Just Give Me Suggestions with Symptoms button.
The suggestions are below, trimmed a little
sucralose
lauric acid(fatty acid in coconut oil,in palm kernel oil,)
enterococcus faecium (probiotic)
garlic (allium sativum)
momordia charantia(bitter melon, karela, balsam pear, or bitter gourd)
Tudca – Tauroursodeoxycholic acid , a supplement
lactobacillus casei (probiotics)
whole-grain barley
fruit/legume fibre
bifidobacterium infantis,(probiotics)
dates
grape polyphenols
naringenin(grapefruit) (Flavonoid)
Cacao
rosa rugosa (Rosavin – an adaptogen)
Hesperidin (polyphenol)
Nicotine, Nicotine Patch
galla chinensis (herb)
Grapefruit seed extract
lactobacillus gasseri (probiotics)
thyme (thymol, thyme oil)
foeniculum vulgare,fennel
Turmeric
N-Acetyl Cysteine (NAC),
Onion
I will create two extracts: one for probiotics and one for teas (i.e. herbs).
Looking at probiotics, we have a good number that would allow easy rotation of probiotics. Two are usually difficult to obtain are removed: lactobacillus kefiri and lactobacillus sakei . Most are available at my usual two preferred sources: Custom Probiotics and Indian Bulk Exporter (Maple Life Sources). See this list for sources not available there. By rotation, I mean 20-50 BCFU daily of one probiotic for 2 weeks and then change to another probiotic.
enterococcus faecium
lactobacillus casei [CB,MLS]
bifidobacterium infantis, [CB,MLS]
lactobacillus gasseri [CB,MLS]
lactobacillus jensenii [MS]
lactobacillus salivarius [CB,MLS]
pediococcus acidilactic
bifidobacterium breve [CB,MLS]
bifidobacterium pseudocatenulatum,
bifidobacterium longum [CB,MLS]
bacillus coagulans
While taking herbs as capsules or oils is very viable, herbal teas has the advantage of effecting the oral cavity (and thus sinus) and extends through the entire system.
Human milk oligosaccharides (prebiotic, Holigos, Stachyose)
red wine
pectin
l-citrulline (supplement)
berberine (supplement)
Pulses
apples, nuts, banana
galacto-oligosaccharides (prebiotic)
low-fat diets, high beef diet, high red meat, animal-based diet, hypocaloric hyperproteic diet
iron
Pork
kefir
bacillus licheniformis,(probiotics)
fasting
galactose (milk sugar)
propionate
Guaiacol (polyphenol)
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
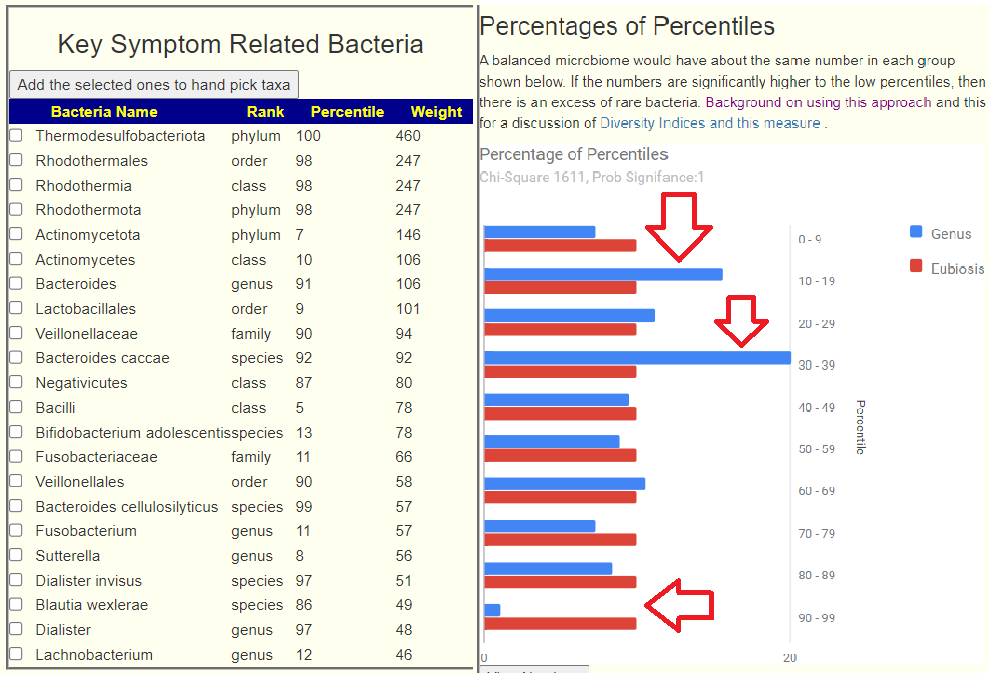
After a good night sleep after doing the video below, I realized the next step in this journey. With hundreds of bacteria in the microbiome the question arises which ones to focus on if the condition is not a known single bacteria condition. I.e. Crohn’s, Asthma vs Tuberculosis, Ulcers.
Recently I had major success is identifying bacteria associated to hundreds of symptoms. This was done by using the percentile ranking of each microbiome sample over the population and then examining the counts of the top and bottom 15%ile (simplified version). These should be equal if there is no relationship of the bacteria to the symptom. The difference allows a Chi2 value and probability to be computed for significance. Comparing the averages perform very poorly for finding equivalent statistical significance.
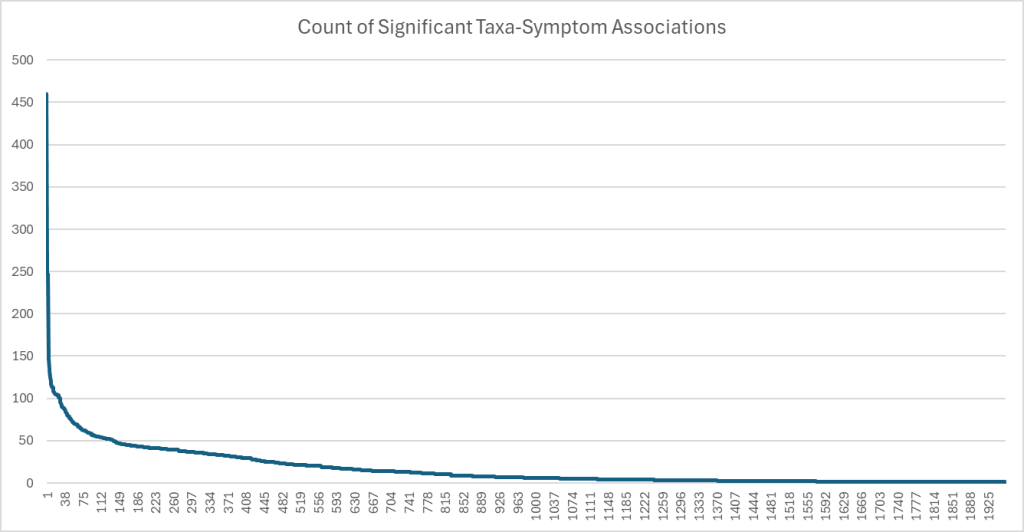
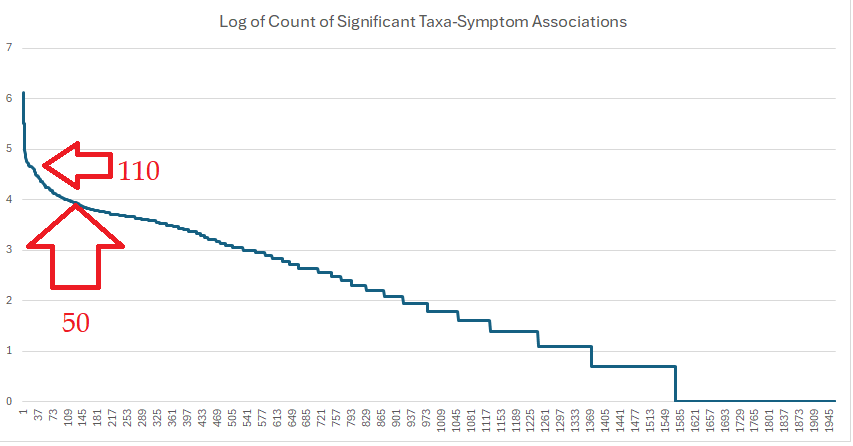
The result was a list of bacteria where the high in these end 15%ile was associated with symptoms / diagnosis. This allows us to filter out the noise from the significance in a sample. The question arises, should all of these be used or is there a critical limit? The current count is 1,960 taxa-shifts with one or more
To address this issue, I decided to plot the counts.
Applying a log function found a region became a straight line. Two apparent inflection points are suggested. Applying different function kept showing the same inflection points.
Bacteria with high and low associated to Symptoms
There are two species in this list. Both are reported in published clinical studies often.
Bacteria
Rank
Faecalibacterium prausnitzii
species
Dorea formicigenerans
species
Weissella
genus
Faecalibacterium
genus
Acidaminococcaceae
family
Acidaminococcales
order
The Short List of Bacteria
We see many bacteria not usually associated plus two familiar ones. Increases means more are in the 85-100%ile, decrease means more are in the 0-15%ile
Bacteria
Rank
Direction
Count of Associations
Thermodesulfobacteriota
phylum
increases
460
Rhodothermota
phylum
increases
247
Rhodothermia
class
increases
247
Rhodothermales
order
increases
247
Actinomycetota
phylum
decrease
146
Holdemania
genus
increases
135
Faecalibacterium
genus
decrease
133
Coriobacteriaceae
family
decrease
125
Coriobacteriales
order
decrease
120
[Clostridium] thermoalcaliphilum
species
increases
116
Coriobacteriia
class
decrease
115
Lactobacillaceae
family
decrease
114
Bifidobacterium
genus
decrease
113
Sphingobacteriaceae
family
increases
113
Longer List of Bacteria
Bacteria
Rank
Shift
Count
Oscillospiraceae
family
decrease
108
Anaerotruncus colihominis
species
increases
107
Actinomycetes
class
decrease
106
Bacteroides
genus
increases
106
Hathewaya
genus
increases
105
Sharpea azabuensis
species
increases
105
Bacillota
phylum
decrease
105
Sharpea
genus
increases
105
Anaerotruncus
genus
increases
104
Sphingobacteriia
class
increases
104
Sphingobacteriales
order
increases
104
Lactobacillales
order
decrease
101
Ruminococcaceae
family
decrease
101
Erysipelothrix muris
species
increases
100
Erysipelothrix
genus
increases
96
Veillonellaceae
family
increases
94
Bacteroides caccae
species
increases
92
Clostridia
class
decrease
90
Bacteroides fluxus
species
increases
89
Eubacteriales
order
decrease
89
Ethanoligenens
genus
increases
89
Finegoldia
genus
increases
88
Hathewaya histolytica
species
increases
87
Hymenobacter xinjiangensis
species
increases
87
Roseburia faecis
species
decrease
85
Blautia obeum
species
decrease
84
[Clostridium] leptum
species
increases
83
Hymenobacter
genus
increases
82
Negativicutes
class
increases
80
Terrabacteria group
clade
decrease
79
Bifidobacteriaceae
family
decrease
79
Bacilli
class
decrease
78
Bifidobacterium adolescentis
species
decrease
78
Marvinbryantia
genus
increases
77
Phocaeicola vulgatus
species
increases
77
FCB group
clade
increases
76
Odoribacter denticanis
species
increases
75
Mediterraneibacter
genus
increases
74
Faecalibacterium prausnitzii
species
decrease
73
Eggerthella
genus
increases
72
Bifidobacteriales
order
decrease
72
Lachnoclostridium
genus
increases
70
Acidaminococcales
order
increases
70
Odoribacter
genus
increases
70
Acidaminococcaceae
family
increases
70
Blautia schinkii
species
increases
69
Dorea formicigenerans
species
increases
69
Collinsella
genus
decrease
69
Bacteroides stercoris
species
decrease
69
Lactobacillus
genus
decrease
68
Pseudomonadota
phylum
increases
67
Odoribacteraceae
family
increases
67
Peptoniphilaceae
family
increases
67
Fusobacteriaceae
family
decrease
66
Dorea formicigenerans
species
decrease
66
Amedibacillus dolichus
species
increases
65
Amedibacillus
genus
increases
65
Candidatus Glomeribacter
genus
increases
64
Eggerthella lenta
species
increases
63
Finegoldia magna
species
increases
63
Oscillatoria corallinae
species
increases
62
Ruminiclostridium cellobioparum subsp. termitidis
subspecies
decrease
62
Oscillatoria
genus
increases
62
Tissierellales
order
increases
62
Ruminiclostridium cellobioparum
species
decrease
62
Hymenobacteraceae
family
increases
62
Pseudoflavonifractor
genus
increases
61
Mycobacteriales
order
increases
61
Tissierellia
class
increases
60
Lachnoanaerobaculum
genus
decrease
60
Coprococcus
genus
decrease
59
Blautia
genus
increases
59
Collinsella aerofaciens
species
decrease
59
Verrucomicrobiota
phylum
increases
59
Veillonellales
order
increases
58
[Ruminococcus] gnavus
species
increases
58
Selenomonas infelix
species
increases
58
Eubacterium ventriosum
species
decrease
58
Lactonifactor
genus
increases
57
Bacteroides cellulosilyticus
species
increases
57
Enterococcaceae
family
decrease
57
Fusobacterium
genus
decrease
57
Alistipes putredinis
species
increases
57
Sutterella
genus
decrease
56
Anaerotignum lactatifermentans
species
increases
56
Anaerotignum
genus
increases
56
Clostridium akagii
species
increases
56
Burkholderiaceae
family
increases
55
Akkermansiaceae
family
increases
55
Turicibacter
genus
decrease
55
Butyricimonas
genus
increases
55
Segatella copri
species
decrease
55
Mycoplasmoidales
order
increases
55
Turicibacteraceae
family
decrease
55
Turicibacter sanguinis
species
decrease
55
Akkermansia muciniphila
species
increases
54
Sporomusaceae
family
increases
54
Limnobacter
genus
increases
54
Limnobacter litoralis
species
increases
54
Lactobacillus rogosae
species
decrease
54
PVC group
clade
increases
54
Thiocapsa
genus
increases
53
Sphingobacterium bambusae
species
increases
53
Enterobacteriaceae
family
increases
53
Pseudoflavonifractor capillosus
species
increases
53
Blautia hansenii
species
increases
53
Akkermansia
genus
increases
53
Marvinbryantia formatexigens
species
increases
52
Enterococcus
genus
decrease
52
Corynebacteriaceae
family
increases
52
Lachnospira
genus
increases
52
Lachnospira eligens
species
increases
52
Corynebacterium
genus
increases
52
Mycoplasmataceae
family
increases
52
delta/epsilon subdivisions
clade
decrease
52
Bacteroides faecis
species
increases
52
Bacteroides gallinarum
species
increases
52
Veillonella
genus
increases
51
Weissella
genus
increases
51
Dialister invisus
species
increases
51
Blautia hydrogenotrophica
species
increases
51
Lactonifactor longoviformis
species
increases
50
Dorea longicatena
species
decrease
50
Best Test/Lab?
The above is based on percentile and not the typical percentage. The results from Clinical Microbiomics A/S (a.k.a. CosmosId) provides percentile ranking again a regionalized healthy population. In the US, their tests are available retail from Thorne. They will soon be available retail from Precision Biome in the EU.
People with mast cell issues typical treatment approach is:
Reduce foods high in histamine
Avoid probiotics that produces histamine
Use DAO supplements.
There is a fourth leg that should be added to this three legged stool. Probiotics (and other substances) that impacts DAO levels. Some could argue that they impact DAO because they produce histamines. That may be true in some rare cases, but many of the items listed below are not known to produce histamine.
The production and activity of DAO can be regulated by various factors, including hormones, inflammatory mediators, and the presence of substrates like histamin. Difference probiotics produces different enzymes which may inhibit or assist with the production of DAO.
The probiotics, impact and study used are listed below:
Reviewing the studies is recommended. In some cases DAO levels were raised due to infection, i.e. Escherichia coli K88; and the probiotic may be inhibiting the increase due to the infection though reducing the infection and not actually impacting DAO levels.
“nicotinamide partially inhibits the in vitro release of histamine ” [1963]
“Release of PGD2 [due to niacin] was not accompanied by a release of histamine which was assessed by quantification of plasma levels of the histamine metabolite,” [1989]
CONCLUSION: Niacin by itself does not cause histamine release (except with excessive use of one form of niacin)
“Moreover, it[Niacin] led to a significant rise in DAO levels on day 30 (p < 0.05). Niacin supplementation significantly reduced the LPS levels on day 30 (p < 0.05).” [1992]
What is needed are control studies measuring DAO levels in humans with different probiotics. The above illustrates that probiotics are likely to make good or bad differences.
1976-2012 – Sustained 7 concussions playing contact sports, minor short term symptoms and fully recovered. Fit, active, and employed as adult. Satisfying family/social life. Higher intensity physical training 5-6 days per week outside or in gym. No drugs/alcohol since 2003, no medical issues or medications.
2012 – Post Concussion Syndrome – Fell and hit head skiing, diagnosed with concussion, symptoms did not resolve. No detectable damage on MRI.
Symptoms
Fatigue, brain fog, intense and unpredictable nerve pain in head
Cognitive and visual processing issues
Sensitivity to light, loud noise, busy environments
GI – constipation
Multiple food, chemical, and environmental sensitivities
Overall functionality reduced, still able to socialize, drive, complete tasks, problem solve, etc… sporadically and in short increments. Physical fitness mostly unaffected, continued to exercise, incorporated yoga/gyrotonic.
Divorced
Received disability benefits in 2019
chronic sinus issues that started after concussion and worsened with vaccine.
diagnosed w nasal mold colonization, nasal biofilms, and chronic staph aureus.
2021 – mRNA Vaccine Injury (2 shots Pfizer)
Symptoms:
Total exercise intolerance, sympathetic activation, anxiety and confusion
Exacerbation of pre-existing symptoms – severe fatigue, brain fog, food/chemical/medication/supplement sensitivities, constipation
Neuropathy – pain, tingling, numbness in legs and feet.
Minimal activity, short walks, occasional driving short distances, most time spent resting
the plasma level of Zonulin was significantly increased after post blast exposure, indicating that blast may contribute to the impairment of the gut barrier in the paracellular pathway “
Repetitive blast exposure resulted in both similar (e.g., increased IL-6), and disparate (e.g., IL-10 increase only in females) patterns of acute serum and brain cytokine as well as gut microbiome changes in female and male mice. Chart is below
increased Clostridium innocuum and Erysipelatoclostridium
reductions in Bacteroides and Clostridium Sensu Stricto
Reductions in Bacteroides have been associated with irritable bowel syndrome (IBS) development and identified after stroke [87]. Bacteroides are imperative for the maintenance of intestinal barrier integrity, with supplementation being associated with increased tight junction proteins [88]. Reductions in Clostridium sensu stricto have been associated with reduced butyrate production and Alzheimer’s disease [89,90].
” Findings from this trial support the feasibility, acceptability, and safety of supplementation with an anti-inflammatory/immunoregulatory probiotic, Lactobacillus reuteri DSM 17938, among Veterans with PPC and PTSD symptoms.” [2020]
COVID Shots
Explicit studies are rare. What we do have is a variety of studies between high and low responder which enumerates the difference of bacteria. We do not clearly know which goes in any specific direction. We do know the bacteria that are likely to change.
Increase Akkermansia muciniphila in some cases, but in general no change
The high response group were primarily characterized by a predominance of Enterococcus faecium, Prevotella bivia, Actinomyces massiliensis, Veillonella dispar, Veillonella_sp_T11011_6, Eubacterium_sp_CAG_38, Ruminococcus torques, Actinomyces odontolyticus, while Alistipes putredinis, Allisonella histaminiformans, Bacteroides clarus, Clostridium lavalense, Clostridium asparagiforme, Bacteroides eggerthii, Coprobacter fastidiosus, Sutterella parvirubra, and Blautia coccoides are more abundant in the low response group
We have two results to work from: Biomesight report and an OATS (Organic Acid) report.
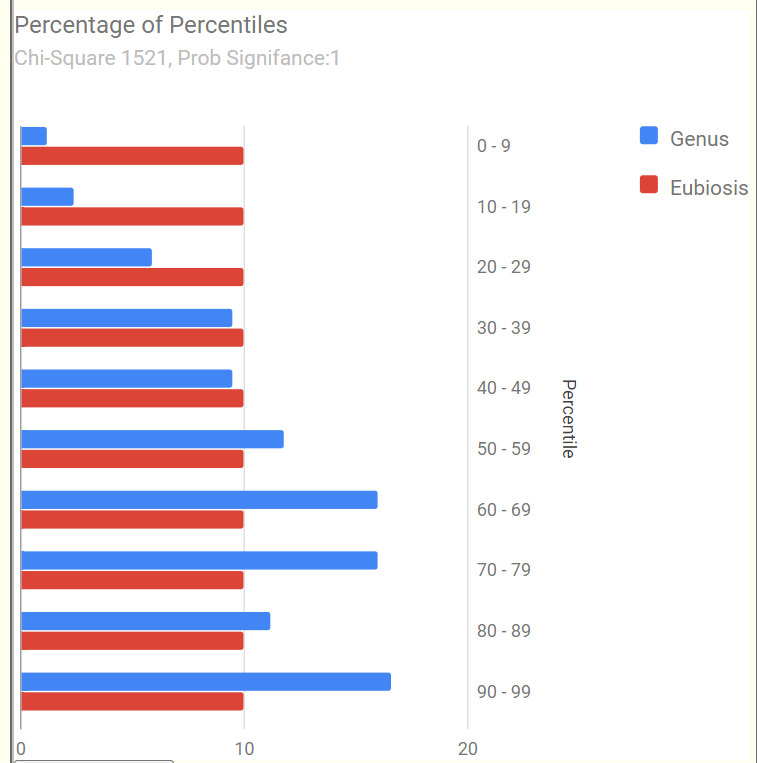
Looking at Forecasted symptoms we have a high rate of pattern matches. This is hopeful because it implies we now have strongly suspected bacteria.
We also see a significant shift of bacteria that are atypically over represented.
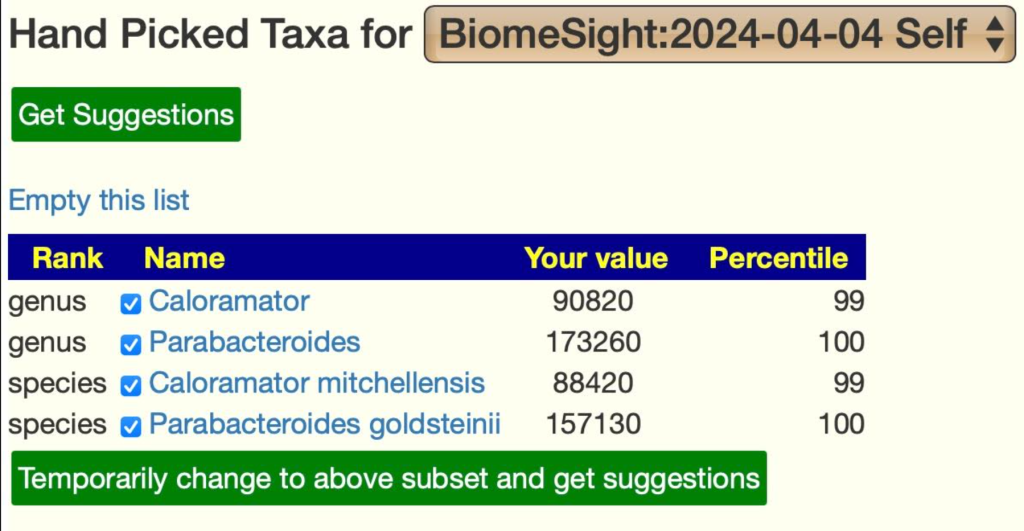
The reader noticed the dominance of some unusual bacteria (species and the genus they belong to). These amount to be 28.4% of the microbiome. These two bacteria usually average 3.5% of the microbiome.
As a starting point, we will do [Just give me Suggestions include Symptoms]. Since we have some condition specific suggestions above, let us see where they rank.
This type of cross validation is nice to see — everything known to help TBI/concussion is in the recommended to take list. It builds confidence in the suggestions being generated.
The next thing is to see which of the bacteria shifts cited in the above literature. We go over the the Bacteria tree. We filter out those not usually reported by Biomesight and ended with just one (which illustrates the benefit of shot-gun tests).
reductions in Bacteroides: was at 32%ile
Other incidental measures of note:
Anti Inflammatory Ratio: 20% (so inflammation is likely)
Other Issues
Last, do we see Staphylococcus aureus in the sample? No.
“Some (poly)phenolics such as caffeic acid [found in Barley, Coffee], hydroxytyrosol [from Olive Oil}, resveratrol, curcumin, nordihydroguaiaretic acid (NDGA) [TOXIC ISSUES], and quercetin have been reported to reduce the formation of 5-LOX eicosanoids in vitro”
I should point out that something is very funky with the OATS report. Every value below is within their declared range but their graphics show it is out of range.
The result was 326 probiotics — specifically, probiotics that are known to consume Malate. We have no significant additions.
Action Plan
First item of note, above we have 100% cross validation on what the fuzzy logic expert system says should help with clinical studies of what helps given his particulars. This hints that other suggestions are far more likely to help than hurt.
The easy set of suggestions are quercetin, clostridium butyricum (probiotics),lactobacillus acidophilus, lactobacillus reuteri (probiotics) because they are double recommended: both clinical studies and the microbiome. Since with this history, getting any prescription drugs is unlikely, the consensus suggestion leads me to consider the following (filtered for availability etc):
Probiotics (no more than 2 at a time, and rotate to different ones every 2 weeks)
IMHO, This is the general problem with diet data — they contain vast baskets of substances: some good and some bad; with a wide variety of definitions. I prefer working substance by substance.
Retest
I would suggest a retest with Biomesight in 3 months (if the reader consents, I would be glad to do a follow up post). Remember these are not generic suggestions for anyone with a concussion but based on the individual’s microbiome with cross referencing to the literature to develop a clean consensus of what may help.
Ideally, the user will do the time consuming process of checking the suggestions against the literature (which I did above for illustration).
There is NO direct linkage using studies of symptoms to supplements by the engine. That is technically possible, but would require major funding to hire qualified people to enter the data.
Experience have found that 85-95% of suggestions that has studies for a conditions are in agreement.
Q: Do you use studies on my conditions to pick bacteria?
If there are sufficient studies, then yes. In your case there is not. Clinical studies on conditions often have contradictory results for a vast number of reasons: the lab and software used; the diet of the people in the studies; often low significance (often P < 0.05 is cited, with our lab specific analysis we typically use P < 0.001 as a criteria).
Q: The high Bilophila on my Biomesight got my attention. Is that something that MP.com does not identify specifically to address but rather it just corrects as part of the overall microbiome rebalancing?
MP does a holistic analysis — so things that may reduce Bilophila but also shifts others bacteria in the wrong direction may be eliminated.
“The typical MP matrix to solve is around 60 taxa (up to 430 in some cases) by 2092 possible modifiers – thus an array of some 12,000 to 800,000 elements to consider. The Monte Carlo method typically uses 5 runs resulting in 60,000 to 4,000,000 elements evaluated.” [blog]
Q: The prebiotic that shows up as #1 rec for me is Prefor Pro, but you have chicory. Is that due to availability?
The retailed probiotic selection is based on the species in the probiotics ignoring additives and relative amounts (often not declared). If there are issues with these additives, then just move down the list.
Q: Do you think using the condition specific bacteria shifts is a better approach than the bacteria identified by the AI as “likely to be causing my symptoms”?
Definitely, my observations from feedback is that targeting those bacteria do moderate or eliminate symptoms.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
This is part of a series of technical notes. If this interests you, you may wish to view others in the series.
A colleague wrote me:
I am currently researching companies who are using machine learning and LLM approaches for Microbiome analysis I wanted to know your opinion why this approach fails/ is less precise than your [MicrobiomePrescription MP] Fuzzy LogicExpert System with Monte Carlo method.
I have been doing a wide variety of Artificial Intelligence development professionally since 1988 for firms including Microsoft, Amazon, Verizon and Starbucks. I also have a reasonable science background including High School General Science teacher and College Chemistry and Physics instructor.
In the early days of Microbiome Prescription I tried a panacea of technics such as Random Forest, linear and non linear regression, supervised learning, etc. The results were less than acceptable. A friend, Richard Sprague, also ex-Microsoft, who worked as Citizen Scientist in Residence for uBiome for a while set up a series of meeting with the teams of the Allen Institute for AI [AI2]. The consensus working with those experts was that my direction of using the expert system model was far superior than what they could come up with.
How does Machine Learning and LLM work?
The core mechanism is pattern recognition of key words and phrases. This allows a numeric representation of the literature to be created, i.e. [subject #,verb #, object #]. When someone asks about subject, a set of equivalent subject # is obtained, a set of equivalent verb # is obtained and we just lookup the data. The number of records may be used to determine priority or most probable outcome.
This leads to the problem with many implementations, phrase recognition. To illustrate consider two articles, one mentions: Limosilactobacillus reuteri and the other mentions for Lactobacillus reuteri. A microbiologist knows that these are the same, but the typical ML or LLM does not. Do we end up with two collections of information? Since both Limosilactobacillus and Lactobacillus are also taxological units, do we get this species information incorrectly applied to the genus?
This is further complicated going to studies dealing with strains. Compare these two species: Escherichia coli O157:H7 and Escherichia coli Nissle 1917. One causes food poisoning, and the other is a probiotic shown to improves Crohn’s disease. Strains often have multiple identifiers and retail names. For example, Enterococcus faecium SF68 is also known as Enterococcus faecium NCIMB 10415 and sold retail as Bioflorin for humans and multiple brands in veterinary practice.
So the number 1 issue is correct identification. We also have some name collisions: Bacteroidetes is the name of both a class [Taxon 200643] and a phylum [Taxon 976] (which is now called Bacteroidota). A knowledgeable reader can reason out what is meant.
Taxonomy Hierarchy Inference
Information on the microbiome is sparse. A microbiome practitioner asked about what would reduce Lactobacillus balticus may discover that there is no literature on it. This practitioner would then infer that whatever reduces Lactobacillus would reduce it. This is an inference which MP does (remember it is an expert system mimicking the behavior of a human expert). MP takes it one step further by recognizing that is now classified as Limosilactobacillus balticus. Instead of items impacting Lactobacillus, it will use items impacting Limosilactobacillus. The suggestions are more probable to be correct.
What to address question
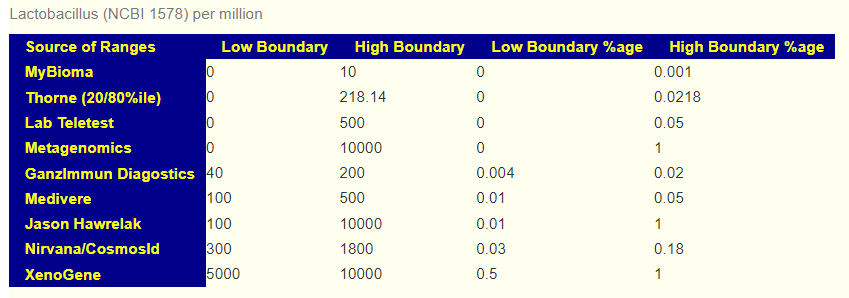
The various AI systems may well scrap ranges from studies to apply to a microbiome sample. Results are not consistent from lab to lab [the back story is this 2019 post: The taxonomy nightmare before Christmas…] . This means that reference ranges are more inconsistent as a consequence. Below are some range examples from commercial tests
The reference range dilemma is why MP generates suggestions based on reference ranges determine by multiple methods: Average +/- Std Dev, Box Plot Whiskers, ranges from specific sources (including the processing lab in some cases), and patent pending algorithms. Each reference range is determined from a large collection of sample processed by the same lab. The suggestions using each of these reference ranges are then aggregated into a “consensus” report (i.e. Monte Carlo method).
“We are using AI to get Suggestions” – marketing hype!
A few years ago, microbiome testing companies would attempt to get creditability by claiming their suggestions were created by registered dietitian. Today, “AI” is the replacement. If you ask about what AI methodology is being used, the size and scope of the data behind, etc. 99% of the time you will be given a “It’s proprietary! We cannot disclose it“.
They may be truthful that is coming from AI, for example, someone asked https://www.perplexity.ai/, “Which foods reduces Fusobacterium” (Example answer – Fusobacterium nucleatum is what is cited). They copy the answer into their database to show their customers. Thus it is true that the answer is coming from AI; but it is a one-dimensional blinkered answer that will often leaves their customer worse. This AI is ignorant that Fusobacterium prausnitzii [The bacteria formerly known as Faecalibacterium prausnitzii] belongs to it. This bacteria has lots of studies that are ignored by the AI! The AI appears ignorant that two studies report both quercetin, mastic gum (prebiotic) reduces it. It likely has the data but has misclassified it.
My observations of reviewing many sites is that suggestions are scoped to a single bacteria and ignores side-effects on other bacteria that would also be impacted. MP uses holistic algorithms [which is what would be expected when someone has done Ph.D. courses on Integer and Non-Integer Programming Optimization]. The typical MP matrix to solve is around 60 taxa (up to 430 in some cases) by 2092 possible modifiers – thus an array of some 12,000 to 800,000 elements to consider. The Monte Carlo method typically uses 5 runs resulting in 60,000 to 4,000,000 elements evaluated.
Examples of LLM gone bad
Most experts know that Mutaflor is Escherichia coli Nissle 1917 and is clearly names as such in publicly accessible papers on the National Library of Medicine. So this response is one of AI’s famous hallucinations; hallucinations are not possible from expert systems.
Bottom Line
Microbiome testing firms may correctly claim[in a legal sense] they are AI based. If they refuse to fully disclose the methodology being used (ideally on their site), then the safest assumption is that they got a summer intern to ask one of the LLM’s the questions and just copied the answers into the database. Without full disclosure, they simply cannot be trusted.
If you are considering using AI because some “hot shot evangelist or venture capitalist” is pushing for it; then — look at the above issues and insists on documentation on how each of these issues will be addressed. Until there is clear, understandable documentation on these issues, “The suitability of AI has not been shown for the proposed AI implementation” and stop wasting time and money!
MP uses a very old model of AI that requires manual data curation being feed to the expert system. This a hallmark of expert systems.
I wish to give a special thanks to Juan Pablo C., Assistant professor in Universidad Mayor, Chile and former Senior Bioinformatician for uBiome for bringing to my attention the article below. He was then kind enough to point me at appropriate data sources to allow me to implement this new measure.
Oral bacteria relative abundance in faeces increases due to gut microbiota depletion and is linked with patient outcomes
The detection of oral bacteria in faecal samples has been associated with inflammation and intestinal diseases. The increased relative abundance of oral bacteria in faeces has two competing explanations: either oral bacteria invade the gut ecosystem and expand (the ‘expansion’ hypothesis), or oral bacteria transit through the gut and their relative increase marks the depletion of other gut bacteria (the ‘marker’ hypothesis). … By distinguishing between the two hypotheses, our study guides the interpretation of microbiome compositional data and could potentially identify cases where therapies are needed to rebuild the resident microbiome rather than protect against invading oral bacteria.
62% of shared ASVs (Bacteria) were more abundant in the oral cavity, indicating that oral-to-gut translocation may be the main route of translocation between environments, and highlighting that this phenomenon might be more common than previously thought in healthy individuals of all ages.
I have implemented a new measure on Microbiome Prescription to estimate the amount of leakage. It is located in the Health Analysis section (a large and often slow loading page)
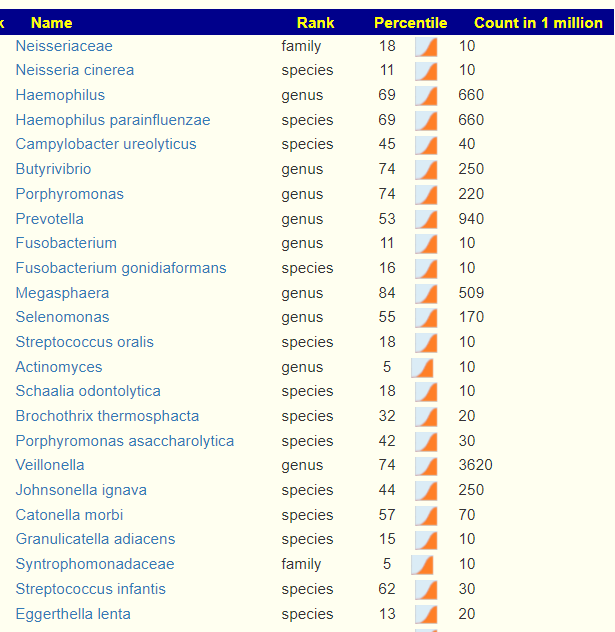
The report gives a percentile ranking based on the total for genus that are Oral Bacteria and then lists the specific genus and species present
As with other study specific pages, you can hand select bacteria of interest or click on the bacteria to get more information about the bacteria. Of special note is Prevotella being listed as there is evidence suggesting that it increases due to fungi in the environment – thus the gut microbiome depletion is likely why it can take up residency.
I will be looking to modify the suggestions algorithms to exclude oral bacteria and thus have the suggestions focused on gut microbiota depletion as a treatment option.
“For the Ombre/Thryve sample data, dated 12/31/24, I found the following:
Rickettsiales – order – 31%ile High
Rickettsiaceae – family – 34%ile High
Rickettsieae – tribe – 34%ile High
Parasutterella excrementihominis – species – 69%ile High
The reason these bacteria stand out to me are because my CFS journey, like many, began with a Lyme diagnosis 20 years ago. And as testing and research improved, Lyme became synonymous with “co-infections” like Rickettsia and Ehrlichia and a whole host of others in the “Lyme Soup”.”
Parasutterella excrementihominis has been present in all samples, varying from 61-89%ile. For Rickettsiaceae, we see in much older samples
2022-04-11 at 6%ile
2022-11-01 at 18%ile
All bacteria wax and wane over time. Personally, I would not be concerned unless it is constantly above 75%ile for pathogenic. It is is over, then take your concerns to your MD for appropriate testing to confirm..
For this person we have a lot of symptom forecasts[new algorithm] matching reported symptoms
Analysis
Ombre Lab Processing
We are looking at the Ombre Lab Report data below. These are a lot of swings over the last 4 sample. Looking at the prior (likely the worse)
Eubiosis was the worse
Bacteria Under 10%ile was the highest
Outside Kaltoft-Møldrup was the highest
Chao1 Index was the highest
A lot of other measures had little or no change (i.e. JasonH, Microba Co-Biome,,Nirvana/CosmosId etc) suggesting low sensitivity to detect shifts. Some hits at a continuous shift (Simpson Diversity Index.
The wide variety of lab read quality makes reliable comparisons difficult. The Lab Read Quality bounces around, and with that, other values may echo these shifts (i.e. up to 20% shifts for some measures). A low read quality means less bacteria are reported, for example, when it was low, the Outside Kaltoft-Møldrup has low, when it was high, the value became high.
Another way to view it is this: If 10% are out of range and 660 are reported then we have 66. If we have 940 in another report then we would expect 94. This could be misread as a 94/66 or a 43% increase in out of range bacteria. Technically, it is more complicated but that should explain the problem.
Criteria
12/31/2023
10/2/2023
7/28/2023
4/18/2023
Lab Read Quality
5.6
12.6
8
4.9
Eubiosis
53.4
8.2
38.8
83.1
Rickettsiaceae
34%ile
0
0
0
Outside Range from GanzImmun Diagostics
17
17
14
14
Outside Range from JasonH
5
5
5
5
Outside Range from Lab Teletest
32
32
25
25
Outside Range from Medivere
17
17
17
17
Outside Range from Metagenomics
8
8
7
7
Outside Range from Microba Co-Biome
5
5
6
6
Outside Range from MyBioma
16
16
9
9
Outside Range from Nirvana/CosmosId
24
24
26
26
Outside Range from Thorne (20/80%ile)
310
310
210
210
Outside Range from XenoGene
51
51
41
41
Outside Lab Range (+/- 1.96SD)
36
20
7
19
Outside Box-Plot-Whiskers
114
97
71
69
Outside Kaltoft-Møldrup
164
239
141
79
Bacteria Reported By Lab
765
941
762
663
Bacteria Over 90%ile
101
82
42
58
Bacteria Under 10%ile
60
302
102
28
Shannon Diversity Index
2.953
3.099
2.987
2.62
Simpson Diversity Index
0.043
0.053
0.079
0.098
Chao1 Index
23041
38183
26135
15707
Pathogens
28
25
23
15
Condition Est. Over 90%ile
1
1
1
1
Top 10 forecast symptoms matching
9
9
10
n/a
Rickettsiaceae was seen in earlier samples:
2022-04-11 at 6%ile
2022-11-01 at 18%ile
Biomesight Reporting
One sample could not be successfully processed thru Biomesight. Biomesight indicated that there are ongoing technical issues with their processing of Thryve FastQ files.
Criteria
12/12/2023
7/28/2023
4/18/2023
Lab Read Quality
5.6
8
4.9
Eubiosis
42.8
80.8
74.3
Outside Range from GanzImmun Diagostics
13
14
14
Outside Range from JasonH
3
5
5
Outside Range from Lab Teletest
16
23
23
Outside Range from Medivere
12
13
13
Outside Range from Metagenomics
5
8
8
Outside Range from Microba Co-Biome
1
2
2
Outside Range from MyBioma
8
4
4
Outside Range from Nirvana/CosmosId
11
23
23
Outside Range from Thorne (20/80%ile)
144
250
250
Outside Range from XenoGene
20
23
23
Outside Lab Range (+/- 1.96SD)
38
22
25
Outside Box-Plot-Whiskers
149
97
81
Outside Kaltoft-Møldrup
99
123
60
Bacteria Reported By Lab
664
696
618
Bacteria Over 90%ile
122
93
61
Bacteria Under 10%ile
38
46
9
Shannon Diversity Index
1.565
1.242
1.507
Simpson Diversity Index
0.037
0.057
0.078
Chao1 Index
17542
14092
10705
Shannon Diversity Percentile
41.2
10.8
32.6
Simpson Diversity Percentile
32.4
55.9
72
Chao1 Percentile
88.4
75.6
53.8
Lab: BiomeSight
Pathogens
25
23
19
Condition Est. Over 90%ile
1
1
1
Top 10 forecast symptoms matching
7
n/a
9
Bottom line, the variability of 16s Lab Quality leaves too much fogginess for interpretations 🙁
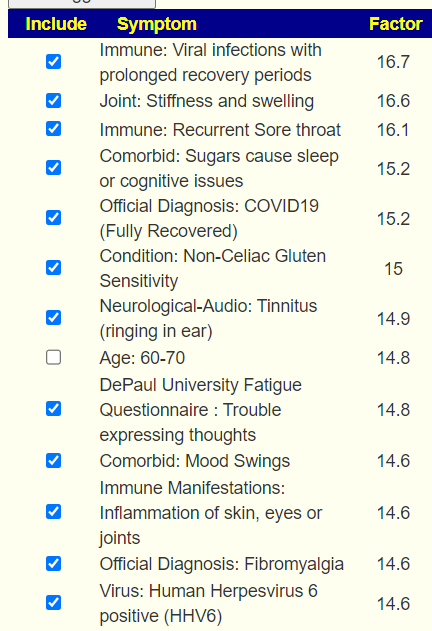
Revised Symptom Forecasting
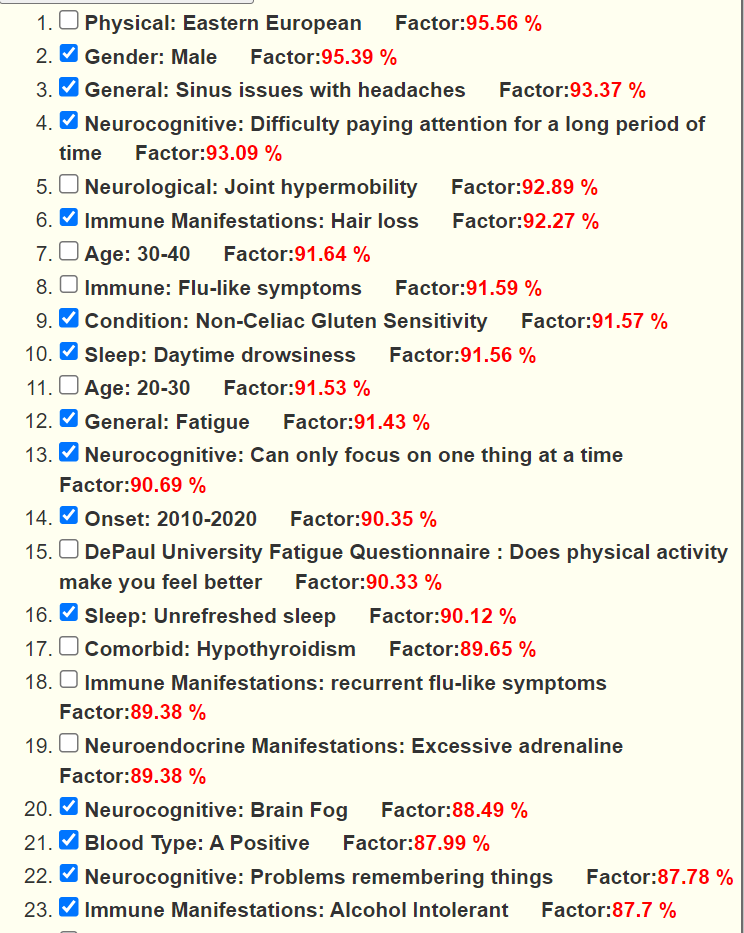
This algorithm is similar to the Eubiosis algorithm. We compute the expected number of matches to bacteria shifts associated with the symptoms. The expected theoretical threshold by randomness is 16%. A higher number indicate increased odds, a lower number decreased odds. This is based on the existing annotated samples uploaded. It is not definitive and often there can be multiple subsets of bacteria associated with a symptom. The match is on too much or too few of a collection of bacteria
The checkmarks are the entered symptoms, the list are the predictions from most likely to lesser.
As seen in another post over multiple samples, we have a good accuracy in predicting symptoms from the microbiome.
Going Forward
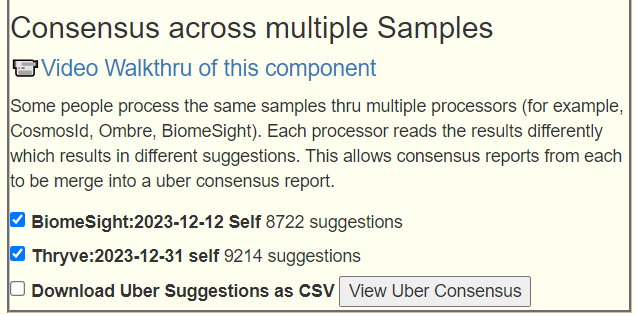
Again, using Just give me suggestions include Symptoms is how we are going to proceed. And then add in the two Special Studies. This results in 7 packages of suggestions for each lab. Since we have two different interpretations (Biomesight and Thryve) of the FastQ files. We then do an Uber Consensus merging 14 packages of suggestions!
And the merge (on [Multiple Samples] tab)
Thresholds: High is 383 thus 190 or higher, Low is -462 this -231 or lower
First we are going to look on what ALL 14 sets of suggestions agreed upon
Remember to check suggested dosages here. A common issue is taking token amounts which are unable to effect changes.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a result on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or anyone. Always review with your knowledgeable medical professional.








Recent Comments