The intent of this site to assist people with health issues that are, or could be, microbiome connected. There are MANY conditions known to have the severity being a function of the microbiome dysfunction, including Autism, Alzheimer’s, Anxiety and Depression. See this list of studies from the US National Library of Medicine. Individual symptoms like brain fog, anxiety and depression have strong statistical association to the microbiome. A few of them are listed here.
The base rule of the site is to avoid speculation, keep to facts from published studies and to facts from statistical analysis(with the source data available for those wish to replicate the results). Internet hearsay is avoid like the plague it is.
For a number of years, I taught a 3rd year Artificial Intelligence survey course for Chapman University. Career wise while my “bread and butter” came from software engineering, I have in that profession often done data science, statistics and artificial intelligence for various employers.
Looking at AI systems for the microbiome back in 2015, I went with a model that I had used professionally: Expert System with Fuzzy Logic. An expert system use logic. The term fuzzy logic means that probability is used at decision points.
History Lesson
The first significant use of an expert system in medicine was the development and application of MYCIN in the early 1970s at Stanford University. MYCIN was designed to diagnose bacterial infections, particularly blood diseases, and to recommend appropriate antibiotics, taking into account factors such as patient weight and the specific infection identified. The system was based on a set of about 500 cause-and-effect rules and could explain its reasoning, as well as suggest additional laboratory tests if necessary.
MYCIN demonstrated the potential of artificial intelligence to support clinical decision-making, often matching or even exceeding the diagnostic accuracy of human specialists—achieving around 70% accuracy in controlled tests. Despite its success, MYCIN was never implemented in routine clinical practice, largely due to legal and accountability concerns regarding the use of AI in critical medical decisions.
Other expert systems were developed around the same time, but MYCIN is widely recognized as the first major, influential expert system specifically designed for medical diagnosis and treatment, marking a pivotal milestone in the history of AI in healthcare.
(Doctor) Watson Healthcare Application
IBM Watson’s entry into healthcare began in earnest around 2011, when IBM started developing healthcare-specific applications leveraging Watson’s natural language processing and machine learning capabilities. The system was designed to analyze large volumes of medical data—including electronic health records, medical literature, and clinical guidelines—to assist physicians in making more informed treatment decisions, especially in complex cases like cancer.
Key milestones and applications include:
2013: Watson’s first commercial healthcare application was for utilization management decisions in lung cancer treatment at Memorial Sloan-Kettering Cancer Center. This marked the beginning of Watson’s deployment in real-world clinical settings.
2016: IBM launched “Watson for Oncology,” a product designed to provide personalized, evidence-based cancer care options to physicians and patients.
Watson was positioned as a tool to bridge knowledge gaps, keep clinicians updated on the latest evidence, and support personalized care by tailoring recommendations to individual patient profiles. However, the initiative faced significant challenges, including high costs, privacy concerns, regulatory hurdles, and mixed adoption by healthcare providers. Notably, the partnership with MD Anderson Cancer Center was discontinued after substantial investment, and Watson for Oncology faced criticism for inconsistent recommendations and limited adaptability to local clinical practices.
Large Language Models
The first significant large language model (LLM) is generally considered to be GPT-1, released by OpenAI in 2018. GPT-1 was relatively small by today’s standards, with only 117 million parameters.
The release of GPT-2 in 2019 (with 1.5 billion parameters), and especially GPT-3 in 2020 (with 175 billion parameters), brought LLMs to much greater prominence and capability. These models, especially GPT-3 and later, are what most consider the foundation for today’s advanced LLM technologies.
Large language models (LLMs) present several well-documented problems and limitations when applied to medicine:
Hallucinations and Incorrect Information: LLMs can generate plausible-sounding but incorrect or fabricated medical advice, a phenomenon known as “hallucination.” This poses serious risks, especially when users do not verify outputs or lack medical expertise.
Lack of Medical Domain Optimization: General-purpose LLMs are often not fine-tuned with sufficient medical data, leading to misinterpretations of clinical terminology and context-specific nuances.
Transparency and Interpretability: The reasoning behind LLM outputs is often opaque (“black box” nature), making it difficult for clinicians and patients to understand or trust the basis for recommendations.
Algorithmic and Data Bias: Biases in training data or model design can result in unfair or inaccurate recommendations, especially for underrepresented patient groups.
Automation Bias and Overreliance: Clinicians may become overly reliant on LLM outputs, leading to uncritical acceptance and reduced independent judgment, a phenomenon known as automation bias.
Limited Regulatory Oversight: There is a lack of clear legal and ethical guidelines governing the use of LLMs in clinical settings, raising concerns about accountability and patient consent.
Information Completeness and Consistency: LLMs may provide incomplete or inconsistent answers, particularly when faced with complex or rare medical scenarios.
Privacy and Data Security: The use of sensitive patient data to train or fine-tune LLMs raises concerns about privacy, data security, and compliance with regulations like HIPAA.
Inequity of Access: Differences in technology access and digital literacy can exacerbate healthcare disparities, limiting the benefits of LLMs for certain populations.
Bottom line: Large Large Models are very questionable for use with the microbiome; while convenient, cheap and heavily hyped – there are so many issues that I view it has having huge legal liability risk dealing with the microbiome in a clinical setting.
Going Forward
A long time Ph.D. friend that attended multiple National Institutes of Standards and Technology conferences with me shared a post with me below. He, like me, have worked in senior positions as Architect and Strategist for firms such as Intel, VMWare, RSA and DELL, while I did time at Microsoft, Amazon, Starbucks and Verizon.
I responded with doing 7 times more data with 1/22 of the memory using my expert system!!!
He added: These LLM-ish technologies cannot approach the efficiency or trustability of an expert system or knowledge based system implementation, and LLMs fall apart under significant ambiguity.
LeCun ( world models (e.g. V-Jepa)), Pearl (Causal Models) and a few others are pointing the way to LLM alternatives (not an extension of LLMs).
The next step is at the intersection of Knowledge Representation and Reinforcement Learning , giving us a place to hang prior knowledge, ground truth, dependencies and real logics ( reasoning as opposed to chain of thought).
For those not familiar with these concepts and naively believe that AI is only Large-Language-Models.
Alternative AI Models
Yann LeCun
Yann LeCun is a Turing Award-winning computer scientist, Meta’s Chief AI Scientist, and a professor at New York University. He is best known for pioneering Convolutional Neural Networks (CNNs) in the late 1980s and early 1990s, which revolutionized computer vision and laid the foundation for modern deep learning systems. His work, especially LeNet-5, enabled breakthroughs in handwritten digit recognition and influenced countless AI applications, from facial recognition to autonomous driving.
LeCun is a vocal critic of the current generation of large language models (LLMs), arguing that they lack true reasoning, understanding of the physical world, persistent memory, and planning capabilities. He advocates for the development of world models—AI systems that can observe, interact with, and reason about the world, aiming for human-level intelligence.
V-JEPA (Joint Embedding Predictive Architecture)
JEPA (Joint Embedding Predictive Architecture) is a new paradigm in AI research championed by LeCun. Unlike traditional LLMs, which predict the next token in a sequence, JEPA aims to develop systems that can reason, plan, and interact with the physical world by learning from observation and experience.
JEPA’s core idea is to move beyond mere language processing, focusing instead on building AI architectures that can:
Understand and model the world (not just text or tokens)
Reason and plan based on learned representations
Maintain persistent memory for long-term understanding and context7
This approach is seen as a step toward more robust, general-purpose AI systems that could eventually surpass the limitations of current LLMs.
Judea Pearl (Causal Models)
Judea Pearl is a computer scientist and philosopher renowned for his foundational work on probabilistic and causal reasoning. He introduced the concepts of Bayesian networks and, most notably, the do-calculus for causal inference, which allows researchers to distinguish correlation from causation in complex systems.
Pearl’s causal models provide a mathematical framework for understanding how interventions (e.g., treatments in medicine) affect outcomes, enabling more accurate predictions and explanations in fields like epidemiology, economics, and machine learning. His work has had a profound impact on AI, particularly in areas where understanding cause-and-effect relationships is critical.
Hybrid AI Systems:
Combining symbolic AI (rule-based reasoning) with neural networks for more robust and interpretable A
Basic Criteria to evaluate an AI Model
Ability to Accurately forecast symptoms and conditions from a sample
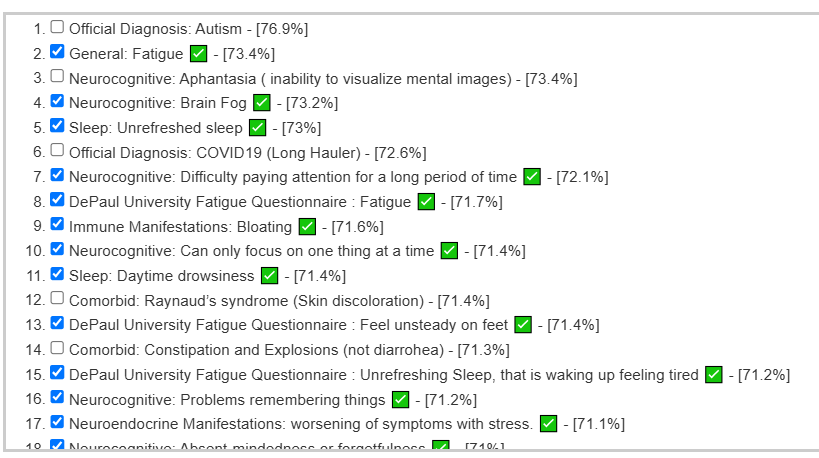
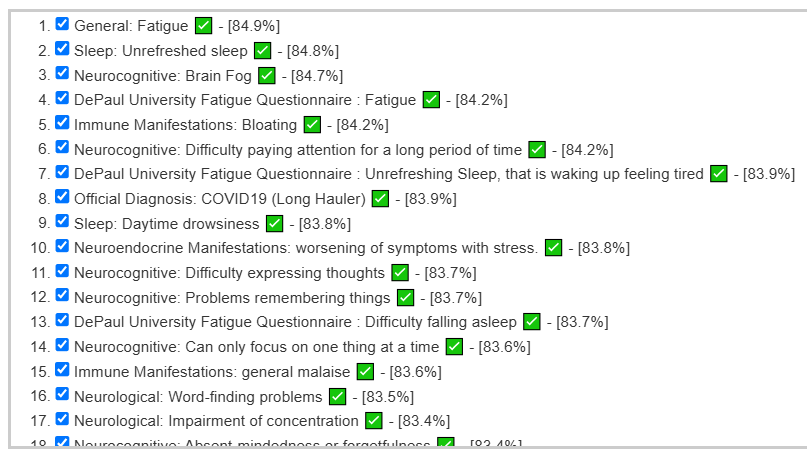
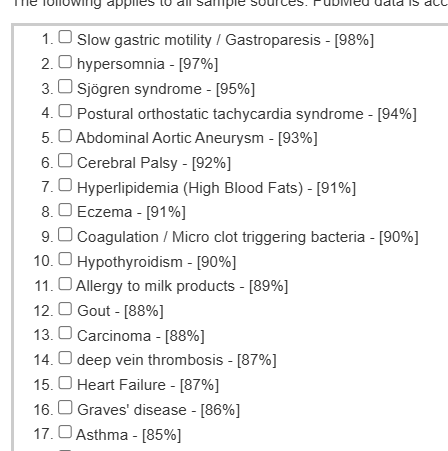
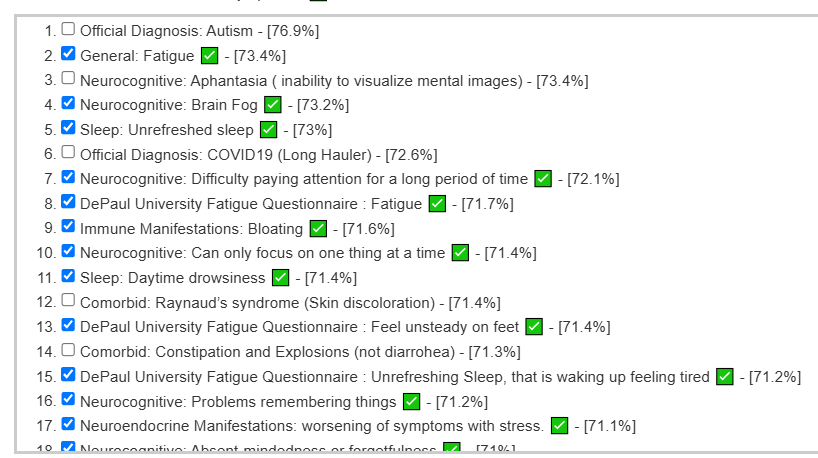
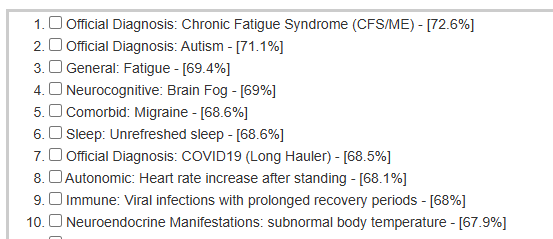
A recent educational analysis that I did had a high rate of correctly predicting symptoms. The illustration below are from developing a predictor on a collection of 4000+ samples processed through the same pipeline. The checkmarks are the symptoms that the user confirm having (i.e. a correct prediction).
The same person’s earlier sample ( when they had more severe issues) was even more impressive:
This can also be done using published studies but this has a challenge because of a severe lack of standardization in studies. This translates usually into rare repeatability of results.
Last week I had a nice session discussing this issue with the Scott whom I cited below.
Ability to provide objective evidence of improvement
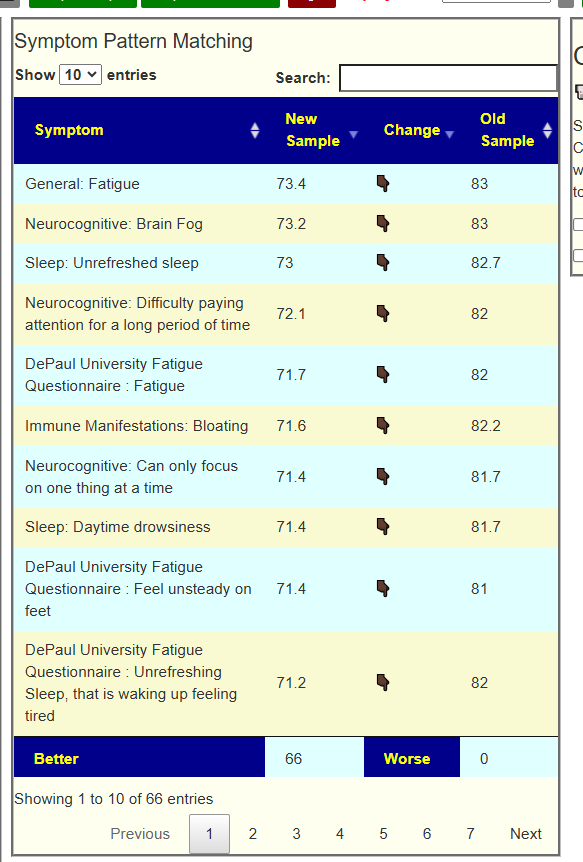
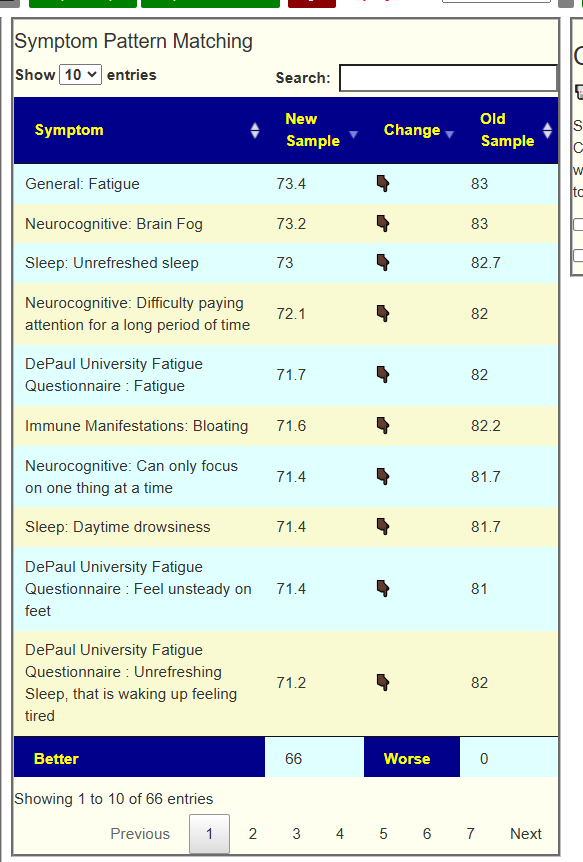
The ability to forecast gives a natural mechanism of evaluation. If the suggestions from the AI improves the microbiome, then one would expect the values for the forecasts to reduce. An example is shown below (full details). In this example, every single forecast value was decreased from implementing the suggestions from the expert system.
Access to data used above
The microbiome sample data annotated with symptoms that my expert system uses to build algorithms is freely available at my CitizenScience site.
Cheap and sloppy OR Expensive and accurate
Large Language Models (LLMs) are often considered relatively inexpensive to develop compared to earlier AI systems, since they can be trained by scraping vast amounts of text from the internet to identify statistical patterns. In effect, the knowledge these models acquire is based on the aggregate of publicly available information—much of which is uncorroborated or unverified, analogous to hearsay in legal terms.
Legal systems do not accept hearsay as reliable evidence, and this foundational limitation raises significant concerns when LLMs are used in medicine. If an LLM’s output leads to patient harm, its reliance on potentially unreliable or unverified sources could make it difficult for clinicians to defend their actions in malpractice lawsuits, as the standard of care in medicine requires decisions to be based on rigorously validated, evidence-based knowledge.
Expert Systems are typically costly to develop because their construction relies heavily on human expertise to define and encode logic rules. This process involves painstakingly translating medical knowledge and clinical guidelines into a structured set of rules that the system can follow. Furthermore, encoding the necessary facts into the system demands a thorough review of medical literature by subject-matter experts, which is both time-consuming and expensive.
These challenges are compounded by the nature of medical information itself. Critical data—such as detailed clinical findings, research outcomes, or supplementary evidence—are often found in tables, charts, and appendices within medical articles. Traditional expert systems can be engineered to process these structured formats, but this again requires manual effort and expert intervention. In contrast, large language models (LLMs) struggle to reliably extract and interpret information from such tabular data, as their training is primarily based on unstructured text and is less adept at handling complex, structured formats.
As a result, while expert systems offer the advantage of transparent, rule-based reasoning that can be clearly explained and audited, their development remains resource-intensive. This is due to the need for ongoing expert involvement, meticulous data encoding, and specialized handling of non-textual information that LLMs currently manage less effectively.
Bottom Line
My choice (before LLM days) of using Expert Systems appears to still be the most appropriate. While I currently use some Bayesian mathematics in the model (the “Fuzzy”). I will be digging into Judea Pearl’s Causal Models to see what may be effectively incorporated into the existing model.
In September 2023 I suffered a series of gut insults (food poisoning, antibiotics and gastritis) in a very short period. This gave me unrelenting brain fog and cognitive issues, fatigue, tinnitus, sleep difficulties, and a slew of other issues.
In an attempt to recover from this I went hard on prebiotics and probiotics, and seemingly without reason these would trigger worsening of symptoms. Looking back at my November 2023 sample (closest after the insult) on your website, I can see some of the items that made me worse, like slippery elm, were at the top of the avoid list! I wish I had an understanding of the website back then...
I have undergone multiple killing phases with antimicrobials, which did nothing but make me worse. I now see that building up the good bugs and crowding out the bad is the better technique for my situation.
After getting enough of understanding of your website and suggestions I have made some objective improvements in my most recent sample and across the board symptom matches are down. Unfortunately, this hasn’t resulted in symptom improvements (yet).
Today
My worst symptoms remain brain fog (cognitive issues, fuzzy thinking, memory issues, etc), fatigue and tinnitus. I remain bedbound since the event in 2023.
I believe your approach of focusing on enzymes and compounds are more likely to result in improvements for me than just targeting bacteria changes.
Upon reviewing my enzyme and compound movements, pre and post 2023, there are some that are likely to be causing my cognitive issues and maybe fatigue (such as very low L-LDH, high H2S, etc). What do you think about this?
Based on the most recent sample suggestions I am using apple cider vinegar, BB536, cannabinoids and dandelion.
Preliminary Analysis
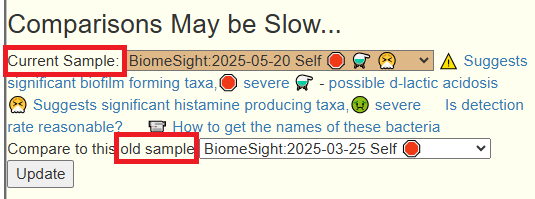
Using [Old Menu] / [Multiple Samples] is my usual start point when there are multiple sample.
I did a compare of the latest sample [2025-05-20] with [2025-03-25] and everything was better!
This person has a series of samples, so I am going to compare each against the prior to see the trend over time. The first sample marked with symptoms was 2023-11-30. Total is the count of distinct symptoms reported from prior and current sample.
Sample
Better
Worse
Total
2024-02-02
7
1
15
2024-09-05
78
0
78
2024-10-30
0
79
79
2025-02-20
0
1
70
2025-03-25
1
0
77
2025-05-20
66
0
66
There was a dramatic reversal in September 2024 which appears to be starting to correct itself in May 2025.
Going Forward
My approach is a three step approach.
Use the symptom patterns to identify the most likely bacteria involved. Then look for the best probiotics to address them
Use the symptom patterns to get a list of suggestions
Do a generic (not using symptoms) to get a 2nd set of suggestions
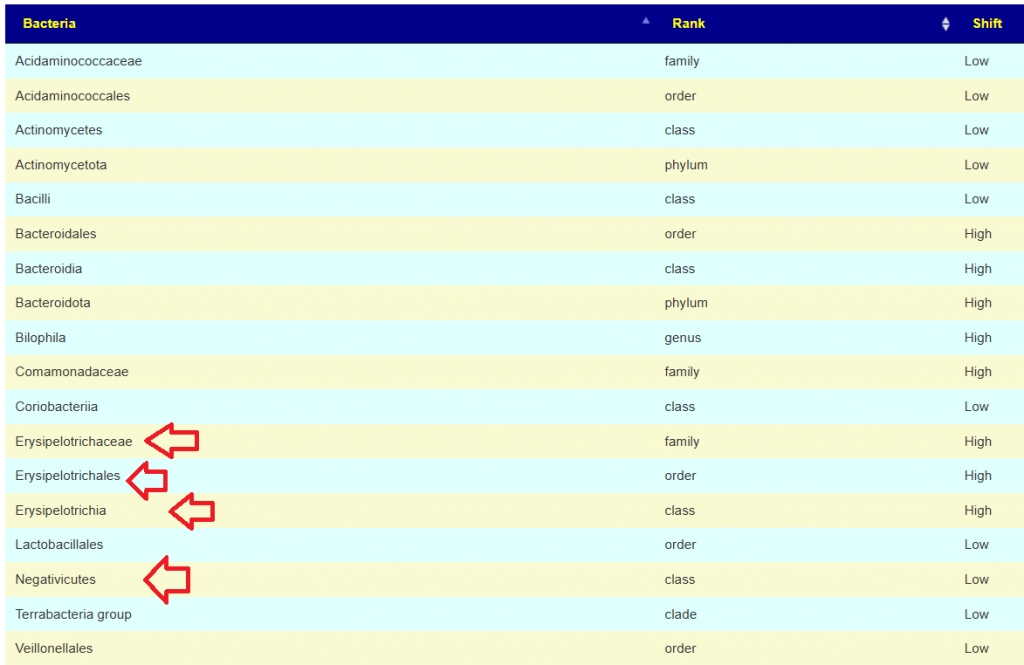
First step, using the symptoms to identify bacteria of interest and then get suggestions. We have a high rate of match for forecast symptoms and actual symptoms — which is a good indicator.
The result was just 6 bacteria identified as off.
Bacteria
Rank
Shift
Dysgonomonadaceae
family
Low
Erysipelotrichaceae
family
High
Erysipelotrichales
order
High
Erysipelotrichia
class
High
Hathewaya
genus
Low
Negativicoccus
genus
High
For comparison, I did the same for the prior sample and instead of 6 bacteria, we had 18. Four are in common with the above.
Focus on Probiotics ONLY
We have the most information on probiotics. We have the following sets of data to work from:
Clinical Studies: Certain probiotics are heavily studies, others are not. Often reporting of changes is on a few bacteria. Studies populations are small resulting in only strong associations.
KEGG Data on Metabolites and Enzymes: Complete coverage of all probiotic bacteria. Ignores epigenetics and related issues, i.e. we assume everything is “turned on”. Yeasts (i.e. aspergillus oryzae, Saccharomyces) not included.
Taxa R2 Site: Complete coverage of all probiotic bacteria and full taxonomy. Yeasts (i.e. aspergillus oryzae, Saccharomyces) not included.
Our goal is determine the bacteria probiotics that every diverse methods agree upon. That is the “consensus” or conservative Monte Carlo Model.
Experiment R2 approach
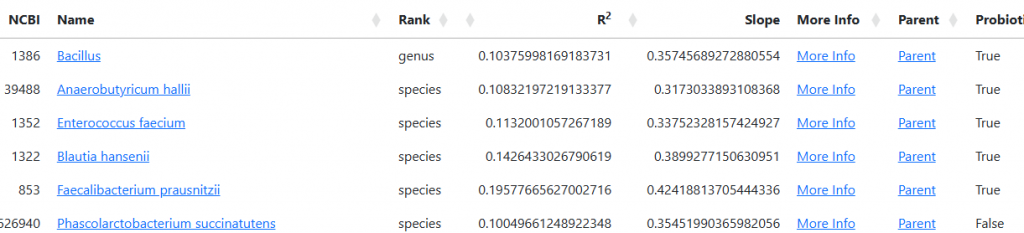
I went to Microbiome Taxa R2 Site to see if there are any probiotics that would be suggested based on these. I have only listed those currently available (not pending)
For Erysipelotrichia, Erysipelotrichales, Erysipelotrichaceae
It appears that E.Coli Probiotics are the only ones with a slim chance of reducing (Mutaflor, SymbioFlor-2) but that they appear adverse to the low bacteria above.
Clinical Studies
I checked probiotics and found the top 2 were Bifidobacterium and thus should be avoided? Why do I trust R2 over clinical studies… simple — clinical studies are sparse for data. Just bits and pieces of the puzzle. R2 is far more complete.
And then Experimental Using Metabolites also had them on the take list. So we have the three key probiotics that are available retail with consensus for all of the above methods.
Other Suggestions
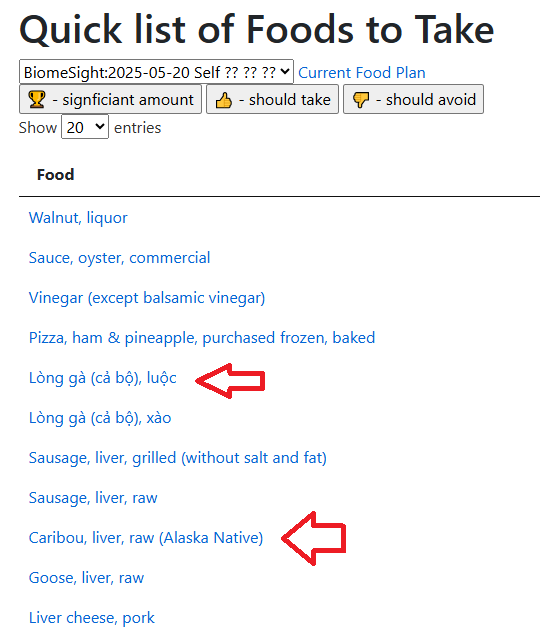
I am going to start with the Food Menu Planner. This look at some 111 nutrients identified and then at what various foods contain.
The site presents all recent results
The simplest way is to just click the “Quick” lists. It uses food nutrients databases from all over the world, so some items are likely not on your local café menu.
My general impression is try to get a single course of each of the two specific antibiotics above (after each course, do probiotics, then the next course, followed by a different probiotic). I see that Rye is positive and wheat is negative… so we will likely be eating 100% rye bread likely with liver paste (that is one of my favorite foods by the way!) and Pizza (light on the cheese).
Remember these are suggestions — not a protocol. suggestions are items you should take a bit more of or a bit less of! The goal is to persuade the microbiome to shift in the right direction. I have only highlighted items of interest, a review of the details should always be done.
Looping back to Brain Fog — typically caused by excessive d-lactic acid. I have several past post on this issue:
Checking your microbiome tree, I see high levels of Veillonella but with a gotcha, Veillonella is mainly Veillonella montpellierensis (99%ile), a novel species. 1/6 of studies on pubmed has this species causing issues like Polymicrobial bacteremia with little known about it. It is not listed on R2 site for Veillonella.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
For a time, the answer to this question was straightforward: uBiome.com was the go-to choice for microbiome testing. However, uBiome went out of business in 2019 following legal and regulatory issues, including an FBI investigation and bankruptcy13. As a result, uBiome is no longer an option.
Today, for most individuals—especially those not working directly with a specialist—the best available test is offered by BiomeSight.com. Unlike many other platforms, BiomeSight allows users full access to their raw data, supports data uploads from other providers, and offers advanced tools for those who want to explore their results in depth. Critically, they have the easiest transfer of data to Microbiome Prescription.
The reasons for this recommendation are detailed below.
Declaration of Interests
I do not sell any products or offer any services, nor do I have any financial interest in any microbiome testing companies.
My experience with microbiome dysbiosis, both personally and within my family, motivated me to develop Microbiome Prescription. Initially, I wrote code for my own use on my personal computer. Over time, I transitioned the platform to the web so that it could be accessible to everyone.
I offer data on Microbiome Prescription freely to individuals out of compassion for the suffering of others and as part of religious obligation-duty. Feel not! I will not preach.
An extreme shortage of expertise
The typical medical doctor or naturopath receives surprisingly little training on how to influence or manipulate the microbiome—often less than what you could learn from a focused day of watching YouTube videos. Most of their education is based on memorizing standard treatment protocols, which they then apply to patients in a “cookbook” fashion. For example:
If a patient has Crohn’s disease, prescribe these drugs.
If someone struggles with insomnia, suggest these herbs.
The core issue is that treatments are usually prescribed based on the diagnosis alone, rather than being tailored to the individual’s unique microbiome. In effect, practitioners are relying on broad stereotypes rather than personalized care.
Many healthcare practitioners have limited familiarity with the vast diversity of gut bacteria, often focusing narrowly on well-known genera like Lactobacillus and Bifidobacterium due to gaps in training and the complexity of microbiome science. Practitioners will often focus on these because they know no better. They do not know the significance of high Sphingobacterium bambusae or Dolichospermum curvum.
First Question: Who will interpret the results?
There are common paths that people take:
The lab themselves.
If they sell any product, there is a huge conflict of interest between their financial health and your personal health!
Often their suggestions are based off trolling the internet or using existing AI search engines
Most AI is prone to hallucinations
Often they may be based on a single study found on the US National Library of Medicine
I know one startup in this area that has a team of 6 Ph.D.s (or candidates) building a superior database than what Microbiome Prescription gas. They are barely 10% done. That is a very significant cost and needs significant financial backing to do. It requires a strongcommitment to not do a “good enough” to keep investors happy.
Word of warning: uBiome.com was one of the earliest labs and dominated the market. They filed for bankruptcy, IMHO due to investor pressure to turn a profit. Many labs keep expenses to the minimum and do not do due-diligence.
The healthcare practitioners that you are using and a specific test that they recommend. This assumes that they have been trained on the test. Buyer Beware: many will keep to cook book recipes.
You will go off and find a consultant to interpret the test. Conceptually that sound wise. The problem is that there are so many tests out there and finding someone with experience and successful track record is likely very hard.
You take ownership and education of the issue using selective resources, for example Microbiome Prescription free site. You should review your plans with your regular medical professional to insure no clear adverse issues with you medical history. In short, you are not asking them to develop a plan — you are asking them to make sure this plan is reasonable with no known health risks.
Amount of information in Test Result
The table below gives the possible test types. Typically:
qPCR gives 30-100 bacteria
16S gives 600 bacteria
Shotgun gives 6000 bacteria
IMHO 16S is the best give what we know about how to change the microbiome.
Method
What It Measures
Strengths
Limitations
16S rRNA Sequencing
Bacterial taxonomy (genus level)
Cost-effective, widely used
Limited resolution, misses non-bacteria
Shotgun Metagenomics
All DNA (all microbes, functions)
High resolution, functional insights
Expensive, complex analysis
qPCR
Specific DNA targets
Rapid, quantitative, targeted
Limited scope, requires known targets
Culture-Based
Viable, culturable microbes
Functional studies, viability assessment
Misses unculturable microbes
Metatranscriptomics
Active gene expression (RNA)
Reveals microbial activity
Technically demanding, expensive
Metaproteomics
Proteins produced
Functional protein insights
Complex, needs advanced equipment
Metabolomics
Metabolites (small molecules)
Functional metabolic readout
Source of metabolites often ambiguous
Specialized Sampling
Microbes from specific locations
Spatial resolution, targeted sampling
Invasive, technically challenging
What test gives the most actionable items using Microbiome Prescription database and expert system?
As a statistician, sample size determines the ability to detect patterns, make forecasts and thus identify the key bacteria connected to your symptoms.
BiomeSight has 308 Symptoms – thus we know which bacteria of the 600 to focus on
OmbreLabs/Thryve has 86 Symptoms
uBiome has 67 symptoms
There are a few things that 16s does not detect which shotgun does (virus, phages, antibiotic resistance etc). A small number of people may need that information … unfortunately, the ability to detect which bacteria are responsible for your symptoms is lost.
For more background, you may want to watch this video.
This recent discussion with a Long COVID patient that used Biomesight and the data from Microbiome Prescription may be helpful.
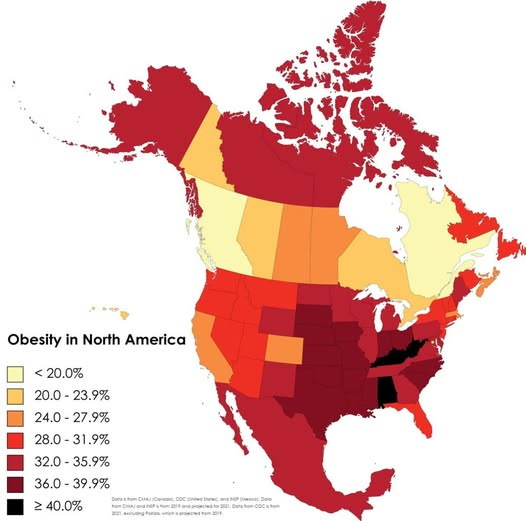
Fecal Transplants has shown the obesity is very microbiome controlled. With no change of diet, a lean mouse with a fecal matter transplant from a fat mouse, became fat.
Like the song about White Rabbit by Jefferson Airplane (referencing Alice in Wonderland book), we need to make sure we take the right (probiotic) pill.
One pill makes you larger And one pill makes you small And the ones that mother gives you Don’t do anything at all
Severity of Issue
Human Studies
When used as single-strain, all probiotic interventions showed positive effects in decreasing body weight, BMI, waist circumference, body fat mass or fat percentage. These strains belonged to the genera Lactobacillus (L. rhamnosus CGMCC1.3724 (LPR) [25], L. gasseri BNR17 [38], L.gasseri SBT2055 [27], L. sakei CJLS03 [46] and L. plantarum Dad-13 [49]), Bifidobacterium (B. lactis Bb-12 [36], B. animalis ssp. Lactis 420 (B420) [51], B. animalis CECT8145 [39]) and Pediococcus (Pediococcus pentosaceus LP28 [34])…. a maximum dose of 5 × 1010 (50 BCFU)
many of the studies the probiotic/synbiotic intervention was accompanied by dietary or physical activity interventions, which may have hidden the real effect of the probiotic strain(s) used.
Probiotic supplementation may also cause weight gain. Jones et al. [122] conducted trial in 19 obese adolescents, administering three packets per day of a mixture probiotics (L. acidophilus BA05, L. plantarum BP06, L. paracasei BP07, L. delbrueckii subsp. bulgaricus BD08, B. breve BB02, B. longum BL03, B. infantis BI04, and S. thermophilus BT01) for 16 weeks. Compared to placebo, observed a statistically significant increase in body weight in people using VLS#3.
“The case from Rhode Island (or mom gets fecal transplant and gains weight).. When Stacy returned to clinic 16 months later she had gone from 136 pounds to 170 pounds” [2015]
From Perplexity: “Systematic reviews and meta-analyses highlight that combinations of various Bifidobacterium and Lactobacillus strains tend to be more effective than single-strain probiotics for reducing body weight, BMI, waist circumference, and body fat mass”
Vet Studies
These appear to lack dietary or physical activity interventions and thus may be preferred combinations.
My model is simple, events pushed someone into a obesity dysbiosis where it become “stuck”. The dysbiosis has a distinct metabolite mixture that alters the human brain to prefer foods that feeds the dysbiosis. The metabolites results in higher efficiency of fat and protein absorption which the body then stores.
If you can alter the bacteria (and thus metabolites) to less efficiency then weight loss may occur naturally. There is some evidence that this may be possible with appropriate probiotics.
Without dietary or physical activity interventions, I believe that the Vet/Dog Studies probiotic pairs are likely the best (study evidence based) with the suggestions from the above exploration being very reasonable.
I have personally tried those combination and slowly loss weight with no clear dietary or physical activity interventions. The source that I used (I trust Maple Life Science for being correctly identified and fresh from the fermentation vat): Click to go to ordering page [No financial interests].
I’m excited to share the launch of R² Microbiome Prescription (https://R2.MicrobiomePrescription.com), a platform dedicated to unraveling bacterial associations in the microbiome. The name “R²” reflects the Coefficient of determination—a statistical measure showing how strongly one variable (like one bacterial presence) correlates with another (e.g., a different bacteria presence). Think of it like income and spending: as salary rises or falls, spending often follows, though this doesn’t prove salary causes spending changes.
Why focus on associations? While correlation ≠ causation, I lean toward the idea that bacterial relationships in the gut often hint at underlying causal mechanisms. For instance, one microbe’s metabolites might directly feed or inhibit another, creating a metabolic chain reaction. With thousands of metabolites (and counting!) interacting in complex ways, pinpointing exact cause-effect relationships is like solving a 4D puzzle.
The challenge ahead Current research is racing to map these connections, but the sheer scale of interactions—combined with individual variability—makes definitive conclusions tough. My goal with R² is to aggregate data, spotlight patterns, and inspire deeper exploration into how these microbes might shape health.
Feel free to explore the site and join the conversation!
Keep It Simple Statistics (KISS)
Over the years, I’ve experimented with various methods to uncover meaningful bacterial associations—a journey that’s been both challenging and gradual. After much trial and error, I finally developed a methodology that consistently delivers reliable results, which I’ve now used to populate the new site.
A turning point came during discussions with Precision Biome. They encouraged me to apply this approach to their extensive dataset of shotgun sequencing samples from healthy individuals. This collaboration provided the perfect opportunity to put my method to the test on a large scale—and ultimately led to the creation of the site you see today.
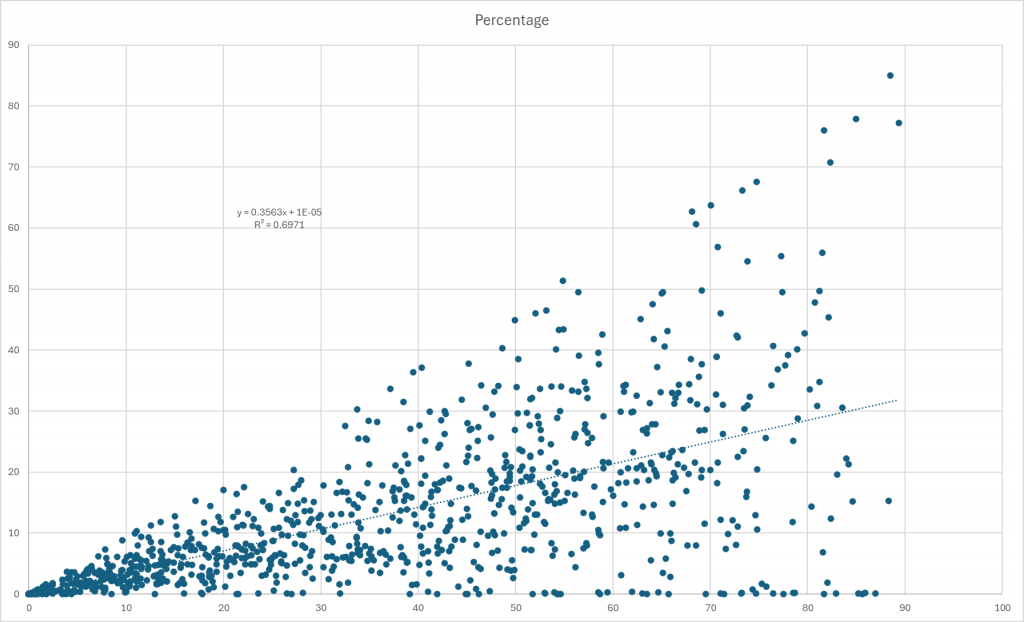
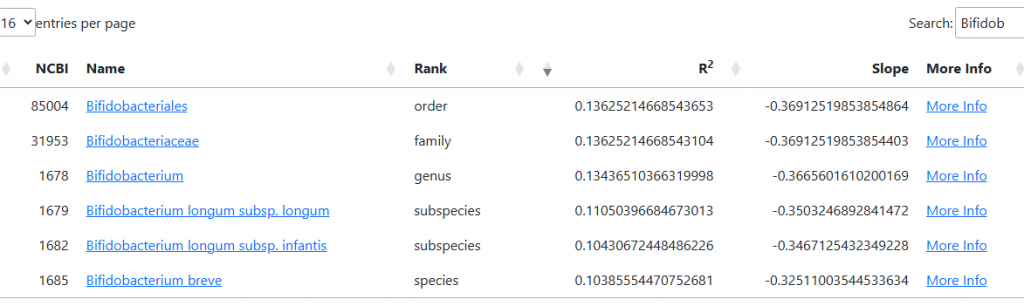
Getting R2 by Percentages
Here’s an example of a clear association between two taxa using percentages of each in samples: R² = 0.6971 and Slope = 0.3563.
An R² value of 0.6971 indicates that nearly 70% of the variation in one taxon’s abundance can be explained by changes in the other, reflecting a strong linear relationship between them. The slope of 0.3563 shows the rate at which one taxon’s abundance changes in relation to the other—specifically, for every unit increase in one, the other increases by about 0.36 units.
This kind of result highlights how statistical measures like R² and slope help quantify and visualize associations within complex microbiome data.
The relationship is typically not so linear. This was a specific example picked for illustration.
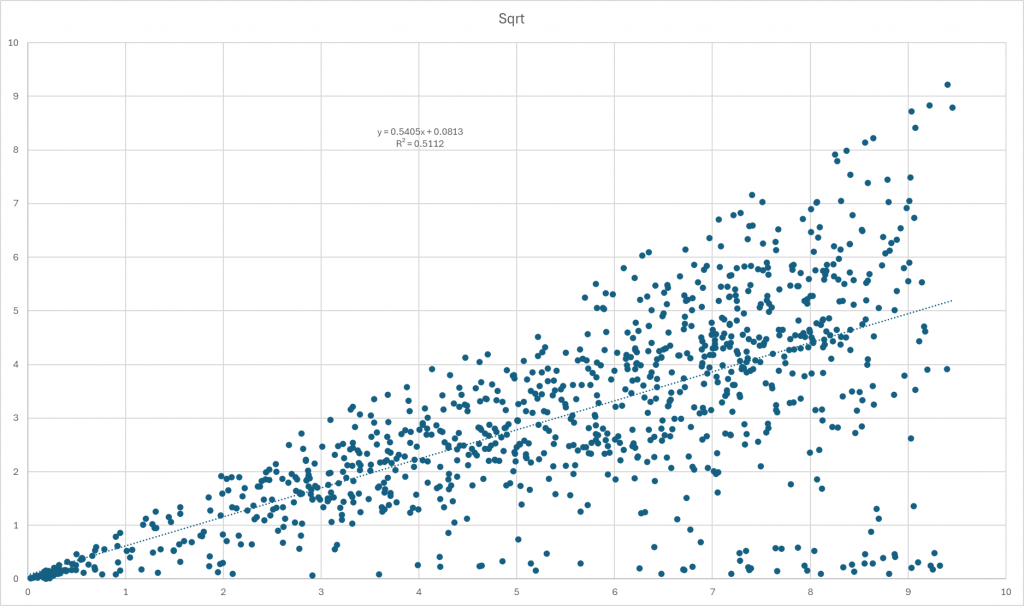
[BELOW] Applying a monotonic increasing transformation like the square root to the data changes the association metrics: in this case, R² drops to 0.5112 and the slope increases to 0.5405, indicating a weaker linear relationship compared to the original analysis. This reduction in R² means the transformed data explains less of the variance between the two taxa, making the association less robust than before.
Square root and similar transformations are commonly used in microbiome studies to stabilize variance, handle skewness, and address issues like zero-inflation and compositionality in the data. However, these adjustments can sometimes reduce the strength of observed associations, as seen here, because they alter the data’s distribution and the nature of relationships. Our goal is not to get a linear relationship, rather to get the best R² while preserving the nature of the data (i.e. all transforms should be monotonic increasing transformation)
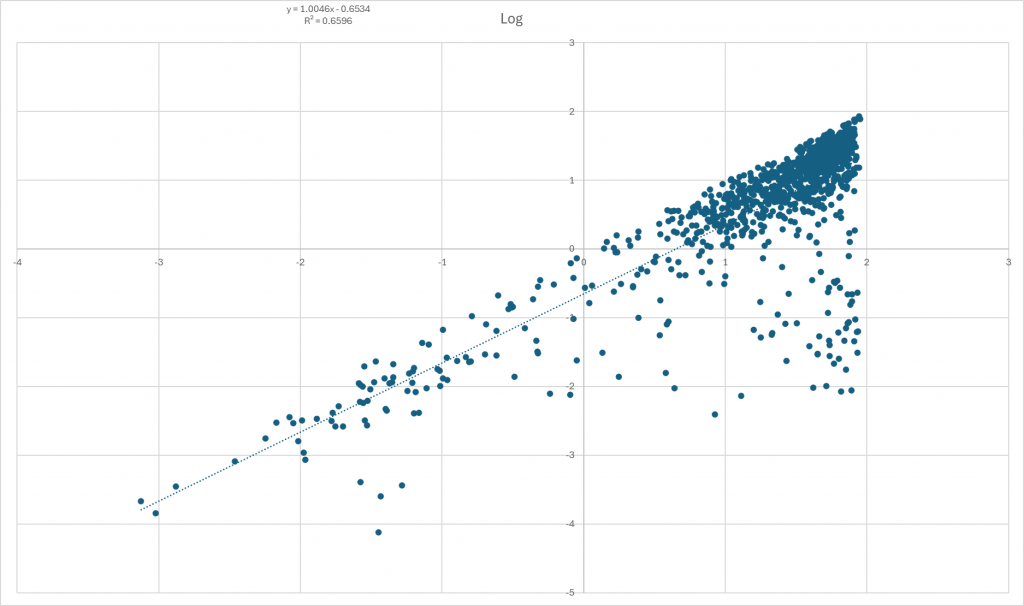
[BELOW] Applying a different monotonic increasing transformation, such as taking the logarithm of the data, yields R² = 0.6596 and Slope = 1.0046. This result is an improvement over the square root transformation, as indicated by the higher R² value; but less than the first linear one.
A logarithmic transformation is often used to manage skewed data and compress large ranges, making relationships more linear and easier to interpret. In this case, the higher R² suggests that the log transformation preserves more of the association between the two taxa compared to the square root transformation. The slope of 1.0046 indicates a nearly one-to-one relationship between the log-transformed values of the two taxa.
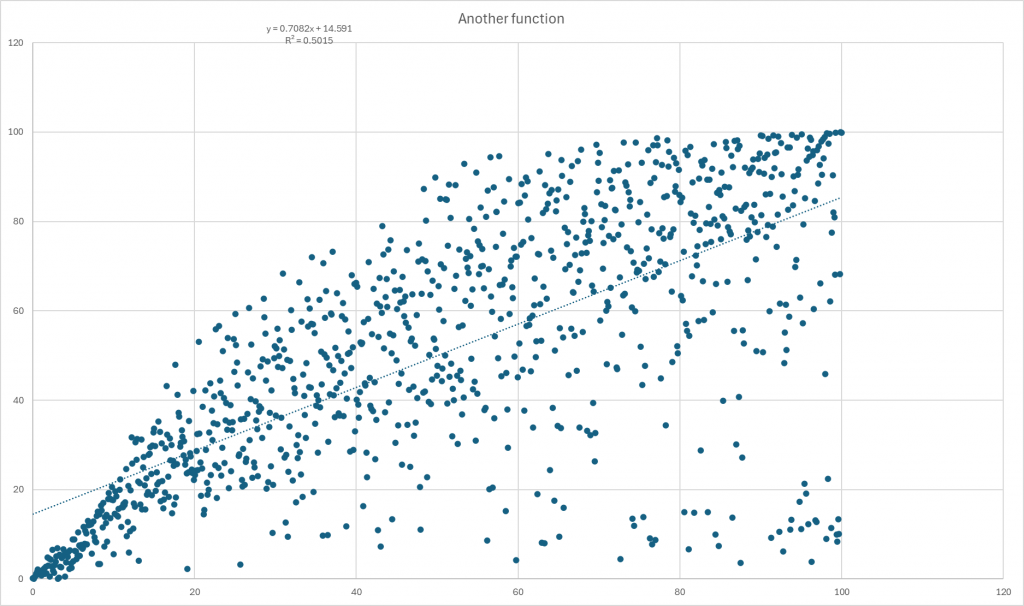
[BELOW] We can also experiment with other transformations to see how they affect the association. The more complex transformation that I prefer yields R² = 0.7082 and Slope = 0.5015.
This R² is the highest among the transformations tested so far, indicating that this method captures the relationship between the two taxa most effectively. The slope of 0.5015 shows a moderate rate of change between the transformed values of the taxa.
This example highlights how choosing the right transformation can significantly enhance our ability to detect and quantify associations within microbiome data. By carefully selecting and testing different approaches, we can better reveal the underlying patterns and relationships that might otherwise remain hidden.
R2 is the amount of influence, slope indicate direction of influence
It’s important to avoid combining R² and slope by multiplying them together. This is not a standard or meaningful statistic in regression analysis and can easily lead to misinterpretation. For instance, a high slope with a low R² suggests that while changes are dramatic when they happen, the overall model does not explain much of the data’s variance.
Remember:
Slope tells you the direction and rate of change (whether the relationship increases or decreases).
R² indicates how much of the variation in one variable can be explained by the other (the strength of the association).
Each metric provides valuable information on its own, but their product does not offer any additional insight and can actually be misleading.
Criteria for selecting transformation
For any given pair of bacteria, it’s technically possible to find a data transformation that maximizes the R² value for that specific pair. However, with 5,000 taxa, there are over 25 million possible pairs (5,000 × 5,000), making it an overwhelming and impractical task to optimize each one individually.
Ideally, the goal is to identify a single transformation that performs well across both low and high R² values for all pairs. Discovering such a transformation was a significant part of my journey. To keep the analysis manageable, I focused only on bacteria present in at least 0.3% (0.003) of the samples, which helped reduce the number of pairs to a more reasonable level.
I’ve found a favorite transformation—demonstrated in the last chart above—that I’m particularly satisfied with. If I discover an even better transformation in the future, I simply rerun the analysis and select the one that yields the highest R² values. This approach ensures that the associations presented are as strong and meaningful as possible.
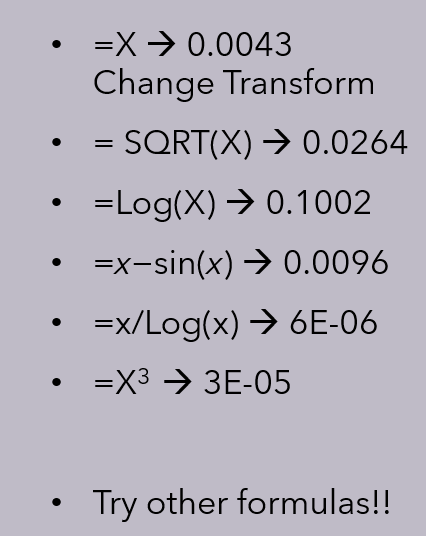
A practical alternative is to run regressions with multiple transformations and picked the transformation for each bacteria pair that has the highest R². I would suggest some of the following transformation be tried:
linear function with positive slope
cubic function
square root function (converting percentage to 0 – 1 range)
exponential function with base e
natural logarithm
logistic function
general exponential function
x−sin(x)
x/(log(x)
This will increase the computations from 25 million to 250 million. Remember computer resources are cheap today (say he would started doing statistics using a HP-21 calculator and WatFor). And fast using parallelism (multiple cores and threads).
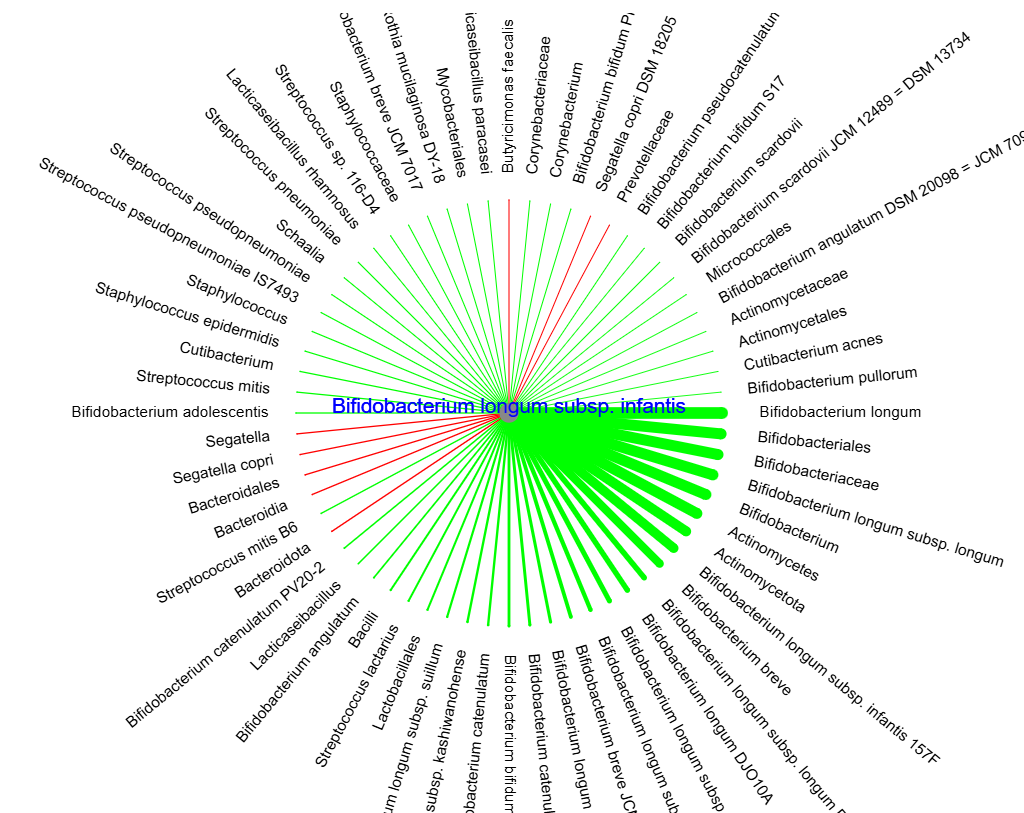
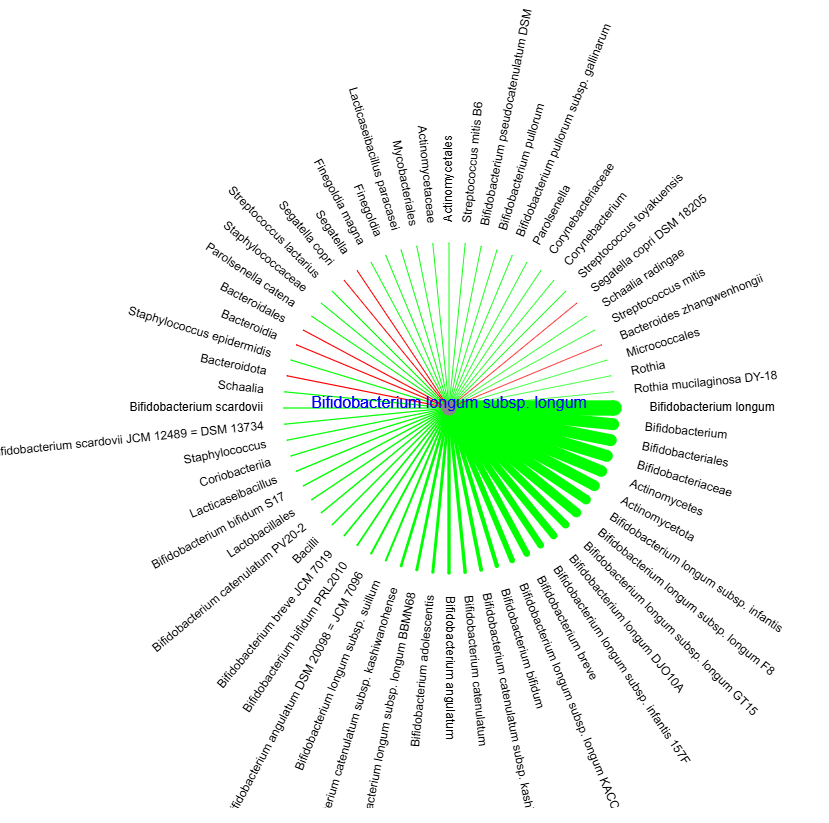
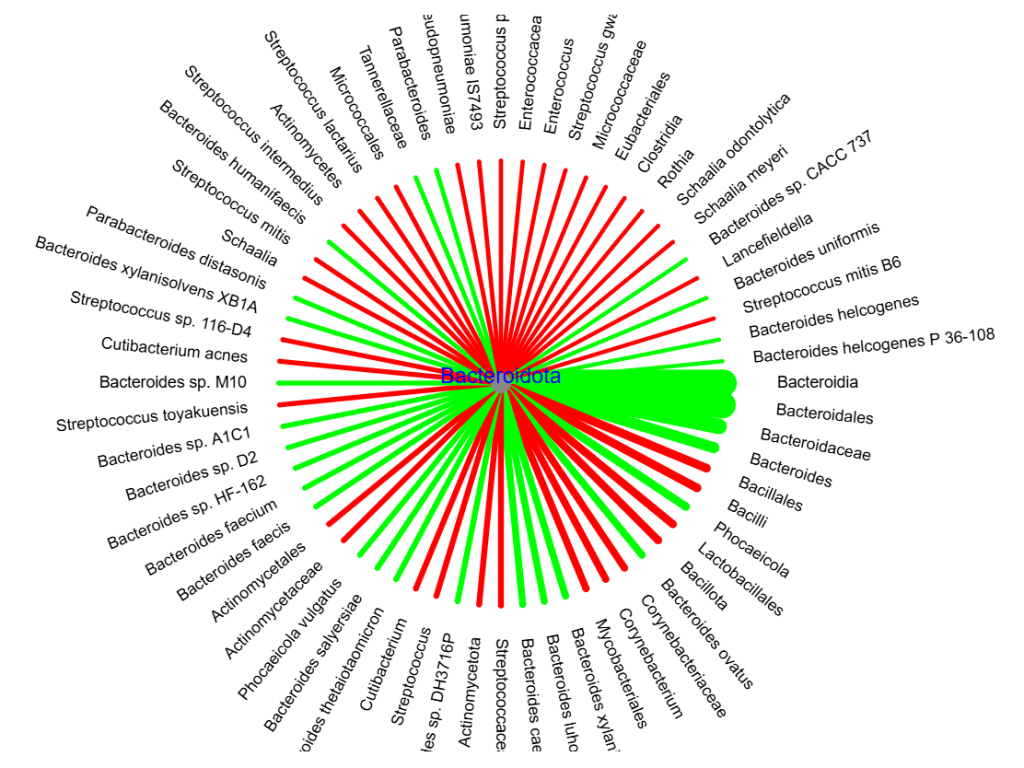
Usage With Probiotics
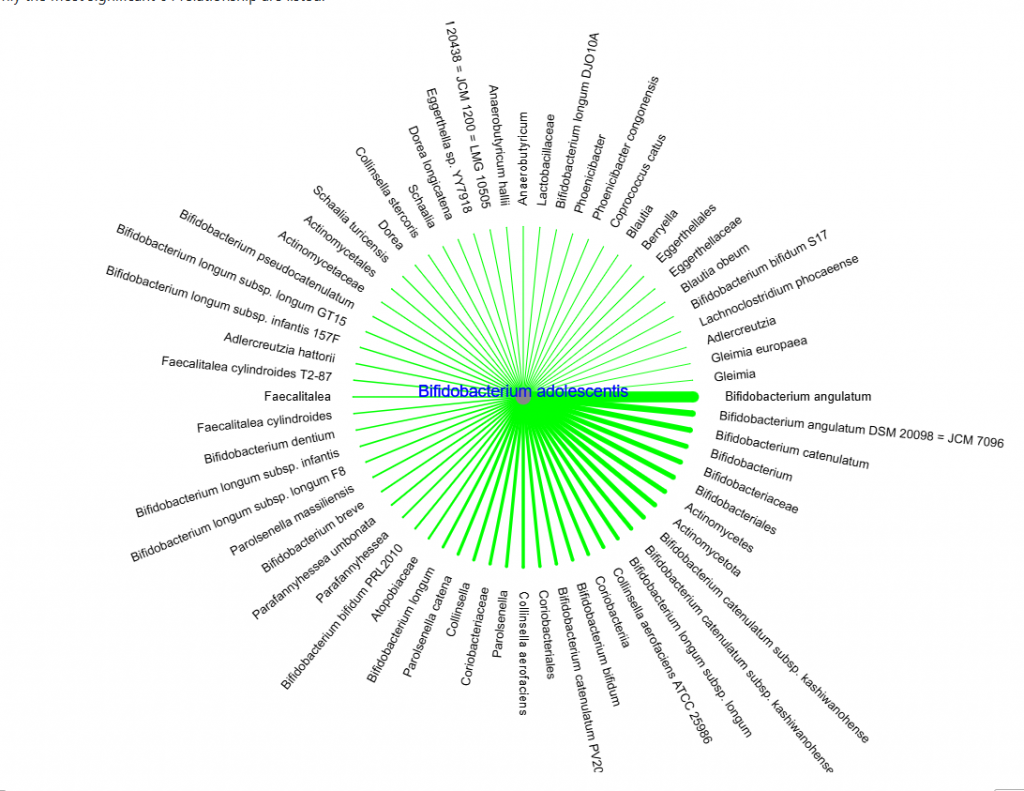
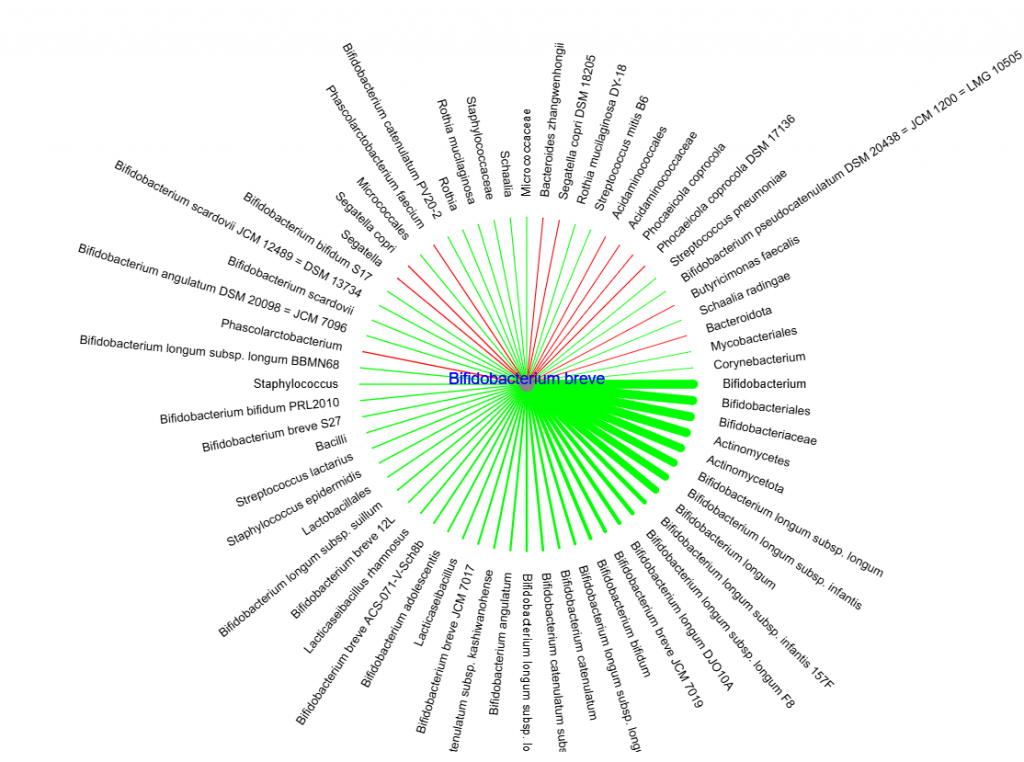
Suppose your Bacteroidota levels are too high and you’re considering which Bifidobacterium probiotic to take. If you turn to published studies, you’ll notice that most research focuses on individual probiotic strains, making it difficult to directly compare their effects. Instead, let’s examine the comparative data in the charts below to help guide your choice.
The harsh reality is that we cannot trust most bacteria identification with the microbiome and with probiotics.
Precision Biome (who supplied the dataset) are doing things what I deem the right way:
They are using the same pipeline that the above data came from (no ambiguity in bacteria identification) for client samples that they received.
They are working with an EU probiotic manufacturer directly.
The contents of the probiotics is also verified with the same pipeline
The probiotics come directly from the factory and are not stored in questionable environments before being delivered to the client
They intend to use the data from this site in identifying the best probiotics for each client
This is (IMHO) the ideal trifecta for clinical use of the microbiome. It is the strategy that I hope responsible microbiome testing firms move to.
Quick Test
Some one asked about probiotics that reduces Campylobacter. The page shows known (and pending) probiotics. We found none listed to reduce it. We did find some that increases it.
Bacillus is a genus and covers many species — so difficult to evaluate.
Not as good as actual studies? — but reasonable for sparse data
Critical Evaluation of Microbiome Study Limitations & Proposed Solutions
Key Factors Impacting Credibility
Current microbiome research faces significant validity challenges due to three core assumptions:
Taxonomic Accuracy of 16S rRNA Sequencing
The 16S pipeline (used in >80% of studies) has notable limitations: ▪ Struggles with species/strain-level resolution ▪ Database gaps create misclassification risks ▪ PCR amplification biases skew abundance data
Probiotic Product Integrity
Studies often assume supplements match label claims, yet: ▪ DNA analyses show 30-50% mislabeling in commercial probiotics ▪ Viability issues occur in 40% of products (esp. non-refrigerated) ▪ Strain-specific effects are frequently overlooked
Population Generalizability
Most trials use narrow cohorts: ▪ 78% of probiotic studies focus on healthy adults ▪ Gut ecosystem dynamics differ in:
Chronic disease states
Antibiotic-treated individuals
Elderly/immunocompromised populations
I prefer the trifecta approach over blind faith that all of the above assumptions are true. Blind faith is reasonable when you have no better data — the odds are that it will be better than no data.
Illustration of a different pair
With our special monotonic transformation: R2 =0.23
This is a thought experiment transformed into an implementation for people to experiment with.
In doing educational reviews of a variety of samples, I came across a person whose progressed had slowed. In trying to understand why [The ME/CFS Quest for Health], I looked at metabolites level between his current sample and previous sample. To my surprise, the highest ones (highest percentile) had barely budgeted.
I looked at the prior Dec 24 sample and compare the KEGG Compounds to the current sample starting with the highest percentile ones:
While the bacteria changed, the extreme metabolites remained high but with a few reducing. There is a potential to generate suggestions based on these KEGG compounds — a little messy and definitely pushing inference into new turf.
An Idea
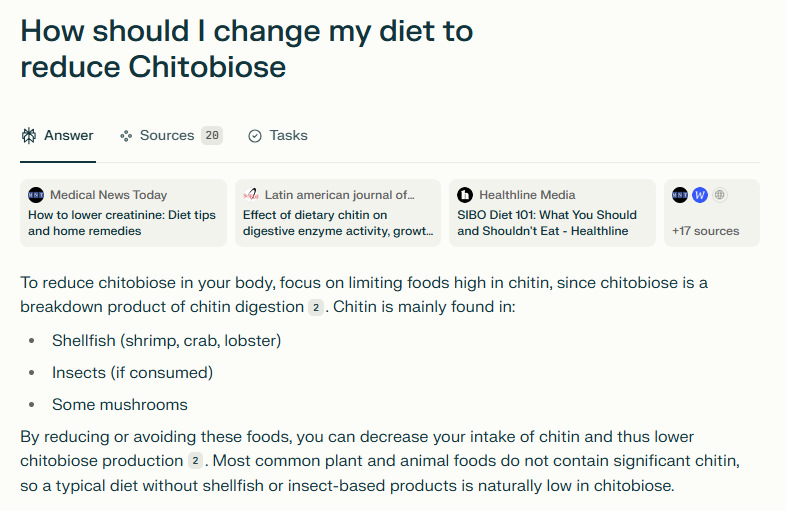
I asked Perplexity.ai on how to reduce a few. A typical response is shown below
On MicrobiomePrescription.com, the suggestion algorithm works solely off the bacteria that is reported by the microbiome test. This is done by using facts harvested from US National Library of Medicine studies. There are no (or likely extremely few) studies dealing with diet and metabolites.
The key phrase is reported by. We know that reporting is not standardized and often using only 16s.
Idea!
Current logic on MicrobiomePrescription.com is bacteria => suggestion impact. What if we add another approach: metabolite => normalized bacteria distribution => suggestions. We want this to have less randomness than 16s. The folks at PrecisionBiome.Eu shared 1000 shotgun results from healthy individuals with me so I could construct a normalized bacteria distribution model. From this model, I computed metabolites using data from KEGG: Kyoto Encyclopedia of Genes and Genomes and ended up with a facts table consisting of:
Metabolite
Suggestion / Modifier
Estimated Impact
The metabolite is identified by KEGG ID.
Implementation
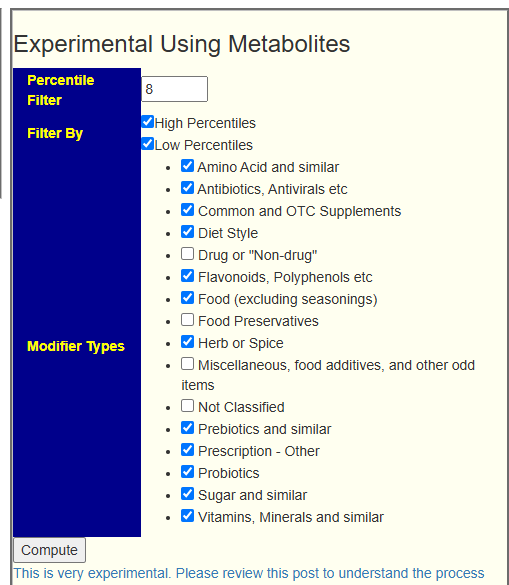
Since the microbiome and its metabolites are very interconnected and interact with each other. I decided that looking at the top and bottom 5-10%ile (i.e. those with a percentile ranking of 90-95%ile or higher, a percentile of 10-5%ile or lower) was a reasonable approach. There is a little trust that the central limit theorem will generate reasonable results and allow metagenomics to be directly used for getting suggestions.
On the [Research Features] tab, this panel has been added:
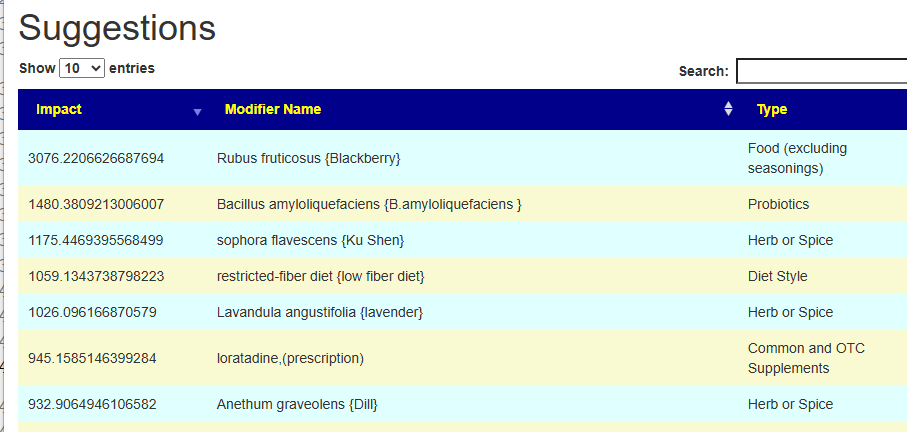
This produces a report listing the Metabolites targeted (High and/or Low) and then Suggestions
Observation
To me, what I found very interesting is that there are a few that are very high in impact with rapid drop off. This means there are only a few critical items to add to the general bacteria-based suggestions.
Hello, I’m sorry to message you privately, but I’m reaching out for help regarding my 15-year-old daughter, who has been homebound with ME/CFS for 2.5 years since contracting COVID in 2022. I came across your story on Facebook, and I felt truly inspired by how you managed to overcome ME/CFS by working with your microbiome. We are currently trying to follow a similar path.
We’ve recently done a Biomesight 16S test for her. As expected, it showed typical deficiencies, like a lack of Lactobacillus bacteria, along with an overgrowth of sulfate-reducing bacteria (possibly SIBO). Since we’re unsure how best to approach this dysbiosis, we sought the help of a microbiome specialist through Viola Sampson in the UK. She recommended lactulose, Lactobacillus reuteri, Lactobacillus rhamnosus, Lactobacillus plantarum, Bifidobacterium breve, along with Allicin and Goulds tincture from Australia. We’re just beginning this treatment, so it’s hard to say much about progress yet. We’ve started with Lactobacillus rhamnosus, plantarum, and breve, and she’s doing well with these so far.Honestly, I’m a bit concerned about these Lactobacillus bacteria because I read somewhere that all people with ME/CFS have some degree of lactic acidosis, so I’m worried that these probiotics might produce even more lactic acid. When I brought this up with my practitioner, she wasn’t aware of it.
I also uploaded a Biomesight test of my daughter to your Microbiome Prescription page, but I noticed that your site has somewhat opposite recommendations for her microbiome, such as advising against lactulose. To be honest, I’m struggling to navigate your page, and it’s a shame because I truly want to follow the recommendations accurately. I was hoping to identify which specific antibiotics or probiotics might be the best fit for my daughter’s case, but I’m not sure how to interpret that information from your site.
Currently, my daughter is mainly dealing with POTS (Postural Orthostatic Tachycardia), histamine intolerance, chronic fatigue, anxiety and panic attacks, and digestive issues. She’s become highly sensitive to various foods and medications, and it all points towards dysautonomia. Although she’s taking many supplements, she reacts to some, like iron supplements, which I suspect might be due to certain bacteria that feed on iron. She has many vitamin deficiencies, yet we can’t supplement effectively due to these reactions. It’s so difficult to manage.
I apologize for the long message, but I wanted to be as clear as possible about her situation. I’d be incredibly grateful if you could review her Microbiome Prescription and offer any insights on what stands out in her microbiome and where we might start. I’m also curious about any thoughts on the potential use of antibiotics or probiotics, as our microbiome practitioner is generally against antibiotics, though I know some people with ME/CFS have found success with a well-planned antibiotic approach.
Here, I am including the link to our microbiome analysis from Microbiome Prescription.
Analysis
First, disagreement between sites is well known and explained here: Why sites suggestions disagree on the same data. Microbiome Prescription tuned it’s advice by doing cross-validation for several conditions, for example: Cross Validation of AI Suggestions for Nonalcoholic Fatty Liver Disease. ME/CFS was the first explicit studies done. To the best of my knowledge, no other microbiome site has done cross-validations of their suggestions and been public in showing results.
Individual practitioners are hard to evaluate because they often find patterns that works for some people by trial and error. It is a rare practitioners that can provide documentation on their suggestions.
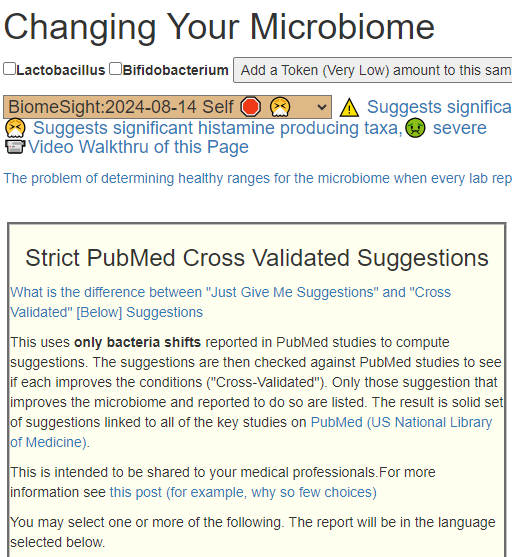
Quick boot strap
Long COVID is one condition that has a built in cross validation list of suggestions. This is on [Old Ui] / [Changing Microbiome]. POTS is not currently on the list because of insufficient studies.
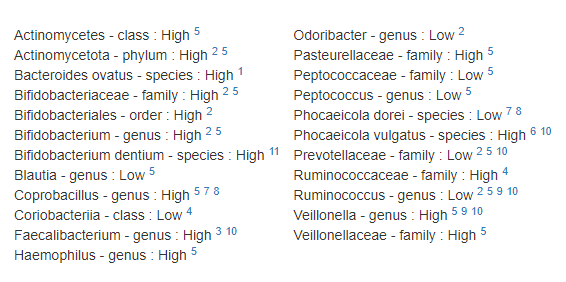
This identified the following bacteria as being probable according to the published literature. The number of cross reference numbers after each item, indicate the number of studies For example Ruminococcus – genus : Low was reported in 4 studies.
The suggestions (based on microbiome shifts cross reference with substance that improved ME/CFS from studies are below. The number of cross reference numbers after each item, indicate the number of studies – as above. This leads to the best suggestions being the ones with the most cross reference. Thus:
Magnesium supplements – 6 studies
Vitamin B9 – 6 studies
Coenzyme Q10 – 6 studies
Far infrared Sauna – 4 studies — as a personal note, we purchased a small one at Costco and use it regularly as preventative.
Vitamin B1 – 3 studies
Omega-3 – 3 studies
Ribose – 3 studies
licorice – 3 studies — we usually use Spezzatina and just suck on them
carnitine Amino Acid – 3 studies
Melatonin – 3 studies
Selenium supplement – 3 studies
This is a significant list and I noticed that none of these were suggested by Viola Sampson despite published literature saying they help.
My suggestion would be to add one of these every three days, noting any changes that results. For dosages see Dosages for Supplements, start low and work up. The above will take a little over a month. All of these items can be taken continuously and together.
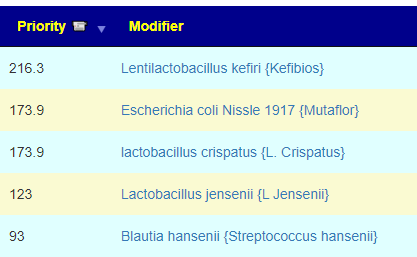
Probiotics
Probiotics are a popular “cure-all” which in some cases help and in other cases hurt. For example, lactobacillus probiotics often will increase brain fog.
Looking at probiotic with positive values, most are actually hard to obtain. For example Kefibios is only sold in Italy. Mutaflor in only a few countries. Of the choices, I would try Mutaflor after adding in the items above — but be warned, it may trigger severe die-off.
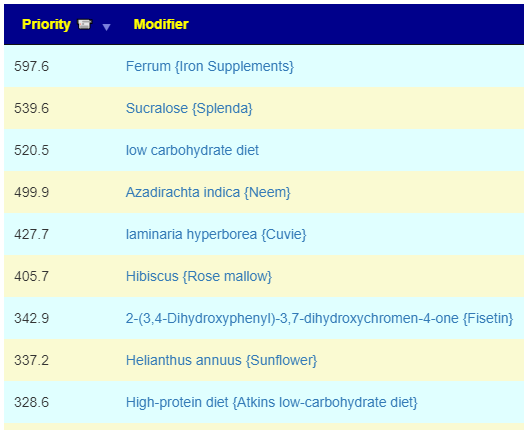
Top items
The list below are other things that likely have never been studied for ME/CFS but should have significant impact on the bacteria shifts.
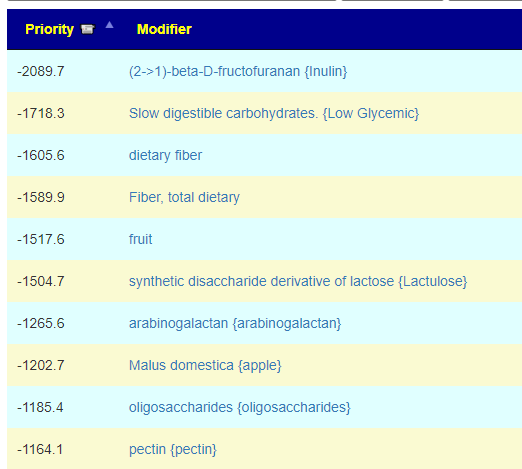
On the other side, the following should be avoided:
Food Site
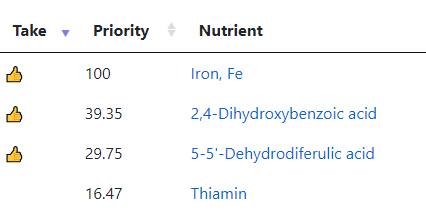
Going to https://food.microbiomeprescription.com/ and entering your login token will show the nutrients computed to help most. Iron supplements or food high in iron is at the top; for example thyme, basil, and my favorite Caterpillar, roasted ;-). Both herbs have positive recommendations.
The second one is found in cranberry (a suitable seasonal food) and raw Olive. The third one is found in maize, rye and Hard wheat, semolina. HOWEVER, none of these are recommended in the list of suggestions. I usually cross reference the two for safety.
Next Steps
I would continue with additional suggestions (1 and 2 studies) at the same pace. Two weeks after the last one was added, do another microbiome test (same firm of course) and get back to me for a follow up analysis if needed.
Postscript and Reminder
As a statistician with relevant degrees and professional memberships, I present data and statistical models for evaluation by medical professionals. I am not a licensed medical practitioner and must adhere to strict laws regarding the appearance of practicing medicine. My work focuses on academic models and scientific language, particularly statistics. I cannot provide direct medical advice or tell individuals what to take or avoid.My analyses aim to inform about items that statistically show better odds of improving the microbiome. All suggestions should be reviewed by a qualified medical professional before implementation. The information provided describes my logic and thinking and is not intended as personal medical advice. Always consult with your knowledgeable healthcare provider.
Implementation Strategies
Rotate bacteria inhibitors (antibiotics, herbs, probiotics) every 1-2 weeks
Some herbs/spices are compatible with probiotics (e.g., Wormwood with Bifidobacteria)
Verify dosages against reliable sources or research studies, not commercial product labels. This Dosages page may help.
Individual health conditions may make some suggestions inappropriate. Mind Mood Microbes outlines some of what her consultation service considers: A comprehensive medical assessment should consider:
Terrain-related data
Signs of low stomach acid, pancreatic function, bile production, etc.
Detailed health history
Specific symptom characteristics (e.g., type and location of bloating)
A reader messaged me about some issues she was having
Hi, could I just have a quick question? I read in the Gut Health group on Facebook that you wrote that if there is too much, for example, lactobacillus, it can cause neurological problems. I suffer from anxiety and depression and was recommended a transplant of intestinal microflora, which made the condition 100 times worse and since then I can’t get out of it and the doctors don’t know what to do with it. I’m still trying to treat dysbiosis, but now I don’t know if the problem is one of the good bacteria? Thank you very much.
yes, I have a biomesight and a GI map, there is an overgrowth of Prevotela, Streptococus, Enterobacter and Citrobacter and a little bifido and lacto. I have yellow stools after the transplant, if I don’t take probiotics. But it seems that nothing works, diet, antimicrobials, probiotics, enemas with probiotics, prebiotics, nothing helps
Initial Comments
This person is not in the US. She lives in a place where Fecal Matter Transplants is allowed for many conditions than the US (where it is only authorized for Clostridioides difficile –after everything else has failed). I view FMT as Russian roulette hoping that a silver ballet will happen to end up in the cylinder. IMHO, before a FMT is done we need at least two shotgun microbiome tests done. One for each candidate donor and one for the recipient. These need to be carefully reviewed by a third party who is very well informed on the microbiome. Only the best donor will be used. After the FMT, monthly shotgun reports of the recipient microbiome should be done for at least 6 months.
Analysis
The first step is to look at predicted symptoms, most are neurological, with the two reported symptoms sitting high up the list.
Comorbid: High Anxiety – [66.6%]
General: Depression – [64.1%]
I marked all of the items with depression and anxiety and then asked for suggestions. The top items are shown below,
The failure to understand that all probiotics are not created equal is a common problem. Often I have heard “I tried probiotics and it did not work”. That is not surprising because often they are sold with dozen of species in one bottle — “because the more species you have, the better your sales will be” from manufacturers and influencers.
You need to get specific species and ideally recently manufactured. A bottle of probiotics stored in an unrefrigerated warehouse for 12 months may have very few viable bacteria left. When they get to a retail store, they may be put into a refrigerator — but that is too late.
Where do I get the probiotics?
I prefer single species — and where I get mine?
Single species with (almost) no fillers. There are precisely three sources that I use:
Maple Life Science™: No strains yet, but shipments usually have manufactured date within 4 weeks of arrival (i.e. FRESH). Contains FOS
Bulk Probiotics: US based Newbie — but has some species not available at the other two sites. No other ingredients just the bacteria. Specifically, Lactobacillus Jensenii that has great potential for Crohn’s disease.
NOTE: none of these sell though retail outlets. This keeps their costs down and their product fresh.
Another Alternative to get Suggestions
On the old UI we have this section and we have enough studies for Depression show up.
With this sample, we have the following bacteria matches against published studies (with links to the studies).
This results in the suggestions below. Each suggestion has also been reported in studies to help depression. This means that the odds of them working is pretty good.
Treatment Suggestions for
This report is for Reader using this sample BiomeSight:2022-10-25 Self 🛑 . It uses their reported medical conditions, microbiome sample, US National Library of Medicine, and a fuzzy logic expert system to compute recommendations balancing study reliability and contraindications. These suggestions should always be reviewed by a medical professional before starting.
NOTA BENE: This is working solely from published studies. Other suggestions algorithms are available on Microbiome Prescription. The URL above may be sent to your MD if you wish to share it.
The reported condition(s) are
This person has a significant amount of bacteria known to form biofilms
Substances with a 🦠 are reported to reduce biofilms. See for studies.
Depression – Depressive Disorder
Omega-3 Fatty Acids: Some studies suggest that omega-3 supplements, particularly those rich in EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid), might have modest benefits as adjuncts to traditional treatments for depression. Omega-3s are essential for brain health, and they may have some mood-stabilizing properties.
Vitamin D: Low levels of vitamin D have been associated with depression. While the exact relationship is complex and not fully understood, maintaining adequate vitamin D levels through supplements or exposure to sunlight may support overall mental health.
B Vitamins: Some B vitamins, such as B6, B9 (folate), and B12, are involved in neurotransmitter synthesis and may have a role in mood regulation. Folate deficiency, in particular, has been linked to depressive symptoms.
Probiotics: The gut-brain connection has led to studies exploring the potential impact of probiotics on mental health. Research suggests that gut health may influence mood, and some studies propose that certain probiotics might have a modest effect on reducing depressive symptoms. However, more research is needed to determine specific strains, dosages, and their impact on depression.
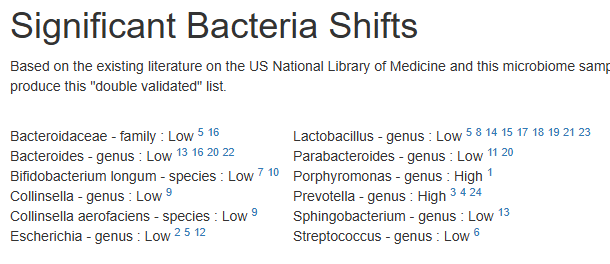
Significant Bacteria Shifts
Based on the existing literature on the US National Library of Medicine and this microbiome sample, we have the following matches for bacteria shifts. There is a growing body of literature finding that the effectiveness of interventions depends on the existing microbiome. We filter by documented interventions that helps some with this condition and suggestions based on this person’s specific microbiome to produce this “double validated” list.
Bacteroidaceae – family : Low 516 Bacteroides – genus : Low 13162022 Bifidobacterium longum – species : Low 710 Collinsella – genus : Low 9 Collinsella aerofaciens – species : Low 9 Escherichia – genus : Low 2512
Lactobacillus – genus : Low 5814151718192123 Parabacteroides – genus : Low 1120 Porphyromonas – genus : High 1 Prevotella – genus : High 3424 Sphingobacterium – genus : Low 13 Streptococcus – genus : Low 6
Cross Validated Suggestions
The following improves the bacteria identified above and also is reported in the literature of helping some people with this condition. Each is link to the source study.
There is no definitive right way to determine how to correct a dysbiosis. We just do not have enough studies. Above, you have two main approach (with some overlap of suggestions)
Working off the microbiome that are too high or too low.
We cross check probiotics suggestions using KEGG data
Working off the microbiome using only peer reviewed studies for one condition: depression.
This report should have high creditability with most medical types — because all of the evidence used to make the report is cited.
I have not been feeling so well lately (since the last 6 months). I would say that my symptoms has become worse. Earlier it has always felt as I have done some progress but the last 6 months it has been the opposite.
At the end of January I had my appendix removed. Since then I have felt even worse. Received some antibiotics while I was hospitalized. Earlier I got rid of my muscle and joint pain but it has come back and I have much bigger issues with my red nose and my body feels very stressed. Also feel very bloated.
A summary of my biggest issues:
Get the red nose (some form of rosacea).
Feel fatigued (both physically and mentally).
Feeling stressed.
Brain fog.
Bloated.
Lots of gas – I fart and burps a lot.
Issues with allergies
Muscle and joint pain
For the last 3 years I’ve been eating large amounts of rye and oats.
Around 150-200 gram of rye bread every day.
Around 70 gram of oats every day.
Been eating low fat, low protein and high carb (specially from rye, oats, apple juice and potatoes) because this diet seem to reduce my symptoms.
As soon as I start to eat high meat and high fat my symptoms get worse.
Quick Overview
I will continue with a table showing recent changes (see above for earlier values)
Criteria
3/30 2025
12/3 2024
9/2 2024
1/22 2024
2/22 2024
Lab Read Quality
7.6
9.8
9.1
7.9
9.7
GanzImmun
10
14
16
16
15
Outside Range from Lab Teletest
21
17
23
20
24
Outside Lab Range (+/- 1.96SD)
10
7
12
5
10
Outside Box-Plot-Whiskers
59
47
48
54
42
Outside Kaltoft-Moldrup
111
85
113
123
139
Bacteria Reported By Lab
718
689
600
511
666
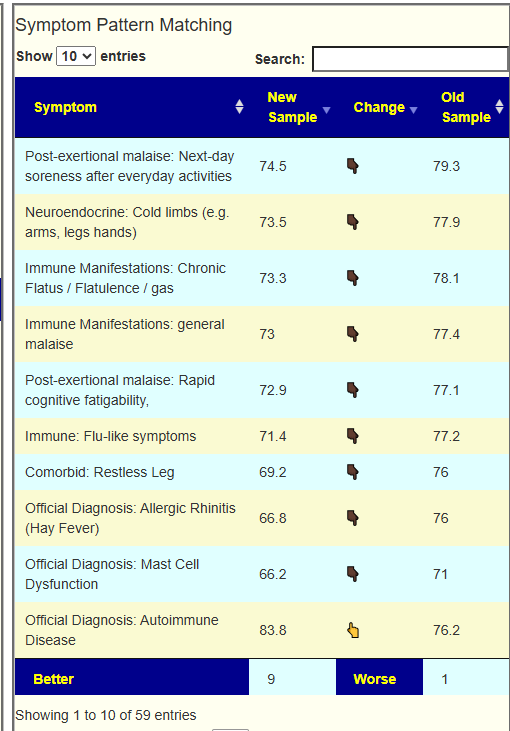
The most striking change was the 4% increased number of bacteria. Looking at Symptom Pattern Matching, we see significant improvement with 15% with significant improvement.
Current Takes Evaluation
I have put together a video trying to describe the complexities of shifting the microbiome. My own experience during a flare was “suggestion whiplash”, the suggestions from one test became avoid on the next and became suggestions on the next test. This is not what I was expecting and caused me to question the process — until I dug deeper and did some modelling. My understanding is in this video.
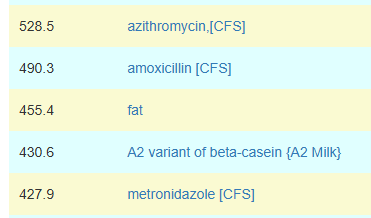
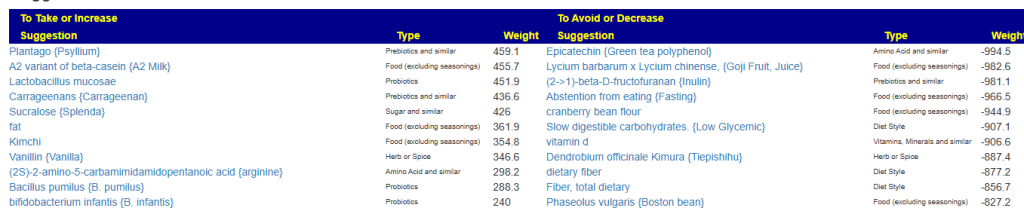
What he reports taking is below. I look at the suggestions and added the weight after each.
amoxicillin: +490.3
Noni -206.1
Propolis {Bee glue} +19.5
Dandelion + 155.3
allium sativum {garlic} -214.4
Parsley + 145.3
Grapefruit seed extract +168.8
mutaflor -78.8
Takes flipping to avoids is not unexpected. It does emphasis the need to do regular tests, especially when progress slows or reverses.
Building Suggestions
Since we have symptoms we use Beginner-Symptoms since it will focus on bacteria associated with symptoms present.
Looking at the Consensus report we see the top 3 antibiotics are all ones associated with CFS
The other items is interesting and would suggest Whole Milk (high Fat) (Yogurt) from A2 cows, I do not know if that is easily available in his country. I happen (as a recovered ME/CFS person) to have some to my daily morning porridge.
The suggestions above do not fit typical patterns that I have seen. I went back and did “just give me suggestions” in case the bacteria filtering by symptoms caused some odd twist. Results were similar as shown below.
One More Analysis
I looked at the prior Dec 24 sample and compare the KEGG Compounds to the current sample starting with the highest percentile ones:
While the bacteria changed, the extreme metabolites remained high but with a few reducing. There is a potential to generate suggestions based on these KEGG compounds — a little messy and definitely pushing inference into new turf.
I have decided to build an adjacent Suggestions Agent using metabolites ONLY. The microbiome is a very complex system and there is a possibility that the metabolites approach may work better. Stay tune!
Reconciliation of Recent Diet and Suggestions
During my own recovery, I had “whip-lash” between suggestions from one test until the next test. One test results had to take, the next result was the same items on the avoid list. This “pendulum” swinging back and forth may be happening here. My own response was to be “less religious” in keeping to the suggestions (i.e. “moderate compliance”) and retest after 6 weeks doing suggestions. The pendulum swing dampened down and lead to a full remission (with patience).
The 300 grams of fiber (Rye, Oats) should be reduced. If you can get a willing MD, then you may wish to rotate to a different antibiotic because of the risk of antibiotic resistance occurring.
And thus have the ability to compute the theoretical differences.
We also have these collections of studies which we can use by flipping things to be negative cognitive function:
Cognitive Function
Intelligence:Comprehension, Cognitive Ability
This resulted in 71 bacteria.
Results
For Sugar we had agreement between reported shift and cognitive issues for the following:
Bacillota
Bacteroides
Coprococcus
Desulfovibrio
Dorea
Escherichia coli
Faecalibacterium prausnitzii
Lachnospiraceae
Ruminococcus
Streptococcus
For Fat we had agreement between reported shift and cognitive issues for the following:
Bacillota
Bacteroidaceae
Bacteroides
Clostridium
Coprococcus
Coriobacteriaceae
Dorea
Faecalibacterium prausnitzii
Oscillospira
Phascolarctobacterium
Porphyromonadaceae
Ruminococcaceae
Ruminococcus
With Fat we had significantly more contrary shifts than with Sugar.
Bottom Line
Both High Fat and High Sugar in isolation appear to impact cognitive function. High Fat has the appearance of having less impact in isolation than high sugar. The following shifts seem to be common with these:








Recent Comments