A reader reached out for an educational review of their 16s microbiome results. I usually try to make time to do an education review once a fortnight unless I am deep in coding or analysis issues. He provided a nice very detailed back story, which is verbatim below
My problem started out approaching eight years ago when I went on a ketogenic diet. I had a massive energy collapse and weight loss (I was not overweight at the start), and I incorrectly believed this was about insufficient calories rather than macronutrients.
It turns out I have some uncommon genetics that make my ability to process fats for energy inefficient, under conditions of severe catabolic stress. Severe catabolic stress would be conditions like starvation, high fever, etc. Keto diet mimics starvation and is an extremely catabolic stress to the body. It looks like this diet was a suicide diet for me, and it started a set of symptoms that are persistent even after reverting to a higher carb diet.
The original symptoms were like CFS, but I have since been able to correct most of those by going to a higher carb diet, mostly using lower-glycemic whole food carbs like lentils, fruit, and vegetables. This took about three years to figure out and I think some infections may have exploited the period of low energy. Those infections may include dysbiosis as well as possibly some kind of brain infection.
During the first month of the diet I had some “event” where I tried to correct the energy collapse with a higher level of exercise, and after one high-intensity running session I spent the entire night drinking a liter of water every hour. I was desperately thirsty and was unable to quench the thirst.The high levels of water probably induced an electrolyte imbalance, further aggravating the underlying cause. I should have made a trip to the emergency room, but I did not. After that one night I started with a tinnitus that has been with me 24×7 for approaching eight years. At first that tinnitus was like something at the brain core activating and literally consuming consciousness. That has improved over time and in the last year feels like it could become just a sound at some point soon. Together with the tinnitus I have some irritation of my optical nerve that gets worse when the tinnitus gets worse. These problems are severe and constant, and I cannot survive the stress of employment with such severe stressors on my brain.
It is worth mentioning that I was an entrepreneur for more than 10 years, working 14+ hour days. So I am the opposite of lazy. I had lifelong IBS-D, which is now well controlled, and most of that IBS I attribute to gluten and to dairy. I am gluten free, and now I get my only dairy exposure from carefully prepared yogurt.
I have neurological symptoms of brain fog (along with tinnutus) tied to food. About 60 to 90 minutes after eating the symptoms begin. I have multiple SIBO tests, that show an ongoing set of issues. My first SIBO test had enormous levels of background methane. My practitioner treated this as a colonic issue and we corrected that completely. My next SIBO test showed completely flat-line hydrogen and methane, a hydrogen sulfide (H2S) SIBO. I went on a heavy yogurt diet and that improved my symptoms. I stopped the yogurt, but when I repeated a SIBO test using the Trio test, it showed totally normally hydrogen, methane, and H2S. So I cured the SIBO. I have organic acid markers suggesting SIFO, and since I still have neurological issues after eating, we will start to treat for SIFO soon.
In terms of microbiome testing, the main trend I perceive here is:
? I started with 18% butyrate producers. I corrected this by a heavy diet of prebiotics including GOS, PHGG, and Acacia. Butyrate producers are now close to 40%.
? I have near extinction levels of Bifidobacterium and Lactobacillus. This I attribute to both antibiotics as well as not eating dairy foods for 20 years. I simply starved these genera out of existence. I do not tolerate Lactobacillus supplements or foods. They induce huge levels of brain fog. I am currently making a Bifido only yogurt that I load with prebiotics, and this has been extremely helpful to my health. The dairy is being completely tolerated, which I suspect is because I have thriving Bifido populations eating the lactose all the way through digestion.
? I have low and inconsistent levels of Faecalibacterium prausnitzii which is a key species I have identified that is almost universally associated with good health. I am addressing this by taking stewed apples as my main breakfast meal each morning. Pectin feeds this bacteria.
? I have low levels of Akkermansia, suggesting possible problems with my mucosal layer. I test with very low secretory IgA and somewhat leaky gut, so these might confirm a mucosal layer issue. I am trying to correct this with Bacillus coagulans, which gave me some success in earlier trials.
? I have slight elevations of methanogens and H2S producers. Biomesight and Thryve disagree about which species are present. I feel my best strategy for keeping these controlled is to focus on enhancing butyrate producers and trying to re-establish my acetate producers.
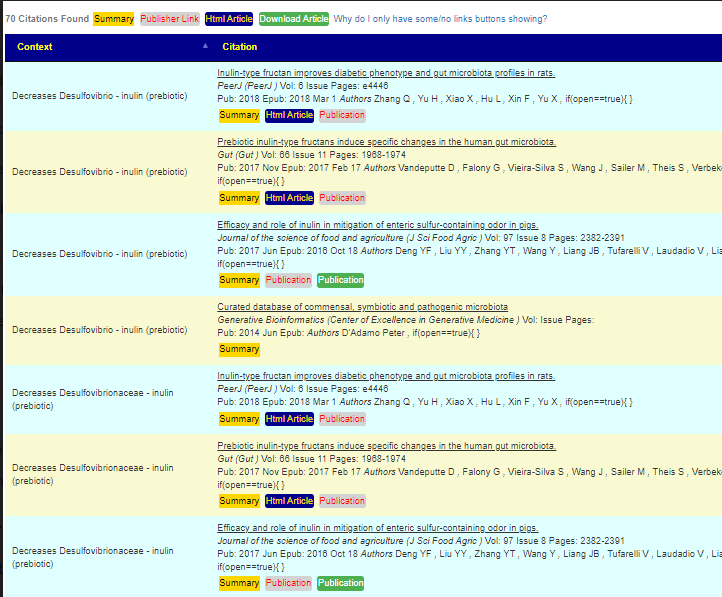
? My Proteobacteria are usually under 4% but I seem to have a large population of Sutterella wadsworthensis, always over 1%. This bacteria is worth calling out because we are measuring levels in the colon with 16s testing, and the research says this bacteria gets more dense as you travel up the small intestine. So I may have a fair amount of it in my duodenum. Since it is a gram negative bacteria, there might be some LPS issues. I plan to treat this with the yogurt.As far as brain infection, this is unfortunately something for which good tests do not exist. I do show significant volume loss in my brain, confirmed by a radiologist on the MRI as well as by software that analyzes brain volume from those images. The severity of my neurological symptoms does seem consistent with some viral load that may have been pre-existing, and that simply exploited a number of years of low energy. There is a really interesting study out of Japan in the last few years where they treated people who had certain viruses with anti-virals and followed them for years after that. Treating with anti-virals effectively eradicated all risk of Alzheimer’s in later years, strongly suggesting a cause and effect between resident viral infection and neurodegeneration. This establishes some credibility for the hypothesis. At some point I may try to find a specialist and do some test around anti-virals to see if that affects symptoms.
My first impressions
One item stood out greatly in his story, the parallelism to what is seen with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Let me document out some of the parallelisms, I will cite just one publication for each:
- Volume loss in brain: “The outcomes from the articles include changes in gray and white matter volumes, cerebral blood flow, brain structure, sleep, EEG activity, functional connectivity and cognitive function.” A systematic review of neurological impairments in myalgic encephalomyelitis/ chronic fatigue syndrome using neuroimaging techniques.Maksoud R, du Preez S, Eaton-Fitch N, Thapaliya K, Barnden L, Cabanas H, Staines D, Marshall-Gradisnik S.PLoS One. 2020 Apr 30;15(4):e0232475. doi: 10.1371/journal.pone.0232475. eCollection 2020.
- Tinnitus (hyperacusis): “Posttraumatic stress disorder, chronic fatigue syndrome, generalized anxiety disorder, depression, exhaustion, fibromyalgia, irritable bowel syndrome, migraine, hearing impairment, tinnitus, and back/joint/muscle disorders were comorbid with hyperacusis. ” Characteristics of hyperacusis in the general population.Paulin J, Andersson L, Nordin S.Noise Health. 2016 Jul-Aug;18(83):178-84. doi: 10.4103/1463-1741.189244.
- Optical nerve that gets worse when the tinnitus gets worse: Restricted Spatial Windows of Visibility in Myalgic Encephalomyelitis (ME).Ahmed NS, Gottlob I, Proudlock FA, Hutchinson CV.Vision (Basel). 2018 Jan 17;2(1):2. doi: 10.3390/vision2010002.
- I do not tolerate Lactobacillus supplements or foods. They induce huge levels of brain fog: See Examining clinical similarities between myalgic encephalomyelitis/chronic fatigue syndrome and D-lactic acidosis: a systematic review [2017]
He eliminated sufficient ME/CFS symptoms to likely not qualify for that diagnosis.
Ketogenic diet Literature
As usual, I go for gold-standard information from the US National Library of Medicine instead of internet rumor and snake-oil cure-alls. There are over 3800 studies. There medical cases when it is used with success (i.e. Epilepsy, Parkinson, Alzheimer’s diseases), but many of the studies have been with mice or with an apparent bias for positive results. Despite this, there was a good number of studies indicating general risks and complications. I have just cited a few studies from 2020 onwards, studies not available when this person made a regretted choice.
- “In all, 21 % of patients under modified Atkins diet had unfavorable effects, while 52.63 % of patients on classic ketogenic diet had complications” [2021]
- Commentary: Consumer Reports of “Keto Flu” Associated With the Ketogenic Diet.Sáenz de Pipaón M, Flores-Rojas K, Gil A, Gil-Campos M.Front Nutr. 2020 Sep 4;7:113. doi: 10.3389/fnut.2020.00113. eCollection 2020. – I smile because ME/CFS was called “Yuppie Flu” once upon a time.
- Acute Ketogenic Diet and Ketone Ester Supplementation Impairs Race Walk Performance.Whitfield J, Burke LM, McKay AKA, Heikura IA, Hall R, Fensham N, Sharma AP.Med Sci Sports Exerc. 2021 Apr 1;53(4):776-784. doi: 10.1249/MSS.0000000000002517.
- Alterations in the gut microbiota contribute to cognitive impairment induced by the ketogenic diet and hypoxia.Olson CA, Iñiguez AJ, Yang GE, Fang P, Pronovost GN, Jameson KG, Rendon TK, Paramo J, Barlow JT, Ismagilov RF, Hsiao EY. Cell Host Microbe. 2021 Sep 8;29(9):1378-1392.e6. doi: 10.1016/j.chom.2021.07.004. Epub 2021 Aug 5.
- Ketogenic Diet Suppressed T-Regulatory Cells and Promoted Cardiac Fibrosis via Reducing Mitochondria-Associated Membranes and Inhibiting Mitochondrial Function.Tao J, Chen H, Wang YJ, Qiu JX, Meng QQ, Zou RJ, Li L, Huang JG, Zhao ZK, Huang YL, Zhang HF, Zheng JM.Oxid Med Cell Longev. 2021 Apr 19;2021:5512322. doi: 10.1155/2021/5512322. eCollection 2021.
- Ketogenic diet aggravates hypertension via NF-kappaB-mediated endothelial dysfunction in spontaneously hypertensive rats.Guo Y, Wang X, Jia P, You Y, Cheng Y, Deng H, Luo S, Huang B.Life Sci. 2020 Oct 1;258:118124. doi: 10.1016/j.lfs.2020.118124. Epub 2020 Jul 21.
- An overlooked danger of ketogenic diets: Making the case that ketone bodies induce vascular damage by the same mechanisms as glucose.Burkitt MJ.Nutrition. 2020 Jul-Aug;75-76:110763. doi: 10.1016/j.nut.2020.110763. Epub 2020 Feb 14.
- Effects of a Ketogenic Diet on Muscle Fatigue in Healthy, Young, Normal-Weight Women: A Randomized Controlled Feeding Trial.Sjödin A, Hellström F, Sehlstedt E, Svensson M, Burén J.Nutrients. 2020 Mar 30;12(4):955. doi: 10.3390/nu12040955. “We conclude that in young and healthy women, a ketogenic LCHF diet has an unfavorable effect on muscle fatigue”
Clearly there are frequent downsides (beyond having DNA issues) that are not declared by advocates.
Testing Predictions
In my recent blog post, Predicted Symptoms – Performance Review, we found at least 50% of symptoms were correctly predicted using either KEGG Products or the Bacteria. This is a fresh test case sample. I forwarded the top 20 symptoms from these two predictors to the reader and he reported back. Results are below with the prediction engine reaching 60%.
| Symptom | Z-Score | Reader Comment |
| Comorbid-Mouth: Periradicular periodontitis inflammatory / chronic lesion around roots of teeth | 3.71 | I have now-well-controlled significant erosion of the gums. It is not reversing but is hopefully not getting rapidly worse. |
| Comorbid: Small intestinal bacterial overgrowth (SIBO) | 3.35 | I apparently treated it and it no longer exists. |
| Post-exertional malaise: Worsening of symptoms after mild mental activity | 3.32 | Reading and focusing on written work quickly brings on fatigue and eye focus problems. |
| Age: 40-50 | 3.21 | 50+ |
| Autonomic Manifestations: Cortisol disorders or irregularity | 2.94 | Fasting brings on high cortisol and high fasting glucose. |
| DePaul University Fatigue Questionnaire : Tense muscles | 2.92 | Tense in general, not just muscles |
| Symptom | Z-Score | Reader Comment |
| Physical: Work-Sitting | 1.86 | ☑️ |
| Physical: Northern European | 1.82 | ☑️ |
| DePaul University Fatigue Questionnaire : Need to nap during each day | 1.77 | ☑️ |
| Neuroendocrine Manifestations: Poor gut motility | 1.65 | 3.5 hour transit time through small intestine |
| Infection: Varicella Zoster Virus | 1.62 | I had chicken pox as a child. Both parents had shingles. |
| Comorbid: Sugars cause sleep or cognitive issues | 1.53 | ☑️ |
| Physical: Long term (chronic) stress | 1.49 | ☑️ |
| DePaul University Fatigue Questionnaire : Ringing in the Ear | 1.44 | 24×7 tinnitus that varies from bad to horrific |
| DePaul University Fatigue Questionnaire : Abnormal sensitivity to light | 1.41 | ☑️ |
| Neuroendocrine: Cold limbs (e.g. arms, legs hands) | 1.4 | Particularly in the feet, I have poor circulation |
| Post-exertional malaise: Worsening of symptoms after mild mental activity | 1.3 | Reading and focusing on written work quickly brings on fatigue and eye focus problems. |
| Immune Manifestations: Chronic Flatus / Flatulence / gas | 1.27 | ☑️ |
Some of the agreements were interesting, especially for Varicella Zoster Virus. The person does not have active, but we know because of Shingles that the virus persists. If the virus persists, then it will do some ‘taxonomy-forming’ of the gut to be friendly to it. I hope this person has gotten a Shingles Vaccinations.
My Approach
I will start by using some citizen science patterns from Microbiome Prescription. Specifically
- Neurological-Audio: Tinnitus (ringing in ear) – 267 in that cohort
- Neurocognitive: Unable to focus vision and/or attention – 240 in that cohort
As well as US Library of Medicine:
- Irritable Bowel Syndrome
- ME/CFS with IBS
- Obsessive-compulsive disorder – while not diagnosed with it, it was a prediction that he agreed with
I will do a consensus report from the collection of suggestions for the 5 items cited above. I picked the largest cohort to get the best precision.
Second, I will clear the consensus report and do a naive consensus report with just the Kaltoft-Moltrup outliers and Dr. Jason Hawrelak. As with most of these educational reviews, I will often explore different paths for analysis.
Third, I will clear the consensus report and do all 15 prediction matches. I will leave it to the reader to do an uber consensus approach of everything together, including these items connected to vision:
First Pass
This is a revision based on the revised algorithms Suggestions from Symptoms are Changed.
Neurocognitive: Unable to focus vision and/or attention
We actually ended up with 100 “Safest Takes”
Second Pass
| Bacteria Name | Analysis |
| Akkermansia | Too Low |
| Bacteroides | Too High |
| Bacteroidia | Too High |
| Bifidobacterium | Too Low |
| Faecalibacterium prausnitzii | Too Low |
| Methanobrevibacter | Too High |
| Proteobacteria | Too High |
| Bacteria Name | Analysis |
|---|---|
| [Ruminococcus] torques | Too Low |
| Aggregatibacter | Too High |
| Blautia hydrogenotrophica | Too Low |
| Chlorobaculum | Too Low |
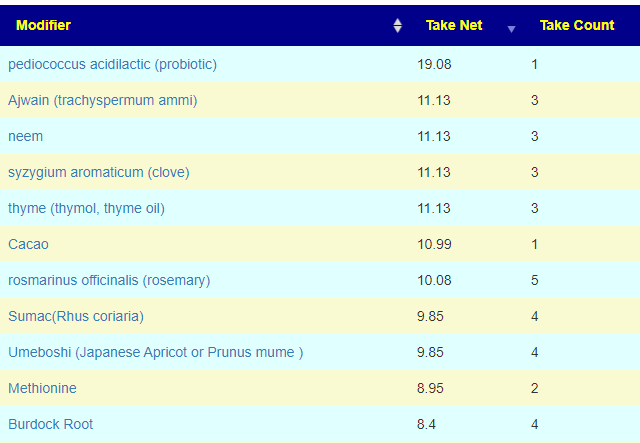
To confirm Kaltoft-Moltrup Ranges, I did a visual scan of his results, and there were no other extreme items. The default result was only 9 items on all lists, and they were only for Safest takes as shown below

Dropping the cut off point to 2 (from the default 3) increased the count to 18, with the items below added
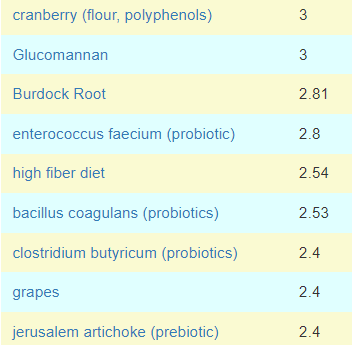
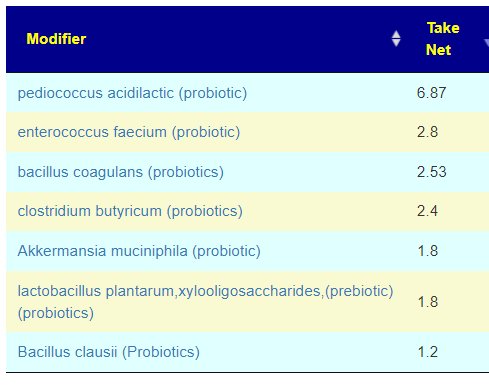
It is interesting to note that we have 3 probiotics listed, none of them are Lactobacillus — the specific type that the reader reported severe issues with. Dropping the filter point to 1 (from default 3) we end up with 47 items and filtering to probiotics, we have the list below. A Lactobacillus showed up but only in combination with a prebiotic. Decreasing further, we see the following added next: bifidobacterium infantis,(probiotics), bifidobacterium longum bb536 (probiotics), bifidobacterium catenulatum,(probiotics)
Third Pass
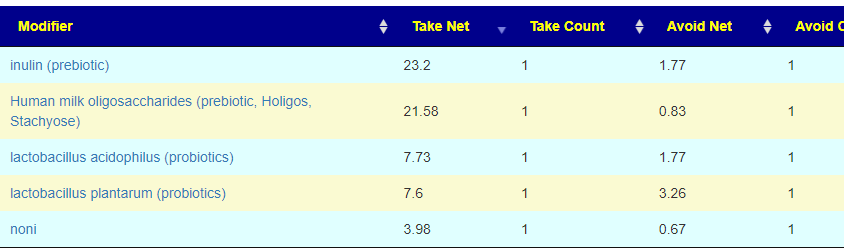
This may seem to be a lot of work, but you can see that it may be done quickly from the YouTube video for this post. Note that we are doing only Bacteria (KEGG Products are too indirect to get suggestions). Remember that we did 12 sets of suggestions so the “Take Count” should be a matter of interest.
This is a revision based on the revised algorithms Suggestions from Symptoms are Changed. I only did the auto checked items. The second level suggestions were not checked.
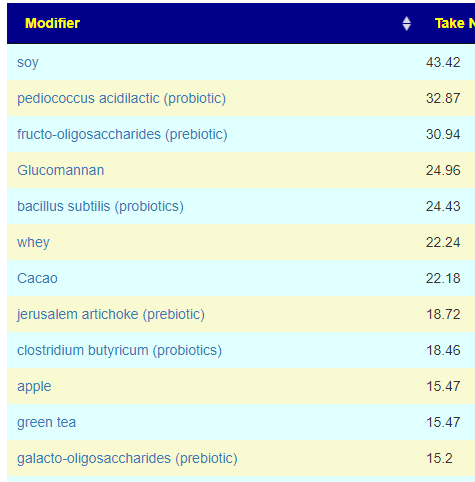

I notices that many SAFEST items are in agreement with our first pass, i.e. Cacao, pediococcus acidilactic (probiotic), thyme (thymol, thyme oil). A few items, like clove are on the avoid list but the avoid came from a single suggestion.
KEGG Suggestions
This obtains suggestions using genes and is independent of the the above processes, all of suggestions had a very low weight of 2 (often we see numbers of 200-300), so these are likely weak suggestions, with the three best candidates below (any one of them is likely sufficient)
For supplements, only L-Cysteine appears (which was on the bottom of the list in our First Pass)
Putting it all together
In terms of probiotics, Bifidobacterium longum or bifidobacterium animalis lactis, symbioflor 2 e.coli probiotics, enterococcus faecium (probiotic), bacillus subtilis (probiotics) and Akkermansia muciniphila (probiotic) appears to be preferred set — especially any that are not currently being taken.
I personally would advocate symbioflor 2 e.coli probiotics, (or Mutaflor) – because E.Coli probiotics appeared to make a major impact on reducing the time to recover for my own relapses/
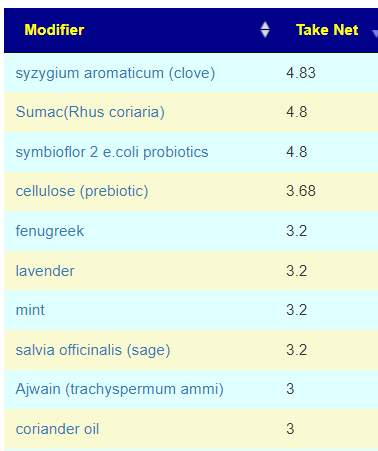
I noticed what seems to be more than normal of polyphenols, herbs and spices. This is apparent on the third pass safest list and also second pass safest list but not on the first pass. I am inclined to ignore the first pass list for several: small number of bacteria in scope, symptoms and medical conditions were ignored.
Below you will find a YouTube of the analysis with additional commentary.
Reader feedback
“Your studies under Keto literature raise the possibility that a high fat diet may have exploded my levels of B wadsworthia during the active keto diet phase, and this alone may have promoted most of my brain fog. That’s an interesting hypothesis I had not considered. “
“On the various suggestions lists, do I understand that AI is not able to give us reasons for the suggestion, but rather it is just making associations between suggestions and reversal of symptoms that have been studied? ” INCORRECT, for the professional user, I detailed out the evidence as shown below
“It might help to define “Take Counts”. Maybe you do that on the video. What is also confusing is that on the Safer Takes list you have a “Take Net” and it is not clear how it is calculated.” The calculation something like this:
SUM( For each Bacteria (Magnitude of Shift desired + Function(Number of studies shifting in the right direction, Number of studies shifting in the wrong direction))
- so substance with only a few (or just one) study for a bacteria will have a lower number
- so substance with many studies for a bacteria will have a higher number
- a bacteria that is slight off will have a lower number
- a bacteria that is very off will have a higher number
The actual computational functions are proprietary and the results of 3 years of experiments.
“it is confusing because the same genus Bacteroides is alternately Too Low and then Too High.” There are THREE reference point the highs, the lows and the middle peaks (used for symptoms). People with a specific symptom may average at 35% of the median, so the goal is to shift you away from the 35% area. This it becomes a question of which direction? I made an “arbitrary” decision that if you are > 35% then we want to push you higher. If you are < 35%, we want to push you lower (ideally keeping you within the Kaltoft-Moltrup range of normal values). There is logic behind this “arbitrary” decision, but explaining it is complex.
Some Facebook comments
Recent Comments