hi ken, what would you do if there’s a massive contradiction between most of the suggestions generated by the general consensus and the suggestions generated by your new “from special studies” biomesight algorithm
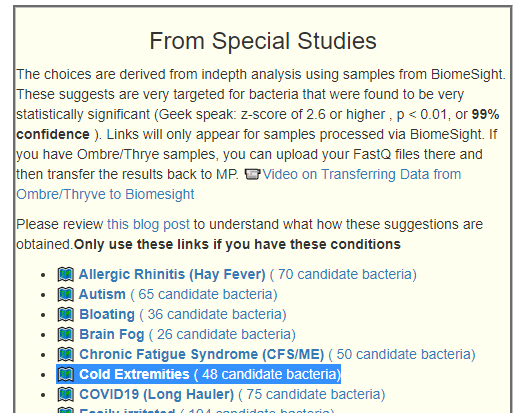
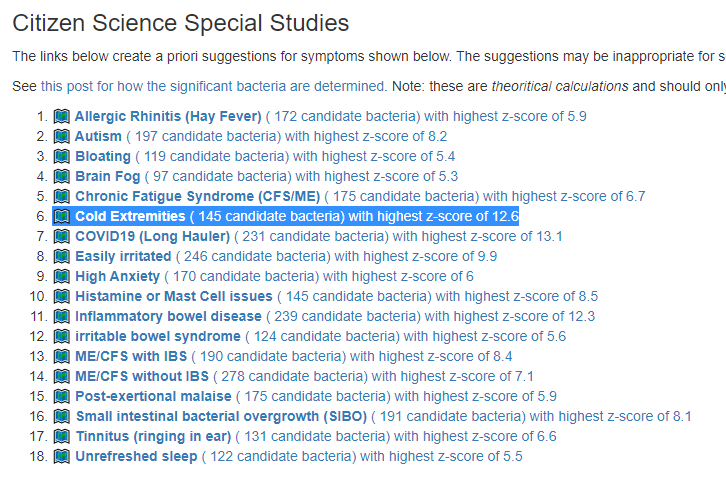
The first thing that I want to point out is the warning on that page.
The main issue you may be seeing is in the selection of bacteria. With the regular selection, you focus on extreme values, i.e. top 10%, outside of standard lab ranges, outside of reference ranges from Jason Hawrelak and others. The amount outside of the reference range is used to give a weight to each bacteria for the importance of shifting. Different algorithms are used with different approaches (we do not know what the ideal one is).
With the special studies, we up-ended the algorithm. We picked the bacteria based on a simple “if the amount is above or below the reference norm+/- twice the standard deviation of the mean for the reference population and then use the z-score as the weight (the statistical significance for this bacteria)”.
This change means that a bacteria that is at the 70%ile may be included in the selection (which is very unlikely with the the first methods), and this bacteria could have a very high weight (which is based on statistical significance and NOT the difference from a mile post). A Bacteria at the 99%ile will be totally ignored if it is not statistically significant for the condition.
Statistically, I prefer the special studies approach because we are using the statistical significance of the bacteria for the significance/weight for suggestions instead of the naïve assuming that being high or low is the cause.
Bottom Line
We pick bacteria based on statistical significance for a specific condition and not whether they are high or low in general
We give the bacteria a weight based on statistical significance for a specific condition and not the difference from a bound.
In theory, with the identical same bacteria and counts selected for two different conditions, you will get different suggestions because the weight assigned will be different since the weight is based on the statistical significance for the condition.
I well understand the confusion of some, the model being used is getting more advanced and handling more complexities.
This is a common symptom for both ME/CFS and Long COVID. This is reported often in samples, and thus being examined if it reaches our threshold for inclusion as defined in A new specialized selection of suggestions links. It does.
My default view is that this symptom is likely due to vesicular constriction/inflammation or “stick blood” (which contains many coagulation possibilities) resulting in low warming blood flow.
Study Populations:
Symptom
Reference
Study
Sleep: Unrefreshed Sleep
1087
78
Bacteria Detected with z-score > 2.6: found 145 items, highest value was 12.6
Enzymes Detected with z-score > 2.6: found 170 items, highest value was 5.3
Compound Detected with z-score > 2.6: found No items
The highest z-scores above are more than most other symptoms. This indicates that the causes are more homogeneous bacteria shifts.
In this study, one species shouts out as the cause by not being therePrevotella copri. I would really emphasis the items listed above as encouraging its growth.
It may be available “soon” as a probiotic, “The gut bacterium Prevotella copri (P. copri) has been shown to lower blood glucose levels in mice as well as in healthy humans, and is a promising candidate for a next generation probiotic aiming at prevention or treatment of obesity and type 2 diabetes.” [2021]
This is a common symptom for both ME/CFS and Long COVID. This is reported often in samples, and thus being examined if it reaches our threshold for inclusion as defined in A new specialized selection of suggestions links. It does, but the degree of association (z-scores) are lower than prior special studies despite having a larger study population.
Study Populations:
Symptom
Reference
Study
Sleep: Unrefreshed Sleep
1041
107
Bacteria Detected with z-score > 2.6: found 139 items, highest value was 5.1
Enzymes Detected with z-score > 2.6: found 208 items, highest value was 5.2
Compound Detected with z-score > 2.6: found 1 items, highest value was 2.8 – effectively zero when false detection rate is considered.
The highest z-scores above are less than other symptoms despite larger sample size. This indicates that the causes are more diverse and thus less homogeneous bacteria shifts.
Location of this custom filter
Interesting Significant Bacteria
All bacteria found significant had too low levels.
Low Veillonella is reported in some studies associated with sleep issues with it’s consumption of lactic acid(lactate) being cited as a possible factor:
“patients with sleep disturbances were characterized by lower bacterial diversities and distinct microbial composition in comparison to those without sleep disturbances. The relative abundances of Salivarius, Veillonella, Klebsiella, and Eubacterium were independent predictors of sleep disturbances in patients.” [2021] for the specific condition studied.
The key take away is that lactate/lactic acid levels appears to be a significant contributor. The reason that it is high is the lack of lactate consumers. Removal of lactate producing probiotics from supplements appears to be a logical first step (i.e. Lactobacillus), followed by taking Vitamin B1 shortly before bed time.
The issue may not be lactate by itself, but by the form of lactate (d-lactate –> bad)
Results and conclusion: Administration of L-lactate does not influence sleep-wake cycle of experimental animals. At the same time, its artificial optical analog D-lactate induces the significant (as compared to the control) decrease in wake (34.8% to 26.5%) and increase in slow wave sleep (57.4% to 69.2%). It has been suggested that D-lactate may be the antagonist of one or several L-lactate receptors.
“Thiamine (Vitamin B1) replenishment at intravenous doses of 100 mg every 12 h resolved lactic acidosis and improved the clinical condition in 3 patients.” [1997]
“Lactomin[300 mg Lactobacillus acidophilus, 300 mg Bifidobacterium longum] was discontinued, and she was treated with sodium bicarbonate and oral antibiotics. The probiotics the patient had taken were likely the cause of D-lactic acidosis ” [2010]
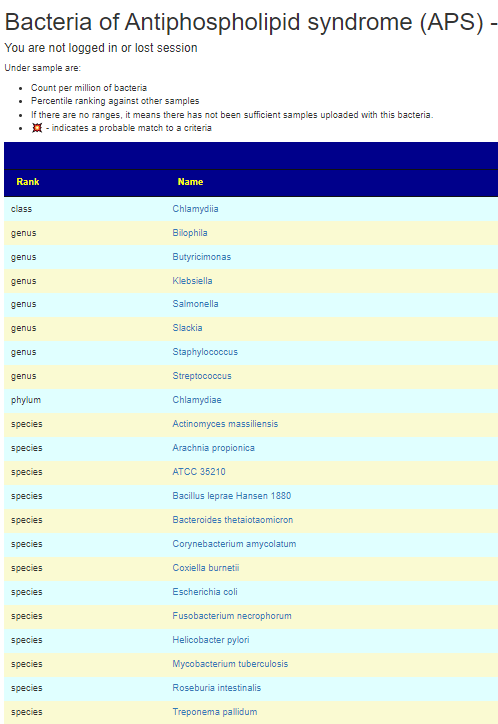
For almost a decade I have suspected that there was an interaction between the microbiome and Antiphospholipid syndrome (APS) also known as Hughes Syndrome (after the MD, see below). This is also called “sticky blood syndrome” [HealthLine]. For some researchers, it is deemed to be a significant contributor to fatigue in Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) [1999 D. Berg] and likely also applies to Long COVID. My own singleton experience seems to confirm it for myself.
A reader asked about phospholipids on Facebook today, so I revisited available literature
This article by Graham R.V. Hughes, MD, FRCP (the discoverer) in 2016 is well worth reading.
For me, APS/Hughes syndrome is very much a neurological condition. Brain function does seem to be especially targeted—the more APS patients one sees, the wider and wider the neuropsychiatric ripples spread.
Of course, running off the experience of just one, or even a few people, is not the best practice. Testimonials suck because of rose color glasses, fake testimonials, mainly positive responders report, and placebo effects. So what does the literature state. First there is some literature that are general discussions without the type of detail that I would love to see:
” In antiphospholipid syndrome, a thrombotic auto-immune disorder, autoreactive T cells and antibodies cross-react with auto-antigen mimicking peptides from gut commensals which appears to contribute to the pathophysiology. ” Gut microbiota and their metabolites in cardiovascular disease, 2021
Digging further we find:
Bacteroides thetaiotaomicron, Actinomyces massiliensis, Pseudopropionibacterium propionicum, Corynebacterium amycolatum, Ruminococcus gnavus and Roseburia intestinalis[2021] lead to the formation of pathogenic T‑cell and autoantibody responses via the cross-reactivity with autoantigens (Ro60, dsDNA and ß2 glycoprotein I).
M. pneumoniae and Streptococcus spp. infections, which are among the most prevalent bacterial infections in children and young adults, were linked to the occurrence of aPL. …. an anaerobic bacterium Fusobacterium necrophorum, although a variety of other bacteria such as streptococci, staphylococci, and enterococci may be also responsible…. a specific change in the gut microbial composition in APS patients. Particularly, a decrease of bacteria belonging to the genus Bilophila and overgrowth of bacteria of the Slackia genus were shown… enrichment by Slackia spp. and by the lower abundance of butyrate-producing Butyricimonas
APS only requires one of the bacteria above to trigger it. In terms of using Microbiome Prescription, I would look at Bilophila and Butyricimonas – if below 50%ile, hand pick it, then look at Slackia, if above 50%ile then hand pick it. Check the other bacteria cited above, and if any are over 75%ile, hand pick those. “It only takes one rotten apple to spoil the barrel” seems to apply here.
I have added APS to my PubMed reference list:
Personal Observations
I checked my samples from my last ME/CFS flare and found that Bacteroides thetaiotaomicron went from 73%ile on first sample after onset, to 96%ile on second sample, down to 79%ile, then 70%ile then 20%ile a few months later with recovery and returning to work. The key triggering bacteria will likely be different for each person but you at least have a candidate list to work from.
For items like antibiotics and probiotics, I have for a long time been a strong advocated for continuous rotation. The original source for this attitude was Cecil Jadin’s treatment protocol for occult rickettsia (which originated with the Pasteur Institute for Tropical Medicine). This was followed by reading studies finding that rotating or even just pulsing (2 weeks on/ 2 weeks off) was more effective in reducing bacteria than continuous. Probiotics often function via the natural antibiotics they produce (a lot of prescription antibiotics originated with bacteria); hence probiotic rotation became part of my preaching.
If you have microbiome related issues, my soapbox has been “your goal is make the stable dysfunctional microbiome, unstable“. Today I read a study on Nature that further clarifies what may be needed.
Together, these findings suggest that the human gut microbiome’s metabolic potential reflects dietary exposures over preceding days and changes within hours of exposure to a novel nutrient. The dynamics of this ecological memory also highlight the potential for intra-individual microbiome variation to affect the design and interpretation of interventions involving the gut microbiome.
Made from white rice flour, organic amaranth flour (Source)
Made from chickpea flour, organic yellow lentil flour, organic red lentil flour, organic kale powder, organic spinach powder (source)
Every two weeks change dominant proteins source
Fish
Pork
Lamb
Duck
Chicken
Turkey
Change vegetables and fruit too…
Change main spices used….
The key aspect is that every new addition results in a change of the microbiome. If you have microbiome issues, that is what you want to do. You do NOT want to take the same supplements, herbs, spices, vitamin or comfort food – continuously. You want to shake things up!
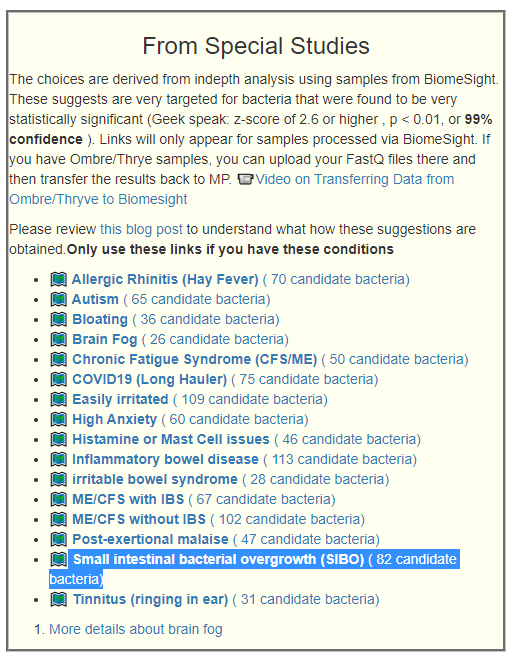
While the location of SIBO and the results of a stool test are a good physical distance apart, as part of an ongoing series of posts on special studies, I ran SIBO thru this morning — really expecting to find nothing, or perhaps a few overgrowths. To my surprise, the results was significant undergrowth with high statistical significance!
A formal post on the results is in the queue, but I thought that I should make the results available for those who wish to commit SIBO heresy!
On the [Changing Microbiome] tab
SIBO reaches our threshold for inclusion as defined in A new specialized selection of suggestions links. A summary table of various studies has been added there which shows the statistical association is actually pretty strong.
Of course, you are saying “but this is down stream how can it impact upstream?!!?” To me, it is like saying, “I was waiting in a queue and everyone is healthy except the first person in the queue who had COVID, how could I get it?” Bacteria spread, including upstream.
I should point out that these bacteria may not be the cause, rather they may be ‘the canaries in the coal mine’ of the microbiome. A few items of special interest are:
Bacteria
Reference Mean
Study
Shuttleworthia (genus)
273
33
Prevotella stercorea (species)
6378
31
Coprococcus eutactus (species)
7987
1463
Streptococcaceae (family)
3567
1473
Veillonellaceae (family)
17295
10944
Tissierellales (order)
4162
1457
Peptoniphilaceae (family)
4158
1456
In terms of enzymes, the four items that were most significant were all low levels of:
SIBO by definition is OVERGROWTH, the stool samples and statistics says it is an UNDERGROWTH condition. Undergrowth means that substances do not get processed fully….
In the mean while, people with SIBO can try the new algorithm on the changing microbiome page. Feel free to add comments here on experience after trying suggestions for a month.
REMEMBER: The usual test is finding various compounds on the breath. Are the compounds from producing too much(overgrowth) or the compounds are not being consumed enough (undergrowth). Both scenarios produce a positive result. It feels like someone jumped to a conclusion and this arbitrary decision stuck in the name.
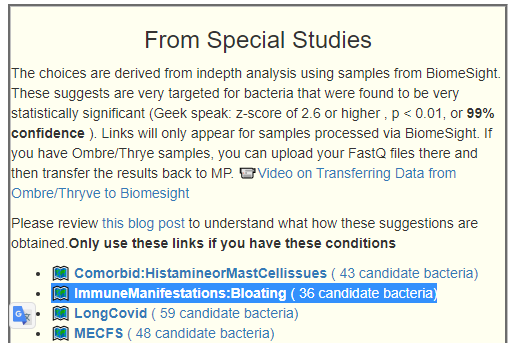
This is a common symptom for people that have uploaded. This is reported often in samples, and thus being examined if it reaches our threshold for inclusion as defined in A new specialized selection of suggestions links (A summary table of various studies has been added there).
Study Populations:
Symptom
Reference
Study
Bloating
1051
98
Bacteria Detected with z-score > 2.6: found 120 items, highest value was 5.4
Enzymes Detected with z-score > 2.6: found 298 items, highest value was 5.4
Compound Detected with z-score > 2.6: found ZERO items
The highest z-scores above are less than other symptoms with smaller study sizes. The likely cause is a more diverse study population
Interesting Significant Bacteria
All bacteria found significant had too low levels.
The dominant bacteria group seems to be Bifidobacterium, low Bifidobacterium . The latter we know little about. I should point out that these bacteria may not be the cause, rather they may be ‘the canaries in the coal mine’ of the microbiome. These studies’ methodology determines association and not causality.
“probiotics might improve the stool consistency of patients with IBS-C and increase the number of Bifidobacteria “
“B. animalis subspecies lactis supplementation may increase defecation frequency and, in short-term treatment, may reduce CTT in healthy adults and improve stool consistency in individuals without GIS. ” [2022]
“Bifidobacterium adolescentis were significantly less abundant in patients with Functional Abdominal Bloating/Distention, compared with healthy controls.” [2020]
REMEMBER: With your appropriate 16s sample, Dr. Artificial Intelligence on Microbiome Prescription will detail out foods, supplements et cetra to take (and to AVOID). If you do not have a sample, then review Bifidobacterium Summary Page.
This is a common symptom for both ME/CFS and Long COVID. This is reported often in samples, and thus being examined if it reaches our threshold for inclusion as defined in A new specialized selection of suggestions links.
Beyond the goal of identifying bacteria involved, I am curious on the intersection of the bacteria with ME/CFS and Long COVID – i.e. bacteria in common and not in common.
Study Populations:
Symptom
Reference
Study
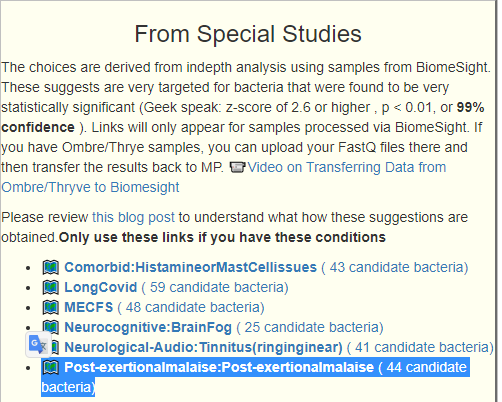
Post-Exertional Malaise (PEM)
1086
62
Bacteria Detected with z-score > 2.6: found 181 items, highest value was 6.2
Enzymes Detected with z-score > 2.6: found 237 items, highest value was 7.0
Compound Detected with z-score > 2.6: found ZERO items
The highest z-scores above are less than other symptoms. There are two possible reasons:
Smaller Study Population
A more varied population in the study group.
Interesting Significant Bacteria
All bacteria found significant had too low levels.
We have two dominant bacteria group, both Bifidobacterium and Sporolactobacillus. The latter we know little about. I should point out that these bacteria may not be the cause, rather they may be ‘the canaries in the coal mine’ of the microbiome. These studies’ methodology determines association and not causality.
hydrogen-sulfide:ferredoxin oxidoreductase (1.8.7.1): This is connected to iron. The blood uses iron to carry oxygen, and thus an absence/low level could [speculation] result in an impact on the blood’s ability to deliver oxygen (thus fatigue).
D-fructose:ubiquinone 5-oxidoreductase (1.1.5.14): This is also connected to iron.
For those wishing to explore more, you may wish to read Oxidoreductase
It does hint at an experiment to try: After exercise, try a dosage of Ubiquinol to see if it influences things.
Common Bacteria Shifts Observed in ME/CFS
We have 45 bacteria in common, they are listed below. A LOT of them are bifidobacterium, and no lactobacillus. This implies that bifidobacterium probiotics may be a good choice for ME/CFS with PEM
Tax_Name
Tax_rank
Thiorhodococcus pfennigii
species
Candidatus Tammella caduceiae
species
Veillonella atypica
species
Tammella
genus
Myxococcales
order
Gemella cuniculi
species
Bifidobacterium catenulatum
species
Nannocystineae
suborder
Olivibacter
genus
Campylobacterales
order
Epsilonproteobacteria
class
Campylobacteraceae
family
Pedobacter kwangyangensis
species
Haemophilus parainfluenzae
species
Haemophilus
genus
Clostridium aestuarii
species
Sterolibacteriaceae
family
Lactococcus fujiensis
species
Bifidobacterium bifidum
species
Atopobium
genus
Balneola
genus
Balneola vulgaris
species
Balneolaceae
family
Thiobacillus
genus
Pigmentiphaga
genus
Thiobacillaceae
family
Balneolia
class
Balneolales
order
Balneolaeota
phylum
Ruminococcus flavefaciens
species
Hydrogenophilalia
class
Hydrogenophilales
order
Hydrogenophilaceae
family
Atopobiaceae
family
Veillonella dispar
species
Veillonella
genus
Clostridium chartatabidum
species
Actinobacillus pleuropneumoniae
species
Sporolactobacillaceae
family
Sporolactobacillus putidus
species
Sporolactobacillus
genus
Bifidobacterium kashiwanohense PV20-2
strain
Bifidobacterium catenulatum subsp. kashiwanohense
subspecies
Bifidobacterium gallicum
species
Bifidobacterium cuniculi
species
Bacteria COMMON to ME/CFS and PEM
Common Bacteria Shifts Observed in Long COVID
We have 42 bacteria in common, they are listed below. We notice some interesting difference from above:
Lactobacillus at the genus level as well as the retail probiotic Lactiplantibacillus plantarum (AKA Lactobacillus plantarum)
Bifidobacterium is still there, but one of them is available as a retail probiotics.
Bifidobacterium animalis
Tax_Name
Tax_rank
Paenibacillus
genus
Veillonella
genus
Actinomycetaceae
family
Lactiplantibacillus plantarum
species
Actinomyces
genus
Flammeovirga
genus
Flammeovirga pacifica
species
Flammeovirgaceae
family
Lactiplantibacillus
genus
Phocaeicola massiliensis
species
Prosthecobacter
genus
Fusobacterium gonidiaformans
species
Candidatus Tammella caduceiae
species
Gammaproteobacteria
class
Tammella
genus
Coriobacteriaceae
family
Fusobacteria
phylum
Fusobacteriia
class
Fusobacteriales
order
Coriobacteriales
order
Bifidobacterium thermophilum
species
Dolichospermum curvum
species
Blautia wexlerae
species
Atopobiaceae
family
Actinobacillus pleuropneumoniae
species
Eggerthella lenta
species
Fusobacteriaceae
family
Atopobium
genus
Schaalia
genus
Bifidobacterium gallicum
species
Eggerthella
genus
Bifidobacterium animalis
species
Aerococcaceae
family
Coriobacteriia
class
Bifidobacterium cuniculi
species
Schaalia naturae
species
Phocaeicola sartorii
species
Leptospira licerasiae
species
Leptospiraceae
family
Leptospira
genus
Leptospirales
order
Alkalibacterium
genus
Bottom Line
There appear to be differences between ME/CFS with PEM and Long COVID with PEM. The main difference is with Long COVID: Lactobacillus probiotics is a suggestion; for ME/CFS it is not.
Remember suggestions that are specific to your unique microbiome are available on the Microbiome Prescription web site.
Tinnitus is not usually viewed as a microbiome issue. It was worth checking if it reaches our threshold for inclusion as defined in A new specialized selection of suggestions links. It did, hence this post
Study Populations:
Symptom
Reference
Study
Neurological-Audio:Tinnitus (ringing in ear)
1075
73
Bacteria Detected with z-score > 2.6: found 129 items, highest value was 6.3
Enzymes Detected with z-score > 2.6: found 493 items, highest value was 7.1
Compound Detected with z-score > 2.6: found ZERO items
Bifidobacterium probiotics: we have 4 in the top group. Unfortunately none of these species are available at the retail level (that I am aware of). Checking interactions for these 4, there was no significant interactions found with common retail bifidobacterium species, just with the general genus.
As above, all levels that were found significant had too little. I will leave it to the reader to go to Kyoto Encyclopedia of Genes and Genomes to learn about these enzymes (a steep learning curve).
gamma-L-glutamyl-L-cysteinyl-glycine:spermidine ligase (ADP-forming) [spermidine is numbered so that atom N-1 is in the amino group of the aminopropyl part of the molecule] (6.3.1.8)
Nothing was found again!!!! In one sense this was a surprise, in another sense, it hints that the results found significant are not random.
Bottom Line
This was an interesting analysis because the dominant deficiencies were in genus that are available as probiotics. In reality, it points to just 3 probiotics: an E.Coli probiotic and two bifidobacterium. Food suggestions will be generated on Microbiome Prescription using an individual’s unique microbiome.
Social Feedback
From The Gut Club: Stool Test Discussion Group
I went and looked at these two in combinations and got a lot of bacteria in common
Suggestions are available on Changing Microbiome tab on https://microbiomeprescription.com/
Study Populations:
Symptom
Reference
Study
Histamine or Mast Cell Issues
1092
56
Bacteria Detected with z-score > 2.6: found 143 items, highest value was 8.5
Enzymes Detected with z-score > 2.6: found 215 items, highest value was 6.1
Compound Detected with z-score > 2.6: found ZERO items
Interesting Significant Bacteria
One of the top items happens to have probiotics that are known to take up residency – are Symbioflor-2 and Mutaflor. . All of these top items are too low levels
Nothing was found!!!! In one sense this was a surprise, in another sense, it hints that the results found significant are not random.
Bottom Line
Histamine or Mast Cell Issues appears to a condition of deficiency. Common internet thinking is that it is a condition of a surplus of histamine producing bacteria. It is more likely that the normal histamine consumers are being starvedof enzymes that are needed to stop the accumulation of histamine.



Recent Comments