Back Story
In 2021, at age 28, I developed an upper respiratory infection while working in a hospital (tested negative for Covid repeatedly). The URI persisted for over a week so I was prescribed a course of Augmentin thinking it might be a sinus infection. On day two of antibiotics, brain fog, headache, orthostatic intolerance, and fatigue began and never went away. I would go on to develop PEM and sleep disturbances and I was eventually diagnosed with ME in 2023.
I have two tests that have been uploaded. The first is from 2023, at which point I was Mild/moderate and still had some bfido/lacto left but was also dealing with a dysbiosis. The second is from 2024 and am now very severe. Probably unsurprisingly, I have had a decrease in levels of desired bacteria and also changes in the dysbiosis.
There seems to be conflicting suggestions between new UI and the cross validated items to add. If I was considering an antibiotic for example, the new IU weights specific floroquinolones highly and lists macrolides as items to aovid, while the cross validated suggestions say to add specific macrolides. Diet styles and some specific supplements also seem to conflict. What do you recommend when there are conflicting suggestions between the two?
Additionally, within the new UIs suggestions,
the individual probiotics in items to add list list don’t always match the recommended probiotic products. (Ex. L. Sakei and L. Hellveticus are listed under to avoid/decrease column, but are also listed in the commercial probiotics section with a relatively high weight.)
I am wondering if you can help me better understand the specific bacteria that have changed as my ME had gotten worse, how to potentially optimize them, which suggestions to follow, and how I might apply all that to Dr. Jadin’s protocol?
I apologize for my lack of understanding and for all that you’ve already explained and that I’ve missed. I’ve spent a lot a time on your site but am very limited in what I can do and process at the moment and want to make sure I’m approaching this the right way.
You have my permission to use the above information for a blog post.
Review of Concerns
Microbiome Prescription does best efforts and without dedicated staff to do checking — a variety of errors can occur. I depend on people like the above person to ask questions.
Conflicting Suggestions
Above there is the subjective report of getting worse, this is objectively seen with predictive symptoms where the number exploded and the agreement with self-reported was significant
| 2023-01-23 | 2024-11-23 |
 |  |
The first question is which methods were used in both the simple UI and the old UI. Different choices result in different suggestions. Suggestions are based on which bacteria were selected to be significant and the type of modifiers. You can get some items flipping from take to avoid with different choices. No one knows the right way to select which bacteria and their significance. Microbiome Prescription tries to give a variety of choices (so people can follow their beliefs on what is significant).
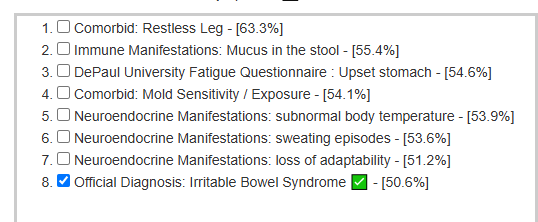
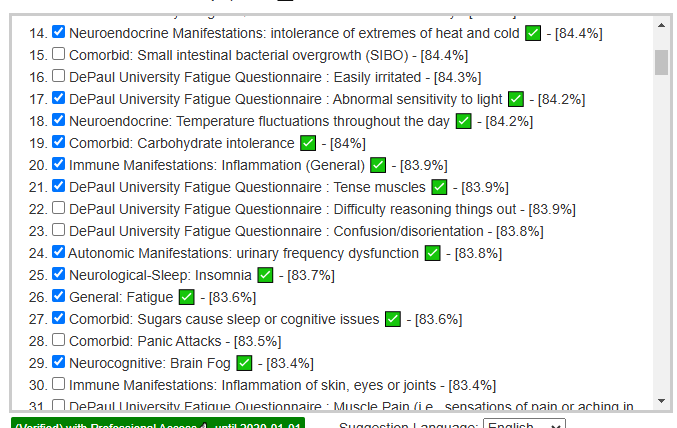
For the New UI suggestions, I will use: Beginner-Symptoms: Select bacteria connected with symptoms . Despite the large number of symptoms, we ended up selecting only 24 taxa, with 12 genus being significant:
The suggestions are below
Old UI
The old UI gives many different ways of getting suggestions. These choices allow users to follow their beliefs for better or worse. A few choices are below
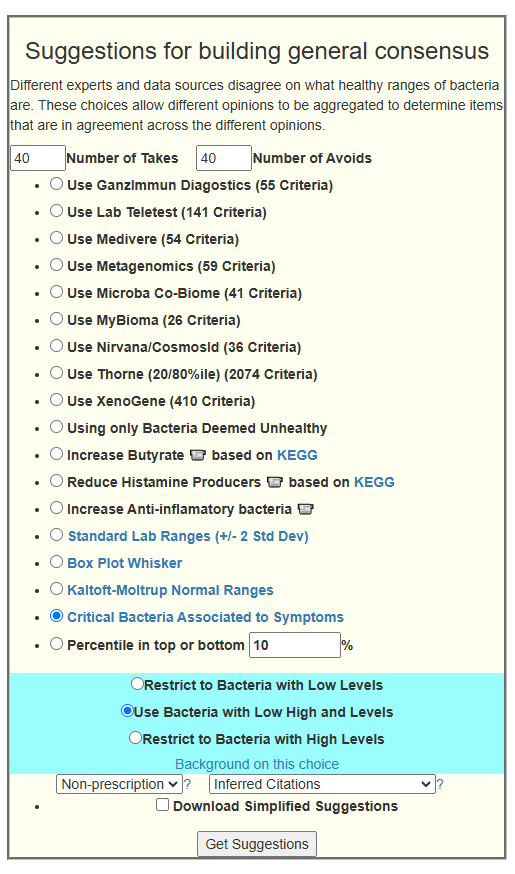
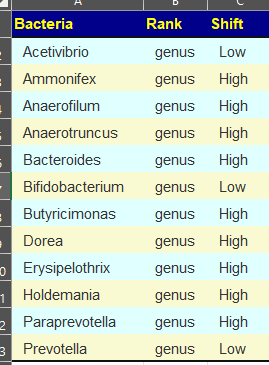
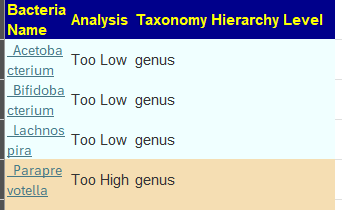
I tried Critical Bacteria Associated to Symptoms. This seems to be the closest equivalent to the Simple UI. We got just 16 bacteria selected with only 4 genus. 1/3 of what we got above. Why? When I wrote the Simple UI, I incorporated a different way of weighting and filtering bacteria as a result of more recent research and observations. Also, I also incorporate multiple algorithms in the Simple UI (which is why it takes much longer to get suggestions).
I checked the top few items from the Simple UI and they were on this to take list, just with a lower value. The additional bacteria shifted the order.
Q: Why did I not revise to make them agree?
- Answer: I do not know which is the best. I intentionally avoid changing algorithms that have been in use for any time (unless there is a gross error). When I did that in the past, I got a flood of email asking for explanations. The Simple UI captures my best current thinking when I added it.
Probiotics Question
From the Beginner-Symptoms: Select bacteria connected with symptoms we have

Looking at the KEGG computations on the Simple UI we have those on the KEGG Compound / Enzymes Lists Suggestions
- aor / probiotic-3 at 45 / 107
- bioflorin (deu) / bioflorin at 41 / 86
- mwsb / candida yeast support at 44 / 105
- Pendulum / Pendulum Glucose Control at 40.6 / 90.6
- miyarisan (jp) / miyarisan at 46 / 115
We have apparent good agreement.
Looking at Critical Bacteria Associated to Symptoms suggestions, we see a short list
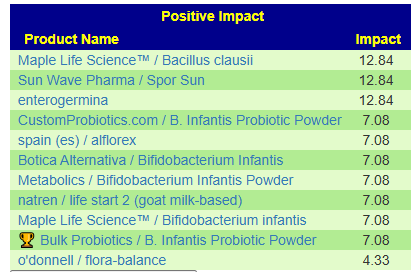
Looking at the KEGG computations on the Simple UI we have those on the KEGG Compound / Enzymes Lists Suggestions
- Maple Life Science™ / Bacillus clausii – 50 /122
- Maple Life Science™ / Bifidobacterium infantis – 38 //75
- o’donnell / flora-balance – 45 / 105
Bottom Line for Probiotics
I do not see either L. Sakei and L. Helvetius in the above list, so I will assume that a different filter was used to get them.
Antibiotic Question
Unlike probiotics, we do not have 2 additional scales to evaluate suggestions (i.e. KEGG Compounds and KEGG Enzymes)
Simple Suggestions
The — numbers below are from the OLD UI
- Floxacin family
- norfloxacin — 0.056
- ciprofloxacin [CFS] — 0.053
- ofloxacin — 0.034
- sparfloxacin (antibiotic) — 0.023
- metronidazole [CFS]
- ornidazole
- benzylpenicillin sodium (antibiotic)
So, what we see is that with the smaller genus count, antibiotics are of a much lower value. When the other genus are added, they become more important.
Bottom Line
I wish that I was omniscient on the microbiome and how to adjust it. I am not. I have listened to people on what they believe is the right way and implemented it. For the Simple UI, I did my best attempt to compute suggestions. With the suggestions computed from PubMed studies and the suggestions computed from KEGG’s data being in general agreement (at least for the top items), I fell confident that they are reasonable. The same core algorithm was used for Suggestions Cross Validation using PubMed where we had an average of 86% agreement.
Post Script
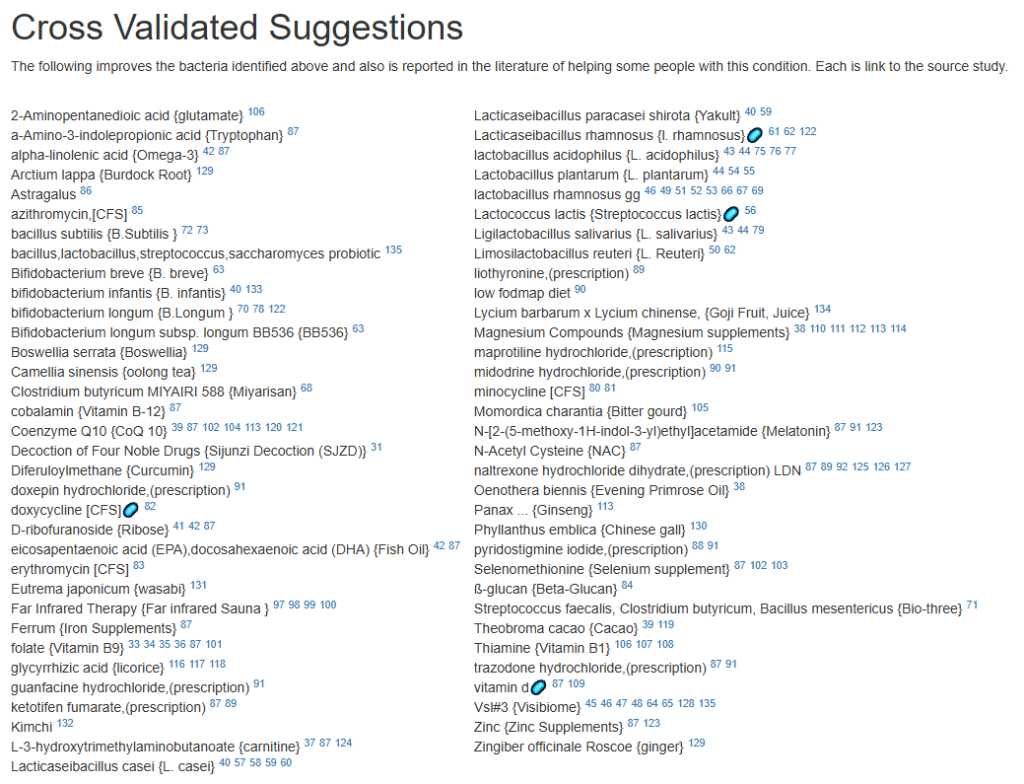
I went and used Strict PubMed Cross Validated Suggestions, with Inflammatory Bowel Disease and Chronic Fatigue Syndrome. This uses a different approach to filtering and thus different suggestions are expected.
The Genus flagged were the 8 below (midway between the 4 and 12 above):
- Bacteroides – genus : High
- Bifidobacterium – genus : Low
- Clostridium – genus : Low
- Faecalibacterium – genus : Low
- Haemophilus – genus : Low
- Lachnospira – genus : Low
- Prevotella – genus : Low
- Streptococcus – genus : Low
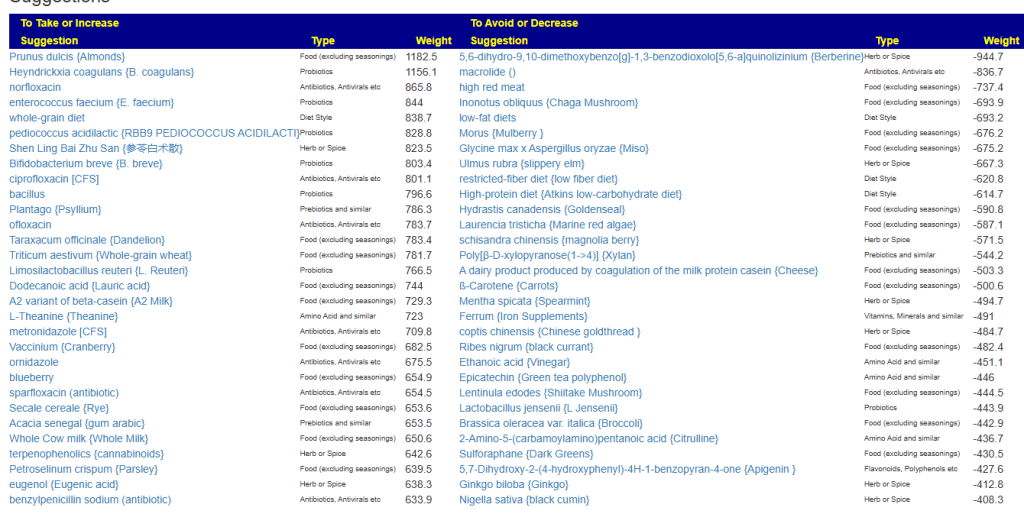
With the suggestions below (remember ONLY items showing positive effects in studies are included, items not reported in studies are excluded):
The “best” would be to use what all methods agree on. If there are conflicts, omit the items. Usually, there will be a significant list of items in agreement.
Postscript and Reminder
As a statistician with relevant degrees and professional memberships, I present data and statistical models for evaluation by medical professionals. I am not a licensed medical practitioner and must adhere to strict laws regarding the appearance of practicing medicine. My work focuses on academic models and scientific language, particularly statistics. I cannot provide direct medical advice or tell individuals what to take or avoid.My analyses aim to inform about items that statistically show better odds of improving the microbiome. All suggestions should be reviewed by a qualified medical professional before implementation. The information provided describes my logic and thinking and is not intended as personal medical advice. Always consult with your knowledgeable healthcare provider.
Implementation Strategies
- Rotate bacteria inhibitors (antibiotics, herbs, probiotics) every 1-2 weeks
- Some herbs/spices are compatible with probiotics (e.g., Wormwood with Bifidobacteria)
- Verify dosages against reliable sources or research studies, not commercial product labels. This Dosages page may help.
- There are 3 suppliers of probiotics that I prefer: Custom Probiotics , Maple Life Science™, Bulk Probiotics: see Probiotics post for why
Recent Comments