A reader wrote:
There’s one thing I which caused some bewilderment though, I put the screenshots from the recommendations from Biomesight here below, and I don’t understand why they seem quite divergent to what you are suggesting. I don’t know if it’s just my amateur eyes and then not so divergent after all, but to me they do seem quite different (apart from the lactobacilli). Shall I just ignore their suggestions ( also food wise) or would you say by and large it goes into the right direction?
Reader, May 23,2024
The answer depends on the logic each provider uses, which bacteria are in their microscope that needs changes, depth of their research and their skills in addressing contradictory results. I will look at three providers below:
- Biomesight (provided by the reader)
- Startup in US(from a review copy)
- Microbiome Prescription
See also this post: Why do metabolite levels disagree between sites?
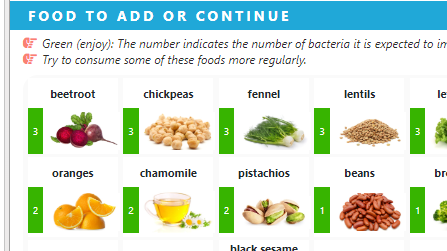
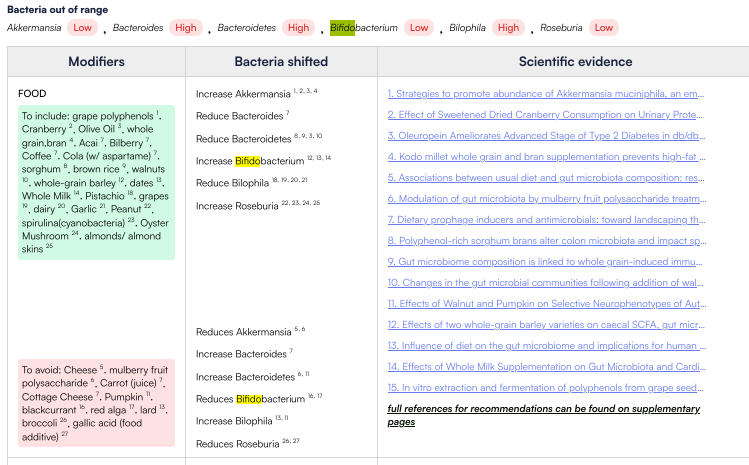
Biomesight
We see a number by each suggestion
Hovering over the item will show the bacteria believed to be impacted
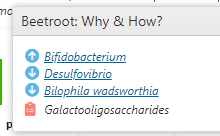
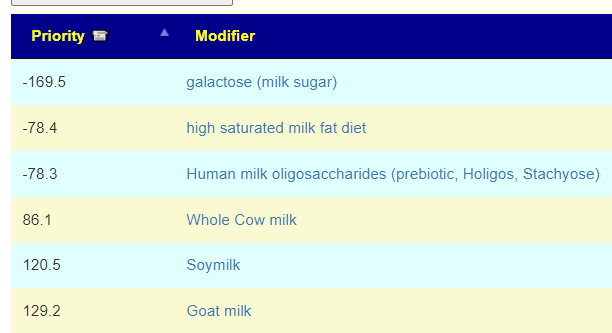
Clicking on the name will show details. Note that the bacteria shown is correct. The link also shows “Galactooligosaccharides (GOS)” and not the food suggested explicitly. The food selected contains GOS but none of the studies are explicitly for Beetroot. To MP, the beetroot contains multiple compounds, some may have overpowering negative effects — hence MP keeps to precisely what is cited in the study.
My inferred take-away from looking at the suggestions
- Foods and substances are done by association and inference
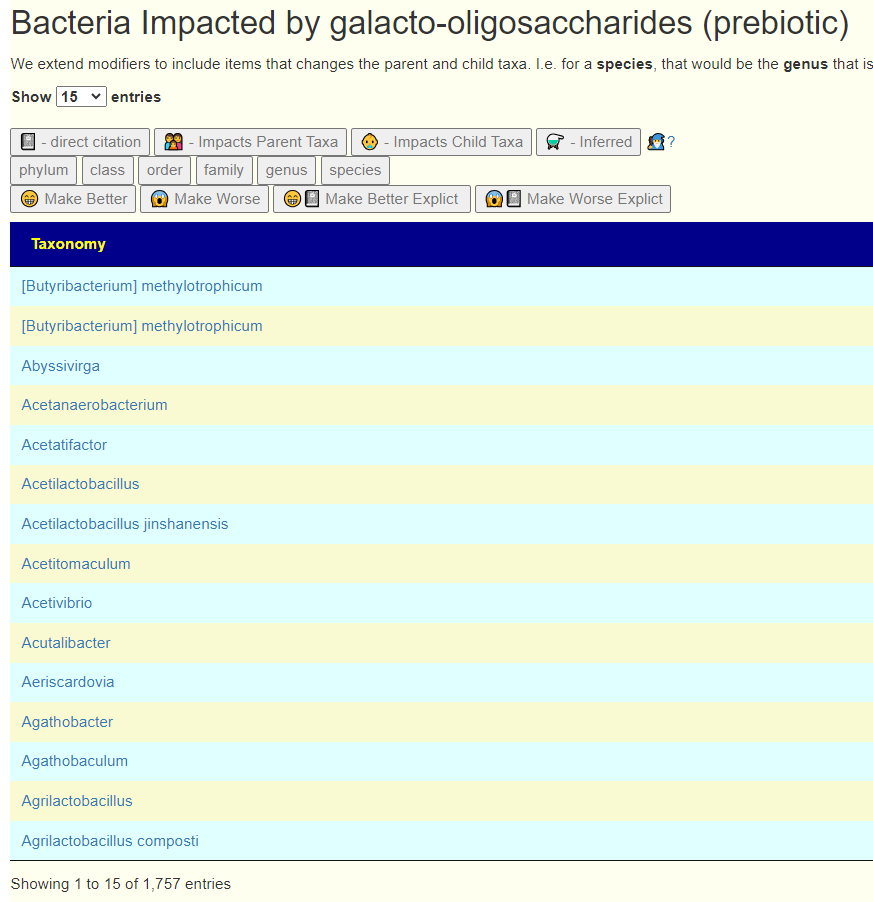
- Only a handful of bacteria are considered.
Consider the bacteria list on MP for the same substance – 1757 citations at the moment.
New Start-up
This is from an early draft. They are using the database of Microbiome Prescription but with a set of proprietary rules, custom ranges, and algorithms. They restrict their scope to a few dozen genus. For the bacteria in their scope, MP has no contraindicated data and do not use inferences to parent or child taxa. That is, there is no need for balance algorithms. In short, it is a proprietary suggestion system designed.
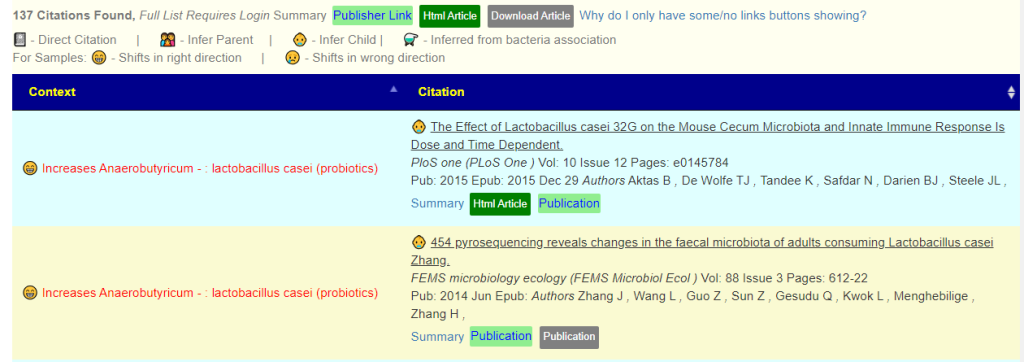
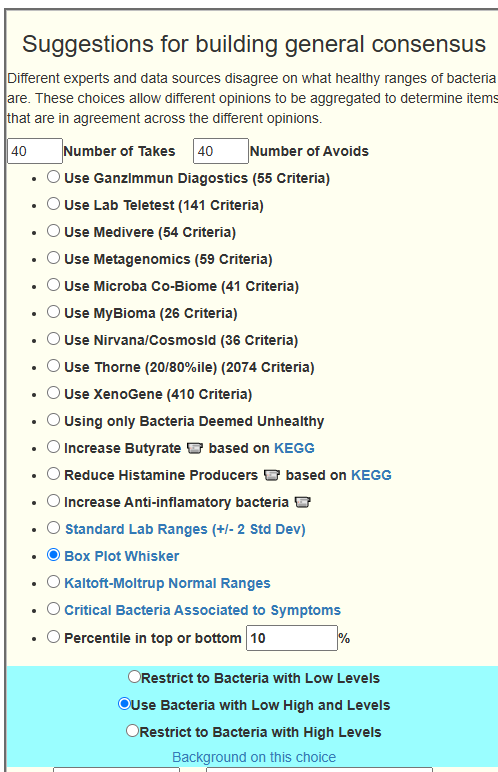
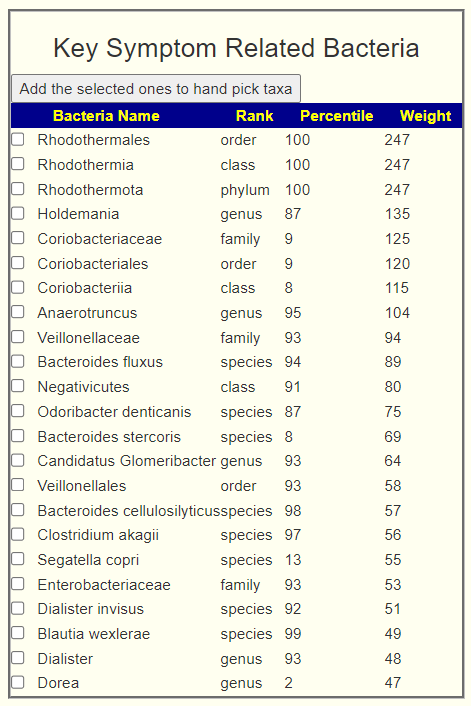
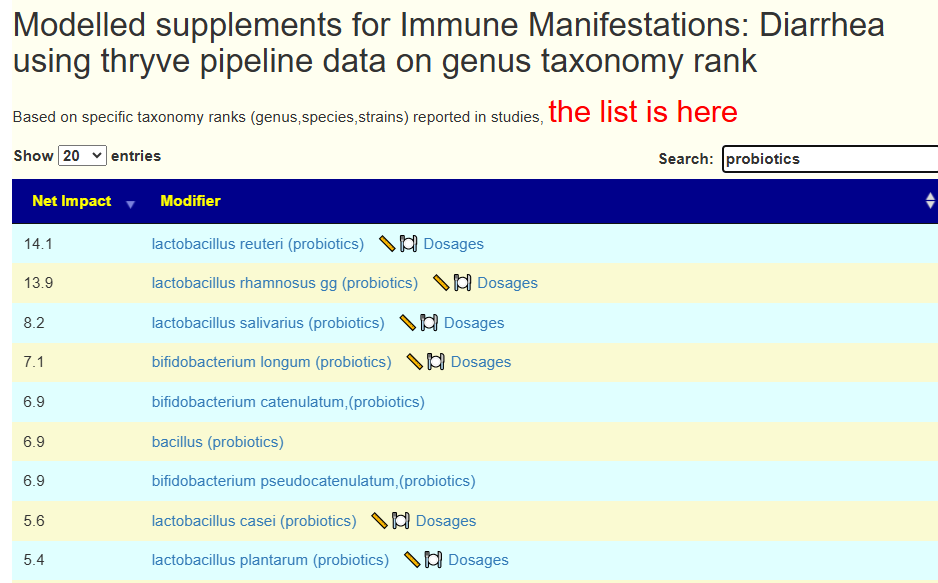
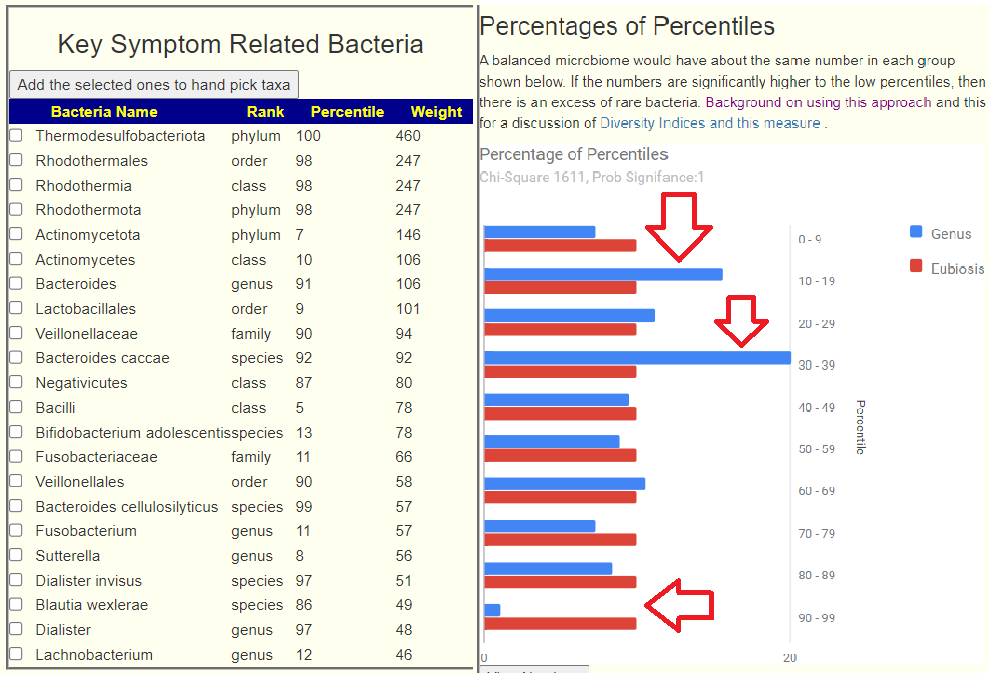
Microbiome Prescription
For details on which bacteria are selected, see Algorithm for “Just Give Me Suggestions”. Typically we have an average of 65 bacteria under our microscope with 600 on some shotgun samples. Roughly 20-30% of the bacteria identified.
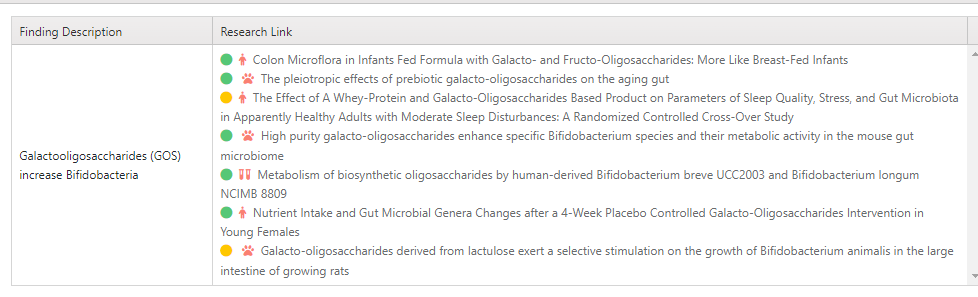
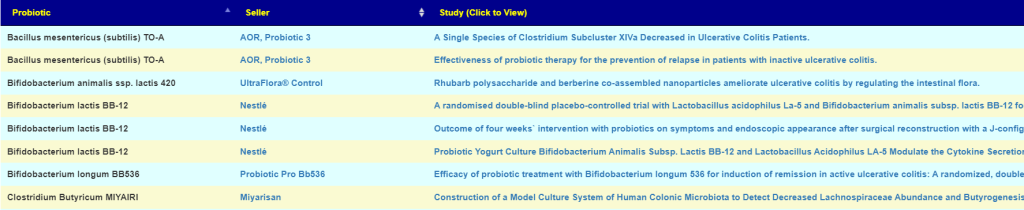
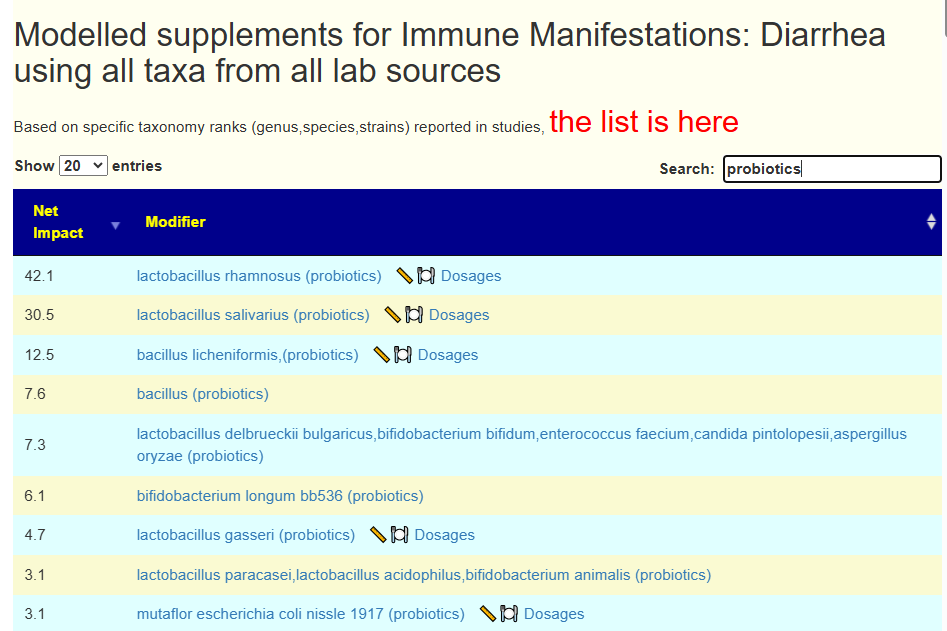
Now for every suggestion we make available the list of studies (137 for this probiotic suggestion). Note in the study names — that this probiotic is explicitly named.
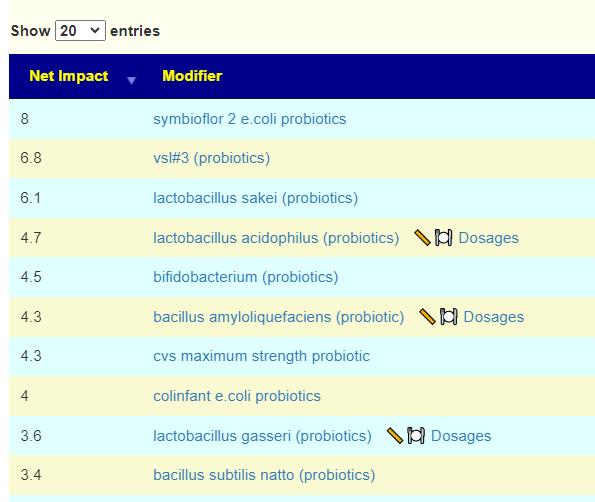
We also include the negative effects
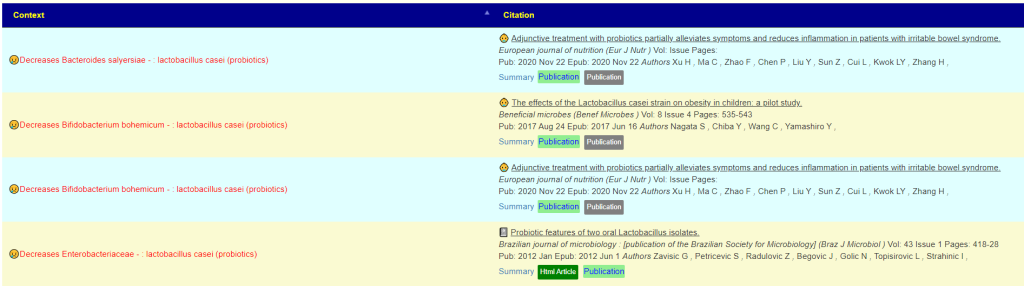
We have our own proprietary algorithm on how to evaluate this data. People can take this data and apply their own logic.
MP’s goal is to be the most comprehensive source with new studies adding every week. We have also been delighted that the startup (who I have been doing pro-bono consultation with) have set a team of their M.Sc. (or higher) staff on checking the citations. They have been finding a very low bad entry rate ( < 1%) but discarding 8% of studies for diverse reasons. The startup criteria (no contradictory results from different studies) often result in only 10% of available studies being used.
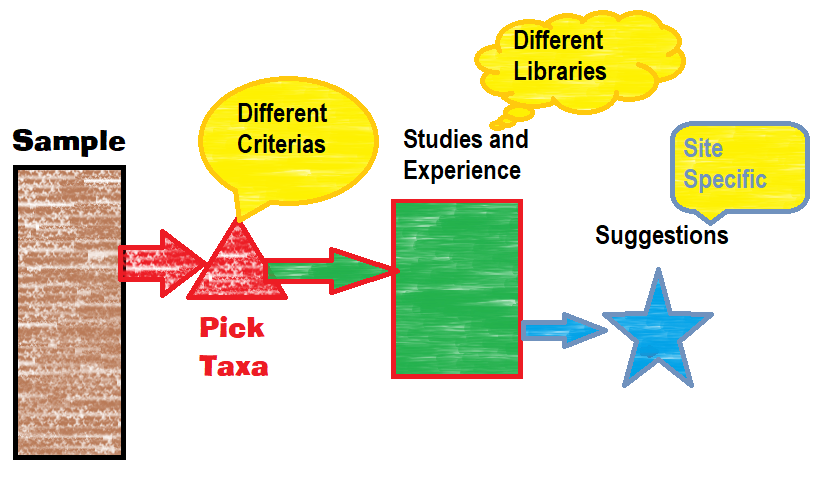
Bacteria Selected Determine Suggestions
Microbiome Prescription does NOT know what is the best method of picking bacteria to focus on. The Simple UI gives THREE different approaches.
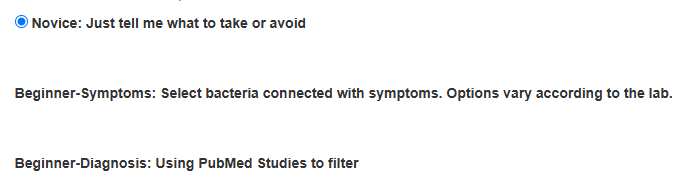
- Novice works on anything out of range – often including harmless bacteria in the calculation.
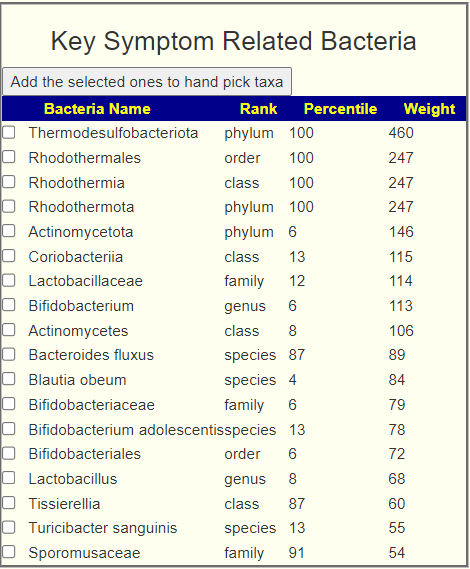
- Beginner – Symptoms: Works off patterns of bacteria associated to user reported symptoms that are statistically significant
- Beginner-Diagnosis: Bacteria shifts reported associated to diagnosis in published studies.
It is possible that the bacteria selected by each of these method will have no overlap. IMHO, Beginner – Symptoms is the most likely to be correct. THE BACTERIA SELECTED DETERMINE THE SUGGESTIONS.
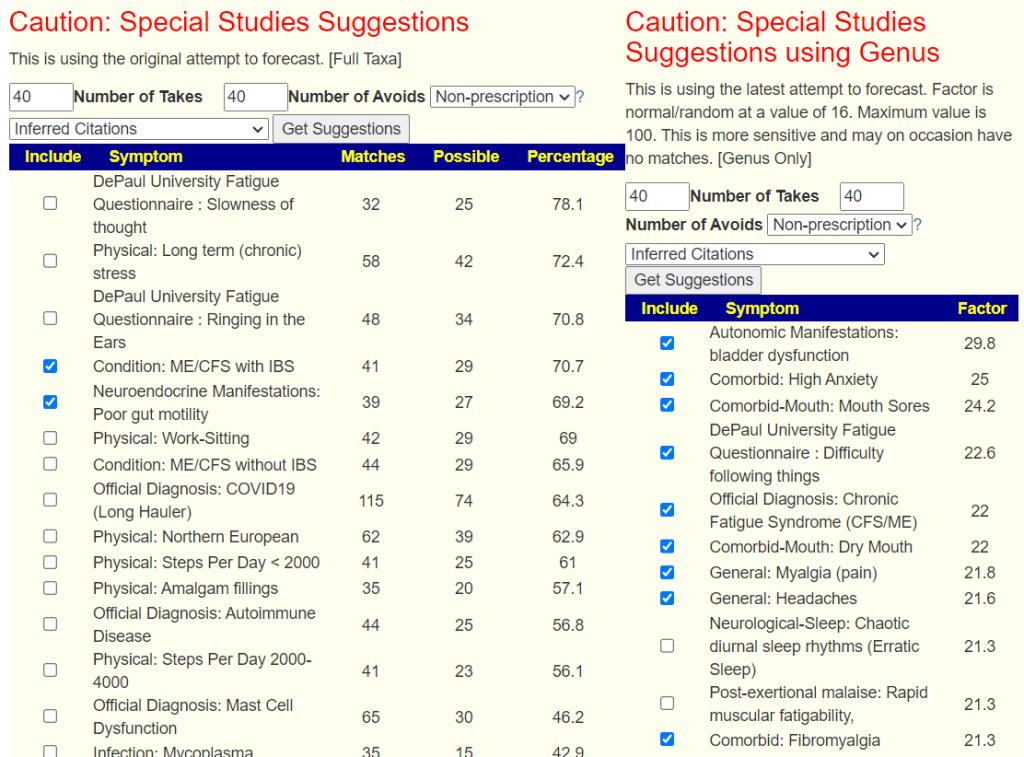
For more advance users, there are a lot more (84x) methods of picking bacteria:
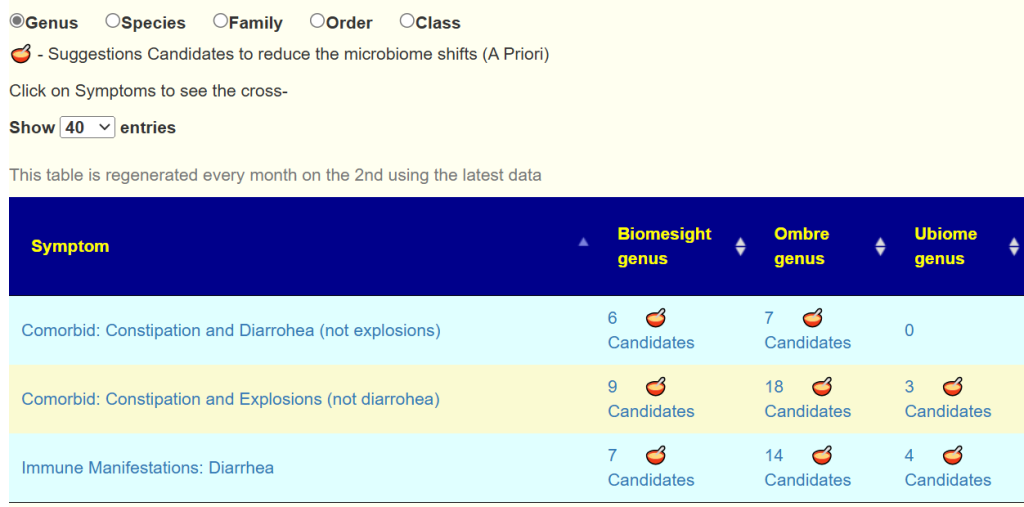
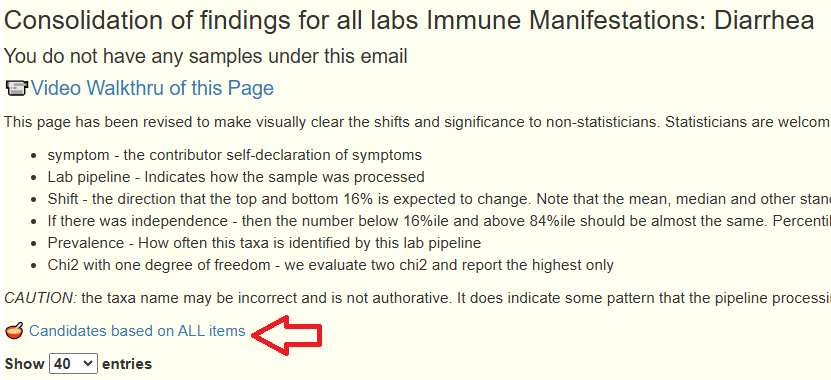
Regardless of method, if you go to Consensus Report
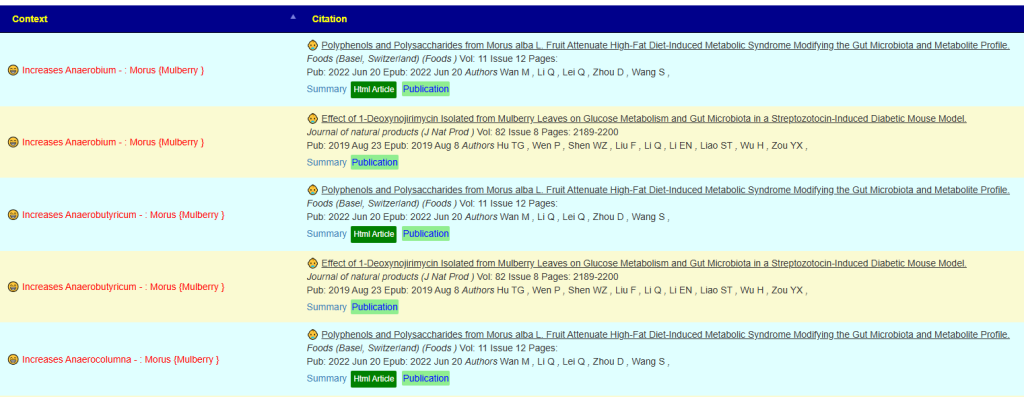
You will see PubMed with stacks of books under it. Just click on the books

This shows the studies used and the logic
Best practice is to always save the page as a PDF and the Consensus View as a CSV. Often people will come back later and see different suggestions because they selected a different method of picking bacteria. One other factor is that data is added weekly to the database which will cause shifts over time.
Bottom Line
- What is the scope of their microbiome scope? IMHO: the bigger the scope, the better the results
- Is the data based on explicit studies or on interference (A contain X and X helps — we’ll ignore B,C,D that is also in X)
- BEWARE of sites that do not provide explicit studies – often they are working from hearsay.
- Does the suggestion consider contraindicated information?
- How big a database are they using? Have there been third party checking of the database?
Suggestions may be reasonable: a professional dietician would likely do the same logic in the case of BiomeSight suggestions.
Questions
- Since Startup and Microbiome Prescription use the same database, will suggestions always agree?
- No, for several reasons:
- The bacteria in-scope-to-change are different. If MP picks one that Startup does not, then suggestions may shift for some substances. Startup computes its own definitions of what is high and low. They also look at a handful of genus only.
- Startup hand select certain studies to be excluded or lessen in values. Studies may be on human, animals or a lab situation (petri dish) – they wanted to weight the value of each study different from MP.
- No, for several reasons:
- What should I do if there are explicit disagreements?
- The safest path is to do only things that there is agreement on.
- If another item interests you, review the studies cited to make a decision.






Recent Comments