Using novel technics for my earlier postBacteria Shifts Seen in Long COVID caused me to look at it’s sibling: Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Since we have a much large sample size, we can get more rigorous and be lab specific (see The taxonomy nightmare before Christmas…). The result are the three tables below. The criteria for shift was a difference of 4 percentile or more.
It means that the bacteria count may be a little bit of a red herring. It is the frequency of detection that may be a better criteria for what is significant.
To put this in human terms, for a political movement, looking at the bank account may not be the best way of detecting if it is significant; it is the number of different types of people that turns up at meetings!
The mathematics and number crunching becomes more complex… but we are dealing with a complex system. For example, if you are using uBiome and many of the following was detected, then the odds of having ME/CFS is significant. It suggests a different criteria for selecting bacteria to generate suggestions.
Planococcaceae
Bacteroides gallinarum
Oscillatoriales
Aerococcaceae
Phocaeicola coprocola
Turicibacter sanguinis
Returning to Long COVID
Below is NOT the amount of bacteria, it is the frequency that these bacteria were detected in the samples. In other words, there is a group of bacteria that blooms – they show up more frequently, not necessarily in larger numbers, just there — trouble makers!
Bacteria Identified in Long COVID
Ombre ME/CFS
Biomesight ME/CFS
Ubiome ME/CFS
Micrococcaceae
More
More
More
Peptostreptococcaceae
More
More
More
Butyricimonas virosa
More
More
More
Sarcina
More
More
More
Enterobacter
More
More
More
Lactobacillaceae
More
More
More
Coriobacteriia
More
More
More
Slackia faecicanis
More
More
Rhodovibrionaceae
More
More
Blautia wexlerae
More
More
Salinicoccus luteus
More
More
Staphylococcaceae
More
More
Bifidobacteriales
More
More
Holdemanella biformis
More
More
Coriobacteriales
More
More
Holdemanella
More
More
Eubacteriales incertae sedis
More
More
Fusobacteriia
More
More
This analysis shows a very similar pattern in the microbiome between Long COVID and ME/CFS.
The back story for this person is long and detailed — with a massive number of tests and conditions done! This is a much shorten version
Back Story
Male, 40yrs of age. Very physically active and successful engineer & businessman prior to illness onset 7 years ago at 33yrs of age.
Illness onset summary:
July 2014 I had bad flu symptoms: very fatigued and bad cough, which took a couple of months to seemly recover from, albeit still had bouts of mild fatigue and random mild cough.
September 2014 I moved into a moldy / water damage building.
October 2014 I had the flu again. Did seem to recover.
2015 On-going random fatigue and insomnia, which is persistent to today.
Sometime during this 2014/2015 period whilst living in moldy house I had a circular red rash (similar to erythema migrans) on my forearm indicating insect bite mark. Took 2 weeks to go away. Did not take photo and did not notice any symptoms during this time. I had not travelled anywhere during this time.
I have for +7yrs managed my symptoms by predominately eating carnivore diet, regular fasts, and having daily water enemas as it is the only way I can pass stool. Start of 2020 I had to stop working all together due to extreme fatigue and brain fog. I have dedicated 100% of my limited energy to my treatment ever since.
I have seen over 17 Health Professionals of various specialities, with numerous treatments with no real improvement. First four years was predominately about treating the gut (which is still my main symptom) with various SIBO treatments, including herbs (e.g. oregano), antibiotics (Erythromycin, Rifaximin & Vancomycin), antifungals (nystatin) and seven Faecal Matter Transplants (FMT), with no success. Have had multiple endoscopy and colonoscopies with no major findings other than removal of some polyps, and negative to Whipple’s PCR albeit +ve antibodies. Many stool samples with no detected parasites.
End of 2019 I identified that Lyme and/or mycotoxin (mold) toxicity could be the cause, and in 2020 was diagnosed with Chronic Inflammatory Response Syndrome (CIRS) from mycotoxin toxicity due to various test results, and subsequently also Mast Cell Activation Syndrome (MCAS) and Cell Danger Response (CDR). I have been treating this for +24 months via various treatments e.g. binders and antifungles, although can’t tolerate most e.g. CSM, nystatin, Amphotericin B, Itranconazole. I did see some initial improvement with charcoal & bentonite which I occasionally still take when herxing, but no noteworthy improvements in symptoms.
My Lyme antibody test results are equivocal with only some IgM +ve results. I did initially respond well to doxycycline but these improvements only lasted 2 weeks. After using it on and off for other a year I can’t tolerate it for longer than 5 days or so. Cannot tolerate azithromycin and erythromycin cause severe large bowel pain, as do many other herbs e.g. Cowden protocol.
Often my bowel pain gets bad enough that pain killers are not enough so I go back on doxy as that has been the only thing helps, but I can’t stay on doxy as it makes me feel horrible after eating (which is when I take it).
Multiple hair analysis indicate that mercury distribution could be an issue, and I have had negative cognitive symptoms to single thiol chelators i.e. chlorella and EDTA. EDTA does make me feel like I’m loosing my mind. Recently start 5mg dosage of OSR which does make me more fatigued and worsen digestion.
My condition only seems to get worse and am not able to tolerate any treatments anymore.
Reinvestigating my gut biome I have taken Biomesight stool sample (whilst taking doxycycline) to see if there is any pre/probiotics I can take that will help, and considering Phage therapy and or retrying FMT treatment.
Note I’ve tried many prebiotics all of which have exacerbated my symptoms e.g. bloating, toxicity, bowel pain fatigue, brain fog etc as do most plants, hence carnivore diet, and many probiotics most of which make no difference or make me very fatigued e.g. Megaspore (presumably due to histamine).
Analysis
See the YouTube for more information and walk thru.
Using Health Analysis Page
Health Status – 2 Healthy, 9 Unhealthy
Jason Hawrelak – at 56%ile , significant issues
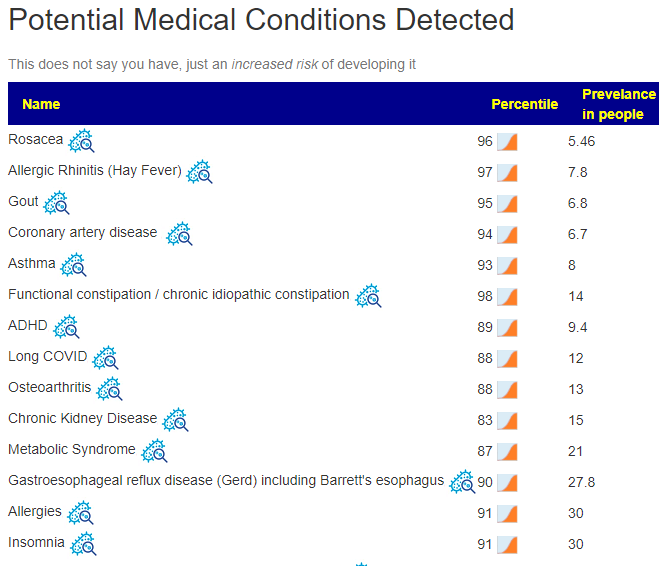
Potential Medical Conditions Detected – a massive list!!!
I am finding that this is a friendly start point because we have multiple logics available to determine them (which, of course, can result in disagreement). The list is very close to the common pattern seen with ME/CFS patients:
The lists are effectively identical! One list was obtain solely by looking at the DNA of the bacteria in your sample and the DNA of the bacteria in the probiotics. The last list was generated from clinical trails reporting shifts of bacteria from taking probiotics. It appears to confirm that the novel experimental DNA produces good results.
I am pleased with that, because our depth of knowledge is actually far greater with DNA. This also allows us to evaluate new probiotics quickly without needing to wait for clinical studies and publications.
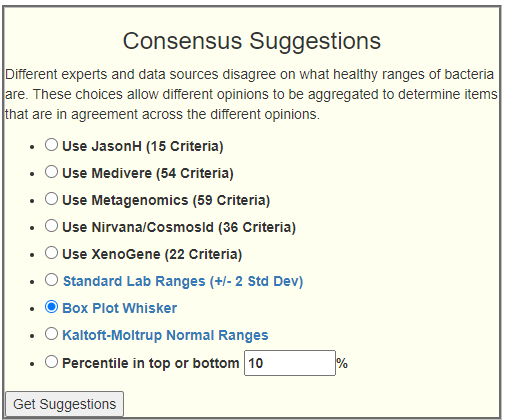
Consensus Report
As has become my custom, I whipped thru all of the suggestions using expert criteria.
Percentile in top or bottom 10%ile – 122 matches (25%)
Looking at the consensus number of suggestions for the above, the numbers were similar, suggesting that despite the differences number of bacteria selected, the suggestions were likely similar.
Takes
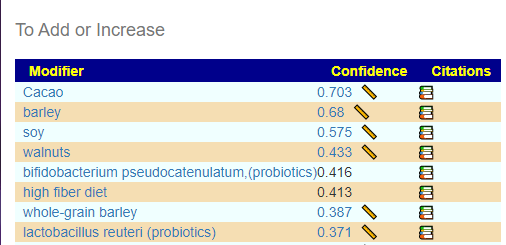
My personal pick of the top suggestions are below (excluding probiotics cited above):
Cacao (i.e. 85% Chocolate or higher) – studies have shown that it helps ME/CFS
This leads to the regular suggestion frequently seen with ME/CFS patients: Start each day with barley porridge with walnuts and appropriate yogurt. Note: Oats is on the safest list too, but less studied.
As a side note: meat and beef do not occur anywhere on the safest list. milk-derived saturated,fat and high saturated milk fat diet does — which suggests that whole milk should be the preferred milk (if milk is taken)
Avoids
The following items caught my eye on the highest risk items:
Miso, Fish Sauce (so type of soy is important) – I would likely keep to the traditional Japanese desert Natto (if you can get it – it is a n acquired taste)
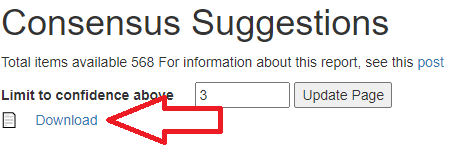
It is left to the reader to go thru the lists. The list suggestion counts, from safest to most avoid, was (258, 88, 33, 52, 33,101) – so full of strongly to take…
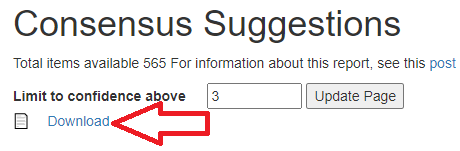
I should point out that the complete list is available for download. I would suggest downloading it and then check everything in the diet against the list.
The land of Supplements
The AI Kegg items detected as being low are:
Glycine – Percentile: 3
L-glutamine – Percentile: 2.1
L-Threonine – Percentile: 9
magnesium – Percentile: 0.7
Molybdenum – Percentile: 3.8
I downloaded the list from consensus and put their results below
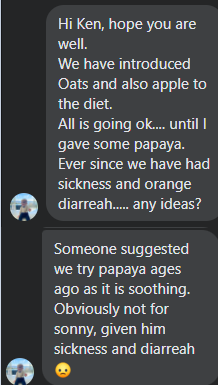
Remember — beware people telling you what is good for you! A mother recently message me. She started the suggestions and everything was going ok and then she listened to a random suggestion.
Prescription Drugs
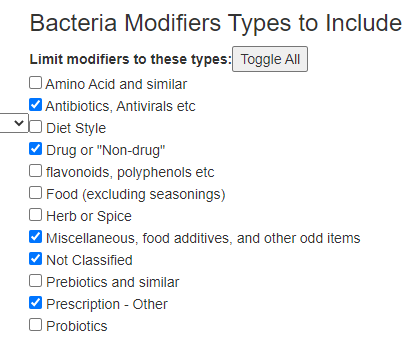
I decided to do a consensus report on prescription items. This is done on Advance Suggestions page. I checked the following items:
And then went thru the same expert choices as above.
The results are actually more items as shown below’
I would suggest downloading and placing the list on your mobile phone to have handy when discussing prescription drugs with your physician. Sometimes, you find alternative drugs would satisfy the MD and be better for your gut… it is negotiation!
I was amused, with some of these results for the alternative substances:
He mentions some antibiotics that he was on without apparent success
Erythromycin, – a mild take (5/0), impact ratio is 4:1
Rifaximin – a stronger take (7/0) impact ratio is 2:1
Vancomycin – a mix result (6/1) impact ratio is 2:1
Doxycycline – (3/4), impact ratio is 3:2 (net positive)
Minocycline – (7/0) impact ratio is 2.5:1 and is suggested as a replacement. I checked all of the tetracycline family and this was the best one.
The nice thing is that none made him worst. I leave it to him to lookup the use, side-effects of the best suggestions and then see if he can persuade his MD to do off-label prescriptions. My usual suggestion is to follow Cecile Jadin approach and do rotation: 7-10 days on, 2 weeks off, take a different one, repeat.
Bottom Line
My intent is to show you how to use the data available. “To teach you to fish“. As you try fishing your skill level will improve and you may be able to teach others to fish.
All of these are suggestions coming from mathematical models and not clinical experience. Suggestions should be reviewed by a knowledgeable medical professional before starting.
I am a computer scientist and a statistician. I am not licensed to practice medicine, and where I live has strict laws about ‘appearing to practice medicine’. What I can do for readers is to write a public blog (anonymous) from your data and back story as an education post on using the software and the statistics it produces. I cannot consult. The content should be reviewed by a medical professional before implementing.
Bottom line, my time is better spent for everyone in building the data and the methods, not in dealing with a small number of clients (thus relationships will go undiscovered and/or data becoming stale). If you want or need hand holding — there are many that will gladly do it for a fee, some uses this site and others use University Training from 1990.
There is a Long COVID Study in progress via the cooperation BiomeSight.com and Microbiome Prescrption. The data is not yet processed for the study, but we have some interest results already from those that uploaded their samples and marked Long COVID as a symptom.
Bacteria
Taxonomy Rank
Average Percentile
Frequency Seen in this Group
Frequency Seen in All Samples
Micrococcaceae
family
19
45.8
36.5
Actinobacteria
phylum
19.7
100
99.7
cellular organisms
norank
20
100
99.9
Adlercreutzia equolifaciens
species
20.1
62.5
42.8
Peptostreptococcaceae
family
22.8
95.8
96.5
Butyricimonas virosa
species
23.3
41.7
38.8
Sarcina
genus
24.7
45.8
52.4
Enterobacter
genus
25.1
41.7
23.6
Lactobacillaceae
family
26
95.8
94.9
Coriobacteriia
class
27
100
99
Actinomycetia
class
27.6
100
99.2
Adlercreutzia
genus
27.8
66.7
45.3
Slackia faecicanis
species
28
37.5
11.8
Bifidobacterium adolescentis
species
28.1
79.2
31.4
Rhodovibrionaceae
family
28.4
37.5
0
Blautia wexlerae
species
29.2
100
94.4
Anaerostipes
genus
29.7
95.8
96.1
Salinicoccus luteus
species
30.9
37.5
12.6
Staphylococcaceae
family
30.9
62.5
40.4
Bifidobacteriales
order
31.2
100
89.7
Holdemanella biformis
species
31.3
66.7
32.7
Coriobacteriales
order
31.3
100
95.7
Holdemanella
genus
31.4
66.7
32.8
Eubacteriales incertae sedis
norank
31.5
95.8
89.5
Bifidobacteriaceae
family
31.7
100
89.6
Fusobacteria
phylum
31.7
45.8
40.8
Fusobacteriia
class
31.8
45.8
40.7
Eggerthellales
order
31.8
100
97
Eggerthellaceae
family
31.9
100
97
Terrabacteria group
clade
31.9
100
99.9
Fusobacteriales
order
32
45.8
40.7
Collinsella
genus
32
91.7
89.4
Leuconostocaceae
family
32
62.5
54.4
Coriobacteriaceae
family
32.7
100
94.7
Bifidobacterium
genus
33
100
88.2
Pseudobutyrivibrio
genus
33.2
79.2
81.6
Turicibacter sanguinis
species
33.8
62.5
55.5
Bacteroides denticanum
species
34.2
70.8
21.9
Fusobacterium
genus
34.2
41.7
33.9
Erysipelotrichaceae
family
34.4
100
98.8
Dorea
genus
34.4
100
98.3
Natranaerobiales
order
34.5
54.2
21
Actinomycetaceae
family
34.6
87.5
82.5
Roseburia faecis
species
34.8
95.8
80.9
Veillonella montpellierensis
species
34.9
37.5
14.6
Holdemania
genus
65.7
95.8
77.6
Chlorobaculum
genus
67.4
50
20.2
Bacteroides ovatus
species
67.6
100
73.9
Anaerotruncus colihominis
species
69.1
100
65.8
Oscillospira
genus
75.1
75
55.5
Data on a Sample Size of 24
What is striking is not higher counts, but certain bacteria are being seen a lot more often. In fact, no bacteria is seen less often with Long COVID people but the amount may be less. That is more types of bacteria but with lower levels than average.
Note: Percentile means the percentile ranking of samples for a specific bacteria. The expected percentile for a random sample of people is 50%ile. Thus a lower percentile means that the median of the group is less than the median of the population. A higher percentile means that the median of the group is higher than the median of the population. The severe skewness of bacteria distribution does not mean the the average of the sample is lower or higher than the average of the population — in fact, they may be the same. (Welcome to statistical gymnastics 301!!!)
The ME/CFS Connection
This type of novel analysis (using frequency of detection and not amount of bacteria) results in Long COVID and Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). being very similar at the microbiome level. see Bacteria Shifts Seen in Chronic Fatigue Syndrome.
My son is born in 2009 and diagnosed with autism in 2011. When he was 3 months old he has lot of reflux and unable to digest milk always used to throw up and we ended up using antibiotics because of mucus forming issues and at 10 months he had few words.
And at 18 months he got diagnosis’s of autism and was completely Non-Verbal.
After removing gluten and dairy from his diet at age 3.5 he started saying words
he also got diagnosed with Lyme and coinfections like bartonella and Babesia .
Now he is 11 years still having lot of issues like his weight is just 55 Lbs he has focus issues and lot/severe OCDs and tantrums and lot of rigidity and not conversational yet ,cognitive issues cannot understand abstract concepts and has lot of echolilia and no social skills and gets head pain all of a sudden which might be PANS will last for few minutes and will be fine again.
And he has lot of Gut issues like failure to thrive even though his diet his healthy he does not gain weight at all and he has leaky gut and always have constipation issues and poor digestion issues and picky eating and he complaints some times that his stomach hurts and some times his stomach gets very tight like gas forming. And he has brain and Gut inflammation.
Very recently from couple of months he started having Acid Reflux issues after eating he will be spitting for an hour as if something is coming back from his stomach.
We also noticed that when ever he eats chicken and eggs he is more constipated. We did the GI work up and everything came up normal except one thing that he does not have enzymes to digest lactose and also we make sure he is not constipated and his bowls are moving everyday with some laxative.
We have two samples for this person, while we will use the last one for suggestions, a comparison may be spark insights.
Basic Analysis
Looking at the two samples, we see that things are very different than with the ME/CFS person in this post. Instead of over representation in rare bacteria, there is over representation in common bacteria (i.e. the bacteria that most people have).
Earlier
Sample
Latest
Sample
Percentile
Genus
Species
Genus
Species
0 – 9
10
1
7
7
10 – 19
10
9
9
12
20 – 29
6
9
8
13
30 – 39
10
18
7
10
40 – 49
12
9
6
12
50 – 59
12
15
9
18
60 – 69
10
7
8
12
70 – 79
10
16
10
16
80 – 89
25
39
22
38
90 – 99
103
149
40
64
Std Dev
29.31
44.00
10.65
17.61
Looking at “Potential Medical Conditions Detected” for both samples we see a very long list of candidate conditions for both samples
For “Bacteria deemed Unhealthy”, again we have some long lists
For “Dr. Jason Hawrelak Recommendations”, we have the earlier sample at 75%ile and the latest sample at 98.8%ile, i.e. “no issues”
AI Computed supplements at 10% level: Neither sample had any.
There is the appearance of improvement between the sample. This may be solely due to the changes due to age (18 months between samples), or moving further away from microbiome disruptive events of the past.
Going Forward
We need to go with some caution because the child microbiome is different than an adult’s and most of the data we are using are from adults.
I am going to build the consensus in a slightly different way than usual:
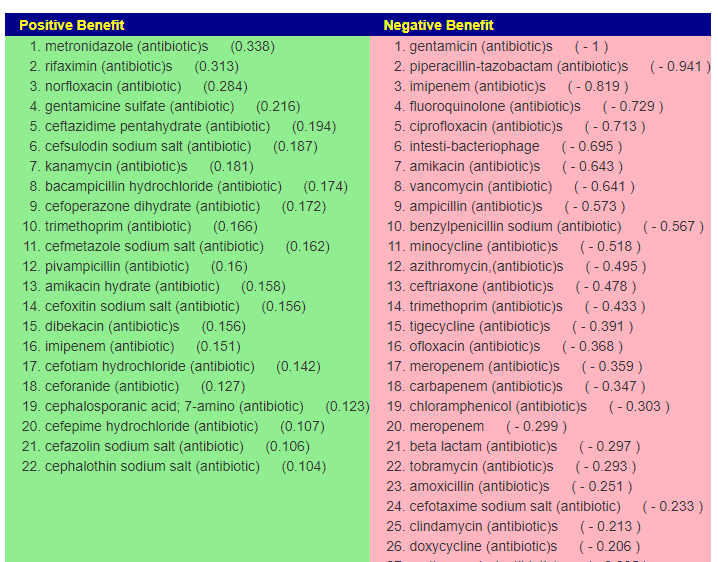
Seeing lactulose as a very strong to be avoid agrees so much with no tolerance for milk. I checked the antibiotics positive/negative benefit and was actually surprise to see on the positive impact many of the antibiotics used for ME/CFS and Lyme: fluoroquinolone (antibiotic)s, tetracycline (antibiotic)s, minocycline (antibiotic)s with the best one being vancomycin (antibiotic). This was interesting because “Vancomycin is used to treat colitis (inflammation of the intestine caused by certain bacteria) that may occur after antibiotic treatment.”[MedlinePlus]
Questions And Answers
Do you mean your current recommendations is not to use any probiotics or use only Lactobacillus salivarius strain of probiotics ?
Only a very small number of probiotics appear to have a positive impact, less than 18. The other 39 came out with a negative effect. You need to read the labels carefully.
I also for the earlier sample you mentioned the PDF use of prescript assist soil based probiotic and also lactobacillus bulgaricus (probiotics) and lactobacillus kefiri . I have not used these so now do you think using them might be helpful based on the analysis
Those are on the recommended list, so YES
And based on your analysis what is most pathogenic bacteria that I need to address from the sample which is problematic such that I research and see how to reduce it?
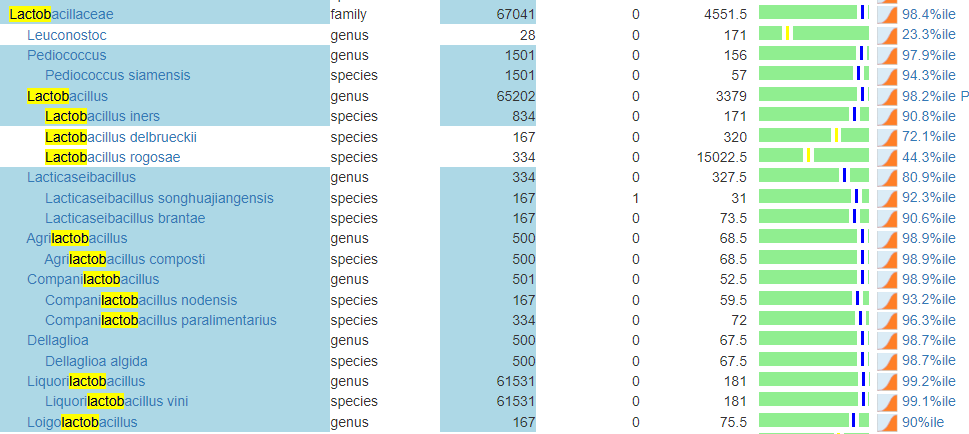
Unlike most people, this child has a huge amount of Lactobacillus bacteria, he has 98% more than anyone else in the database. Clicking on the link above (and those below) are the worst offenders where his levels are higher than 95% of peoples
In the video, I will show how you can find suggestions EXPLICIT for these.
What key strains of good bacteria do you think is missing for weight gain or in general ?
Every good strain becomes bad if there are too many of them, for example Lactobacillus above. The microbiome should be viewed as “Yin/Yang” and not good and bad. I really do not have a clean answer for that question.
Which Lactobacillus strains does he have has 95% which I need to avoid further is it Lactobacillus Reutri and Lactobacillus Johnson and Lactobacillus planetarium are those the ones which I need to avoid completely to give or any other list?
ALL Lactobacillus are similar with only small changes between them. They are a family. As with human families, they cross support each other. You want to lower all of the Lactobacillus, ideally have no lactobacillus probiotics.
Currently I started using sauerkraut , thinking he needs more Lactobacillus strains and I read sauerkraut has lot of different good strains. Would it be still okay to use it?
He DOES NOT need more Lactobacillus strains — he needs a lot less!
In my humble opinion NO. Two main reasons:
You have no idea of which bacteria are in. Commercial versions usually do not list the species. On the few that do, it is very questionable if the label is correct. ” the species of lactic acid bacteria present in sauerkraut fermentations are more diverse than previously reported and include Leuconostoc citreum, Leuconostoc argentinum, Lactobacillus paraplantarum, Lactobacillus coryniformis, and Weissella sp.” [2007] For Weissella, he is at 90%ile — too high. He does not need more
Do I need to do anything to reduce Lactobacillus strains that are high?
A word of caution here. Are you going to target just one item of concern in several dozens by focusing on this item (with the potential cost of many other things becoming worst); or work from suggestions that are targeted to improve the microbiome as a whole?
In response to question #3, I did a hand picked of all of those over 95%ile on the Health Summary with the results shown below
In response to quest 5-7, the Lactobacillus tree. Note that of 65,000 Lactobacillus bacteria — less than 1,400 ( 2%) had the species identified. We do not know the species that he is high in.
A short list of Suggestions
To be discussed with family MD before starting
Antibiotics
A course of vancomycin (antibiotic) to start
3 weeks after this course is finished one of (piperacillin-tazobactam or gentamicin)
Supplements (add one a week for 3 weeks than take 2 weeks off)
A baby aspirin once a day — watch especially for any improvement in brain activity
He may have a sub-clinical (mild) form of Antiphospholipid syndrome (thick blood) triggered by the microbiome shifts – I am reflecting my own experience here.
One of the easiest modern ways to do it, is to download this data as a CSV and save on your smart phone when shopping.
REMINDER: The items indicate odds/confidence in shifting the microbiome is the intended direction. It is NOT how effective it is. Each item in the take likely improves your odds of improving when taken; keep taking items the avoid list — continuing likely increase the odds of not changing.
Short bio: 35yr Male have had ME/CFS for about 7 years, see A review of a ME/CFS Microbiome for prior review plus backstory. This was my review for “A – Thryve:2021-11-21 self” below.
This person has had done three samples, so we will both look at the latest sample and across samples.
The key questions focus on objective improvement and subjective improvement.
General Health Issues
The evenness of Genus and Species across percentile is shown below
A
A
B
B
C
C
Percentile
Genus
Species
Genus
Species
Genus
Species
0 – 9
11
16
6
9
11
15
19-Oct
12
30
15
30
19
27
20 – 29
19
31
20
24
12
31
30 – 39
18
35
23
45
16
33
40 – 49
16
24
20
37
18
30
50 – 59
21
31
25
45
21
33
60 – 69
18
20
17
30
14
22
70 – 79
16
23
11
28
16
23
80 – 89
5
14
16
24
13
21
90 – 99
3
14
13
20
5
14
Total
139
238
166
292
145
249
Std.Dev.
6.05
7.71
5.72
11.10
4.60
7.02
My reading is that at the Genus level, the microbiome is stablizing. An ideal microbiome would have a Standard Deviation of 0.0 (i.e. the appropriate percentage is in each class). We see for Genus move from 6.0 -> 5.7 -> 4.6. Species have a far greater degree of randomness because may species are not identified, most genus are identified.
Potential Medical Conditions Detected
The count has been similar: A:3 B:6 C:2 with the one items in common being Allergies.
Unhealth Bacteria
The counts were similar between all samples: A:18, B:20, C:21
Dr. Jason Hawrelak Recommendations
We had significant improvement between the first two samples and a slight loss going to the third: A: 56.5%(5) B:95.5% (8) C: 89% (7)
AI Computed Probiotics
Sample ASample BSample C — NOTHING!!!
AI Suggested Supplements
Using the default 10% level, we found samples A and B only suggested one supplement. C suggested 2 (L-Histidine and manganese). I looked up the item from A and B and saw that it had continued to improve. 🙂
Supplements
A
B
C
beta-alanine
7.3
9.2
17.3
Has there been positive change?
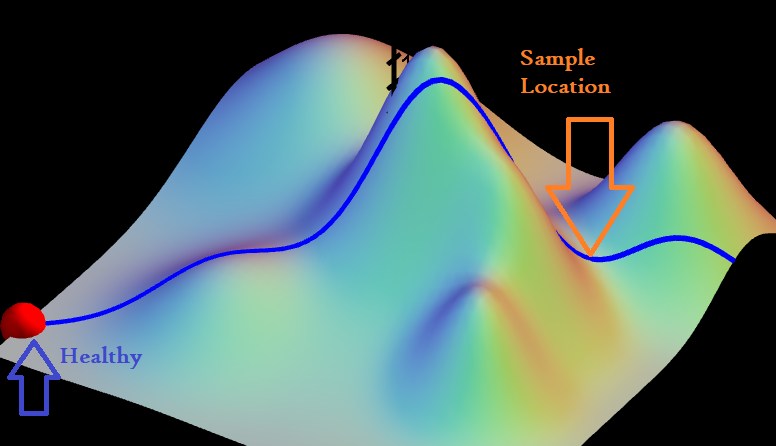
My reading of the above objective numbers is yes in several vectors. There was nothing show a clear negative change. Somethings stayed put — that is fine, it is small steps. As the picture below illustrates, it is not a direct line/tunnel through the mountain ranges of dysbiosis, we have to work our way across passes and valleys.
The “I don’t feel better” quicksand
I have too often seen — especially with people suffering from Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) — patients giving up on a course of action because they reached a point where they may state “I don’t feel better from doing this, so I am changing…”. For these people, this is often caused by several factors:
They do not remember how they were actually 2 weeks or 2 months ago…
Their MD have no objective tests to show progress
They expect significant constant change constantly (they are frustrated waiting for improvement)
Using the microbiome and repeated testing, they can get objective measurement of changes instead of relying on subjective measurement being done under the influence of brain fog with memory problems.
In this person case, we do see objective improvement of the dysbiosis. What about subjective?
“You’re welcome to mention I have noticed improved sleep and lower anxiety despite my good and bad bacteria shifting around “
From the reader
Moving Forward
As reviewed above, we have no KEGG suggested probiotics, but do have these supplements suggested:
L-Histidine – Percentile: 2.7
manganese – Percentile: 3.7
NADH – Percentile: 15.6 (this has been studied for ME/CFS
On a personal note, I used NADH during my 1999-2000 relapse (1st time diagnosis). I eventually switched to 400 mg of flushing niacin twice a day (after MD checked my liver function see facts) and have continue to do so (with liver being tested every year).
Getting suggestions based on US National Library of Medicine Studies
As is my pro forma approach, I did each of the following (with number of bacteria picked after):
For more information on probiotics see the bottom section of this recent review.
For supplements, there are only 3 easily accessed items that are positive, everything else is negative impact!!: Ferric citrate (iron supplement), magnesium (commonly used for ME/CFS) and vitamin k2
For other things, see the video or the suggestions on your microbiome.
Bottom Line
You are making objective progress. A word of caution, if some of the items that you are currently taking on the avoid list, slowly remove them by reducing amount and watching for potential adverse effect. Some of the positive objective changes may be due to them (there is a risk of a feedback loop: if you are taking them, they are not needed BUT it you stop taking them, your microbiome may devolve to a state needing them).
Last – Using Symptoms
This is EXPERIMENTAL. It is a thought experiment and I am still learning it’s behavior. For some symptoms it may reduce awesome results, for others it may improve one set of symptoms at a cost of other symptoms getting worst. I picked two of the more unusual symptoms that he had:
Comorbid: Methylation issues (MTHFR)
Immune: Chronic Sinusitis
This resulted in this list being selected with a very strong Filter (first time I have seen this)
All of the prebiotics listed are similar, any one would do.
I would suggest using it to increase the priority of some items that are positive suggestions in the consensus list, I would not go with using this set of suggestions alone.
Questions from Reader
Ferric Citrate , haven’t been able to find this type? Have you seen it anywhere? Also how would one figure out the dose for gut bacteria shifting?
I am an ex-science teacher and thus know it more common name, Iron Citrate. Swanson and others sells it.
Bacillus- taking terraflora , think I’m up to 6 caps. I saw in a study I need to get to 20 !! …I also have prescript on hand BUT that has a lot of other SBO strains. Would you stuck to TERRAflora for now?
I would keep the Prescript Assist on the shelf, and keep to Terraflora, I would keep increasing the dosage every second day until the bottle was finished. I would look around for ones with similar probiotics for the next cycle, for example Youtheory, Spore Probiotic, 6 Billion CFU, 60 Vegetarian Capsules – for two reasons:
Cheaper per BCFU (and also higher BCFU per dosage)
Different strains often helps because they produce slightly different products
Miyarisan , I thought I saw this in my results somewhere , maybe it was far down the list…would you save or finish if you had my results?
It is on the list, I would finish it before starting the next cycle of probiotics (REMEMBER: we want to be rotating the probiotics – not take them continuously)
Akkermansia – I have 2 bottle of this stuff actually from pendulum . I read you and your wife has taken it. How much did you take or I know it’s a new product but if you’ve seen a study with dosing please let me know.
The one existing study used 10 BCFU/day, and the bottle reads 0.4 gm. Lacking more information, I would just keep to the bottle recommended dosage.
NADH- I have the flush stuff and cq10? Do you think that combo works or does it have to be Nadh?
Personally, I found flush niacin had greater impact and still look forward to my morning flush to get the mind working (it improves oxygen delivery because it’s a vascular dilator). Assuming you can tolerate the flush.
ALWAYS REVIEW WITH YOUR MEDICAL PROFESSIONAL FIRST
This person has limited experience with the microbiome, so the video provides an enriched commentary on this blog post.
Person’s Back Story
August 30th, 2016 I was in the post office and I got vey light headed and almost fainted. I was never the same. I was very dizzy and extremely lethargic. A brain MRI found a pituitary adenoma which MDs and neurosurgeons said had nothing to do with my symptoms.
Symptoms were getting worse; head pressure, head tightness, extremely sensitive to sound, sensitive to light, low body temp and resting heart rate of 112. I went on a 25 day course of doxycycline to treat what some thought could have been Lyme disease.
This destroyed my already compromised gut. I had my gallbladder out in 2006, h pylori in 2007 and have since had stomach issues.
All kinds of additional testing and they could find nothing.
Every doctor recommended anti depressants which I refused.
November of 2016, I started ozone injections directly into the vein.
I was put on hundreds of supplements for Leaky gut.
Feb 2017, Neurologist found the brain SPECT scan was not normal. Poor blood flow to certain parts of the brain due to systemic inflammation.
I had changed my diet and eliminated gluten entirely.
Started coffee enemas a week prior to having these tests done
New medical professional after reading my labs, she believed 100% I had celiac.
I had eliminated all gluten and was also sugar, dairy, soy, grain and nightshade free.
Started hyperbaric oxygen therapy and completed 45 dives in a hard chamber. I purchased a chamber for home use in August and received in October. I was doing daily dives until I got a sinus infection and got fluid in my ears do I have not dove in weeks.
I’m scared because I have done so much for my health I don’t understand how I have a fatty liver.
I am 5’2″ 114 lbs and eat and live so healthy.
I have a whole house filtration system
Purchased an infrared sauna in December and use that a couple of times a week.
Diagnosed with SIBO in Feb 2018 after breath test at gastroenterologist.
I kept going to doctors and they were telling me nothing was wrong.
I had my gallbladder out in 2006, umbilical hernia in 2007 and h pylori in 2007 treated with triple antibiotic therapy.
And this is the very edited version, lots of specialists (many of whom have written books or have articles published on peer-review journals).
My Blinkered View
I am not a medical professional, I am a data scientist, statistician and software developer (see my Linked In for details). I am also very high function ASD — which gives me the ability to handle massive amounts of data with unbroken focus. The limits of my expertise is with building tools and designing artificial intelligence systems for the microbiome.
I work off the hypothesis that many symptoms and their severity are the results of microbiome dysfunction.
Looking a Potential Medical Conditions — there are definitely major issues, there are mountains of concerning shifts.
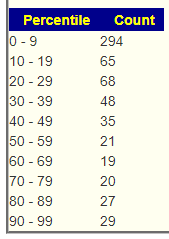
And on the normal side of the house, bacteria deemed unhealthy and Jason Hawrelak suggestions appear normal. In other words, it is not your usual case of gut dysbiosis. Rare bacteria are over represented as shown below. This will create some challenges, because modification of rare bacteria has very little information.
A new table on the “My Profile” Page
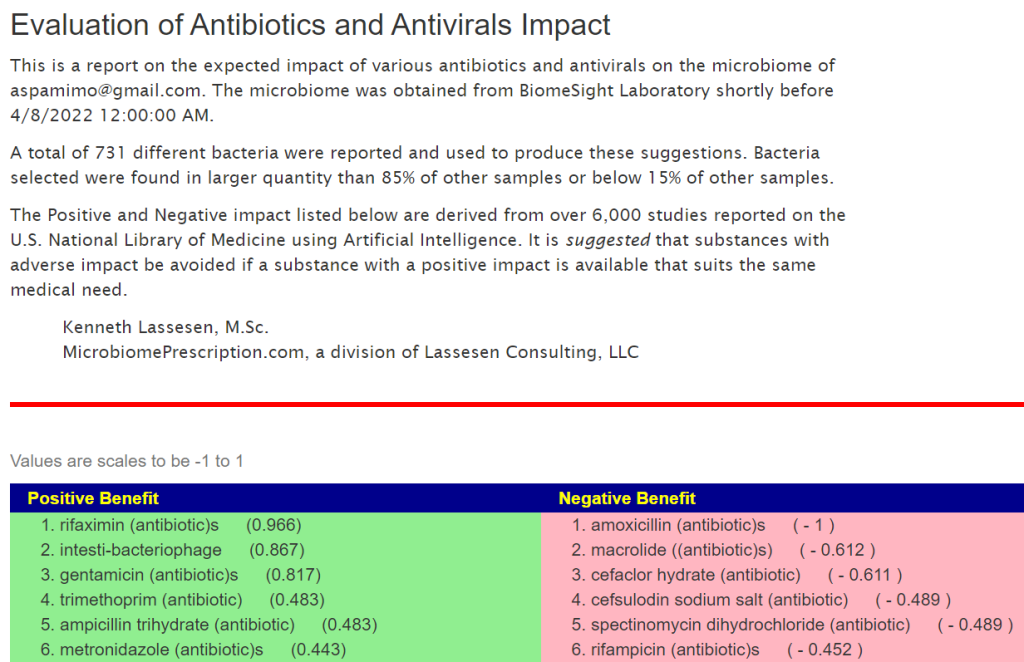
Looking at the Antibiotics page, we see that her poor response to the antibiotics she was given is reflected in the numbers computed from her microbiome.
Note that all of common antibiotics for Lyme disease and ME/CFS are NEGATIVE.
Moving forward
Given the high number of unusual bacteria, my prefer start is at the DNA level, i.e. using KEGG data to see if there are deficiencies that can be moderated.
RETAIL Probiotics is very similar to many people with dysfunction (so much that I keep double checking the computation). I listed the species after so you can better understand what you want in the probiotics)
Supplements – this is a much longer list than I usually see. Magnesium and Molybdenum are the my first choice from this list since they are involved in a lot of biological processes.
Amylase (Enzyme) – Percentile: 5.7
beta-alanine – Percentile: 1.5
L-Cysteine – Percentile: 10.4
L-glutamine – Percentile: 5.9
L-Lysine – Percentile: 3.6
L-Proline – Percentile: 5.7
L-Threonine – Percentile: 6.5
magnesium – Percentile: 1
Molybdenum – Percentile: 5
NADH – Percentile: 2.8
Phytase (Enzyme) – Percentile: 12.7
I will move on to the usual process of generating consensus suggestions. Given the unusualness of this sample, I do not know what to expect. It could be outside of our existing database (the above suggestions was based on DNA and thus we have almost complete coverage).
We will run each of the above and then look at the consensus report.
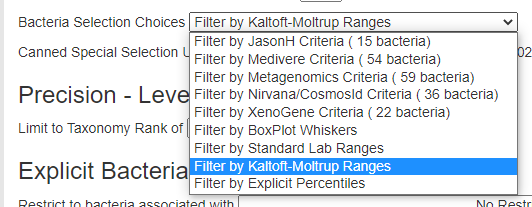
The top 5 selected 9 bacteria; Standard Lab Ranges came in with a very low (and surprising) 5 bacteria; Box Plot Whiskers Ranges had lower than usually seen, just 36; Kaltoft-Moltrup Ranges came in with a normal looking 137 bacteria, Filter by 10 percentile came in with a massive 332 bacteria!! Given what we saw above, these unusual atypical results are not surprising.
l-glutamine – counter indicated to the DNA suggestions above, so I would omit it
There are 568 different items (I downloaded the file and open in Excel). With the exception of l-glutamine, all of the DNA based suggestions were either positive or not found (i.e. no clinical studies using them).
How to download the data as a CSV file that will load into most spreadsheets.
For diet planning, it may be good to write out your weekly supplements, food (including herbs used) and check each against the Excel spreadsheet and make minor changes as appropriate.
Trying the new Experimental Symptom Filtering
This person entered their symptoms, so it is available. If you are not familiar with this process, see this post.
Symptoms Picked
Immune Manifestations: Hair loss
Comorbid: Small intestinal bacterial overgrowth (SIBO)
Comorbid: High Anxiety
Comorbid: Hypothyroidism
Neurological-Audio: Tinnitus (ringing in ear)
When I went to the bacteria list, I was impressed by the number of bacteria listed with Weak Association
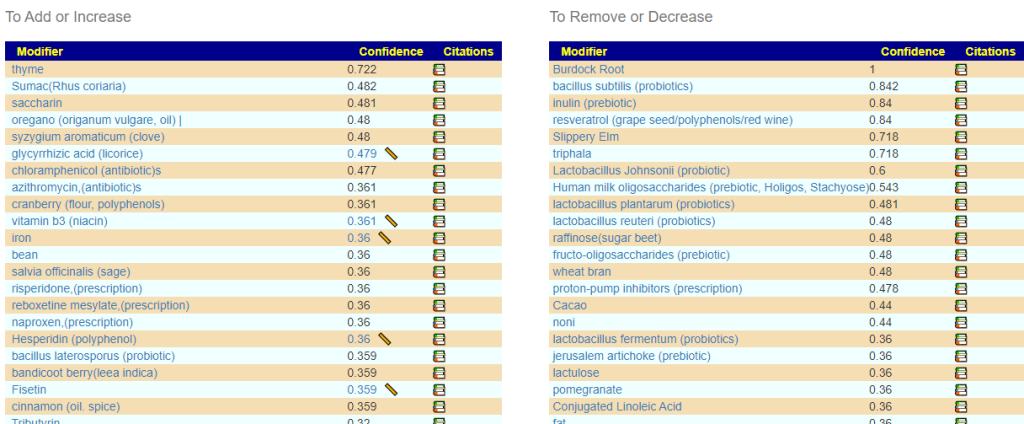
Items to take — in general, these were also found as should take on the consensus report
I went back to Weak Association, and the list was very similar.
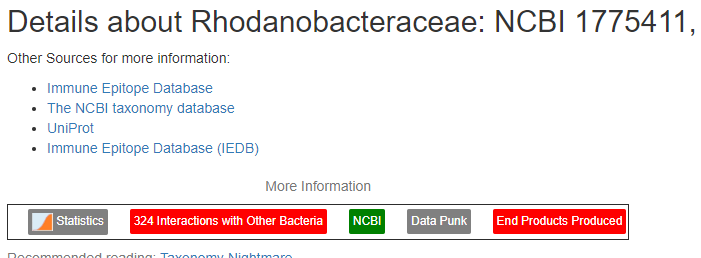
A trip to the wilderness…
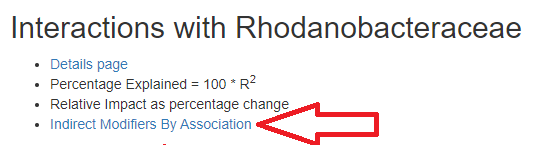
There is a manual “back door” to suggestions when there is no direct clinical study. Clicking on the bacteria listed above takes you to the information page. Note that there is an Interactions with Other Bacteria link.
Clicking on this link, goes to a page showing the estimates for these interaction. On that page, there is a quiet link that we will now use.
For this one, we wish to increase it (in fact for all of them), only one items shows up as increasing for any of them:
All of them have very similar list (likely because they are in the same “bacteria fraternity” )
Bottom Line
At this point, I have covered all of the paths that I prefer to shift the microbiome closer to normal / healthy. I would suggest the person takes this information and development an action plan (diet, supplement changes). As always, it should be reviewed by a medical professional familiar with the patient. After 2-3 months, a new microbiome should be done. I will gladly do a follow up to see how well things work or did not work. I am interested in learning, not being right!
Now to feedback from this person:
This is too much information!
To prevent people from being overwhelmed, I would suggest working from the DNA suggestions above. The other suggestions have a bias because it is based on the number of studies (and thus popularity with researchers). The DNA suggestions lack this bias, there is a little bias because the bacteria sequenced for DNA are influenced by researchers choices, but the data is reasonably comprehensive.
Probiotics: Which product, dosage, when to take, for how long?
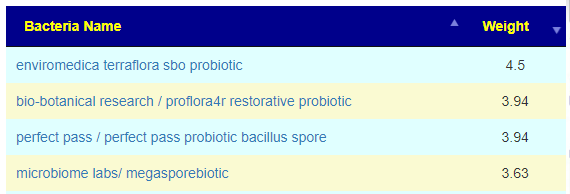
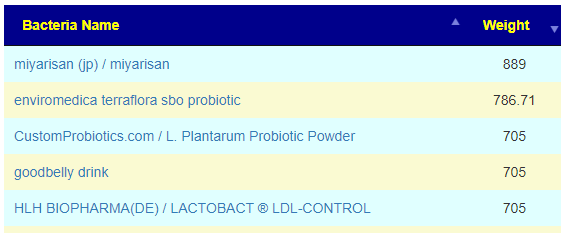
Q: “Enviromedica terraflora has 3 different sbo probiotics; advanced care, immune and daily. How do I know which one to get?”
A: Compare the contents to the list that it was computed from (click on enviromedica terraflora sbo probiotic to see the bacteria in it) . If all of these produces have the same amount of bacteria/probiotic, then use the one that is best pricing (i.e. BCFU/ $). The bacteria are:
Terraflora Advanced Care SBO Probiotic – $54, 1 BCFU per TWO capsules
Terraflora Daily Care – $43, 1 BCFU per TWO capsules
Terraflora Deep Immune SBO Probiotic – $51, 1 BCFU per TWO capsules
The daily care is what you want. The other have additional additives which may help or hurt — you need to check each one additives. We are keeping to the least complex route — so go with the Daily Care.
In general, these additives allows firms to upsell to more expensive products (far more than the price of the additives).
Dosages
There is a page with dosages for many supplements and probiotics — based on clinical studies (not what the manufacturer suggests on the bottle). The page is located here. Unfortunately, you will not find the retail product name listed, the list is by the bacteria name in the product.
Since two capsules are 1 BCFU (aka 1000 MCFU), I would start a two capsules and every second day increase it by two capsules until you hit 10,000 MCFU (20 capsules!). If you notice changes, then either keep that dosage or step back the dosage. 10BCFU have been explicitly tested for safety [Study]
When to take?
This is a personal opinion, but just before bed time seems best. There are many many opinions out there and no well done studies. Typically there are one of two responses (depending on the person)
Deep sleep, often with night sweats, as the bacteria interact with your immune system rebuilding itself (i.e. energy is not being directed at your activities, but the immune system) [Taking probiotics at night could make them way more effective. 2019]
Insomnia — the effect of the probiotics is releasing chemicals causing wakefulness. If this is the case, switch to 1 hr after breakfast.
For how long?
Since probiotics do not persists, often their effect on “bad bacteria” is caused by them producing antibiotic compounds (most of our commercial antibiotics were discovered in bacteria). There are several studies that found that rotating antibiotics is far more effective than keeping to the same one. We should do the same with probiotics. A rule of thumb that I use is simple (and helps with monthly budget), is to do one month or one bottle (which ever comes first) and then move on to a different probiotic. For Terraflora, it’s a 60 count, doing the suggested dosage pattern cited above, it will last just 8 days until the bottle is empty.
For Miyarisan, (🍽️ clostridium butyricum (probiotics)) we have 330 tablets in a bottle. And studies [list] range from 60mg/day to 1050 mg/day. The literature says: 270 mg of butyrate-producing bacteria (Miyairi bacteria) in 9 tablets … so start with 4 capsules and keep increasing every 2nd day. It will take 21 days to get thru a bottle.
CustomProbiotics.com / L. Plantarum Probiotic Powder . This can come as a price shock to many people ($115 for a bottle) but their bottle recommends 0.8g, that is 320 BCFU per day. So one bottle is 62 days at that dosage (suddenly the price/day is similar to the above). The maximum for reference studies is 60 BCFU/day [src], so you go with lower dosage (this is a powder, not capsules). In this case, switch after 3-4 weeks.
Question: Where does this information come from
This was a question from this reader. The short form:
Some 8,052,707 facts were extracted and entered into a database.
This data from used to build a mathematic model of the microbiome, what happens in it and what modifies it.
A longer form can be done as a walk thru:
To get the documentation
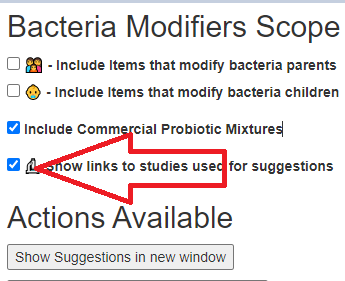
If you go to the ad-hoc suggestion page, there is a checkbox, “Show links to studies used for suggestions“. Checking this and then asking for suggestions results in the suggestion page showing a 📚
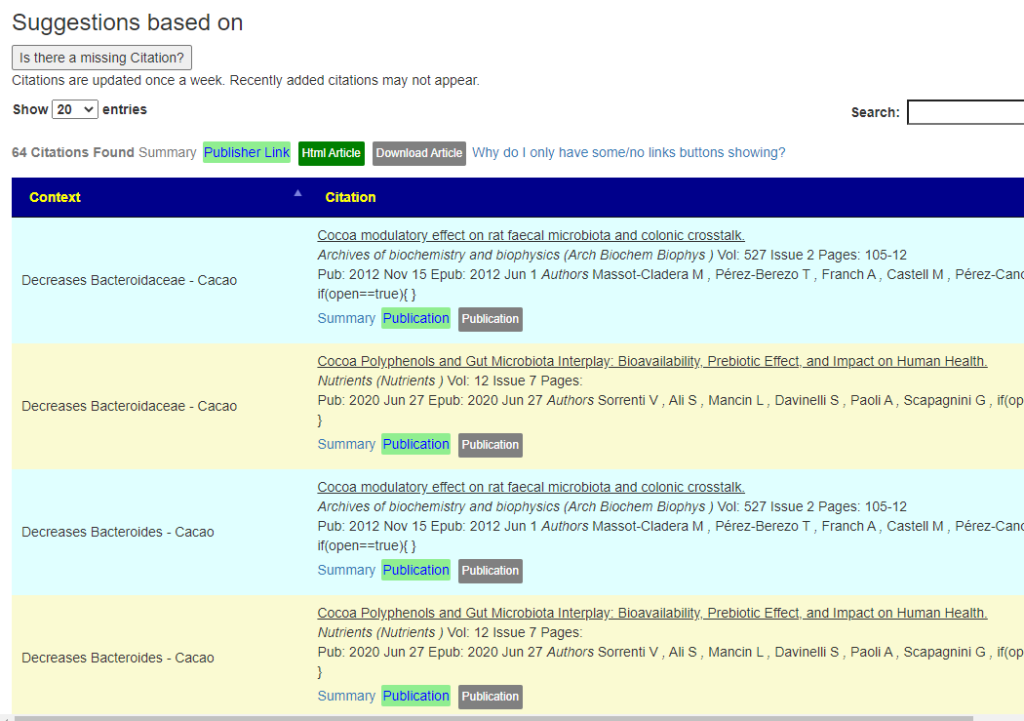
Clicking on this will list off the studies used to make this decision. An example below
This is for just the first item, Cacao. Note we have 64 studies providing information. This list of studies provides information on the 108 bacteria picked to modify. Potentially, to make this decision we could have looked at 64 x 108 = 6,912 different facts (bits of information) to determine if it was good or not.
What is very different from this versus advice from a MD is extremely simple. A MD may make a decision on typically a dozen facts that stuck in their mind, not the 10 million facts that this program, Artificial Intelligence, considers.
The downside is that a MD will not overwhelm you with information, he may prescribe just one drug or suggest something vague like “eat more fiber”. With this Artificial Intelligence, it will often identify which types of fiber should be eaten and which should be avoided. All of this is based on studies with the where did you get this suggestion from documented and linked to. If you ask a MD, you will be lucky to get a single document and could get an angry MD because asking for documentation could cause him offense.
Bottom line, you are investing in your body, similar to investing in the stock market. You are told to invest in tech stocks — so you buy some bit-coin stock…. and discover that you are worth a lot less (looking at recent history), or you start wading thru the various stocks and reading opinions for each, and likely make better choices and have a healthy collection of stocks (or body). There is no easy route for investing in either the stock market or your body (unfortunately).
Reversion of Gut Microbiota during the Recovery Phase in Patients with Asymptomatic or Mild COVID-19: Longitudinal Study. Microorganisms (Microorganisms ) Vol: 9 Issue 6 Pages: Pub: 2021 Jun 7 Epub: 2021 Jun 7 Authors Kim HN , Joo EJ , Lee CW , Ahn KS , Kim HL , Park DI , Park SK , Summary
The gut microbiome of COVID-19 recovered patients returns to uninfected status in a minority-dominated United States cohort. Gut microbes (Gut Microbes ) Vol: 13 Issue 1 Pages: 1-15 Pub: 2021 Jan-Dec Epub: Authors Newsome RC , Gauthier J , Hernandez MC , Abraham GE , Robinson TO , Williams HB , Sloan M , Owings A , Laird H , Christian T , Pride Y , Wilson KJ , Hasan M , Parker A , Senitko M , Glover SC , Gharaibeh RZ , Jobin C , Summary
Gut Microbiota May Not Be Fully Restored in Recovered COVID-19 Patients After 3-Month Recovery. Frontiers in nutrition (Front Nutr ) Vol: 8 Issue Pages: 638825 Pub: 2021 Epub: 2021 May 13 Authors Tian Y , Sun KY , Meng TQ , Ye Z , Guo SM , Li ZM , Xiong CL , Yin Y , Li HG , Zhou LQ , Summary
Temporal association between human upper respiratory and gut bacterial microbiomes during the course of COVID-19 in adults. Communications biology (Commun Biol ) Vol: 4 Issue 1 Pages: 240 Pub: 2021 Feb 18 Epub: 2021 Feb 18 Authors Xu R , Lu R , Zhang T , Wu Q , Cai W , Han X , Wan Z , Jin X , Zhang Z , Zhang C , Summary
16S rRNA gene sequencing of rectal swab in patients affected by COVID-19. PloS one (PLoS One ) Vol: 16 Issue 2 Pages: e0247041 Pub: 2021 Epub: 2021 Feb 17 Authors Mazzarelli A , Giancola ML , Farina A , Marchioni L , Rueca M , Gruber CEM , Bartolini B , Ascoli Bartoli T , Maffongelli G , Capobianchi MR , Ippolito G , Di Caro A , Nicastri E , Pazienza V , INMI COVID-19 study group. , Summary
Alterations of the Gut Microbiota in Patients with COVID-19 or H1N1 Influenza. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America (Clin Infect Dis ) Vol: Issue Pages: Pub: 2020 Jun 4 Epub: 2020 Jun 4 Authors Gu S , Chen Y , Wu Z , Chen Y , Gao H , Lv L , Guo F , Zhang X , Luo R , Huang C , Lu H , Zheng B , Zhang J , Yan R , Zhang H , Jiang H , Xu Q , Guo J , Gong Y , Tang L , Li L , Summary
Gut Microbiota Interplay With COVID-19 Reveals Links to Host Lipid Metabolism Among Middle Eastern Populations. Frontiers in microbiology (Front Microbiol ) Vol: 12 Issue Pages: 761067 Pub: 2021 Epub: 2021 Nov 5 Authors Al Bataineh MT , Henschel A , Mousa M , Daou M , Waasia F , Kannout H , Khalili M , Kayasseh MA , Alkhajeh A , Uddin M , Alkaabi N , Tay GK , Feng SF , Yousef AF , Alsafar HS , Summary
Gut microbiota dynamics in a prospective cohort of patients with post-acute COVID-19 syndrome. Gut (Gut ) Vol: Issue Pages: Pub: 2022 Jan 26 Epub: 2022 Jan 26 Authors Liu Q , Mak JWY , Su Q , Yeoh YK , Lui GC , Ng SSS , Zhang F , Li AYL , Lu W , Hui DS , Chan PK , Chan FKL , Ng SC , Summary
Alterations in microbiota of patients with COVID-19: potential mechanisms and therapeutic interventions. Signal transduction and targeted therapy (Signal Transduct Target Ther ) Vol: 7 Issue 1 Pages: 143 Pub: 2022 Apr 29 Epub: 2022 Apr 29 Authors Wang B , Zhang L , Wang Y , Dai T , Qin Z , Zhou F , Zhang L , Summary
Alterations in Gut Microbiota of Patients With COVID-19 During Time of Hospitalization. Gastroenterology (Gastroenterology ) Vol: 159 Issue 3 Pages: 944-955.e8 Pub: 2020 Sep Epub: 2020 May 20 Authors Zuo T , Zhang F , Lui GCY , Yeoh YK , Li AYL , Zhan H , Wan Y , Chung ACK , Cheung CP , Chen N , Lai CKC , Chen Z , Tso EYK , Fung KSC , Chan V , Ling L , Joynt G , Hui DSC , Chan FKL , Chan PKS , Ng SC , Summary
Alterations in Fecal Fungal Microbiome of Patients With COVID-19 During Time of Hospitalization until Discharge. Gastroenterology (Gastroenterology ) Vol: 159 Issue 4 Pages: 1302-1310.e5 Pub: 2020 Oct Epub: 2020 Jun 26 Authors Zuo T , Zhan H , Zhang F , Liu Q , Tso EYK , Lui GCY , Chen N , Li A , Lu W , Chan FKL , Chan PKS , Ng SC , Summary
Challenges in the Management of SARS-CoV2 Infection: The Role of Oral Bacteriotherapy as Complementary Therapeutic Strategy to Avoid the Progression of COVID-19. Frontiers in medicine (Front Med (Lausanne) ) Vol: 7 Issue Pages: 389 Pub: 2020 Epub: 2020 Jul 7 Authors d`Ettorre G , Ceccarelli G , Marazzato M , Campagna G , Pinacchio C , Alessandri F , Ruberto F , Rossi G , Celani L , Scagnolari C , Mastropietro C , Trinchieri V , Recchia GE , Mauro V , Antonelli G , Pugliese F , Mastroianni CM , Summary
It Ain`t Over `Til It`s Over: SARS CoV-2 and Post-infectious Gastrointestinal Dysmotility. Digestive diseases and sciences (Dig Dis Sci ) Vol: Issue Pages: Pub: 2022 Mar 30 Epub: 2022 Mar 30 Authors Coles MJ , Masood M , Crowley MM , Hudgi A , Okereke C , Klein J , Summary
Gut Microbiota Disruption in COVID-19 or Post-COVID Illness Association with severity biomarkers: A Possible Role of Pre / Pro-biotics in manipulating microflora. Chemico-biological interactions (Chem Biol Interact ) Vol: 358 Issue Pages: 109898 Pub: 2022 May 1 Epub: 2022 Mar 21 Authors Alharbi KS , Singh Y , Hassan Almalki W , Rawat S , Afzal O , Alfawaz Altamimi AS , Kazmi I , Al-Abbasi FA , Alzarea SI , Singh SK , Bhatt S , Chellappan DK , Dua K , Gupta G , Summary
The significance of the gut microbiome in post-COVID-19 gastrointestinal symptoms. Clinical medicine (London, England) (Clin Med (Lond) ) Vol: 22 Issue 2 Pages: 189-190 Pub: 2022 Mar Epub: Authors Lampejo T , Summary
Integrated analysis of gut microbiome and host immune responses in COVID-19. Frontiers of medicine (Front Med ) Vol: 16 Issue 2 Pages: 263-275 Pub: 2022 Apr Epub: 2022 Mar 8 Authors Xu X , Zhang W , Guo M , Xiao C , Fu Z , Yu S , Jiang L , Wang S , Ling Y , Liu F , Tan Y , Chen S , Summary
Respiratory dysfunction three months after severe COVID-19 is associated with gut microbiota alterations. Journal of internal medicine (J Intern Med ) Vol: 291 Issue 6 Pages: 801-812 Pub: 2022 Jun Epub: 2022 Mar 17 Authors Vestad B , Ueland T , Lerum TV , Dahl TB , Holm K , Barratt-Due A , Kåsine T , Dyrhol-Riise AM , Stiksrud B , Tonby K , Hoel H , Olsen IC , Henriksen KN , Tveita A , Manotheepan R , Haugli M , Eiken R , Berg Å , Halvorsen B , Lekva T , Ranheim T , Michelsen AE , Kildal AB , Johannessen A , Thoresen L , Skudal H , Kittang BR , Olsen RB , Ystrøm CM , Skei NV , Hannula R , Aballi S , Kvåle R , Skjønsberg OH , Aukrust P , Hov JR , Trøseid M , NOR-Solidarity study group. , Summary
Gut Microbiome Alterations in COVID-19. Genomics, proteomics & bioinformatics (Genomics Proteomics Bioinformatics ) Vol: Issue Pages: Pub: 2021 Sep 21 Epub: 2021 Sep 21 Authors Zuo T , Wu X , Wen W , Lan P , Summary
This sample reminds me of an earlier sample that was similar frustratingly normal looking despite the person having significant issues. That person went with the suggestions that I could muster for 2 months and then did another sample. His symptoms improved slightly ANDthe microbiome because usefully abnormal. I am hoping that will be the case with this person.
In terms of mathematic models, the person’s microbiome seems to be on an infection point. The diagram below illustrates this concept with the blue line indicating recovery.
Back Story
I’m 33 years old and I have been sick for my last 12 years.
I suffer from:
Multiple chemical sensitivity,
Gut issues,
Severe insomnia,
Loss of collagen in joints and muscle
along many others.
The 1000 doctors that I have visited in Spain never had much idea.
The OAT test says bad methylation but i don’t know how to interpreted it or what to do, nor my doctors.
I’ve already doing all the basics, no gluten, cow dairy, processed foods etc.
I can’t eat much but I eat fish, meat and some very cooked tomato and cauliflower.
I was diagnosed with Giardia but it was not treated because I did not have diarrhea or constipation.
I feared the antibiotics causing candida issues. In other test more recent didnt show up but i think was another method of testing
Analysis
See the YouTube for more information and walk thru. Note: Giardia has a high incidence of evolving into chronic microbiome dysfunction (treated or untreated), see this post.
Using Health Analysis Page
Health Status – 1 Healthy, 7 Unhealthy
Jason Hawrelak – at 99%ile , no significant issues
Potential Medical Conditions showed only hypersomnia, the opposite of what is being experienced
I am finding that this is a friendly start point because we have multiple logics available to determine them (which, of course, can result in disagreement). To my surprise, nothing showed up – it appears that the collection of bacteria where outside of expected/supported species! (I spent a couple of hours verifying that if was not a coding error). Similar for using symptoms with KEGG Enzymes. This was totally unexpected and a little concerning (both in terms of this person’s microbiome as well as what the site is able to handle). Fortunately, we have the other logic that produces results
The top probiotic suggestions in my view are just two:
lactobacillus bulgaricus (probiotics) – typically in many yogurt. NOTE: Mutaflor and this should NOT be taken at the same time, they are hostile to each other. Alternate each one week )
Consensus Report
As has become my custom, I whipped thru all of the suggestions using expert criteria.
Percentile in top or bottom 10%ile – 134 matches (18%)
Looking at the consensus number of suggestions for the above, the numbers were similar, suggesting that despite the differences number of bacteria selected, the suggestions were likely similar.
Number of suggests from best take to worst avoid (139, 53, 40, 116, 25, 63)
The land of Supplements
We only have consensus report producing examples. There was very few items that occurred in more than 1 or 2 suggestions. The best of a poor situation were:
In general, the rest of vitamins and minerals were too close to come to a conclusion for. In that situation, I would suggest avoiding instead of rolling dice.
Supplemental Information
The reader also provided an OATS test done by Teletest Lab Analisis(laboratory@teletest.es) in Spain (and in Spanish). Abnormal values were (with links to Spanish Wikipedia)
I’ve been prescribed rifaximin + boulardii based on symptoms only. Ive been told is.”” Good antibiotic””
Feedback
Rifaximin is on the top of suggested antibiotics!! A lovely agreement….
We were not as lucky with saccharomyces boulardii (probiotics) which has a 1:3 ratio between take and avoid. I would suggest doing Rifaximin without the boulardii, after the course is finished — give it a try in isolation. Doing both at the same time will generate confusion over the cause of improvement or deterioration. As always, discuss with your MD before doing.
Bad methylation
This was reported from the oats test. “The OAT assesses organic acid markers which indicate methylation status through the crucial cofactors ie B12, folate B9, B6. One of the most sensitive markers for vitamin B12 deficiency is methylmalonic acid and kynurenate is a reliable marker for B6 status.” [Src]
Few medical professionals are aware of the microbiome side-effects of the medications they prescribe. As a result of exchanges with a user about to be prescribed antibiotics based on a positive Lyme test, I created here 2 pages intended for you to share with your Medical Professional.
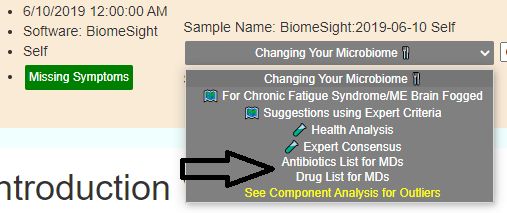
Where the new pages are located
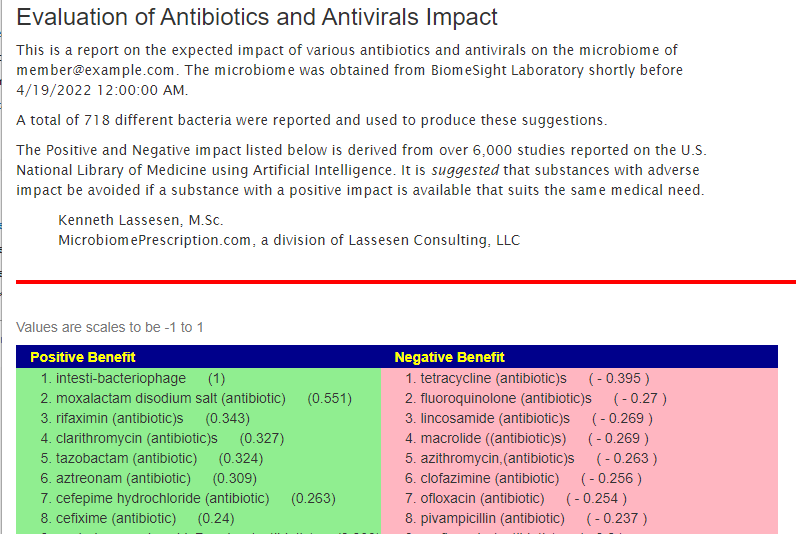
The Antibiotic Page
What the Antibiotics Page looks like.
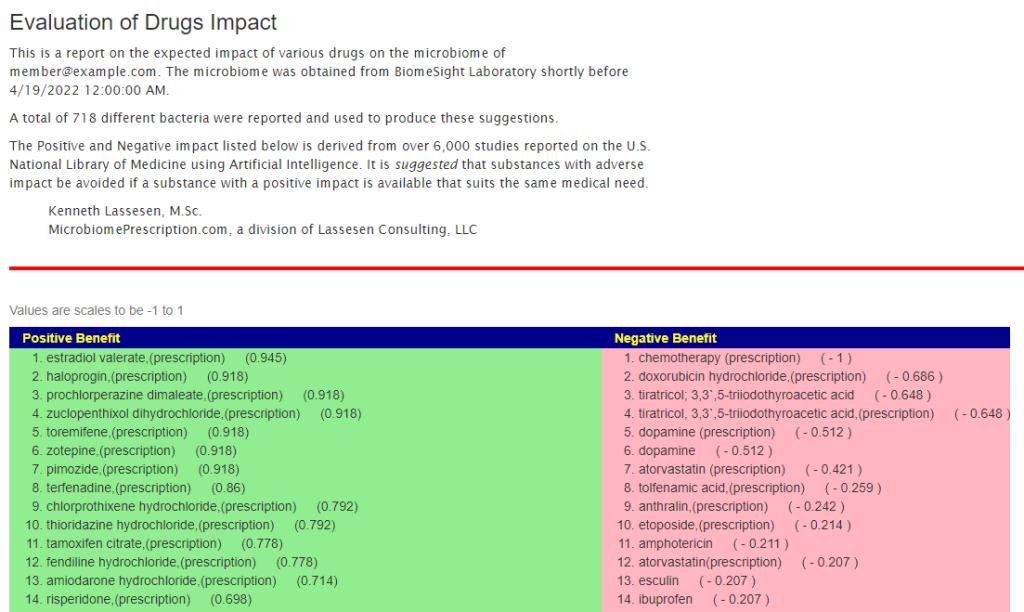
Drugs Page
The list of drugs for which we have available data.
Today I had a long Zoom call with someone that we hope to cooperate with for Long COVID. She mentioned that one species of probiotics works very well for some people with long COVID and it’s sibling do not. I explained that my working hypothesis is that a lot of interactions depends on the enzymes.
This resulted in us doing a quick lookup experiment using Microbiome Prescription databases.
In theory, the 13 items above may be excellent candidates for novel pharmaceuticals to be trialed for treating long COVID.
This same approach may be done with other conditions and probiotics. By trials identify which probiotics have the most impact, use the same approach to identify possible enzymes causing the difference, then do a clinical trial.


 Have you seen it anywhere? Also how would one figure out the dose for gut bacteria shifting?
Have you seen it anywhere? Also how would one figure out the dose for gut bacteria shifting? …I also have prescript on hand BUT that has a lot of other SBO strains. Would you stuck to TERRAflora for now?
…I also have prescript on hand BUT that has a lot of other SBO strains. Would you stuck to TERRAflora for now? 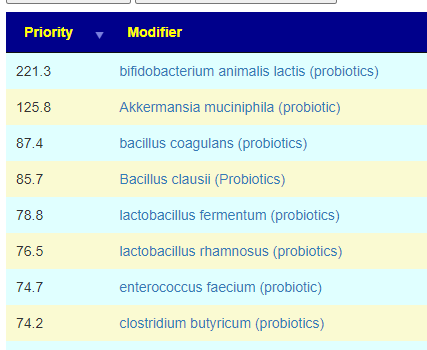
Recent Comments