And thus have the ability to compute the theoretical differences.
We also have these collections of studies which we can use by flipping things to be negative cognitive function:
Cognitive Function
Intelligence:Comprehension, Cognitive Ability
This resulted in 71 bacteria.
Results
For Sugar we had agreement between reported shift and cognitive issues for the following:
Bacillota
Bacteroides
Coprococcus
Desulfovibrio
Dorea
Escherichia coli
Faecalibacterium prausnitzii
Lachnospiraceae
Ruminococcus
Streptococcus
For Fat we had agreement between reported shift and cognitive issues for the following:
Bacillota
Bacteroidaceae
Bacteroides
Clostridium
Coprococcus
Coriobacteriaceae
Dorea
Faecalibacterium prausnitzii
Oscillospira
Phascolarctobacterium
Porphyromonadaceae
Ruminococcaceae
Ruminococcus
With Fat we had significantly more contrary shifts than with Sugar.
Bottom Line
Both High Fat and High Sugar in isolation appear to impact cognitive function. High Fat has the appearance of having less impact in isolation than high sugar. The following shifts seem to be common with these:
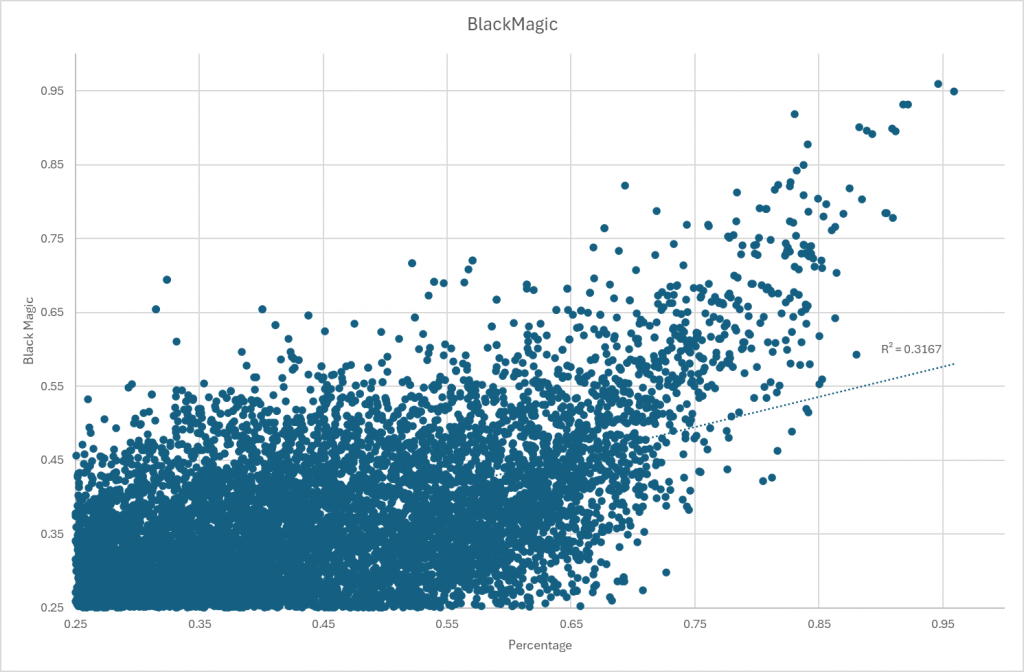
A few days ago I posted the results for Bacteria Association (with graphics). I did some operations Research black magic in transforming the data. This black magic is a key part of a patent application that has been filed.
Over the last decade, I have been focused on understanding the statistics of the microbiome bacteria. My multiple degrees are in Probability and Statistics, hence the desire to build mathematical models for the microbiome bacteria.
One of my key observations is that “one model does not fit all taxa“. One observation is very consistent: no bacteria fits the gaussian (normal or bell curves) rendering the use of mean and standard deviation not only suspect, but naively dumb.
This post exhibits the challenges. We take 1000 Shotgun samples of healthy people using 10 million reads and look for associations by doing classic linear regression. We apply a variety of monotonic increasing transformations to the percentage/counts and see where we get the most relationships with R2 > 0.25.
First Pass Analysis
I decided to see how well “common textbox solutions” would do compared to my “Black Magic” monotonic increasing transformation. If people want to suggest other monotonic increasing transformations, I am very willing to run other transformations on this dataset and add it to this report.
Method
“Black Magic”
Using Percentage / Count
Using Log(Count)
Number of R2 > 0.25
15,183
1,764
9,616
Number with higher R2
1,356
7,167
Number with lower R2
408 [13,827]
2,449 [8016]
Numer of items with R2 > 0.25
The [ ] is the sum of not found and lower R2.We see that the “Black Magic” clearly found more statistically significant relationships. Taken in isolation, “Black Magic” also found more relationships with a higher R2. The Log(Count) items with a higher value are worth some extra analysis.
Percentage or Count
This is the typical naïve approach used by people who rote-learn statistics. We found only 10% of those we got via “Black Magic”. Many relationship were very similar, they tend to be for bacteria with low rates of detection (i.e. occurs in < 25% of samples) and low amounts of bacteria. To translate, very few distinct values in these subsets.
Other has significant differences
A chart comparing results.
Log(Count)
Using a log(values) is a common statistical trick dealing with non-gaussian (normal/bell curve) data to get semi-normal data. For R2 that were higher than “Black Magic” we have:
Mean Difference: 0.23
StdDev Difference: 0.09
Maximum Difference: 0.43
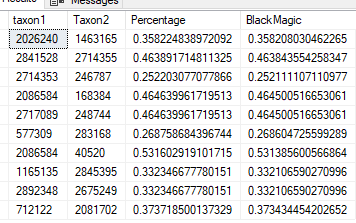
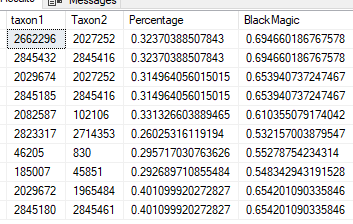
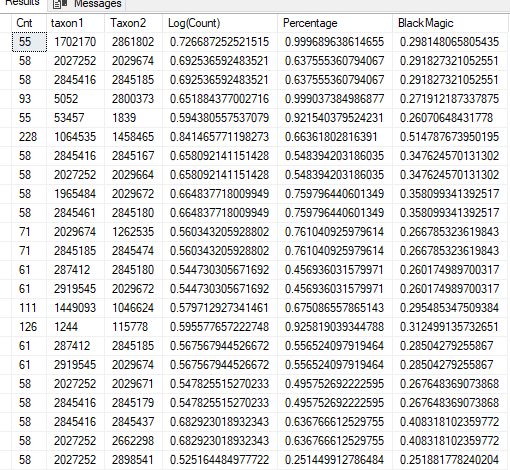
We have a sample of the greatest difference below, and note that the sample size was relatively small. The top line has R2 of 0.999. This suggests that we may need to exclude taxa that has less than N distinct values (a possible follow up post)
Restricting to samples where we have 300 or more (incidence of detection: 30%). In this case Log(Count) with higher R2 exceed those with lower R2 compared to “Black Magic”
Method
“Black Magic”
Using Percentage / Count
Using Log(Count)
Number of R2 > 0.25
10,733
702
8,121
Number with higher R2
494
6130
Number with lower R2
208 [10239]
1991 [4603]
Bottom Line
Log(Count) produces acceptable results while failing to detect 20% of those detected by “Black Magic”. The ideal solution would be to do both methods and take the highest R2 from each regression. I await other suggestions for monotonic increasing transforms to try. It is very clear that using counts / percentage is a poor statistical choice.
There is a follow up post suggested based on the density/sparseness of different values. Having too few distinct values appears to over-fit and produce suspect/false higher R2.
Methane may be reduced by up to 98% by eating a small amount of Red Seaweed. Bromoform in red seaweed inhibits a key enzyme used by microbes to produce methane gas. It is commonly found in red seaweed Asparagopsis taxiformis(Recommended reading)
Asparagopsis is one of the most popular types of limu.[4] in the cuisine of Hawaii, it is principally a condiment.[5] It is known as Limu kohu in the Hawaiian language, meaning “pleasing seaweed”.[6]Limu kohu has a bitter taste, somewhat reminiscent of iodine,[7] and is a traditional ingredient inpoke.
In reviewing the literature on different types of seaweeds, most studies found that they reduced methane. Consumption of common seaweeds supplements or foods are a viable approach. The levels of Bromoform may not be as high, but may be enough to cause changes while generally considered safe to consume..
There are no studies on using seaweed with SIBO that could be located.
L-lactic acid (L-lactate, (S)-lactic acid, or (+)-lactic acid):
This is the form produced in human metabolism, especially during anaerobic glycolysis (when oxygen is limited, such as during intense exercise or tissue hypoperfusion).
L-lactate is the predominant form found in human blood and tissues.
D-lactic acid (D-lactate, (R)-lactic acid, or (−)-lactic acid):
This form is produced mainly by certain bacteria during carbohydrate fermentation, including some gut bacteria.
Humans produce very little D-lactate, but it can accumulate in specific conditions, such as short bowel syndrome, where bacterial overgrowth leads to increased D-lactate production and absorption. Typically this form often manifest itself as Brain Fog.
Lactic acidosis refers to the accumulation of lactic acid in the body, leading to a decrease in blood pH. It is classified based on the underlying cause:
Type A Lactic Acidosis:
Caused by tissue hypoperfusion and hypoxia (lack of oxygen), leading to increased anaerobic metabolism and L-lactate production.
Common in shock (septic, cardiogenic, hypovolemic), severe hypoxemia, or cardiac arrest.
This is the most serious and common form.
Type B Lactic Acidosis:
Occurs without obvious tissue hypoxia or hypoperfusion.
Subdivided into:
Type B1: Associated with underlying diseases (e.g., liver failure, cancer, diabetes).
Type B2: Caused by drugs or toxins (e.g., metformin, antiretrovirals).
Type B3: Due to inborn errors of metabolism or microbiome dysbiosis.
Can also result from intense exercise, seizures, or certain metabolic conditions.
D-Lactic Acidosis:
A rare form caused by excess D-lactate, typically in patients with short bowel syndrome or after certain intestinal surgeries.
Human enzymes cannot efficiently metabolize D-lactate, so it can accumulate and cause neurological symptoms (encephalopathy)
In Home Treatment Options for Normal Acidosis
The common approaches include:
Vitamin B1 or Thiamine : A deficiency of this vitamin can cause lactic acid issues
Water / hydration: Goal is to urinate out the excessive lactic acid
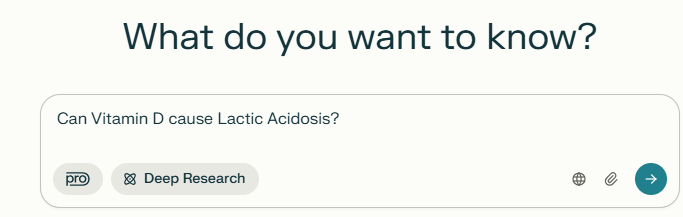
Stop any medication associated, to do this do google search or use perplexity.ai naming your medication or supplement and asking if lactic acidosis can be cause by it. Example below
Treatment Options for d-Lactic Acidosis
“Symptoms typically present after the ingestion of high-carbohydrate feedings. Neurologic symptoms include altered mental status, slurred speech, and ataxia, with patients often appearing drunk. Onset of neurologic symptoms is accompanied by metabolic acidosis and elevation of plasma D-lactate concentration. “
“Treatment includes correcting the acidosis and decreasing substrate for D-lactate such as carbohydrates in meals. In addition, antibiotics can be used to clear colonic flora.”
“Oral antibiotics that are poorly absorbed are most effectively used locally in the gut—these include clindamycin, vancomycin, neomycin, and kanamycin”
“There have been reports as described above regarding probiotics being implicated as a causative agent in a few cases of D-la”
Bottom line for d-Lactic Acidosis
Reduce or eliminate carbohydrates
Antibiotics
Avoid probiotics
Get a detailed microbiome report (ideally shotgun) to identify candidate bacteria and then alter diet appropriately.
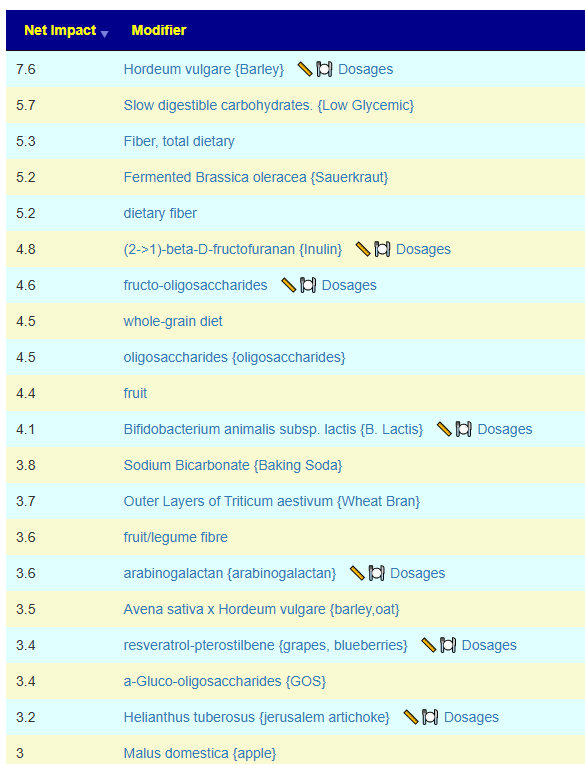
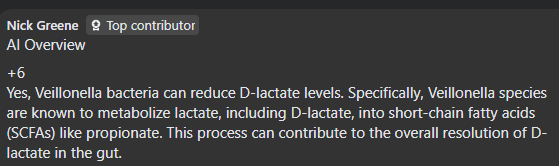
See what encourage it here. MAKE SURE TO EXCLUDE everything that could contain d-lactic producing probiotics (i.e. ANY probiotics, i.e. Yogurt). Items that modifies Veillonella are there.
I’d love some additional help, please. I’ve done two BiomeSight.com tests. I followed the suggestions after the first test and my microbiome has changed and some of my symptoms are improving. However, I couldn’t tolerate any of the bifidobacterium strains I tried, all of them caused very painful long-lasting migraines. Despite taking them for a combined 6wks (3 different strains for 2wks each), my bifidobacterium levels look unchanged. The suggestions do say that ‘No Probiotics without some adverse risks could not be identified.’ so maybe it’s better I just avoid them altogether for now?
I was diagnosed with ME/CFS 16yrs ago, after EBV 22yrs ago.
I caught Covid-19 in 2023.
I was diagnosed with chronic migraines in 2024 – they have increased in severity and occurrence over the last 5yrs, since the Covid-19 vaccines, though I can’t be sure it’s related.
My primary symptoms are: fatigue, pem, migraines, brain fog, ibs, acne, and hair loss.
I give my permission to use the above information anonymously for a blog post.
Analysis
I smiled when I saw ” ‘No Probiotics without some adverse risks could not be identified” and “I couldn’t tolerate any of the bifidobacterium strains I tried“. It seems that the expert system are making good (probable) suggestions. Suggestions are based on odds and not guaranteed.
Pass 1 – Based on Reported Symptoms
When there are many symptoms, my usual path is to get symptoms entered and then get suggestions focused on the bacteria likely associated to those symptoms. This is a targeted approach.
This person had entered any symptoms for their latest sample, and did for the sample from 7 months prior. 4-9 months between samples is what I advocate (balancing costs and time to change the microbiome).
I usually check all of the types of suggestions (I have no ideological position against using any of the types)
Then on the resulting page we see 12 bacteria that are the most likely causes. 2 low and 10 high. Suggestions are computed using five(5) different algorithms and then we use Monte Carlo Model to improve the odds of making good choices. Why different algorithms — simple, microbiome tests are fuzzy in their identification and many different criteria for selecting bacteria are advocated in the literature.
We go to the Consensus Suggestions and sort by Take Count — to get what all agrees about.
Looking at positive 5’s only:
Vitamins
Vitamin B2
Vitamin B1
Zinc
Amino Acid
Melatonin
Carnitine
Glutamine
Taurien
Antibiotic (Only 5’s)
loperamide hydrochloride Loperamide is most commonly used to treat acute and chronic diarrhea, including traveler’s diarrhea and diarrhea associated with inflammatory bowel disease (IBD).
florfenicol. Florfenicol is effective against a wide range of bacterial pathogens in animals, including both Gram-positive and Gram-negative bacteria. It is commonly used to treat respiratory infections, gastrointestinal infections, urinary tract infections, and other bacterial infections in livestock and companion animals
AtorvastatinAtorvastatin belongs to a class of medications known as statins, which work by inhibiting HMG-CoA reductase, an enzyme involved in cholesterol synthesis. By reducing cholesterol production in the liver, atorvastatin helps lower total cholesterol, LDL cholesterol (often referred to as “bad” cholesterol), and triglyceride levels.
It is interesting that Lactobacillus dominate with just one Bifidobacterium. I would carefully try these, one at a time, starting with a low dosage and increases, then change every 1-2 week to the next (keeping notes!!!), My preferred source of probiotics are listed here.
Pass 2 – Based on PubMed
I view this method as less accurate but the suggestions are ideal for discussion with a MD if antibiotics or other prescription items are suggested. It is available as the last item.
Rather than detailing items, I attached the report below
I’ll give this new round of suggestions a go, and then I’ll do another test.
I don’t have a willing GP (or vet, lol) to prescribe antibiotics but it’s very interesting that statins suggested – high cholesterol runs in my family and a lot of them are on statins.
The cholesterol issues are often DNA related… and DNA also impacts the microbiome. DNA is hard to change, the microbiome is easier.
From Perplexity: High cholesterol levels can indeed be influenced by genetic factors, with both common and rare gene variants playing significant roles in LDL cholesterol regulation. Here’s a breakdown of the genetic mechanisms involved:
Key Genes Affecting Cholesterol
LDLR (LDL Receptor) Mutations in this gene (chromosome 19) disrupt LDL cholesterol clearance, causing familial hypercholesterolemia (FH). This autosomal dominant condition leads to lifelong elevated LDL levels (200–300% higher in heterozygotes) due to defective receptor production or function126.
APOB (Apolipoprotein B) Mutations in APOB impair LDL binding to receptors, reducing clearance. For example, the APOB variant causing “familial ligand-defective apoB-100” increases LDL by 200–300%17.
PCSK9 Gain-of-function mutations in this gene degrade LDL receptors excessively, raising LDL levels. Conversely, loss-of-function variants (e.g., in 2% of African Americans) lower LDL by 30% and protect against heart disease168.
E4 carriers have ~5% higher LDL due to rapid lipoprotein clearance and LDLR downregulation.
E2 carriers have ~5% lower LDL but risk familial dysbetalipoproteinemia13.
Inherited Disorders
Familial Hypercholesterolemia (FH): Caused by mutations in LDLR, APOB, or PCSK9. Affects ~1/250 people, leading to LDL >190 mg/dL and premature atherosclerosis if untreated146.
Familial Hypobetalipoproteinemia: APOB mutations reduce LDL production, resulting in very low cholesterol levels13.
Autosomal Recessive Hypercholesterolemia: Rare ARH mutations cause LDL receptor dysfunction, leading to severe cholesterol elevation1.
Polygenic Influences
Most hypercholesterolemia cases involve interactions between multiple common variants (e.g., APOE, NPC1L1) and lifestyle factors. These variants individually exert small effects but collectively contribute to cholesterol variability137.
While genetics set baseline risks, diet and exercise remain critical for management, especially in individuals with predisposing variants368. Genetic testing is recommended for suspected FH to guide early intervention
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.



Recent Comments