Back Story
Back story: I have probably been infected by Covid since Nov 2021 and developed post Covid. In mid 2022 I got many urinary tract infections and took many antibiotics including ciprofloxacin. After another infection in End of 2022, I developed MECFS in early 2023 and was diagnosed with viral myocarditis in 2024. I have had problems with medication intolerances (bile issues: losartan, clopidogrel; pain, breathing: prednisolon, ketotifen, LDN) since 2023 and develop biliary pain every time I take them, which has persisted since the first time I took clopidogrel and is made worse again by the abovementioned medications. Everything has been checked many times with ultrasound, bloodwork, faecal examination, MRI and the like, including the pancreas. Nevertheless, the potential medical condition worries me. Can I counteract it?
It has been confirmed that I am dealing with chronic myopericarditis. Additionally, I have been suffering from constant gastritis since July 2024, which has caused ongoing issues. In the first half of 2024, I tried new medications. Ivabradine works well for me, and I continue to take it. However, I could not tolerate Prednisolone and Losartan due to side effects. Losartan, like Clopidogrel previously, caused biliary pain. Prednisolone led to severe muscle and joint pain, likely due to FQAD (following Ciprofloxacin use), which has had long-term effects on me.
Currently, my main symptoms are:
- Chronic gastritis, likely triggered by Pentoxifylline, turmeric, or possibly diet.
- Persistent biliary pain, worsened by fatty meals (extensively checked by gastroenterologists with examinations including bloodwork, MRI, ultrasound, and tests for the pancreas and gallbladder – all results were normal).
- Severe fatigue and lack of energy.
- Muscle pain. (feels like lactic acid. Tested after a lot of sugar/carbs on christmas)
- Persistent tiredness.
- Anxiety and nervous system overstimulation.
- Medication reactions (possibly MCAS).
- Reactions to carbohydrates/sugar, resulting in heart palpitations and autonomic nervous system overstimulation.
- Concentration difficulties.
- Angina Pectoris symptoms.
I am currently housebound and feel that I need to rebuild my stomach health to heal the gastritis and regain energy. Unfortunately, I had to take Pantoprazole, Gaviscon, and slippery elm for a long time due to the gastritis.
I have already purchased all the probiotics from your list and created a 4-week plan (attached) based on your PDF. However, I recently read your December 2024 post about the potential dangers of Lactobacillus, which has left me feeling uncertain.
Analysis
First, the lactobacillus probiotics issue is mainly a caution. There are lactobacillus probiotics that will produce significant amount of d-lactic acid that will worsen brain fogs etc. This is compounded by both species mis-identification issues on retail probiotics and that different strains of the same species may produce different compound. Avoiding lactobacillus is the safest (simplest) course for many.
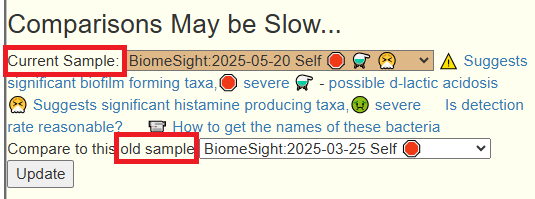
Chronic myopericarditis has no explicit literature on microbiome shifts. I suspect Heart Failure is the closest match for what I have gathered data on. My expertise is assembling “the facts” from studies on the microbiome and the mathematical application of these facts. So proceeding with my skill sets and available data, let us look at your data.
Quick Health Review
- Low bacteria leak from the Oral Cavity
- General Health Predictors has no concerns
- Mold ratio is higher – 82%ile than ideal (See Associations of observed home dampness and mold with the fungal and bacterial dust microbiomes .)
- MHI-A Ratio is very high – 96%ile. This is an indicator of post-antibiotic dysbiosis — which is very much in agreement with your back story.
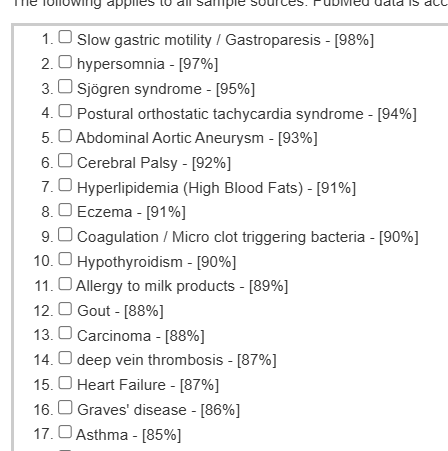
- No medical conditions pattern matched your microbiome
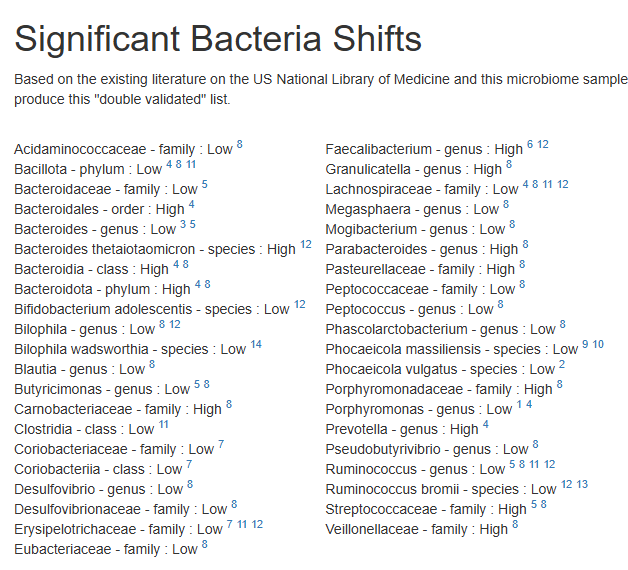
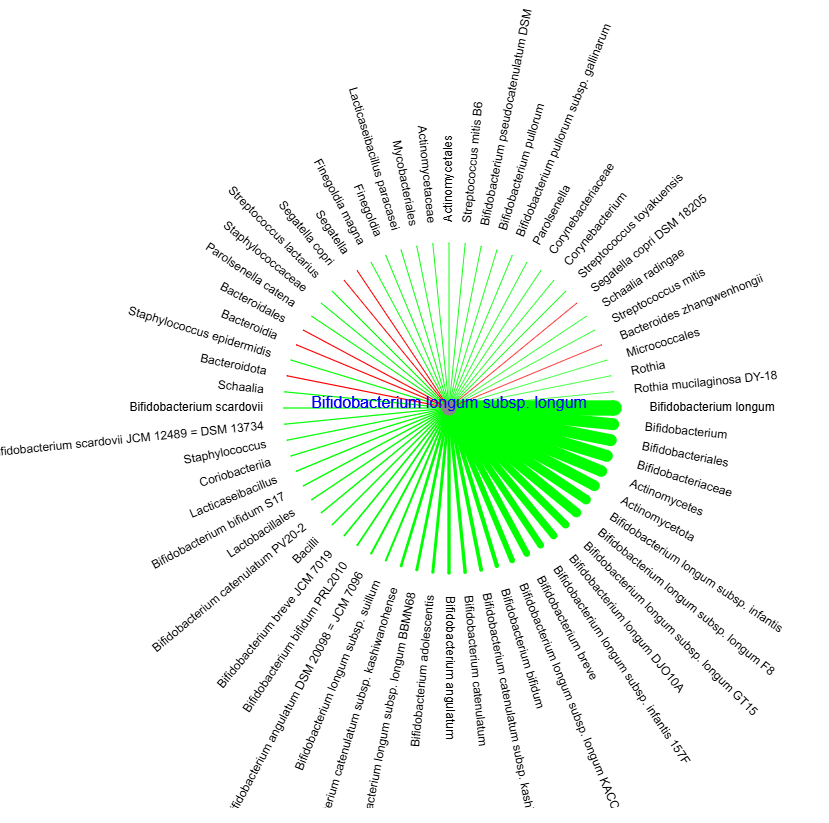
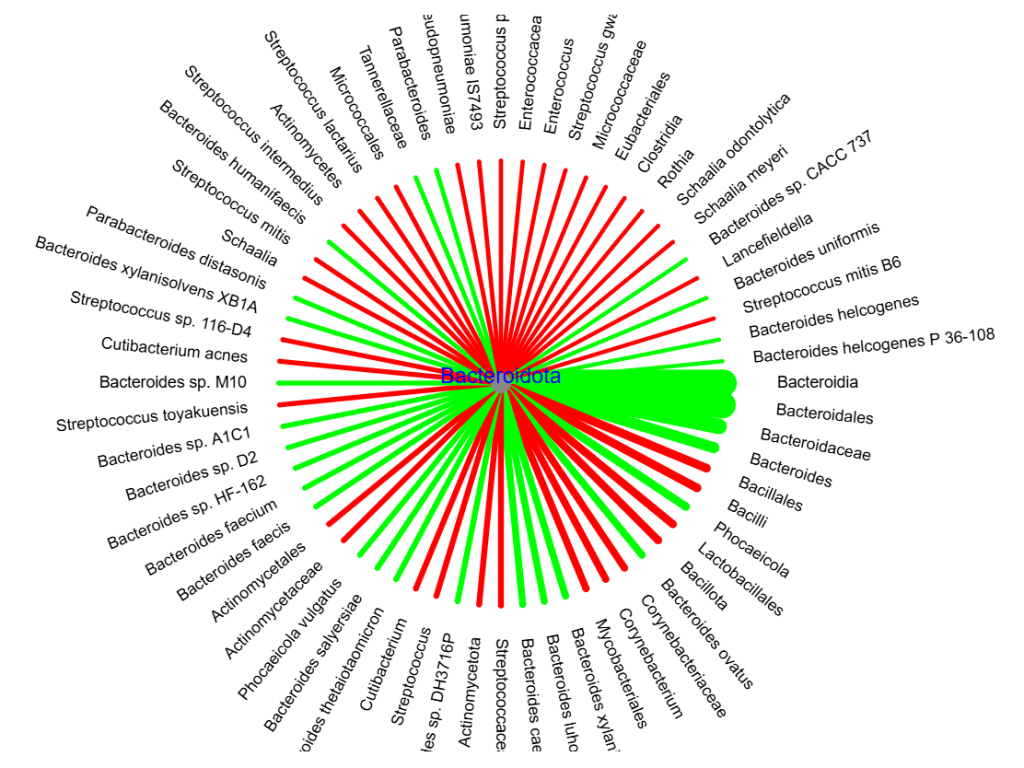
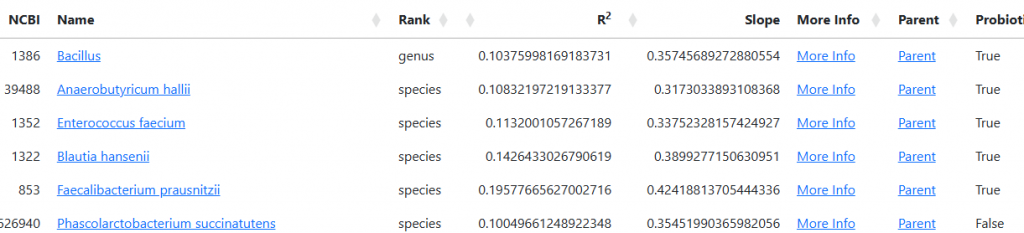
- Two bacteria are of possible concern: Faecalibacterium and Bacteroides uniformis
Most of the other measures are questionable in their usefulness given your back story.
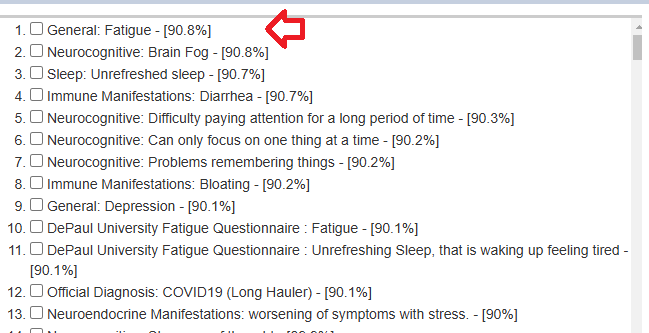
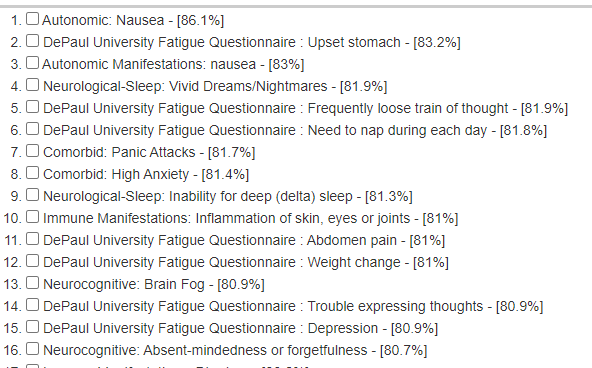
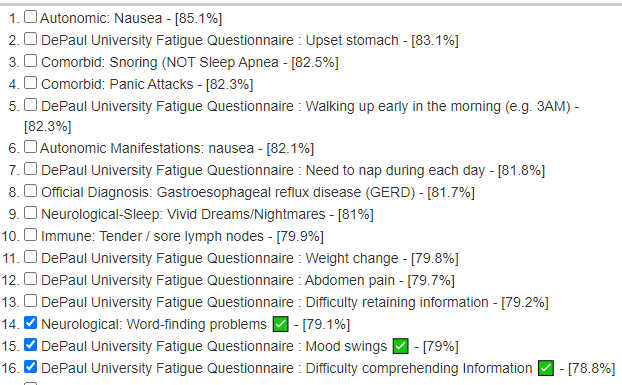
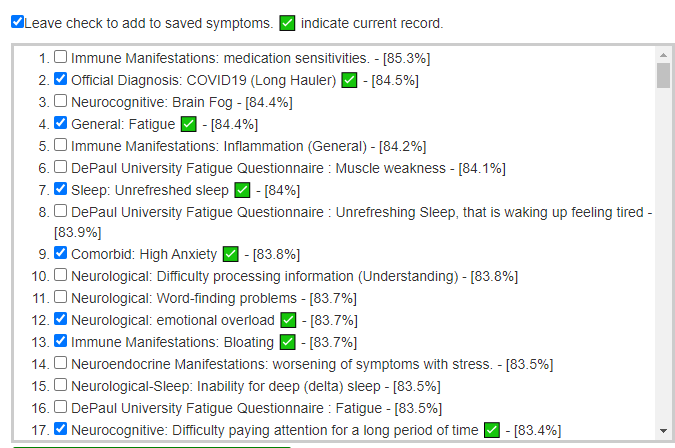
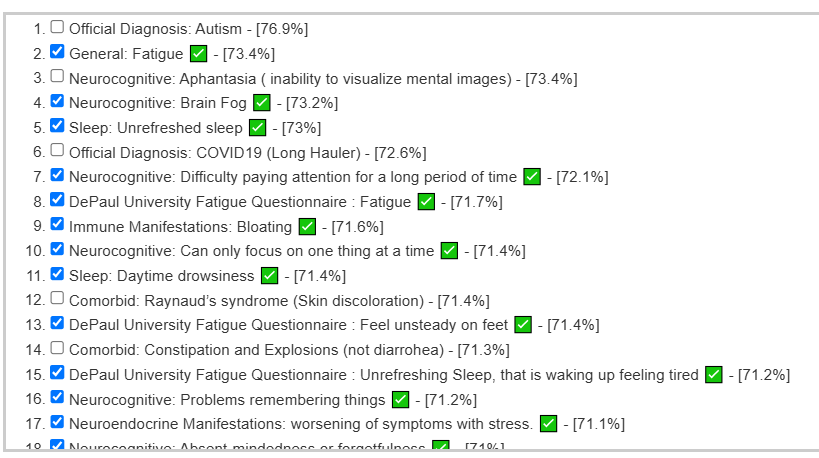
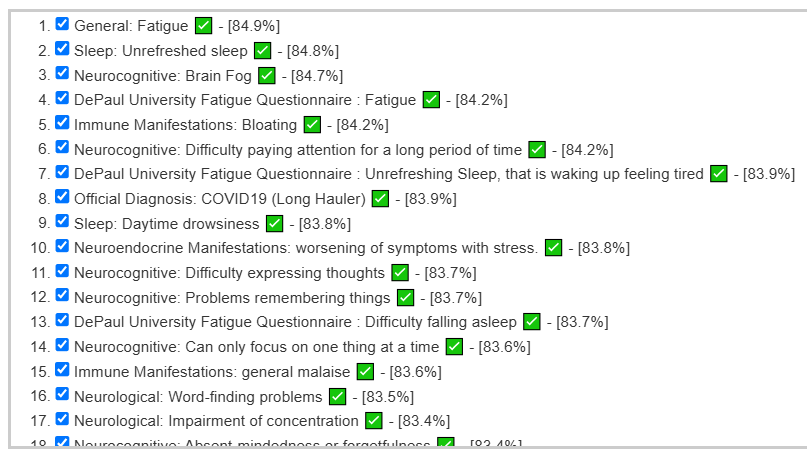
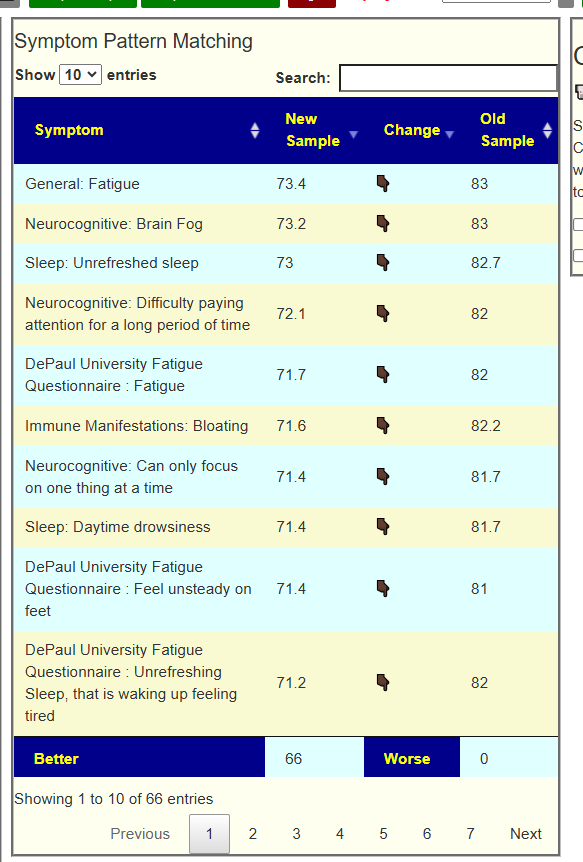
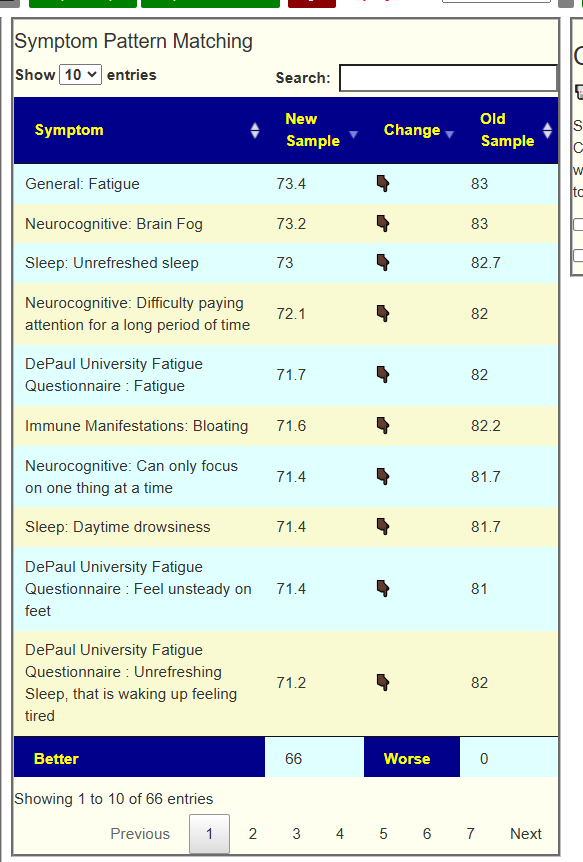
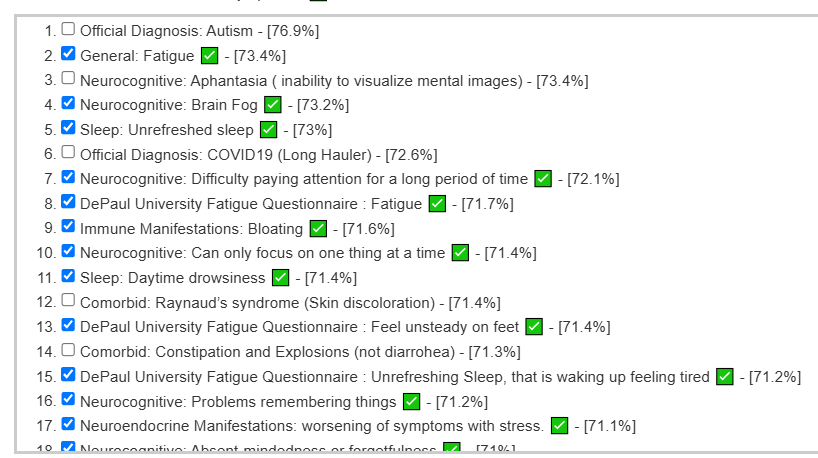
Predicted Symptoms that matches back story
A few of the clear matches are below.
- General: Fatigue – [88.5%]
- Neurocognitive: Brain Fog – [88.2%]
- Official Diagnosis: COVID19 (Long Hauler) – [87.6%]
- Comorbid: Histamine or Mast Cell issues – [86.9%]
- DePaul University Fatigue Questionnaire : Anxiety/tension – [86.5%]
- Comorbid: High Anxiety – [86.2%]
- Immune: Sensitivity to smell/food/medication/chemicals – [86%]
- DePaul University Fatigue Questionnaire : Abdomen pain – [86%]
- Autonomic Manifestations: palpitations – [85.9%]
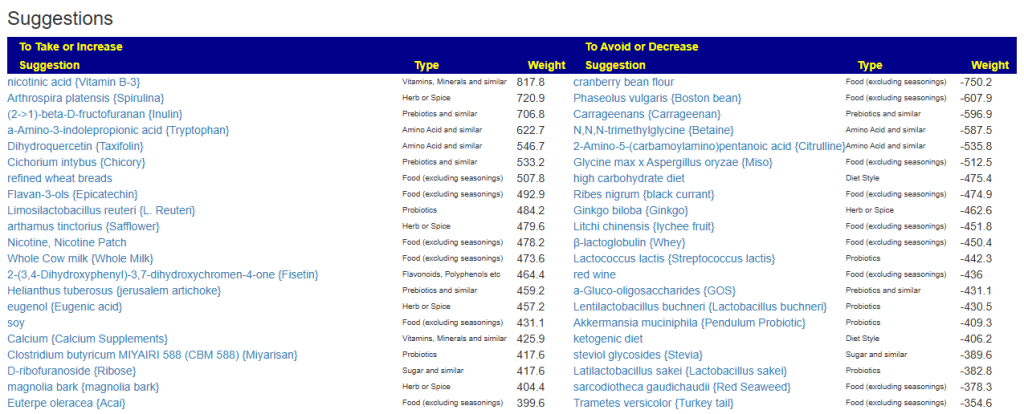
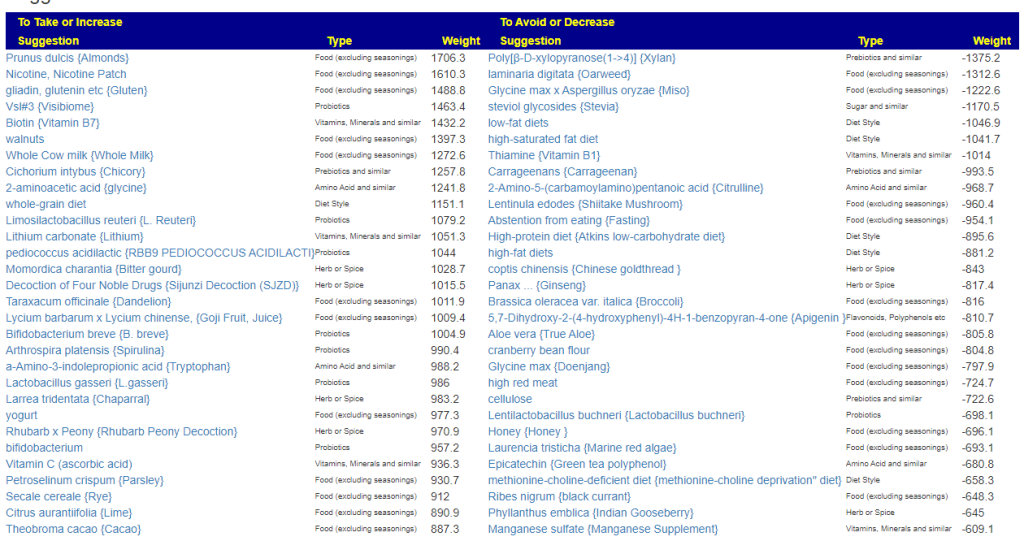
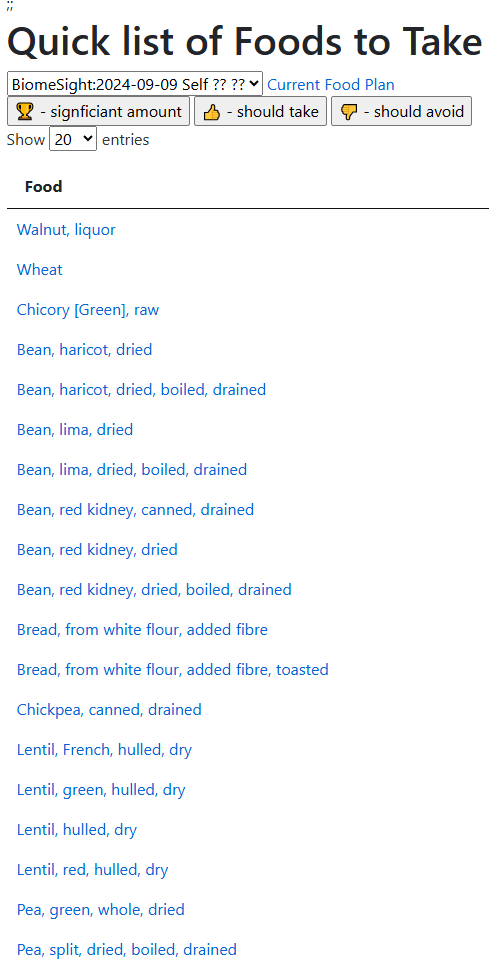
These are checked and use to generate suggestions. Because of the existing use of prescription drugs, those are included in the suggestions.
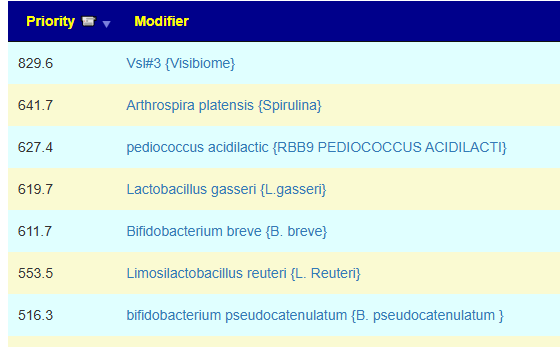
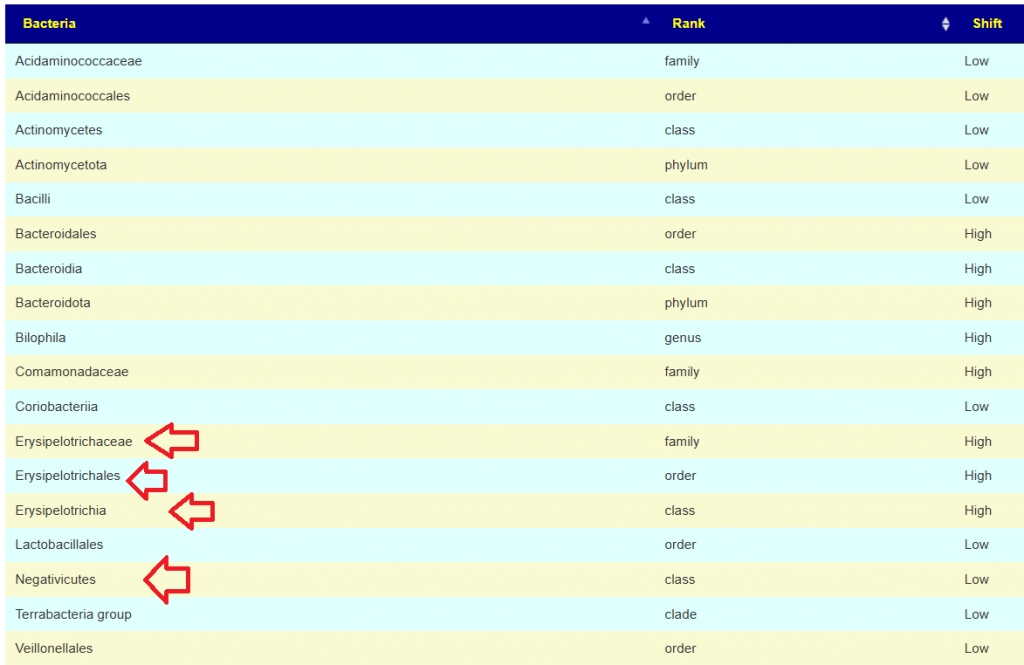
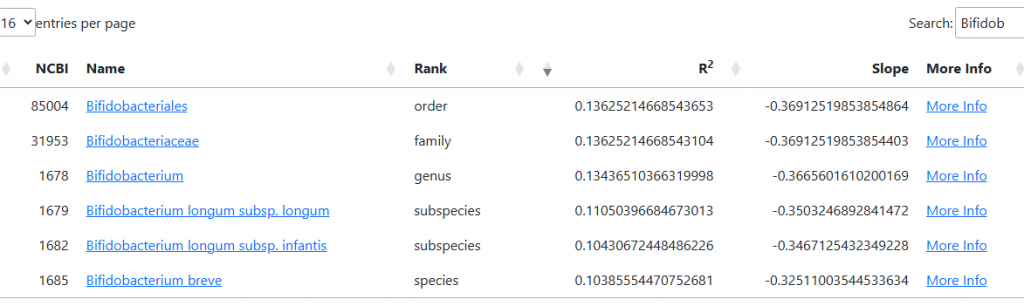
Some 66 bacteria were picked from the matching patterns

Checking substances tried or taking (where we have information). The goal is to see what helps or hurts the microbiome. I have switched to % of highest or lowest value below
- ciprofloxacinm, LDN, around 61 ( -20%)
- losartan, clopidogrel, ketotifen, clopidogrel, Ivabradine, Prednisolone, Losartan, Gaviscon, Pantoprazole – no listed (i.e. no effect on microbiome or balanced effect)
Alternatives to clopidogrel likely include:
- aspirin, resveratrol: -30% which are likely worse choices.
- slippery elm: -30%
- Ginkgo biloba {Ginkgo}: +80%
So no major hurt and no apparent better with the exception of these antibiotics that are round +30% positive (lincosamide, kanamycin, paromomycin, ofloxacin) and a potential discussion point with your MD.
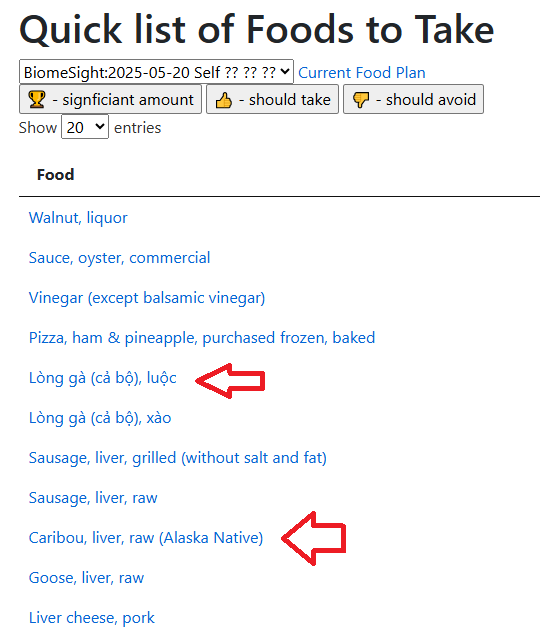
Prescription items high on benefits are:
- proton-pump inhibitors (prescription): +100%
- metformin (prescription): +85%
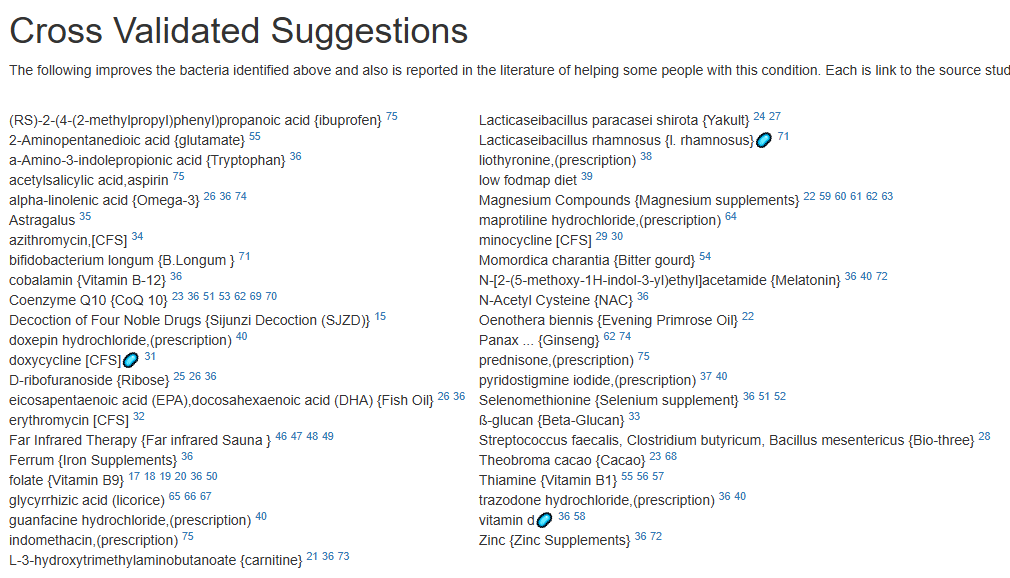
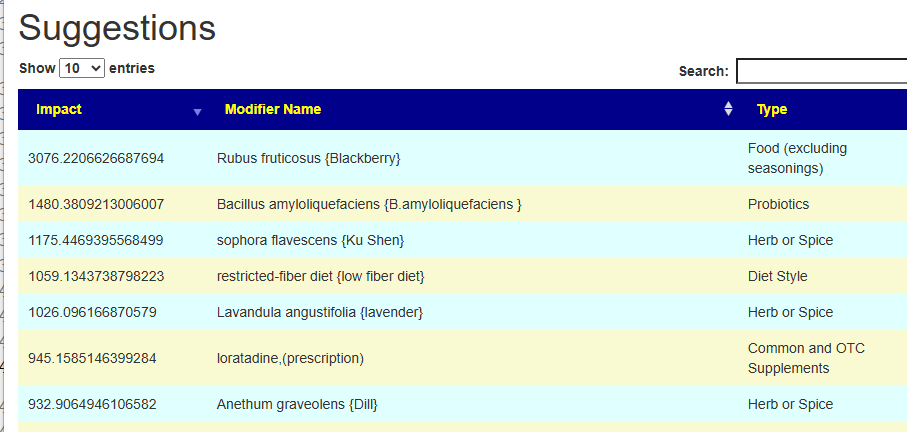
Cross-Validated Suggestions
I went to the old UI to see what shows up with cross validation.
The algorithm is slightly different (no one knows the right answer — and I have implemented multiple “reasonable” approaches across the site. We see that with this alternative algorithm, the slightly negative for LDN above is now positive. Similarly with Prednisolone.
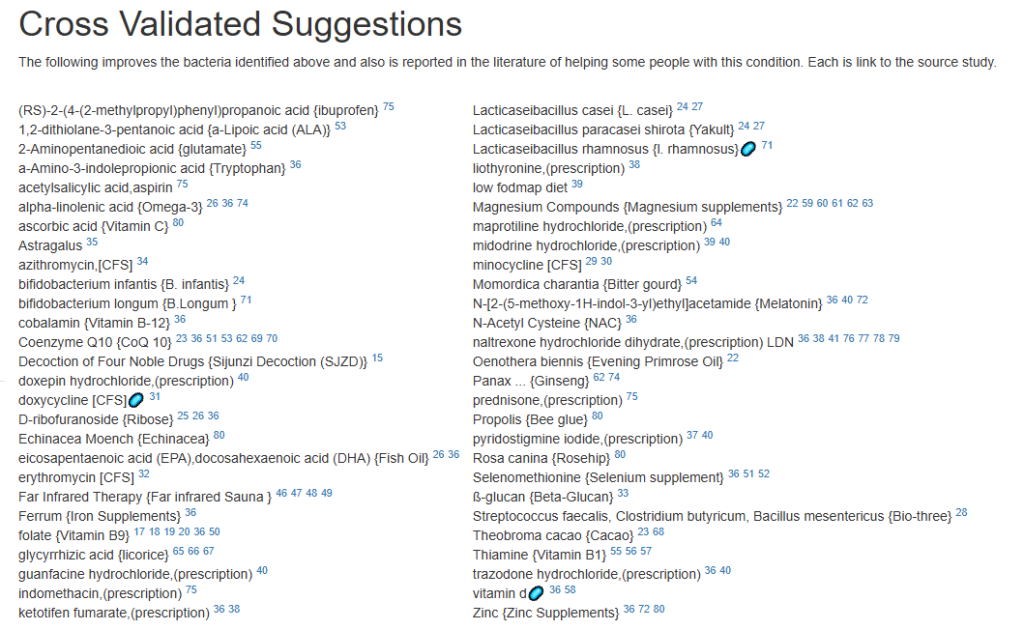
The preferred pattern is to always discuss with your MD, try items in isolation (i.e. one new item a week) and taking notes for response.
Postscript and Reminder
As a statistician with relevant degrees and professional memberships, I present data and statistical models for evaluation by medical professionals. I am not a licensed medical practitioner and must adhere to strict laws regarding the appearance of practicing medicine. My work focuses on academic models and scientific language, particularly statistics. I cannot provide direct medical advice or tell individuals what to take or avoid.My analyses aim to inform about items that statistically show better odds of improving the microbiome. All suggestions should be reviewed by a qualified medical professional before implementation. The information provided describes my logic and thinking and is not intended as personal medical advice. Always consult with your knowledgeable healthcare provider.
Implementation Strategies
- Rotate bacteria inhibitors (antibiotics, herbs, probiotics) every 1-2 weeks
- Some herbs/spices are compatible with probiotics (e.g., Wormwood with Bifidobacteria)
- Verify dosages against reliable sources or research studies, not commercial product labels. This Dosages page may help.
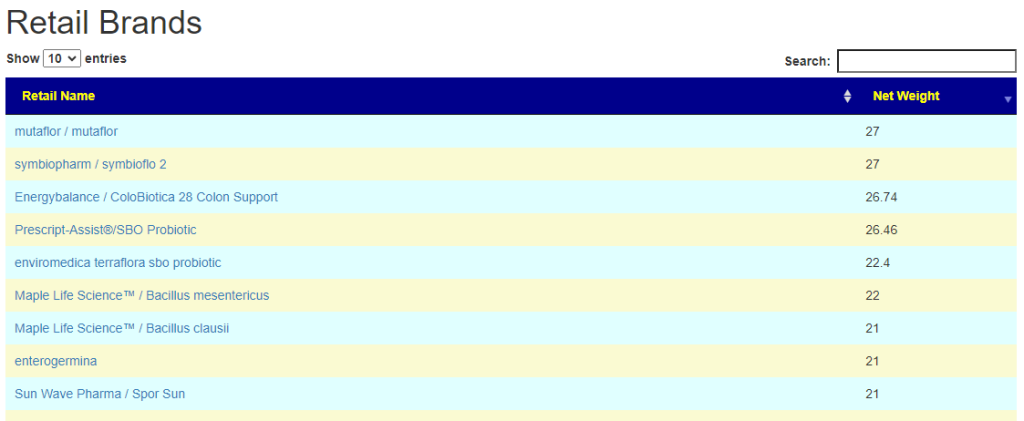
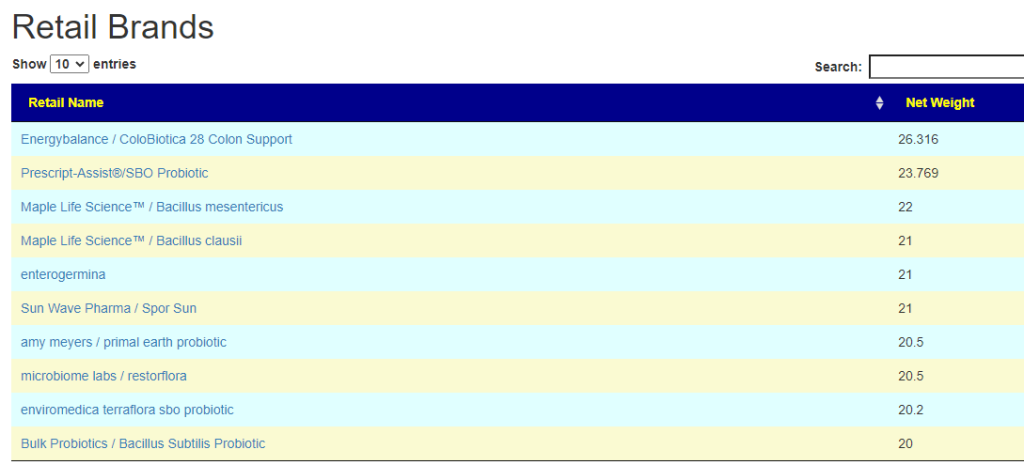
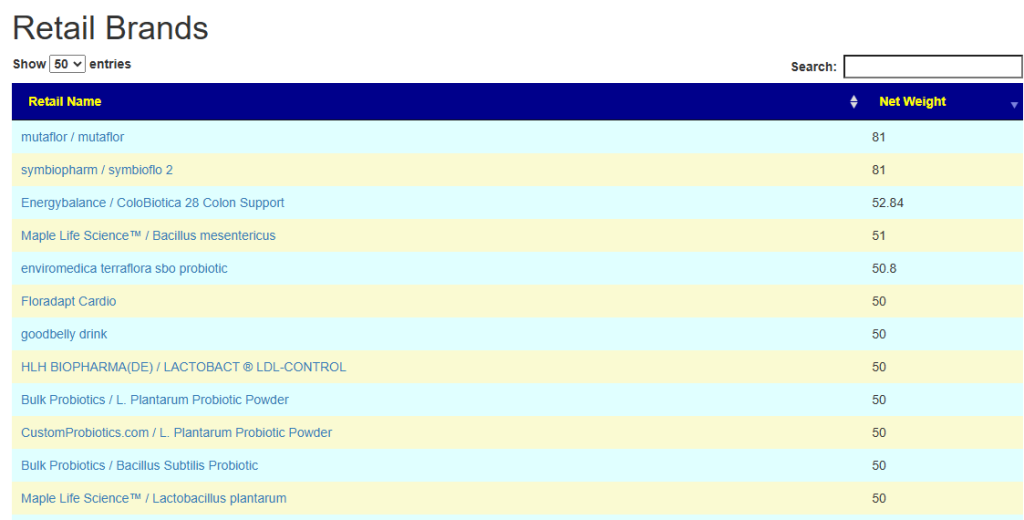
- There are 3 suppliers of probiotics that I prefer: Custom Probiotics , Maple Life Science™, Bulk Probiotics: see Probiotics post for why






Recent Comments