This is part of this continuing saga with this person. Prior posts and the labs shown below. Repairing the microbiome is not a single test, take a pill, and you are done. It may be like a long journey by sail through the fjords of Norway: a lot of course corrections!
- The ME/CFS Quest for Health [May 2025]
- Ongoing ME/CFS Journey [Jan 2025]
- ME/CFS Continues Improvement + Lab Read Quality Issues [Feb 2024]
- Rosacea, Circulation and mild CFS [Dec 2021]
- Update on ME/CFS Person [Sep 2023]
- Follow up Microbiome Analysis from a prior post [Apr 2022]
Person’s Summary
I would say that there is no improvement since the last test. So this is still applicable:
I have not been feeling so well lately (since the last year). I would say that my symptoms has become worse. Earlier it has always felt as I have done some progress but the last 18 months it has been the opposite. Earlier I got rid of my muscle and joint pain but it has come back and I have much bigger issues with my red nose and my body feels very stressed.
Also feel very bloated.
- A summary of my biggest issues:
- Get the red nose (some form of rosacea).
- Feel fatigued (both physically and mentally).
- Feeling stressed.
- Brain fog.
- Bloated.
- Lots of gas – I fart and burps a lot.
- Issues with allergies
- Muscle and joint pain
For the last 4-5 years I’ve been eating large amounts of rye and oats.
- Around 150-200 gram of rye bread every day.
- Around 70 gram of oats every day.
Been eating low fat, low protein and high carb (specially from rye, oats, apple juice and potatoes) because this diet seem to reduce my symptoms. As soon as I start to eat high meat and high fat my symptoms get worse.
In this analysis, I am going to look at:
- Changes since the last sample
- Review a new approach that is being incorporated
- Looking at suggestions and the difference between the new approach and the traditional approach
At the end, I suggest following the new approach with the motivation that the traditional approach has appeared to have stalled. The microbiome adapts to antibiotics and diet changes; rotation to alternatives often seems to be needed to keep destabilizing the microbiome dysbiosis.
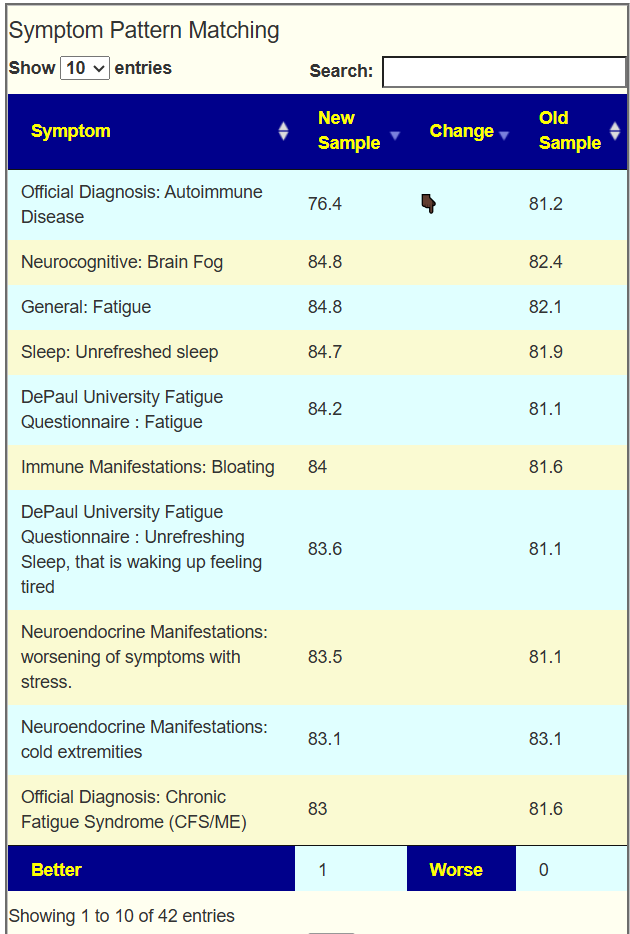
Changes Between Samples
Going to Old UI/Multiple Samples we compare symptom matching values. We see that just 1 of 42 showed improvement.
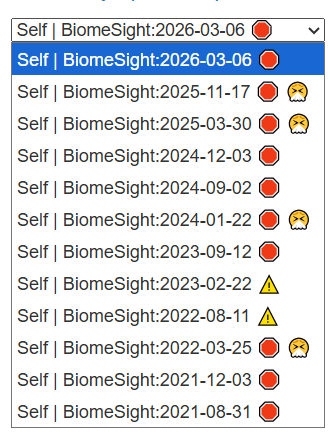
Looking at the new Odds Ratio data, we see the number of bacteria identified as critical in different samples below / Odds Estimate. I am not clear on the meaning and significance…
- Odds Estimate: The higher the number, the more likely that the person is healthy
- Number of Bacteria: Not reliable because different bacteria contribute differently to health.
- 2026-03-06: 59 / 1632
- 2025-11-17: 36 / 1588
- 2025-03-30: 20 / 1671
- 2024-12-03: 21 / 1561
- 2024-09-02: 36 / 1611
- 2024-01-22: 58 / 1586
- 2023-09-12: 38 / 678
- 2023-02-22: 52 / 1707
- 2022-08-11: 30 / 886
- 2022-03-25: 24 / 1037
- 2021-12-03: 15 / 1287
- 2021-08-31: 49 / 757
My general reading is that from 2021-2024 there was improvement and now the person is in a new stable healthier state but with still dysbiosis. I am hoping that the switch to an alternative view of solving his health may result in further improvement. In other words, rotation of approaches.
Another View on the Same Issue
In my recent post, Turning Fixing the Microbiome Upside Down!, I introduced a different way to think about repairing the microbiome. A human–society analogy might make it clearer.
Imagine your city is struggling with homelessness, vagrancy, and petty crime. The usual response—especially in the U.S.—is to send in the police. Round up those panhandling on the streets! In microbiome terms, that’s like identifying “bad bacteria” and launching an attack.
But there’s another approach: offer housing, mental health care, and job training. You don’t punish people—you help them heal and reintegrate.
Traditionally, Microbiome Prescription has focused on detecting problematic bacteria and trying to suppress or adjust them. The challenge is that most people have many interconnected symptoms. Research often shows that substance X improves one symptom but worsens another. You end up chasing symptoms—fixing one only to see another emerge or intensify.
A more holistic alternative, which has only recently become possible, is to guide the person’s microbiome toward a naturally healthy state instead. See this post: Mathematically Derived Healthy Microbiome.
Recently I asked the head of a microbiome testing company, what statistical evidence do you have for what is a healthy or desired microbiome profile. How do you obtain the importance of each bacteria? He knew that using means and standard deviation were invalid because of the high skew with the data. His response was requesting his staff to remedy this situation, looking at odds-ratio as a starting point.
Evaluation
I am a modeler, not a medical professional. Modelers try putting together mathematics using available data and use that to generate predictions. Once the predictions are made, they are evaluated against any available facts.
Above we have some observations from the person, the model does not know this information — so we can evaluate predictions against this data.
Been eating low fat, low protein and high carb (specially from rye, oats, apple juice and potatoes) because this diet seem to reduce my symptoms. As soon as I start to eat high meat and high fat my symptoms get worse.
Comparing Suggestions
| Health | Symptoms | Novice | |
| Rye | -0.11 | -183.5 | -352.3 |
| Oats | 0.15 | -179.2 | -742.6 |
| Apple | 2.34 | -385.1 | -351.5 |
| Potato | 1.32 | -1102.7 | -1418.5 |
| High Meat | 2.2 | 155.9 | 763 |
| Raw Meat | -2.78 | 105.5 | 21.2 |
| High Fat Diet | -.79 | 154.4 | -246.1 |
| high-saturated fat diet | -.35 | 96 | -291.1 |
| low-fat diet | 0.86 | 195.9 | 378.4 |
| Range of Values | -6.82 to 5.43 | -2075 to 1359 | -2296 to 1461 |
| Best to Take | Catechol {Catecholamines} | restricted-fiber diet {low fiber diet} | restricted-fiber diet {low fiber diet} |
Each of the above depends heavily on the bacteria selected and the threshold used. It is interesting to see that the new “Make Healthy” is a clear winner against his observations.
What is particularly interesting with the “Make Healthy” is that values were computed for 1,632 substances. Looking at the list os suggestions, we do not have a mass of antibiotics seen on the other lists. We are not focused on reducing bad bacteria, rather on improving the good bacteria, and letting those address the bad bacteria. The top items are below.
- Bromelain
- N-acetylneuraminic acid {Sialic acid} : a bioactive sugar involved in cell signaling, glycoproteins, glycolipids, and is abundant in the brain; it is linked to cognitive function, memory, and immune function in general mechanistic descriptions
- 1,2-dithiolane-3-pentanoic acid {a-Lipoic acid (ALA)}
- pediococcus acidilactici {P acidilactici}
- lactobacillus paragasseri {L. Paragasseri}
- Rubus fruticosus {Blackberry}
- Eutrema japonicum {wasabi}
- Cucurbita pepo {Pumpkin}
- Alkalihalobacillus clausii {Bacillus clausii }
- Faecalibacterium prausnitzii {Faecalibacterium prausnitzii}
- Capra hircus milk {Goat milk}
- 1,4-linked ß-D-xylopyranosyl {arabinoxylan}
- Gamma-Aminobutyric Acid {GABA}
- Ulmus rubra {slippery elm}
- Musa acuminata {Banana}
My impression is that this is a much friendlier set of suggestions. In fact, the bottom of the list (to avoid) are pages of antibiotics and prescription drugs.
Probiotics Exploration
There are two ways of getting probiotics:
- Using published studies on their impact. In general, each study describes one or two bacteria impacted. This results in low data
- Using the R2 Associations: This is a modelling of their impact with hundreds of bacteria impact estimated.
The new Healthy Algorithm includes R2 recommendations

We got the following suggestions
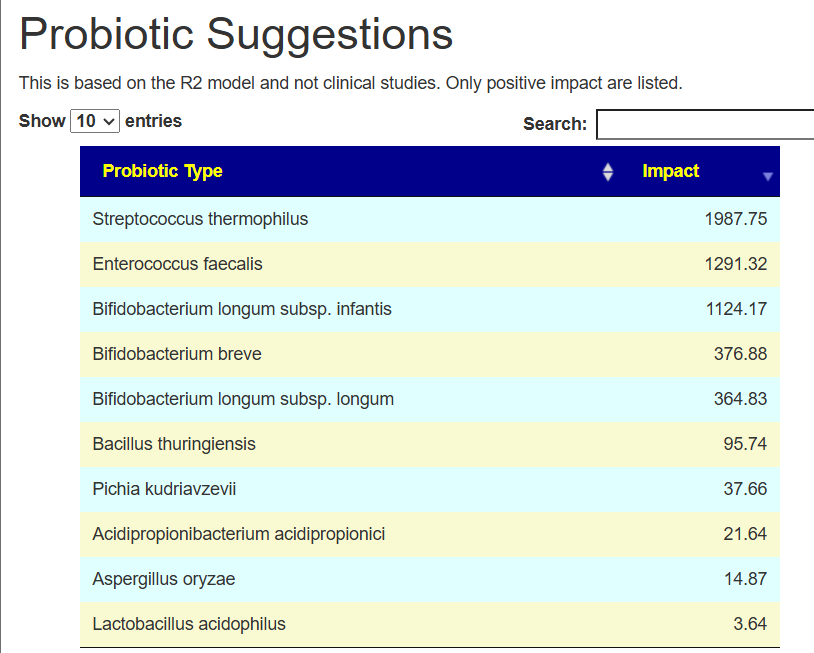
We will explore how different algorithms evaluate these.
| Bacteria | Healthy With R2 | Healthy With Studies | Symptoms With Studies | Novice with Studies |
| Streptococcus thermophilus | 1988 | -1 to 4 | -132 to -139 | -132 to -139 |
| Enterococcus faecalis | 1291 | .6 | -579 | -579 |
| Bifidobacterium infantis | 1124 | -2 | 76 | 76 |
| Bifidobacterium breve | 377 | 1 | 213 | 213 |
| Bifidobacterium longum | 365 | 1 | -1423 | -1423 |
| Bacillus thuringiensis | 96 | n/a | n/a | n/a |
| Pichia kudriavzevii | 38 | n/a | n/a | n/a |
| Acidipropionibacterium acidipropionici | 22 | n/a | n/a | n/a |
| Aspergillus oryzae | 15 | .1 – 3 | -192 to 8 | -192 to 8 |
| Lactobacillus acidophilus | 4 | 0 | -574 | -574 |
Keeping to the “When in disagreement, leave it out” a.k.a. Minimal Risk a.k.a. “Do not harm”, we have
- Top choice is Bifidobacterium breve
- Reasonable choice is Bifidobacterium infantis
Alternatively, Streptococcus thermophilus high value, cheap, and easy availability — it is a good candidate to try a 2-4 week experiment.
Personally, I would be tempted to try the following pattern (starting at a low dosage and increasing):
- 3 weeks of Streptococcus thermophilus (up to 10 BCFU)
- 2 weeks of Bifidobacterium breve (up to 20 BCFU)
- 2 weeks of Bifidobacterium infantis (up to 20 BCFU)
Bottom Line
My personal choice would be to go with the “Healthy Algorithm” for the following reasons:
- The traditional approach has appeared to stall, time for a change
- It is heavily based on very statistical significance over the entire scope of bacteria involved (i.e. dense data) but it has not been validated by clinical studies.
- I have always been unhappy about clinical studies because the data is:
- Messy (typically in the context of one or another medical condition)
- Small sample sizes
- Low resolution to bacteria
I am also curious to see how well the “Healthy Algorithm” performs.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
Recent Comments