To use this feature, you need to upload a 16s sample (Ombre/Thryve, uBiome, BiomeSight) to Microbiome Prescription.
The new special studies are all done on Symptoms that could have sufficient data to detect statistical significance at p < 0.01 or p < 0.001. Many studies on the US National Library of Medicine report significance with p < 0.05. I prefer to reduce the risk of false positive results given that we have so many bacteria possible. 800 bacteria with p < 0.01 would expect 8 items by random chance. p < 0.001 would expect just 1 or less item by random chance.
I also did a more formal presentation showing the t-score, degrees of freedom and probability.
How to Find These Special Studies
Click the Research Tab and scroll to the bottom, you will see:
Pick 1 to go to version 2
On this new page, select your sample and then the symptom that you are interested in. There are a lot more symptoms than in the original version
The table below show all of the taxa from the same lab that you also had reported.
If something is clearly significant, you will see P < 0.001- Too High displayed. The Degree of Freedom is the number of samples that have this bacteria. For example Thiocapsa is seen in just 151 samples, thus a rare bacteria. Look at Phascolarctobacterium, this sample has 24000, people with the condition averages 8500 and people without this symptom averages just 5000. It is clear that you have an increased risk of this condition.
You also have age range… which indicates how much you microbiome agrees with an age range (sorry, getting older is not curable!).
For a few items, you may get no rows. That means that none of the bacteria you have matched the list of ones that were found significant.
There is a lot of data there. I am planning to add hand picking bacteria to these pages eventually.
The Difference Between Version 1 and 2
One of the challenges with earlier attempts to find clear associations between bacteria and symptoms has been insufficient data. Earlier attempts made best efforts with the data that was available. Thanks to people uploading more samples, and annotating them with symptoms, we have entered a time of sufficient data for better analysis. The table below shows the difference between the penultimate version and the current version.
Aspect
Prior “V1”
Current “V2”
Sample of people with condition
Reported a specific symptom
Reported a specific symptom with Source Lab
Control Group
Everyone that did not report symptom. Including people that did not report any symptoms.
Only samples with symptoms reported, but not those with a specific symptom.
Weight for suggestions
z-score
Different between sample and mean for control group. Difference is scaled by a linear monotonic function.
Handling of multiple symptoms
“Clumsy” – bacteria get double counted often
Allow one pass to get bacteria shared across symptoms. No double counting
Nota Bene: The control group is not healthy people, just people without the specified symptoms. This is a two edge sword that many would debate.
Histamine issues can occur from consuming food high in histamines. This is the typical approach for people dealing with this issue. There is an another route that should not be overlooked — things that do not contain histamine but which triggers histamine release.
Citations
Histamine release caused by reactions to drug product and/or excipients/vehicles is a phenomenon observed in both toxicology and pharmacology studies. This type of reaction is also referred to as pseudoallergic reaction, anaphylactoid reaction or complement activation-related pseudoallergy (CARPA).
“Codeine and meperidine are examples of other opioids that can induce mast cell activation with the release of histamine” [ 2020]
“Quaternary ammonium compounds (e.g., NMBDs) are generally weaker histamine-releasing substances than are tertiary amines such as morphine.”
“Histamine release can occur with administration of certain opioids” [2015]
“Histamine release is primarily caused by morphine, followed by hydromorphone,” [2009]
“Histamine release and the severity of reactions during vancomycin administration are directly dependent on the rate of infusion.” [2007]
“It is not clear whether histamine levels are altered following hypo– or hyperthermia seen during several clinical or experimental situations.” [2004]
“Histamine release and non-IgE-mediated anaphylactic (anaphylactoid) reactions occur with alcuronium” [2016]
The above means that care needs to be taken if a herb, spice or supplement causes a histamine reaction. It may not be histamine in the substance, rather the substance causes mast cells to react and dump histamine. It is a significantly different situation. Other items that have been reported to cause histamine release include: Vitamin C(L-Ascorbic acid), Niacin (vitamin B3), Quercetin, Stinging nettle, Licorice root, Ginkgo biloba, Chamomile and Echinacea.
Histamine toxicity is sometimes confused with an allergic reaction to fish. Here is why: Some kinds of fish contain naturally high levels of the chemical histidine. This chemical can be converted to histamine by bacteria [ the enzyme histidine decarboxylase EC 4.1.1.22]. In an allergic reaction, mast cells release histamine which triggers allergy symptoms. So, if a person eats fish that has a high level of histamine, the response may resemble an allergic reaction to that food.
Based on frequency of detection and average amount detected
Hypothesis Testing on Bacteria Conversion
The citizen science site, Microbiome Prescription, allows people to share their microbiome results from many labs and to annotate their samples with symptoms. Over 1000 samples have these annotations as shown below, so we can suggest a hypothesis and test it.
Hypothesis: People with Histamine Issues are likely to have higher counts of bacteria producing histidine decarboxylase
The hypothesis failed with statistical significance!
The results was a bit of a surprise. The Hypothesis failed dramatically! Having more bacteria producing this enzyme appears to be associated with less histamine issue!! This pattern persists across all three labs with significant data sample size.
One hypothesis that could be suggested by this data is that the histamine issue is due to the body’s base level of histamine being abnormally low and thus the body is unfamiliar with histamines and thus overreacts.
An Analogy to Consider
Imagine someone whose diet lacks ANY added sugar. After a year, he drops into a friend who makes him his favorite herbal tea. The friend, she, likes sweet tea and adds several teaspoon of sugar. This person drinks it and gets an atypical headache which confuses the friend – he drinks it regularly! The real cause is too low a base level of sugar consumption for this person to tolerate.
The above suggests that the same may be occurring with histamine reactions.
Did you know that both too much sugar and too little of sugar can cause headaches? When you consume too much sugar at once or don’t eat for an extended period of time, you can cause rapid fluctuations in your blood sugar levels which can trigger a headache. Some people are more prone to these sugar-triggered headaches.
While a bacteria has an enzyme, it is not a given that it is active. Our second pass is looking at the frequency of each bacteria taxa appearing in each group. If a specific taxa is significantly more or less frequent, it may be a trail worth following. Drilling down to species causes our observations to drop to the point that many data points cannot be examined for significance. We have three taxa with good sample sizes.
Remember, different labs use different software resulting in different taxa names.
Bacteria
Percent Having
Mean
SD
Subset
Lab
Bacteroides fragilis
79.2
5138
8629
Histamine
BiomeSight
81.4
6369
16168
No Histamine
75.6
6736
22788
Histamine
uBiome
51.8
16628
47841
No Histamine
94.2
7343
14279
Histamine
Ombre
94.2
8646
27095
No Histamine
Eggerthella lenta
74
57
611
Histamine
BiomeSight
69.8
365
346
No Histamine
74.4
67
1323
Histamine
uBiome
69.5
235
1502
No Histamine
77.9
824
2407
Histamine
Ombre
79.4
1059
4131
No Histamine
Gordonibacter pamelaeae
57.78
52
459
Histamine
uBiome
61.2
207
413
No Histamine
51.9
124
177
Histamine
Ombre
46.1
187
358
No Histamine
The most statistically significant was uBiome with Bacteroides fragilis
Bacteroides fragilis for Ombre(Thryve), uBiome and BiomeSight were the most statistically significant and all have the same pattern: People reporting histamine issues had less than people that did not report histamine issues. Bacteroides fragilis is also the main source of histidine decarboxylase from the microbiome.
uBiome data was very interesting because the detection rate for Bacteroides fragilis was significantly less for samples that did not report histamine issues with the differences of means being much much more than with other labs. This hints that some part of the base pairs collection that uBiome used to determine Bacteroides fragilis in their software may be particularly important for histamine issues. To put it another way, some part of the sequence being used to determine the taxa, also appears to detect histamine issues. This leads to the possibility that specific strains of Bacteroides fragilis may result in better histamine tolerance.
uBiome and others use a reference database. Because a 16s test only looks at a tiny portion of the microbial genome, of necessity different bioinformatics pipelines will assign slightly different microbial genus/species names for the string of base pairs they sequence.
uBiome, a company that offered microbiome testing services, used a proprietary reference database called the uBiome Microbial Insights Test (MIT) reference database for the taxonomic classification of 16S rRNA gene sequences. This database was specifically designed for the analysis of human microbiome samples, and included over 1,000 microbial taxa that were commonly found in the human gut, oral, and skin microbiomes. The database was built using a combination of publicly available 16S rRNA gene sequences and uBiome’s own sequencing data, and was regularly updated to incorporate new microbial taxa and improve the accuracy of taxonomic assignments.
From Chat_GPT
Biomesight: SILVA SSU Ref NR 99 database,
Ombre: GreenGenes 13_8 release
American Gut: Greengenes 13_8 release,
Thorne: Their 16s database is built from a combination of publicly available reference databases, including the Greengenes and SILVA databases, as well as Thorne’s own sequencing data.
Unfortunately uBiome reference database disappeared with it going into bankruptcy. Only time will tell if Thorne’s reference database will identify the key base pairs that appears to be connected to histamine issues.
What is very interesting comes from a 1999 study, “Intestinal mucosa-associated bacteria modulate rat mast cell reactivity” which reports a ConA-induced histamine release was diminished up to 71% of maximal histamine release by Bacteroides fragilis!! This supports that increasing Bacteroides fragilis may be the right way to go.
Where do we go from here for bacteria?
The above suggests that there is a bacteria taxa with a specific key base pair that is connected to histamines issues. Let us call it “Bacteroides Histamilis”(BH). This taxa has some overlap with Bacteroides fragilis (BF). They appear to occupy a similar niche in the microbiome world with an increase of BF decreasing BH (or it’s impact). We are shooting in the fog here, but it seems encouraging BF growth may reduce BH and ease histamine issues. We have know items that increases or decrease listed here: Bacteroides fragilis and a link to possible foods. The top food nutrients are iron, zinc and Riboflavin (Vitamin B2).
Going to Chat_GPT for some quick answers, we get a pleasant surprise:
Iron plays an important role in the regulation of histamine levels in the body. It is required for the activity of an enzyme called diamine oxidase (DAO), which is responsible for breaking down histamine in the gut. Low iron levels can lead to reduced DAO activity and increased histamine levels, which can contribute to histamine intolerance or sensitivity.
Zinc is also important for the activity of DAO, as well as for the regulation of histamine receptors in the body. Zinc deficiency has been linked to increased histamine levels and may contribute to histamine intolerance.
Riboflavin (vitamin B2) is required for the synthesis of DAO, and low riboflavin levels have been associated with reduced DAO activity and increased histamine levels.
Answer from Chat_CPT to question: “Is histamine sensitivity connected to iron, zinc or Riboflavin deficiency?“
So, we have an interesting cascade… the 3 key nutrients available concurrently in food that increasesBacteroides fragilis, are all associated with DAO production. Should we speculate that BH is a mutation that thrives better with low levels of Iron, Zinc and Riboflavin and the difference in base pairs is connected with this mutation? Continuing this thought experiment, would this mutation also have reduced (or no) enzyme histidine decarboxylase EC 4.1.1.22 being produced resulting in an abnormally low level of histamine on an ongoing basis and thus increased sensitivity?
A Parallel Thread in Autism?
Antihistamines have been reported to reduce some autism behaviors [2018]. For example “Altered expression of histamine signaling genes in autism spectrum disorder” [2017]. Bacteroides fragilis has been reported to be low with autism. I will leave it to others to explore this further.
One study published in 2013 found that children with autism had lower levels of Bacteroides fragilis in their gut microbiome compared to typically developing children. Another study published in 2017 found that a group of children with autism had higher levels of Bacteroides fragilis in their fecal samples compared to a control group of typically developing children.
Iron plays an important role in brain development and function, and some studies have suggested that iron deficiency during pregnancy or early childhood may increase the risk of autism.
Zinc is also important for brain development and function, and some studies have found that children with autism may have lower levels of zinc in their blood or hair compared to typically developing children.
Riboflavin (vitamin B2) is required for several important metabolic pathways in the body, and some studies have suggested that children with autism may have lower levels of riboflavin compared to typically developing children.
However, other studies have not found a significant association between these and autism.
Chat_GPT.
Bottom Line
There is a scent that specific strains of Bacteroides fragilis may be associated with histamine sensitivity. In an environment deficient of iron, zinc or riboflavin, this strain increases. This strain may not produce histidine decarboxylase EC 4.1.1.22 (epigenetics?) resulting in a much lower level of histamine in the body resulting in “sugar-shock” when a food containing histamines is consumed. We saw above a consistent pattern of having a lower count has an increased probability of histamine issues. A lower count is typically viewed as having less appropriate nutrients available – and the missing nutrients are implied by our analysis.
A common pattern seen by people with Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), Irritable Bowel Disease and other gut disturbances is increasing histamine issues. Mal-absorption due to gut disturbances would result in a dropping of iron, zinc and riboflavin absorption causing this “Bacteroides Histamilis” strain to dominant.
With this model, supplementation with iron, zinc and riboflavin to increase the body’s level to at least the 75%ile may result in significant improvement.
A suggestion for a study would be to measure iron, zinc and riboflavin levels of people with histamine issues against an appropriate matched control population. This may determine if deficiency of just one of this trio is sufficient, or do we need multiple deficiency.
Appendix Statistical Significance Table
The following is general data mining. Remember the lab’s software determines the taxa names using probability. Safest conclusions are when multiple labs report significance in the same direction for the same taxa. Taxa cannot be safely be applied to different labs. Labs report on different bacteria, especially at the species level, on occasion they will pick one name and a different lab will pick a different name.
REMEMBER: These may not be the cause, rather bacteria altered by the bacteria that are the cause.
Taxa name
Taxa Rank
Lab
Histamine Mean
Control Mean
T-Score
DF
Probability
Cyanobacteria /Melainabacteria group
clade
uBiome
6444
268
4.338711
12
P < 0.001
Alphaproteobacteria
class
uBiome
26227
15210
3.283924
269
P < 0.01
Chitinophagia
class
Thryve
94
69
2.824838
330
P < 0.01
Clostridia
class
BiomeSight
619159
558435
2.713198
667
P < 0.01
Deltaproteobacteria
class
uBiome
10291
6987
2.794664
401
P < 0.01
Flavobacteriia
class
Thryve
377
93
4.138491
241
P < 0.001
Spirochaetia
class
Thryve
22731
196
2.747053
68
P < 0.01
Bifidobacteriaceae
family
uBiome
30890
14422
2.643228
474
P < 0.01
Carnobacteriaceae
family
uBiome
815
138
2.86021
182
P < 0.01
Chitinophagaceae
family
Thryve
94
69
2.818824
330
P < 0.01
Chromatiaceae
family
BiomeSight
110
74
2.962499
525
P < 0.01
Coprobacillaceae Verbarg et al. 2014
family
BiomeSight
4986
2981
2.905239
662
P < 0.01
Desulfovibrionaceae
family
uBiome
10288
6984
2.797459
401
P < 0.01
Flavobacteriaceae
family
Thryve
376
95
3.766135
215
P < 0.001
Lachnospiraceae
family
BiomeSight
244569
201657
3.461006
667
P < 0.001
Micrococcaceae
family
Thryve
2041
279
2.732836
198
P < 0.01
Odoribacteraceae
family
uBiome
13802
9604
2.953385
386
P < 0.01
Pasteurellaceae
family
uBiome
11259
3343
2.952883
325
P < 0.01
Rhodospirillaceae
family
uBiome
29014
17878
3.045209
229
P < 0.01
Rubritaleaceae
family
BiomeSight
118
51
3.018423
231
P < 0.01
Streptococcaceae
family
uBiome
12988
6609
3.294864
469
P < 0.01
Syntrophaceae
family
BiomeSight
88
34
3.602406
95
P < 0.001
Weeksellaceae
family
Thryve
826
140
2.707921
42
P < 0.01
Adlercreutzia
genus
BiomeSight
856
346
3.933686
493
P < 0.001
Anaerofustis
genus
BiomeSight
85
45
2.957077
132
P < 0.01
Anaerolinea
genus
BiomeSight
31
18
3.145373
49
P < 0.01
Anaerotruncus
genus
BiomeSight
2476
1835
2.82706
650
P < 0.01
Bacteroides
genus
uBiome
283855
247858
2.683065
471
P < 0.01
Bifidobacterium
genus
uBiome
30859
14357
2.650187
474
P < 0.01
Blautia
genus
BiomeSight
109238
86161
3.171679
667
P < 0.01
Butyrivibrio
genus
Thryve
2238
863
2.78185
414
P < 0.01
Chromatium
genus
BiomeSight
54
23
2.899706
89
P < 0.01
Chryseobacterium
genus
Thryve
112
28
5.423269
18
P < 0.001
Clostridium
genus
uBiome
9065
7003
2.64738
469
P < 0.01
Clostridium
genus
BiomeSight
24536
18253
3.27004
667
P < 0.01
Cronobacter
genus
uBiome
7047
250
3.67629
51
P < 0.001
Desulfomonile
genus
BiomeSight
94
34
3.874419
94
P < 0.001
Desulfovibrio
genus
uBiome
8575
4552
2.939696
243
P < 0.01
Granulicatella
genus
uBiome
839
137
2.901195
179
P < 0.01
Haemophilus
genus
uBiome
12156
3087
3.235353
314
P < 0.01
Henriciella
genus
Thryve
386
176
2.642494
155
P < 0.01
Hungateiclostridium
genus
BiomeSight
4457
2097
2.785968
200
P < 0.01
Limosilactobacillus
genus
uBiome
48109
2843
2.818423
44
P < 0.01
Macrococcus
genus
BiomeSight
1558
388
2.673296
222
P < 0.01
Marvinbryantia
genus
uBiome
4529
2564
2.773658
369
P < 0.01
Negativicoccus
genus
BiomeSight
1370
264
3.038088
353
P < 0.01
Odoribacter
genus
uBiome
8724
5405
3.26612
369
P < 0.01
Pelotomaculum
genus
BiomeSight
259
96
2.808263
236
P < 0.01
Rothia
genus
Thryve
2787
326
2.925505
153
P < 0.01
Rubritalea
genus
BiomeSight
118
51
3.025228
232
P < 0.01
Senegalimassilia
genus
Thryve
2823
617
3.184808
143
P < 0.01
Shuttleworthia
genus
Thryve
105
75
2.606498
318
P < 0.01
Slackia
genus
uBiome
3566
1488
4.3098
154
P < 0.001
Streptococcus
genus
uBiome
12882
6211
3.438454
465
P < 0.001
Trabulsiella
genus
BiomeSight
2381
72
2.944962
84
P < 0.01
Chryseobacterium group
norank
Thryve
112
28
5.423269
18
P < 0.001
unclassified Parabacteroides
norank
uBiome
2321
760
3.29071
91
P < 0.01
unclassified Streptococcus
norank
uBiome
9530
3840
3.188989
429
P < 0.01
Bifidobacteriales
order
uBiome
44064
18404
3.118635
363
P < 0.01
Chitinophagales
order
Thryve
94
69
2.824838
330
P < 0.01
Desulfovibrionales
order
uBiome
10291
6987
2.794631
401
P < 0.01
Eubacteriales
order
BiomeSight
614126
553568
2.710308
667
P < 0.01
Flavobacteriales
order
Thryve
377
93
4.138507
241
P < 0.001
Micrococcales
order
Thryve
1469
345
2.755253
326
P < 0.01
Pasteurellales
order
uBiome
11259
3343
2.952883
325
P < 0.01
Rhodocyclales
order
uBiome
888
327
2.799376
44
P < 0.01
Rhodospirillales
order
uBiome
27884
17148
3.002822
241
P < 0.01
Syntrophobacterales
order
BiomeSight
75
45
2.874101
331
P < 0.01
Chloroflexi
phylum
Thryve
1529
170
3.281628
262
P < 0.01
Cyanobacteria
phylum
uBiome
6444
268
4.338711
12
P < 0.001
Fibrobacteres
phylum
Thryve
180078
34
4.876895
83
P < 0.001
Firmicutes
phylum
BiomeSight
646426
582627
2.769104
667
P < 0.01
Spirochaetes
phylum
Thryve
22731
196
2.747053
68
P < 0.01
Adlercreutzia equolifaciens
species
BiomeSight
549
211
3.480457
447
P < 0.001
Alistipes putredinis
species
uBiome
14784
10219
3.567818
346
P < 0.001
Alistipes sp. NML05A004
species
uBiome
2861
1594
3.211406
270
P < 0.01
Anaerofustis stercorihominis
species
BiomeSight
85
45
2.937001
130
P < 0.01
Anaerolinea thermolimosa
species
BiomeSight
30
18
2.73704
47
P < 0.01
Anaerotruncus colihominis
species
BiomeSight
2335
1749
2.696412
650
P < 0.01
Bacteroides finegoldii
species
BiomeSight
4441
2045
2.613824
552
P < 0.01
Bacteroides heparinolyticus
species
BiomeSight
59
33
2.652157
173
P < 0.01
Bacteroides nordii
species
uBiome
5809
1153
3.833993
148
P < 0.001
Bacteroides reticulotermitis
species
Thryve
724
301
4.303933
341
P < 0.001
Bacteroides sp. 35AE37
species
uBiome
24271
10025
3.724252
219
P < 0.001
Bacteroides uniformis
species
Thryve
39266
26321
3.311011
405
P < 0.01
Bifidobacterium dentium
species
uBiome
18963
288
3.177668
33
P < 0.01
Bifidobacterium longum
species
uBiome
21851
6860
4.131341
271
P < 0.001
Bifidobacterium pseudocatenulatum
species
uBiome
34144
8671
3.752826
94
P < 0.001
Blautia glucerasea
species
BiomeSight
2184
606
2.887145
550
P < 0.01
Blautia obeum
species
BiomeSight
11262
5088
4.539525
642
P < 0.001
Chromatium weissei
species
BiomeSight
54
23
2.899706
89
P < 0.01
Corynebacterium spheniscorum
species
uBiome
12700
3296
2.737118
99
P < 0.01
Desulfohalotomaculum peckii
species
Thryve
35
16
3.191543
21
P < 0.01
Desulfomonile tiedjei
species
BiomeSight
94
34
3.874419
94
P < 0.001
Granulicatella adiacens
species
uBiome
626
100
2.637126
176
P < 0.01
Haemophilus parainfluenzae
species
uBiome
10429
3084
2.943034
310
P < 0.01
Klebsiella oxytoca
species
BiomeSight
2975
337
2.885423
113
P < 0.01
Negativicoccus succinicivorans
species
BiomeSight
1381
248
2.970997
330
P < 0.01
Pelotomaculum isophthalicicum
species
BiomeSight
259
95
2.82543
236
P < 0.01
Phocaeicola coprophilus
species
BiomeSight
18667
2437
3.75374
151
P < 0.001
Phocaeicola plebeius
species
uBiome
104385
39611
2.841081
49
P < 0.01
Porphyromonas bennonis
species
uBiome
9563
2189
2.832604
170
P < 0.01
Ruminococcus bromii
species
BiomeSight
15277
7865
2.709478
558
P < 0.01
Shuttleworthia satelles
species
Thryve
102
71
2.89508
304
P < 0.01
Slackia piriformis
species
Thryve
1676
634
2.804074
126
P < 0.01
Slackia piriformis
species
uBiome
5996
1513
4.050816
41
P < 0.001
Comments from Early Reviewers
“Interesting the connection between histamine and iron. I have some Mast Cell issues which have finally been diagnosed. I also have low ferritin [a blood protein that contains iron], although hemoglobin and even serum iron are within range…. BTW, I recall Hawrelak saying once that histamine behavior of bacteria is strain dependent, not species.”
My original motivation to get into the Microbiome was Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). The Artificial Intelligence was originally tuned for that condition. Cross validation for other conditions has shown that the tuning is robust.
The intent of the site, the blog and videos is to teach people how to be self-empowered with tools and knowledge. In the case of people with ME/CFS and Long COVID, that is often an expectation too far due to cognitive issues (brain fog and other neurological disturbances). This is why many of these blog post are on people with these issues.
The Back Story
I’ve been on a downward spiral now for quite a long time (since June 2021). And ended up unable to walk and at one point, control (or feel) my right leg and both arms below the shoulder. I looked nearly identical to, and had the same state of existence as this guy, with the TPN feeding port to my heart (still in me, here) and all and being given liquids via IV because I couldn’t even drink water. Hospitalized, foley-cathetered, no bowel movements for 20+ days.
I left the hospital for 2 reasons:
To spend some last good days with my wife (in case my research was wrong). I ate a cheeseburger from In-And-Out Burger (and nearly died), rode in a Tesla (here), sat on the roof to enjoy sunsets (here). And generally just did a last-hoorah.
To enable myself to self-treat (which I started immediately upon leaving). The doctors were not allowed (by law) to prescribe what I needed (as it was off-label), and by the nature/constraints of TPN osmolality were feeding me with nearly 80% sugar through TPN (Total Parenteral Nutrition, here), which according to my research (and the impact I saw/felt my body) is HORRIBLE for this condition.
Upon leaving the hospital, I initiated self-treatment and started to recover. I can walk again. Make jokes, and write all this up. Every once a while I even dance a little. And most importantly I can eat at or above my calories each day. And I went from almost no deep sleep at all (monitored by Apple Watch 8) to 1 hour and 42 minutes as of last night.
Namely hesperidin which your suggest says to not take. Tried that before your suggestions. So that confirms at least to some degree your suggestions are likely right.
I hadn’t thought of a lot of the foods I’m evaluating now.
FYI. I was CRAVING peanuts all late 2021 and all 2022 and peanut butter (I would eat them on brown rice crackers!). [See suggestions below]
And I was looking for E. Coli! [See suggestions below] As it’s lacking in ME/CFS and IBS (both of which I have) and also used to produce Kineret, which is a powerful anti-inflammatory drug which is extremely beneficial for recovering from ME CFS (in my opinion) because it causes the body to stop making “thick, clotted blood”. So E Coli makes kinert in your body! Instead of it being cultured outside of your body and then injected. (Which is yet another reason I was looking for it.) I already ordered symbioflor-2, but it will be here in California mid April. [Gave link to Canadian store that will ship Mutaflor to the US]
Oh forgot to mention I took lactobacillus Rhamnosus based my my research before I noticed your big red note to not take it and other lactobacillus because they block the impact of heparin. I think that’s what really got me! Haven’t pooped for 3 days since that mistake! Before that pooped every day for 14.
Analysis
We have one sample available, done via Ombre Labs.
Dr. Jason Hawrelak Recommendations – sits at 89%ile, not ideal, but not too bad.
My Profile
As seen in other reviews, there is a ton of bacteria with token representation. The numbers in each bin below should be similar counts.
Percentile
Genus
Species
0 – 9
60
78
10 – 19
36
49
20 – 29
13
20
30 – 39
13
18
40 – 49
12
12
50 – 59
12
22
60 – 69
8
14
70 – 79
6
10
80 – 89
6
21
90 – 99
9
28
Reporting Distribution
Looking at Potential Medical Conditions Detected, there was only one flagged
Unhealthy Ageing (9 of 17 bacteria matched)
Looking at Bacteria Deemed Unhealthy
The following stands out because of the association with COVID
The top suggestions echoes a frequent suggestion for a subset of ME/CFS: Start each day with barley porridge with walnuts! Another interesting item is peanuts!!! For my own recovery it was important, see these posts from a decade ago: Peanut Butter – a complex food? [2013], Peanuts – A recommended part of diet [2015]
The top suggestions echoes a frequent suggestion for a subset of ME/CFS: Start each day with barley porridge with walnuts! Another interesting item is peanuts!!! For my own recovery it was important, see these posts from a decade ago: Peanut Butter – a complex food? [2013], Peanuts – A recommended part of diet [2015]
The fruit/legume suggestion is a bit vague — fortunately our new Diet Component helps: with the following being more explicit suggestions:
I also checked for Peanut and Peanut butter — and it was not listed (when using the nutrients alone). Remember the Food suggestions are second class — intended to be an auxiliary set of suggestions, not to be a replacement.
The very first lactobacillus was almost 1/2 the priority of the above: lactobacillus reuteri (probiotics). I would suggest avoiding lactobacillus entirely — too high a risk of them causing brain-fog. My typical suggestions for probiotics is to take one for two weeks and then rotate to the next in the list. Remember to track any subjective or object changes (stool shape, frequency). Later you could go on to take them concurrently. Remember, may probiotics produces natural antibiotics hence you do not want to go continuously, but rotate.
Kegg Derived data were all low values, with E.Coli (Mutaflor or symbioflor-2) being the highest available single species probiotic.
My suggestion is to do the suggestions for 2 months and then resample and do the next course adjustment.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
Below is a guest post of someone that has done a lot of their own detail research and is adding Microbiome Prescription into his treatment plan. He has made good use of my original/complementory site, CFS Remission. See this post on his microbiome: Once More, a Long COVID patient
ME/CFS, COVID-19 Post-Sequelae & Mental Health
Postulation Summary:
The root of long-COVID, ME/CFS and many unsolved illnesses is a genetic propensity towards immune system dysregulation that is triggered by environmental such as infection, trauma, stress, diet and/or toxin exposure (detailed below), resulting in a cascade and feedback loops of inflammation, gut dysbiosis, nutrient deficiency, infection, under-production of blood and most deleterious, production of poor quality blood that is “aged and poor quality” and filled with fibrin micro emboli.
There are multiple inflammatory mechanisms, but as the disease progresses, the main inflammatory mechanism that causes “aged, clotted blood” seems as a result of senescent T-cells (here)which are behaving as if the body were dying/bleeding out, largely in response to persistent gut dysbiosis/infection, aggressively releasing inflammatory cytokines and triggering excessive clotting. Which together then results in further feedback of the above-mentioned issues, which feeds back into further stress on the T-cells.
The resultant feedback mechanisms of inflammation, microclotting and poor blood quality then leads to a dizzying array of secondary problems and symptoms (examples below) – which vary per person based on their genetics, lifestyle, and physical/organ structure but fit with all the major findings of Long-COVID, Nature.
For those who do not naturally recover (see divergence of response, below), the inflammation, gut dysbiosis, infection, micro emboli, and poor blood quality cause feedback loops, sometimes with a continuous viscous downward cycle, resulting in severe ME/CFS (detailed here).
The tiny blood clots, which are indicative of the poor blood quality, are so small that they are undetectable via normal scans (CT, MRI, XRAY) and blood tests. New tests (e.g. WebMD, NIH) and old/discontinued blood tests (e.g. blog) both could catch these. But normal blood tests cannot. There is now an online symptom-based test (apheriscenter) and a blood test at Mount Sinai in New York, WebMD.
In this disorder, fibrin, the smallest of the clotting factors (see them all here) clot over the capillaries throughout your whole body (biopsies here), which in combination with systemic and chronic inflammation from a dysregulated immune system, and importantly – T-cell induced inflammation (via IL-1β, TNF-α, etc.), which is deleterious to blood production and quality (“aged, clotted” blood (NIH)) – reduce oxygen and nutrient delivery to every muscle and organ – causing feedback cycles of fatigue, muscle pain, infection, further gut dysbiosis, and general organ/muscle/brain dysfunction all the way to the mitochondrial level.
This inflammation- and microclotting- induced low-oxygen environment forces the mitochondria to move from aerobic operation to anaerobic, resulting in the often-observed (but not explained) insulin resistance in ME/CFS (e.g. here) as the mitochondria cannot use glucose without the presence of oxygen. This also explains why mitochondria dysfunction has so often been observed in biopsies ME/CFS patients (e.g. here).
If/as the condition worsens (see divergence of response, here), progressively severe MCAS (NIH) and associated environmental/food sensitivities are triggered.
The fibrin deposition and low oxygen environment also makes it significantly easier for pathogens of any kind to evade the immune system (which normally uses oxygen as a primary defense, e.g. here), which can then sometimes result in viral and/or bacterial reactivation (e.g here), and explains why so many can recover using hyperbaric chambers (e.g here, NIH).
The combination and feedback of concurrent (and potentially progressively-worse) issues including progressively-worse inflammation, blood clotting, rampant infections, MCAS activation, poor blood quality, and vascular damage is part of the reason ME/CFS is considered so hard to treat.
It is possible to treat.
But it requires early, aggressive, parallel action and attention to the body’s response in a coordinated and monitored approach to make sure that not just one symptom is being addressed, but the root causes are being addressed in parallel.
The treatment is multi-pronged (detailed below), involving fixing gut dysbiosis, inflammation, energy production, whole body oxygenation, infections, and most importantly, poor quality blood production.
Ideally, the treatment should be data-driven, taking advantage of
Genetic information on propensities for inflammation (TNF, IL-1B, etc. e.g here)
Thorough analysis of (frequent) fecal testing for gut pathogens and lack of useful bacteria and how to address them (e.g. here)
Blood work for markers such as TNF, IL-1B, cytokine activity, ferritin, usable iron, and reactivated viruses to guide what supplements and/or drugs to use to suppress chronic inflammation.
A good analogy for treating this disease is like finding and treating cancer:
Attack it with everything you have, as soon as you can, before it gets worse.
“Do no harm” in cancer would mean not starting treatment and “just seeing what happens”.
And that’s the crux of the problem:
Nearly always this disease is treated by one symptom at a time, instead of being treated aggressively like cancer in a holistic and monitored way.
And for many, this means seeing doctor after doctor until (like me) they end up in a bed-bound existence with the potential of no hope of recovery, e.g. here.
And for millions (e.g. here) this means living what patients describe as “a continued nightmare version of my life” and removal from the workforce (perhaps permanently), e.g. CNN.
And overall, I think there’s going to be a huge shift in medicine as a result of Long-COVID/ME/CFS where diseases are treated based on the 3 things mentioned above; genetic information, gut biome status, and blood work – and all 3 are factored in to advise overall non-prescription (food, supplement) and prescription (if needed) treatment.
In my self-treatment, I’m piecing this together using disparate tools, but the whole process can and will be fully automated.
The discoveries from this automation will likely solve most/all mental illnesses.
A Note on Severe ME/CFS
If the above postulation holds water then this disorder in its severe form (which effects about 25% of ME/CFS sufferers, here) is of the same nature as Lupus. Lupus, which carries nearly all the same symptoms and immune dysregulation as severe ME/CFS, is put into remission via CAR T Therapy (e.g. here, details below).
And therefore CAR T Therapy (e.g. here, details below) is likely have a meaningful impact on the quality of life of severe ME/CFS patients (e.g. here), if not put them back into full remission. And for non-severe, anticoagulants and natural supplements, below, will bring most back to full health. Anecdotally, this author has experimented on himself with:
T-cell stimulants (AHCC, NIH, NIH) (which acts via IL-1B)
Resulted in the condition overnight getting severely worse. Nearly unbearable pain and flares of all symptoms.
T-cell suppressants (e.g. Rapamycin, NIH, and supplements below)
Resulted in the condition overnight improving, and continuing to improve (but at great risk to the author, as Rapamycin carries immunosuppressive risks).
Personal Note on Sources and Special Thanks:
Much of the sources from NIH studies/etc. that I wanted to link in this document may not have been linked because my health deteriorated VERY quickly after finally figuring out what the source of the disorder is and was unable to convince doctors to take drastic action, so I ended up in the same state as this guy – unable to eat, paralyzed except my left arm, unable to urinate, defacate, eat, or drink liquids.
Armed with my understanding of the disorder, and the doctors’ unwillingness to follow this document in-hospital, I requested to leave the hospital to die in peace (via starvation).
Upon leaving the hospital, I started aggressive treatment based on the above-summarized and below-detailed thesis. And have improved back to the point where I can eat my calories every day, and I have regular bowel movements (once a day).
The triggers for this disorder seem to be the following:
Viral or bacterial exposure (listed in order of severity):
SaRS (2003)
Lyme
West Nile
COVID-19
Epstein Barr
RSV
Trauma
Surgery
Childbirth
Internal organ damage
Food poisoning
Bacterial or Fungal
Prolonged Stress
Environmental Toxins
Mold
Most commonly it is 2 or more of the above that trigger the disorder.
For example, in my case, I had COVID-19 in early 2020 with no discernible change in quality of life, aside from heightened anxiety (a sign of microclotting/inflammation in the brain) for a month or two after my COVID-19 infection.
But then June 12th 2021 I had trauma to my small intestine, which initiated my downward spiral.
The Nature of the Disorder
Short-form description of the disorder:
The triggers result in inflammation, gut dysbiosis, poor blood quality, and excess fibrin clotting of capillaries resulting in low oxygen and nutrients to the whole body.
This causes fatigue, brain-fog, and just general malaise that worsens with activity.
Opportunistic pathogens take advantage of the low-oxygen environment and the resultant compromised immune system. here
The increased pathogenic load (viral, bacterial, and/or fungal) often result in further triggering of the disorder.
The body progressively goes further into a mode of panic as a result of the above, eventually resulting in progressively-more-severe systemic inflammation, MCAS sensitivities, poor blood quality (“aged blood”) and resultant vascular damage.
There’s a huge divergence in response per patient (more below).
For some, the cycle self-corrects, for others, they are held at a lowered quality of life (long-COVID), and for the worst, the cycle gets progressively worse until fully bed-ridden or close to bed-ridden (severe ME/CFS, POTS, Fibromyalgia). For those that self-correct, they may never get to the state of severe inflammation/MCAS.
In all cases, the symptoms vary wildly from patient to patient, depending on which organs or portions of the body are impacted worst by the inflammation and microclotting and the severity of the genetic propensity towards this disorder. Some have predominantly neurological symptoms, some have predominantly pain, and others suffer primarily from mental symptoms (brain-fog, etc.). It all comes down to which organs are most severely impacted.
For me, it all started in the gut after trauma to my small intestine, which was 1.5 years after getting the first-wave COVID.
Long-form description of the disorder:
The triggers result in IL-1β-driven inflammation, overproduction of fibrin, the smallest portion of blood clots (made with fibrinogen, see Figure below) in the body concurrent with exhaustion of the enzymes (kinases) that consume the fibrin, and progressively worse blood quality as a result of IL-1β’s impact on the body’s capability to produce high quality blood (see example here).
The above results in capillaries (the smallest of the vasculature in the body) being covered over by fibrin and/or inflamed shut.
This results in organs/muscles/etc. not receiving enough oxygen from red blood cells.
And this low oxygen state has several negative impacts:
General fatigue (oxygen is what allows the mitochondria to operate aerobic instead of anaerobic).
Rampant infections, including viral, fungal, and bacterial. The reason is twofold:
As a result of the clotting, the immune system itself has less oxygen to use for energy to fight infections.
The immune system has a harder time getting to infected tissues, as similar to the red blood cells, it is blocked at the capillary level by inflammation and/or micro-emboli.
Body entering further levels of distress (measurable with low heart rate variability) and visually evidenced by progressively-worse inflammation.
Insulin resistance and diabetic-like response to sugar, which fits with the significantly-increased risk of developing diabetes following COVID infection, here. (Recall that mitochondria in the absence of oxygen go anaerobic, and thereby do not consume glucose, here.)
Important Diagnostic Note: One easy way to measure the low oxygen state is to read out the perfusion index say measured at the fingers, or best, toes. A normal/healthy person will be significantly higher (usually by 10x) than someone suffering with this microclotting/microcirculation disorder.
I am 0.3 typically at my thumb (using this), whereas healthy volunteers are typically 5+.
And Sp02 measurement devices cannot get a reading at my toes. Whereas in healthy volunteers the toe readings are identical to fingers.
Both of which are quick/easy indications of microcirculation issues.
If 1 is not stopped (see Divergence of Response below), then overproduction of Histamine occurs as the body goes deeper into a stressed/panicked state and begins to enter severe MCAS territory – with associated sensitivities to foods, chemicals, and pharmaceutical fillers/dies/etc.. (Again, you can monitor HRV decreasing over time during this, which I have a full log of myself over 3+ years.)
The overproduction of Histamine/MCAS/IL-1β inflammation (more here) results in a vicious cycle:
General inflammation body-wide (including the the brain – brain fog)
Lower absorption in the small intestine, resulting in malabsorption/malnutrition/vitamin-deficiency.
Ischemia-reperfusion injury to the intestines (here) which reduces gut motility – resulting in higher likelihood of SIBO and Candida – and further reducing absorption.
Red Blood Cell (RBC) and vascular damage resulting High ferritin levels (400 to 500 in my case) while usable iron in the blood is low as the body tries to keep up with blood production in the face of RBC damage and malnutrition from b.
The loss of red blood cells convinces the body that it is indeed bleeding out, the response-to-which is (1) more fibrin is release, and (2) a stronger Histamine/MCAS response, and the cycle continues.
The IL-1β inflammation and fibrin deposition leads to multiple mechanisms that result in poor blood quality and low oxygen-carrying blood volume. And the (progressive) MCAS results in inflammation which further reduces oxygen perfusion – perpetuating the downward cycle. It is important to note that here we are referring to the total amount of oxygen-carrying blood in the body, which cannot be measured with blood samples. The way to measure include radioisotope testing (e.g nuclear medicine imagine as mentioned here and here) or a total blood transfusion where blood volume is measured. NIH on the fibrin deposition here.
First is the near-constant overproduction of histamine to fight the clotting.
The histamine levels are sufficiently high to damage or destroy red blood cells and damage the vasculature (e.g. here).
And these levels also damage the vasculature.
Second is malnutrition.
The inflammation results in intestinal malabsorption which results in malnutrition, and in severe cases (like mine) constant weight loss.
The malnutrition results in the body having a harder time producing red blood cells (and likely equally, plasma).
Specifically, in blood tests of those impacted, usable iron will be low (as the body is trying to replace destroyed blood) while ferritin is high (which eliminates hemochromatosis as a cause of the issue – and many doctors will expect hemochromatosis given the high ferritin).
Third is the process of blood production itself.
The persistent IL-1β inflammation impacts the mechanisms through which blood is produced from stem cells in bone marrow.
This same phenomenology is observed in regular aging. See here. In severe ME/CFS you feel like a 100-year-old, and the blood process seems nearly identical.
“Treating elderly patients with anti-inflammatory drugs blocking IL-1B function should help with maintaining healthier blood production.”
Interestingly, severe acute COVID cases have resulted in emergency authorization of Kineret® (Anakinra) here in treatment of such patients as it is understood that IL-1β inflammation and commensurate macro-clotting is what quickly results in hypoxemia and death in severe acute COVID-19 patients.
Which further reinforces the author’s postulation that a “slower burn” version is at the root of post covid sequelae and ME/CFS.
The Divergence in Response
There seems to be 3 categories of body responses once the clotting disorder triggered:
Natural recovery. High-anxiety, fatigue/malaise may last weeks, months, or years after COVID, and the body naturally recovers with rest and relaxation.
The body over time regains the capability to clear reduce the inflammation, clear the clots, and restore healthy blood production, returning to normal health.
Steady-state reduced quality of life/energy. The body seems to find an equilibrium of malaise and stays there.
The body stays at an inflamed/clotted level, getting neither worse nor better.
This class is likely treatable with supplements and OTC medications only (i.e. no prescriptions required)
Continual downward spiral.
In this case, the inflammation, clotting, infection, inability to produce healthy blood and malnutrition continually get worse until organ failure occurs (heart attack, liver failure, intestinal failure, or aneurysm/stroke), usually after years of slowly losing physical and mental capabilities.
This case usually requires supplements and prescriptions in an aggressive regimen of anti-inflammatories (MCAS stabilizers), anti-coagulants, immune support, and IL-1β suppression (e.g.Anakinra or similar; or HELP Apheresis, here) to stop the inflammation, improve blood quality, and improve microcirculation and body-wide nutrient delivery.
Once the cycle is mostly broken, treatment can then be continued with vascular dilators to clear out the remaining excess fibrin.
And it’s worth repeatedly stressing that the impact of the inflammation, poor blood quality, and clotting varies extremely per person.
This is why the disease is so confusing.
In some, the brain may be impacted the most (brain fog, or anxiety, non-sequitur thinking, mental disorders, with no other (noticeable) symptoms.
In others, unexpected heart attacks while otherwise young/healthy may occur (e.g. here) and other symptoms may note even be noticeable. In others, dysautonomia. Others, severe food intolerances. Others, strange neurological symptoms.
This is because it all depends on which organs, per person, are most susceptible to the clotting and inflammation – as well as the severity of genetic propensity – and the individual’s diet, stress, and environmental factors. And often the less-severe symptoms may not even be noticed by the patient (in the face of the more severe symptoms).
The Overall Approach to Treatment
Recovering involves going after a cascade of problems, with varying degrees of aggressiveness, depending on the severity of the patient.
The 5-pronged approach involves treating the following cascade, in that order
Chronic Inflammation
Poor/Aged Blood Production Quality
Excess Fibrin Coagulation
Suppressed Immune System and Gut Dysbiosis
Damaged Vasculature
Note that if the disease is not progressed far, the supplement-only approach will work and likely only A, B, and C are needed. And in light conditions, even A alone with supplements only is enough.
In fact the supplement-only approach of A, B, and C worked on me very effectively (from 1 minute walk capability to 30 minutes of walking and 30 minutes of biking). Unfortunately at that time I was not confident in my self-treatment and a team of doctors who were treating me for POTS (a secondary condition) convinced me to abandon this self-treatment plan, and over 10 weeks I got very sick following their treatment. After which I re-initiated my self-treatment plan and started to improve again – but in those 10 weeks I had become severely ill (lost 45lbs) – so I am now on prescription approach and starting to improve again.
A. Treating Chronic Inflammation:
The main inflammatory mechanism in this disease is Histamine released from a variety of sources, by the potent proinflammatory interleukin cytokine IL-1β and TNF-α seem to be common.
The mechanisms vary per person, so doing genetic testing is highly recommended, along with leveraging Genetic Lifehacks, here to decode the meaning for diet, supplements, and drugs to help you recover, based on your genes. And one requisite aspect of getting inflammation down and keeping it down is rebalancing your gut Microbiome, which often means checking (and understanding) the current state, which can be done with Microbiome Prescription, here, with details below.
Either way, as the disorder progresses, the inflammatory mechanisms result in progressively poorer blood (clotted, aged) blood being produced, which then triggers even more MCAS/histamine release to break blood clots (NIH).
So the core focus for anti-inflammatories should be anti-histamines and in essence, treatment of MCAS – H2 and H1 blockers, supplements that reduce or consume histamine, and foods that are anti-histamine (and for sure not high in histamine), but with a particular focus on inhibiting IL-1B. A reference on MCAS treatment is here.
However, it is critical to stress that we need to treat not only MCAS. That is to say, MCAS is a result of the clotting disorder and the clotting disorder is a result of MCAS (and IL-1B). And one of the trickiest parts is that some of the traditional treatments for MCAS actually trigger the clotting disorder, and vice-versa. So when taking anything to treat MCAS, double-check to make sure they do not trigger the clotting disorder. An initial list of which is here. But please double-check anything you take to make sure it is not a trigger for the clotting disorder – as it is the root of the problem – so triggering it makes all secondary syndromes worse.
And note that this process of getting MCAS/histamine inflammation down is SLOW; 14-30 days to see an impact on histamines in the body, from here (and this fits my experience). And generally the mast cells (and mast cell signaling system including cytokines and leukotrienes) are having to be retrained over time to be less over-active.
And before starting any supplements, see Advice on (Self) Treatment here.
Much of the information below is pulled from the resources below, and then I am in the process of cross-checking the recommendations against if they cause other adverse reactions, here.
Genetic Lifehacks, here – focus on decreasing inflammation based on genetic propensity
Hoffman Centre, here – focus on overall MCAS treatment
Carlos Tello, PhD, here – focus on Leukotriene inhibitors
And before jumping into it, a background on energy supplementation, gut inflammation, gut dysbiosis, and excess inflammation and histamine release – as they are all tightly related.
And to explain this, let me use ChatGPT, as it can do it better than me, about what cAMP is, and why it’s important.
“Cyclic AMP (cAMP) is a molecule that plays an important role in a wide range of biological processes in the body. It is a type of second messenger, which means that it acts as an intermediary between external signals and the internal response of a cell.
cAMP is formed from ATP (adenosine triphosphate) through the action of an enzyme called adenylate cyclase. It is involved in the regulation of numerous cellular processes, including energy metabolism, gene expression, and the response to various hormones and neurotransmitters.
When a cell receives a signal, such as a hormone or a neurotransmitter, it triggers the activation of adenylate cyclase, which then catalyzes the formation of cAMP from ATP. cAMP then goes on to activate a variety of protein kinases and other signaling molecules, which ultimately leads to changes in cellular function.
cAMP has been implicated in a wide range of physiological processes, including the regulation of blood pressure, insulin secretion, immune function, and memory formation, among others. It is also an important target for pharmacological interventions, with numerous drugs designed to target cAMP signaling pathways for the treatment of various diseases and conditions.”
And recall that in ME/CFS, mitochondria dysfunction is always found (which is a result of low oxygenation, and inflammation), resulting in low ATP. So in ME/CFS. Which means cAMP will be low in ME/CFS patients because of the chronically-low ATP.
And further, activity requiresATP (its the energy of cells). And in ME/CFS, there is post-exertional malaise because ATP is used up. And generally, inflammation is found to be high after activity (which lowers oxygenation and ATP production).
Now, we’ve established why ATP is low, resulting also in low cAMP.
Now how does cAMP relate to inflammation?
cAMP regulates the release of histamine.
Low cAMP -> High histamine release (high inflammation)
High cAMP -> Low histamine release (low inflammation)
cAMP regulates pro- and anti-inflammatory activities: drugs that elevate intracellular cAMP levels reduce the production of pro-inflammatory mediators and increase the production of anti-inflammatory factors in numerous immune cells. Source: NIH.
So then the key to getting out of this disease is revolves around all 5 things (Chronic Inflammation, Poor, Excess Fibrin Coagulation, Suppressed Immune System, Gut Dysbiosis and Damaged Vasculature), but one core part of that is supplementing and pacing such that:
The body can make more ATP in a day than is consumed.
The body has enough nutrients to make cAMP, to then reduce inflammation.
That sounds simple, but making it happen is the very difficult part, particularly if you (or your loved ones) have severe ME/CFS.
And note that this is why the multi-pronged approach is needed, as Broccoli and Cauliflower extracts (see below for details), for example, are high in the ingredients that the body needs to make cAMP from ATP… however, if the body is short on ATP, then it cannot adequately produce cAMP – and so adding Broccoli and Cauliflower would not help (and might hurt). So in parallel to taking supplements that reduce inflammation, as below, it is important to take supplements that help the body produce ATP while also balancing your gut microbiome to make sure helpful bacteria are being feed by the supplementation rather than pathogenic bacteria.
And since ME/CFS and Long-COVID’s main symptom is low energy and post-exertional malaise, let’s start with energy supplementation.
Natural Supplements
Energy Supplementation
Energy supplementation is necessary because of the vicious cycle of inflammation, malabsorption, low oxygenation (switching mitochondria to anaerobic), constrained diet (because of SIBO/SIFO), and many other factors among the feedback loop of this disorder.
The goal of energy supplementation is to help the body make ATP even in the face of low oxygenation. To help bootstrap the process. And to do that, supplements that make it easier for the Mitochondria to make ATP are necessary. These include:
Oxaloacetate, NIH, 500mg to 5grams, need one without Vitamin C, like here
Best in morning as it may re-align circadian rhythm per ResearchGate, 1 and 2
D-Ribose, 5 to 15 grams per day
Malic Acid, 500mg to 1.5g per day
And note that anything that either (1) increases oxygenation (e.g. reducing inflammation and/or reducing clotting) or (2) reduces glycation will help the body produce ATP, as mitochondria will naturally produce ATP in the presence of glucose and oxygen. The clotting and inflammation is what is preventing the mitochondria from effectively producing ATP (by forcing them into anaerobic, i.e. no-oxygen, cycle, which effectively results in more energy consumption than production).
And this explains why hyperbaric chamber time has been so beneficial in recovering from ME/CFS/Long-COVID (e.g. here) – it helps the body produce ATP, which then enables cAMP production.
For reducing inflammation, just like correcting gut dysbiosis below, understanding the following will give you a HUGE leg up on recovery:
Your genetic propensity to inflammation (with Genetic Lifehacks, here)
Your current gut microbiome (with Ombre and/or Microbiome Prescription), as SIBO/SIFO and general gut dysbiosis is a HUGE source of inflammation. And in some cases these bad bacteria can feed off of the energy supplementation above, making your condition worse.
Your current labs (e.g. are you high ferritin, low absorbable iron, do you have reactivated EBV, etc.?)
And with that, some general recommendations to reduce inflammation.
Mast Cell Stabilizers:
Vitamin D, probiotics, krill oil:
“A study using an animal model of gut inflammation found that a mixture of krill oil, Lactobacillus reuteri (probiotic), and vitamin D decreased intestinal inflammation, reduced TNF-α, IL-1β and IL-6 levels (inflammatory cytokines), and increased IL-10 (anti-inflammatory).[ref] This may be important for anyone with IBS.” from here, and more details on probiotics that help below.
If you have elevated ferritin but normal or towards-the-low-end iron, you have a form of anemia which is the most common kind in hospitalized patients (see here), which is a result of constant/chronic inflammation.
“Ferritin is an acute phase reactant and a marker of acute and chronic inflammation. It is elevated in a wide range of inflammatory conditions, including chronic kidney disease, rheumatoid arthritis, and other autoimmune disorders, acute infections, and cancer [1, 2].”
Anemia of chronic disease is the most frequent anemia in hospitalized patients. It develops in people suffering from diseases in which there is chronic activation of cell-mediated immunity, such as chronic infections, immune-mediated inflammatory disorders, or malignancy. It’s characterized by the presence of low iron, but increased blood levels of ferritin [4].”
This was the case for this author, and Curcumin always sat poorly, which is explained by it being known in the literature that Curcumin blocks the absorption of iron, making the author’s anemia even worse, source NIH 1 and 2.
Chamomile tea (Apigenin, luteolin) – 1 to 2 cups before bed, here.
Apigenin prevents the infiltration and degranulation of mast cells and suppressed mRNA and protein expression of IL-31 in the skin of mice. Here. Apigenin reduces IL-1B expression as well, NIH
Research has suggested that CoQ10 may have anti-inflammatory effects through several mechanisms. One way it may work is by reducing the production of reactive oxygen species (ROS) and free radicals, which are molecules that can cause oxidative stress and inflammation in the body. CoQ10 is a powerful antioxidant that can help neutralize these molecules and reduce their harmful effects.
In addition to its antioxidant effects, CoQ10 may also modulate the activity of certain pro-inflammatory cytokines, including interleukin-1 beta (IL-1β) and tumor necrosis factor-alpha (TNF-α). Research has suggested that CoQ10 can reduce the production of these cytokines and thereby reduce inflammation. NIH
CoQ10 may also have other beneficial effects on the immune system, such as enhancing T cell function and reducing the production of certain pro-inflammatory enzymes.
Berberine
Has the benefit of also being anti-microbial and anti-fungal (here), helping to remove SIBO/SIFO that’s common in ME/CFS (here)
CAUTION: research drug interactions first! For example do not use with Zyrtec!
“Cannabinoids dramatically improve the symptoms of gastroparesis. Furthermore, an improvement in abdominal pain with cannabinoids represents a breakthrough for gastroparesis-associated abdominal pain treatment, for which there are currently no validated therapies.”
If doing CBD, CBD isolate is recommended as many MCAS patients are allergic to the other parts of hemp oil and THC, source is potentially biased as a vendor, here
Dosing recommendations from here (the author had/has MCAS)
For the first 10 days, 600mg daily – that’s 3 droppers of the 6,000mg bottle.
Day 11-30 – 300mg daily – that’s 1 1/2 droppers of the 6000mg bottle.
Beyond that period, adjust according to need. The lowest level that matches any research would be around 50mg daily.
Like many MCAS treatments, it may not be effective in ME/CFS because of (deleterious) interactions on the other 4 parts of the disease.
“… evidence has indicated a role for CBD in the modulation of mitochondrial processes, including respiration and bioenergetics, mitochondrial DNA epigenetics, intrinsic apoptosis, the regulation of mitochondrial and intracellular calcium concentrations, mitochondrial fission, fusion and biogenesis, and mitochondrial ferritin concentration and mitochondrial monoamine oxidase activity regulation.” NIH, found here
“Thus, under pathological conditions involving mitochondrial dysfunction and Ca2+ dysregulation, CBD may prove beneficial in preventing apoptotic signaling via a restoration of Ca2+ homeostasis” NIH, found here
And note that where CBD may be beneficial, THC is resolutely deleterious:
“THC exposure alters brain maximal oxidative capacity. It impairs mainly the complexes I, II, and III of the mitochondrial respiratory chain and mitochondrial coupling. THC also increases brain ROS production and mitochondrial free radical leak.” NIH, found here
Clinical trials using high doses of DHA/EPA and also measuring specialized pro-resolving mediators (SPMs) show:[ref]
In chronic kidney disease, 4g/day of an omega-3 supplement for eight weeks increased resolvins (RvE1, RvE2, RvE3, RvD5).
In overweight major depressive disorder patients, supplementing with between 1 and 4 g/day of EPA was investigated. The results showed that all of the supplemental doses increased EPA, DPA, and subsequent SPM levels in a dose-dependent fashion.[ref] (Note that this clinical trial didn’t find that EPA was better than placebo at reducing depressive symptoms – everyone improved, even the placebo group.)[ref]
In peripheral artery disease, a 4.4g supplement of DHA/EPA for 3 months increased resolvin E3.
Another study of peripheral artery disease found that a marine oil supplement of 4.5g (DHA/EPA/DPA) increased maresins.
In people with arthritis, a microalgae oil supplement containing 2.1g DHA/day for ten weeks increased SPMs.
Vitamin D, probiotics, krill oil: A study using an animal model of gut inflammation found that a mixture of krill oil, Lactobacillus reuteri (probiotic), and vitamin D decreased intestinal inflammation, reduced TNF-α, IL-1β and IL-6 levels (inflammatory cytokines), and increased IL-10 (anti-inflammatory).[ref] This may be important for anyone with IBS.
Note that fish oil/SPMs seem to have a combo effect with Aspirin, see below in Treating Excess Microcoagulation
Fish oil seems to be best taken in the morning. And need 3+ grams to have therapeutic effect, from here/here, as below:
Summary below of how Fish Oil (and Marine Oil Extracts) impact Resolvins is below, from here.
Notice fish oil impacts many anti-inflammatory pathways.
Traumeel
An herbal pain relief product offered as an injection or cream, has been shown to increase the production of resolvin D2, resolvin D5, and lipoxin A4 after 24 hours (animal study, injections).[ref].
Reduces inflammatory markers in RA, per ChatGPT. Does not impact the function of T-cells and is not immunosuppressent, but reduces IL-1B by up to 70% and other inflammatory markers, per NIH.
More information from manufacture on it here, particularly its impact on TNF and IL-1B
Tripterygium wilfordii
Also known as Thunder God Vine, is a traditional Chinese medicine used for rheumatoid arthritis. Recent research shows that it induced “pronounced formation of specialized pro-resolving mediators (SPM) and related 12/15-LOX-derived SPM precursors, without COX and 5-LOX activation.”[ref] Other research identifies that celastrol is the active component of Thunder God Vine that is responsible for elevating SPMs.[ref]
Note that Tripterygium wilfordii can be TOXIC to multiple organs, so the author does not recommend using it. And this information is provided for context only and if it provides clues to other SPMs.
Zileuton, a leukotriene synthesis inhibitor, also blocks the formation of SPMs.[ref]
Should be avoided most likely for ME/CFS
Leukotriene inhibitors
These help with shortness of breath, nasal/sinus closing, overview of naturals here (and overall and amazing resource)
Ginger blocks the production of prostaglandins and leukotrienes [58], here
“α-LA acts as an enzymatic cofactor able to regulate metabolism, energy production, and mitochondrial biogenesis.” NIH
“In addition, co-administration of LA (alpha lipoic acid) with other mitochondrial nutrients, such as acetyl-L: -carnitine and coenzyme Q10, appears more effective in improving cognitive dysfunction and reducing oxidative mitochondrial dysfunction.” NIH
“Our results showed that FAC results in a significant increase of tissue iron accumulation, oxidative stress, and autophagy and such detrimental effects were reversed by ALA treatment. “ NIH
Bromelain
Helps absorption of Quercetin and other bioflavonoids
Lowers high LDL and Cholesterol which are often resultant disorders in this condition.
It reduces inflammation by blocking the very-potent inflammatory interleukin cytokine IL-1B.
Which then also results in newly-produced blood not being so prone to clotting and overall higher-quality (less aged).
And “poor quality, clotted blood” is being found to be at the root of much of the issue of this disorder, and blocking this inflammation explains it, per NIH here.
CAUTION: This may be problematic for those with reactivated viruses.
Potentially not recommended for ME/CFS because of GI upset issues.
Colchicine: (not recommended; high risk) This anti-inflammatory may reduce inflammation around the lining of the heart (pericarditis) and lungs (pleuritis). Colchicine is also used for pericarditis and may reduce chest pain and breathlessness (dyspnea) in Long COVID.[3]
Used to treat Behçet’s disease (which I think Chris has).
Foods that help
Collagen Peptides and supplements that encourage collagen production.
In ME/CFS, collagen production is lowered (e.g. NIH, NIH).
Correcting this can help pain in the joints, spine, and intracranial pressure (caused by disc atrophy)
Collagen peptides with no additives anecdotally helped me.
For example ibuprofen has been found to block the formation of SPMs (lipoxins, resolvins, and protectins), source here, and found through here (pay wall)).
Aspirin is a very-notable exception, helping to produce SPMs, see details on SPMs above.
alcohol-containing medicines and intravenous vancomycin
In addition to the physical and chemical support above for inflammation, stress, of any kind – even about the disease itself can be a trigger for inflammation – which then reduces oxygenation and ATP production.
And so this stress can trigger your physical condition to worsen – which can trigger more stress. And this becomes a downward spiral.
Depending on the severity of the disease, using techniques to keep yourself calm and stress-free can be equally important. These include:
Deep breathing (6 breathes per minute, into stomach, not chest)
Yoga, if you are that capable – I am not, yet)
Visualization (I do this many times a day)
Calming phrases such as “I’m going to fully recover from this” that you repeat over and over (repetition, whether something is true or not, makes your mind think it is).
The Gupta Program is strong, and not overly expensive, here (I do this every day)
The Calm app is fairly great.
And Amazon has a series of nature and city-view videos that are calming
Sitting and staring at nature (if you can walk)
Sleep
Overproduction of Histamine (from MCAS) results in poor quality sleep and sleep disruptions. And this further triggers the downward spiral. In the literature there are a variety of advised supplements to aid in sleep. The safest and most effective appears to be Glycine. It’s well tolerated and seems to have no side effects even at high doses.
Glycine is considered very safe even in high doses, both in humans and animals. In rats, high doses over four weeks of 2g/kg were not toxic.10 In some cases, doses of up to 30 (!) grams per day were used in human studies. In one case, nausea with vomiting occurred, which caused the discontinuation of treatment in this individual..11(p)
Leaky blood-brain barrier allows this to help directly.
L-Theanine
L-Carnosine
Helps reduce sleep disturbances, best taken at night, and it is beneficial for gut and muscle function as well, see below in correcting gut dysbiosis.
Gut dysbiosis, and histamine release, is one of the primary mechanisms resulting in sleep disturbances.
And the sleep disturbance further disbalances the gut microbiome.
Glycine (and Taurine) have the added benefit of being beneficial for the liver (hepatoprotective effect, here) which is often struggling in ME/CFS. Additionally glycine has been shown to help prevent muscle wasting, per here.
Glycine is also used in the biosynthesis of hemoglobin, which is very important in the maintenance of red blood cell integrity and oxygen transport, per here.
The chronic inflammation will result in nutrient deficiency throughout the body. Most notably, magnesium. If you’re not already taking magnesium, adding it will make you feel significantly better.
Acetylcholine cannot be directly absorbed, so to fix this nutrient deficiency, taking Acetyl-L-Carnitine, which the body readily absorbs and converts into Acetylcholine (see here) is the way to get these levels back up.
The malabsorption will likely mean you are short on nearly all of the B-vitamins. Make sure to take a B-vitamin that uses Niacinamide (Inositol Hexanicotinate) instead of Niacin, as Niacin causes flushing which can make this condition worse, explanation at LiveStrong.
General vitamins, e.g. here. Take a daily (in the morning) multivitamin. Make sure again that it uses Niacinamide (Inositol Hexanicotinate) instead of Niacin, as Niacin causes flushing which can make this condition worse, explanation here.
And try for one without Vitamin K, or little vitamin K, as that vitamin increases blood clotting (NIH).
It is also a powerful anti-inflammatory through multiple mechanisms, see above for details.
Ubiquinol is the more bioavailable form of CoQ10.
Better absorption.
CoQ10 may be more gut-inflammation modulatory and Ubiquinal may be more whole-body inflammation modulatory.
“These results show that ubiquinol-10 may enhance mitochondrial activity by increasing levels of SIRT1, PGC-1α, and SIRT3 that slow the rate of age-related hearing loss and protect against the progression of aging and symptoms of age-related diseases.” NIH, found here.
Malic Acid is reduced in ME/CFS patients because of diet, poor absorption, and typically Candida infection, and is a key part of the Krebs cycle.
It’s lacking is suspected by the mitochondrial dysfunction in muscles (NIH), and helps to make the mitochondria less dysfunctional (NIH).
Collagen and supplements that encourage collagen production.
In ME/CFS, collagen production is lowered (e.g. NIH, NIH).
Correcting this can help pain in the joints, spine, and intracranial pressure (caused by disc atrophy)
Collagen peptides with no additives anecdotally helped me.
B. Treating Poor Quality Blood Production (Aged Blood):
Novel research in anti-aging (and ME/CFS is like premature aging) has found that blood quality is one of the main causes of (premature) aging. And specifically, the literature has found the inflammation caused by senescent T-cells is what causes chronic inflammation (e.g. here). Among the T-cell induced chronic inflammation, and likely the most deleterious, is an overactive inflammatory cytokine interleukin-1β (IL-1β) – which has been shown experimentally to result in aged blood. And additionally has been demonstrated to be reversible (e.g. here) by blocking IL-1β. And it is this author’s postulation that using an antagonist to block this will result in drastic improvements for ME/CFS patients, just like has been found for elderly, here. And this fits with multiple practitioners having success with ME/CFS (and Long-COVID) patients by using treatments that show anti-aging effects, e.g. here.
But most importantly, addressing the source of the IL-1β (i.e. senescent T-cells) will be even more beneficial, longer-lasting, and carry fewer risks.
The most effective way to do so is through CAR T Cell therapy, which is usually used for cancer (e.g. here), but has recently been found to be extremely effective in treating auto-immune diseases as severe as Lupus (e.g. here).
And given that the mechanisms behind Lupus and ME/CFS appear incredibly similar, with ME/CFS being more an immune system dysregulation rather than a full-blow auto-immune disorder, treatment of ME/CFS with CAR T Cell Therapy is even more likely to be successful than with Lupus – where great success has been had!
The author is actively researching the exact T cells impacted, but the literature seems to indicate, CD8 T cells become exhausted/senescent (here). One patient I’ve interacted with here also has senescent CD57+. And it is looking like T cell lymphocytes
So then the approach breaks into 3:
CAR T Cell therapy
Resolves the core issue in this disease, senescent, malfunctioning T-cells
Interleukin-1 Receptor Antagonists
This can be done via foods in not-severe cases, supplements for those harder impacted, and then prescription drugs for those who are worst impacted.
Does not treat the underlying T-Cell senescence and dysfunction, but reduces inflammation and may allow the body (even in sever cases) enough change to recover.
Author’s note: Technique 2 is working for me, coming back from being paralyzed nearly completely (including bladder,
HELP Apheresis
This removes the clots (and other deleterious elements) that the senescent, malfunctioning T-cells are constantly producing.
Since this is furthest from addressing the production of blood that’s high quality, it is the most likely to be of short-term help, or no help at all, e.g. here
Albeit the temporary reduction in blood clotting in the body, in combination with parallel treatment of secondary disorders, may be enough for the body to “snap out of it” – which seems to be the case for many who are treated.
Natural Approach – Foods
Interleukin-1 receptor antagonist (IL-1Ra) is a protein that acts as an inhibitor of interleukin-1, a pro-inflammatory cytokine. IL-1Ra is not a nutrient found in food, but some foods have been shown to have anti-inflammatory properties and may help to regulate levels of interleukin-1 in the body (source: chatGPT):
Omega-3 fatty acids found in fatty fish such as salmon, mackerel, and sardines.
Ginger, turmeric, and other spices that contain anti-inflammatory compounds.
Fruits and vegetables, especially those high in antioxidants such as berries, leafy greens, and dark, colorful produce.
Whole grains and legumes, which contain fiber and other nutrients that may help to reduce inflammation.
Nuts and seeds, which are a good source of healthy fats and antioxidants.
Some patients (the author included) have passed the point where they can eat all the foods on that list (because of gut dysbiosis – SIBO/SIFO – and the inflammatory response caused thereby when the foods are consumed). So supplementation can be extremely helpful. Below are supplements of interest.
Supplements for Suppressing IL-1B:
Akkermansia (from ChatGPT)
One study published in the journal Cell Reports showed that supplementing with Akkermansia muciniphila in mice reduced the levels of HMGB1 in the blood, improved intestinal barrier function, and reduced inflammation. This suggests that Akkermansia may have potential benefits for reducing inflammation in the body, in part by modulating the levels of HMGB1.
Studies have shown that HMGB1 can induce the production of IL-1β in various cell types, and that IL-1β can in turn upregulate the expression of HMGB1. This suggests that there is a feedback loop between HMGB1 and IL-1β that can contribute to the persistence of inflammation.
Elevated levels of HMGB1 and IL-1β have been associated with various inflammatory conditions, such as sepsis, rheumatoid arthritis, and inflammatory bowel disease. Thus, targeting the production or activity of these molecules has been a focus of research into the treatment of these conditions.
And according to ChatGPT (here), all the following should help suppress IL-1:
“Interleukin-1 (IL-1) is a pro-inflammatory cytokine that plays a crucial role in the immune response and inflammation. While there are some supplements that have been shown to have anti-inflammatory effects, there is limited evidence to suggest that any specific supplements can directly block IL-1. However, some supplements may help modulate the immune response and reduce inflammation, which may indirectly lead to a reduction in IL-1 activity.
Here are a few examples of supplements that may help reduce inflammation and potentially modulate the activity of IL-1:
Supplements Summary
Omega-3 fatty acids: Omega-3 fatty acids are known for their anti-inflammatory properties and may help reduce the production of pro-inflammatory cytokines, including IL-1.
Curcumin: Curcumin is a compound found in turmeric with anti-inflammatory properties. It may help reduce the production of IL-1 and other pro-inflammatory cytokines.
Resveratrol: Resveratrol is a polyphenol found in red wine, grapes, and some berries with antioxidant and anti-inflammatory properties. It may help modulate the immune response and reduce inflammation.
Quercetin: Quercetin is a flavonoid found in many fruits, vegetables, and herbs with antioxidant and anti-inflammatory properties. It may help reduce the production of pro-inflammatory cytokines, including IL-1.
Vitamin D: Vitamin D is known to have immunomodulatory effects and may help regulate the immune response. Some studies suggest that it may reduce the production of IL-1 and other pro-inflammatory cytokines.
It’s important to note that while these supplements may have some anti-inflammatory effects and potentially modulate the activity of IL-1, the evidence is still limited, and more research is needed to fully understand their effects on the immune system and inflammation. Additionally, it’s always best to talk to a healthcare provider before starting any new supplement or making significant changes to your diet.”
And this author’s experience has been that all of these help substantially. Before I got severely ill, I was taking all of these up until a team of doctors told me to stop taking them.
Prescription Drugs (treatments) for suppressing IL-1B:
NOTE THAT THESE CARRY SIGNIFICANT RISKS!
CHECK WITH YOUR DOCTORS ON THESE, PARTICULARLY FOR SIGNS OF EXISTING INFECTIONS.
Specifically, in the research on this phenomenon, it has been found that Kineret® Anakinra is very effective at preventing this inflammation.
It is however hard to convince a doctor to give you this, even though it is FDA approved for treating acute COVID (but not long-COVID). See here. These work by blocking IL-1B (IL-1Beta), which is a potent inflammatory.
Summary:
Likely the safer approaches:
Aptemer BC 007 (#1 recommendation, but not available until 2024) (details below)
This may be the only exception WRT risks for existing infections
Looks very effective, but likely not available until 2024, per here
Need to see if there are other sources for it.
IvIg
Shown to reduce inflammation and lower IL-1B
Needs to be done long-term.
Note that a 1-time administration to the author had a net positive impact. But the literature indicates long-term is needed for ME/CFS to keep the inflammation down.
Likely very risky, particularly if you have existing viral/bacterial re-activation:
Rapamycin / Rapamune / Sirolimus (dosing WIP, seen 4-6 mg one time weekly)
Big additional risk: High lipids and glucose resistance.
“Rapamycin is a drug that works by inhibiting a protein called mTOR, which plays a key role in regulating cell growth and metabolism. Interleukin-1 beta (IL-1β) is a cytokine that is produced by immune cells and plays a key role in the inflammatory response. There is some evidence to suggest that rapamycin may have potential benefits for reducing IL-1β levels and mitigating inflammation.
Some studies have shown that rapamycin can inhibit the production of IL-1β in various cell types, potentially through its ability to modulate the immune response and reduce inflammation. For example, one study published in the journal Frontiers in Pharmacology showed that treating human dendritic cells with rapamycin reduced their production of IL-1β in response to lipopolysaccharide (LPS), a bacterial toxin that can trigger an inflammatory response.
In addition, some studies have suggested that rapamycin may have potential benefits for reducing inflammation and improving immune function in a range of inflammatory conditions, such as rheumatoid arthritis and other autoimmune diseases. While the exact mechanisms of action are still being studied, it is possible that rapamycin’s ability to inhibit mTOR and reduce IL-1β levels may play a role in its anti-inflammatory effects.”
And it has the benefit of being an antibiotic (NIH) that’s also antifungal (NIH), both of which are helpful for fighting the gut infections that are so common in ME/CFS.
See here for information about how to buy. Includes info about importing and also for finding Rapamycin-friendly doctors locally who might prescribe it. Note to use SpeedPost EMS for medicine shipments where you do not have a prescription, as other shipping companies require a prescription.
Potent anti-aging (and ME/CFS is like advanced aging) per NIH
And this post, originally on reddit but censored, had many helpful links. Replicated here.
And it also reduces inflammatory Macrophage activity, which then could be why it is shown to reduce PEM in ME/CFS, per NIH.
Explains why the blood clotting occurs in ME/CFS, here.2
More information from Dr. Green, who’s treated thousands, here
Note that taking it with CBD doubles or triples its activity, here, but can result in toxicity.
Some note taking Rapamycin off and on can be beneficial, here
Ken Lassessen also has a piece on it, here – and the reader notes the exact thing I noticed, VERY strong die-off symptoms from 1mg of it (same dose I’m doing).
Great post on someone who was housebound for 13 years improving on it, here, but then getting worse over time.
0.5 mg on alternate days for 24 weeks in a 2 : 1 ratio.
Low-dose sirolimus immunoregulatory therapy selectively upregulated Tregs and partly replaced the usage of immunosuppressants to control disease activity without overtreatment and evaluable side effect. Further study is required using a large sample of RA patients treated with sirolimus for a longer period. This trial is registered at the Chinese Clinical Trial Registry (http://www.chictr.org.cn/showproj.aspx?proj=17245).
Dosing for anti-aging, here is 6mg every week or so, just like the reddit post.
Great post on reddit about immune system dysregulation:
Post vax or Covid long hauling (they’re 99% the same thing!), are immune disorders (dysregulation) at core. Note: this does not always mean auto-immune! It’s an immune dysegulation (e.g. T, NK, B cells) that is primarily expressed as various vascular disorders and secondarily as neurological disorders (nuance here between neuo precipitated by vascular and direct effects from immune)
If you were going directly after vascular, then the focus would be on a mix of anti-platelet, anti-coagulants, and endothelial stabilizing medicines and supplements. Rapamycin would be going after the upstream immune dysregulation.
Rapamycin has a long half life (50hrs +/-) and it takes 5.5 half lives for a drug to reach peak concentration, so maximal effects would not begin until after 12 days or so. Even then, immune modulation takes time. Any more immediate benefits would be from anti-inflammatory actions (cytokine regulation) and neuro chemical changes that effect signaling.
In diverse studies, rapamycin extends life span in mice (see for numerous refs. 2,3,4,5). It also improves health not only in rodents, but also in dogs6 and primates7, and its analog everolimus improves immunity in elderly humans without causing side effects8,9. Here
So mTOR, if over-active (and I postulated it is in ME/CFS), actually blocks Gluconeogensis and lipolysis. And Gluconeogensis and lipolysis are both way too low in ME/CFS
“Because mTOR is a nutrient-sensing pathway, it can be deactivated by fasting and severe calorie restriction (CR), which exert metabolic effect that are somewhat similar, but not identical, to those of rapamycin42.”
This is why I feel better when I don’t eat!
This scenario is in agreement with the hyperfunction theory125,126, which posits that aging and age-related diseases are associated with cellular (e.g., hypertrophy, hyper-secretory phenotypes, or SASP) and systemic (e.g., hypertension, hyperlipidemia, pro-inflammation, and hypercoagulation) hyperfunction. mTOR-driven hyperfunction eventually leads to organ damage, but it can be suppressed by rapamycin/everolimus125.
Intermittent rapamycin or a single high dose
Intermittent rapamycin administration (pulse treatment) was proposed in 2008, as a means of rejuvenating stem and wound-healing cells, thereby improving wound-healing instead of impairing it, as chronic treatment with rapamycin did138. Intermittent administration (e.g., once a week) can be considered a single dose repeated over time. In mice, a single dose of rapamycin does not cause glucose intolerance, but a single dose of a dual mTORC1/mTORC2 antagonist does causes it128. Consistent with that finding, weekly treatments with rapamycin for 22 weeks inhibited mTORC1 and protected against insulin resistance in C57BL/6 mice fed a high-fat diet, whereas mTORC2 activity remained intact70. Higher single doses of rapamycin can be used when administration is intermittent than when it is chronic, and it appears that it is the peak concentration of rapamycin that is especially beneficial2. This is in part because high peak levels enable rapamycin to cross the blood–brain barrier. For example, rapamycin prevents obesity associated with hyperactive mTOR in hypothalamic POMC neurons139. Furthermore, intracerebroventricular injection of rapamycin is sufficient to decrease weight gain140. Intraperitoneal injections of rapamycin produce high blood levels of the drug and prevent weight gain when administered every other week. Indeed, a single intraperitoneal administration decreases weight gain for 10 weeks without additional injections140. By contrast, administration of rapamycin by oral gavage did not prevent weight gain132.
Kineret® (Anakinra)
“Treating elderly patients with anti-inflammatory drugs blocking IL-1B function should help with maintaining healthier blood production.” here
“Anakinra is a medication used to treat a range of inflammatory conditions. It is a synthetic version of the naturally occurring interleukin-1 receptor antagonist (IL-1Ra), a protein that helps to regulate the body’s immune response.
Anakinra works by blocking the action of interleukin-1 beta (IL-1β), a cytokine that plays a key role in the body’s immune response and is involved in many inflammatory diseases. By blocking the action of IL-1β, anakinra can reduce inflammation and improve symptoms in conditions such as rheumatoid arthritis, systemic juvenile idiopathic arthritis (SJIA), and cryopyrin-associated periodic syndromes (CAPS).
Anakinra is given as a subcutaneous injection by a healthcare professional or by the patient themselves. The dosage and frequency of injections depend on the specific condition being treated. Common side effects of anakinra include injection site reactions, upper respiratory infections, and headache. More serious side effects may occur, such as an increased risk of infection or allergic reactions, so it is important to talk to a healthcare professional before taking anakinra to determine if it is an appropriate treatment option.
Anakinra is generally well-tolerated, but it is not recommended for use in people with a history of severe allergic reactions to anakinra or other components of the medication. It is also not recommended for use in people with active or chronic infections, such as tuberculosis or hepatitis B. It is important to follow the healthcare professional’s instructions carefully and to report any side effects or concerns promptly.
Anakinra works by blocking the inflammatory signal interleukin-1β (IL-1β), which damages the biological machinery used by the stem cells that develop into blood cells.
“An aging blood system, because it’s a vector for a lot of proteins, cytokines, and cells, has a lot of bad consequences for the organism,” says geneticist and senior author Emmanuelle Passegué, from the Columbia University Irving Medical Center in New York.
Ilaris® (Canakinumab)
“Canakinumab is a monoclonal antibody medication used to treat a range of inflammatory conditions. It works by targeting interleukin-1 beta (IL-1β), a cytokine that plays a key role in the body’s immune response and is involved in many inflammatory diseases.
Canakinumab is primarily used to treat a rare genetic disorder called cryopyrin-associated periodic syndromes (CAPS), which includes three different conditions: familial cold autoinflammatory syndrome (FCAS), Muckle-Wells syndrome (MWS), and neonatal-onset multisystem inflammatory disease (NOMID). These conditions are characterized by recurrent episodes of fever, rash, joint pain, and other symptoms.
Canakinumab is also used to treat a type of arthritis called systemic juvenile idiopathic arthritis (SJIA), which is characterized by joint inflammation, fever, rash, and other symptoms. In addition, it has been investigated as a potential treatment for a range of other inflammatory conditions, including gout, atherosclerosis, and certain types of cancer.
Canakinumab is given as a subcutaneous injection by a healthcare professional. It is usually given once every 8 weeks for CAPS and once every 4 weeks for SJIA. Common side effects of canakinumab include injection site reactions, upper respiratory infections, and headache. More serious side effects may occur, such as an increased risk of infection or allergic reactions, so it is important to talk to a healthcare professional before taking canakinumab to determine if it is an appropriate treatment option.” From ChatGPT
“Rilonacept is a medication used to treat a rare genetic disorder called cryopyrin-associated periodic syndromes (CAPS), which includes three different conditions: familial cold autoinflammatory syndrome (FCAS), Muckle-Wells syndrome (MWS), and neonatal-onset multisystem inflammatory disease (NOMID). These conditions are characterized by recurrent episodes of fever, rash, joint pain, and other symptoms.
Rilonacept is a recombinant fusion protein that works by binding to interleukin-1 beta (IL-1β), a cytokine that plays a key role in the body’s immune response and is involved in many inflammatory diseases. By binding to IL-1β, rilonacept prevents it from activating immune cells and causing inflammation.
Rilonacept is given as a subcutaneous injection by a healthcare professional. The dosage and frequency of injections depend on the specific condition being treated. Common side effects of rilonacept include injection site reactions, upper respiratory infections, and headache. More serious side effects may occur, such as an increased risk of infection or allergic reactions, so it is important to talk to a healthcare professional before taking rilonacept to determine if it is an appropriate treatment option.
Rilonacept is a relatively new medication, and its long-term safety and efficacy are still being studied. It is not known whether it is safe and effective in children under the age of 12 or in pregnant or breastfeeding women. It is important to follow the healthcare professional’s instructions carefully and to report any side effects or concerns promptly.
Cartivix®, Matrix® and Verboril® (Diacerein) (Not Available in US)
“Diacerein is a medication used to treat osteoarthritis, a degenerative joint disease that is characterized by the breakdown of joint cartilage and underlying bone. Diacerein is classified as a slow-acting drug for osteoarthritis (SADOA) and is believed to work by inhibiting the production of certain cytokines, including interleukin-1 beta (IL-1β) and tumor necrosis factor alpha (TNF-α), which are involved in the inflammatory response in osteoarthritis.
Diacerein is a derivative of rhein, which is a natural substance found in the roots and leaves of some plants, including rhubarb. It is available in capsule form for oral administration and is typically taken once a day. Diacerein is usually well-tolerated, but common side effects may include gastrointestinal symptoms such as abdominal pain, diarrhea, and nausea. Rarely, it can cause liver problems, so liver function tests are usually performed before and during treatment.
It is important to note that diacerein is not a painkiller and may take several weeks to months to produce noticeable effects on joint pain and function. It is typically used in combination with other treatments for osteoarthritis, such as nonsteroidal anti-inflammatory drugs (NSAIDs), physical therapy, and lifestyle changes. As with any medication, it is important to talk to a healthcare professional before taking diacerein to determine if it is an appropriate treatment option.” From ChatGPT
More information from ChatGPT that’s revealing:
Interleukin-1 (IL-1) is a pro-inflammatory cytokine that plays a crucial role in the immune response and inflammation. It is involved in many different diseases and conditions, such as rheumatoid arthritis, osteoarthritis, gout, and autoinflammatory syndromes. Therefore, blocking IL-1 signaling can be an effective strategy for treating these conditions.
There are several ways to block IL-1, including:
IL-1 receptor antagonist (IL-1RA): IL-1RA is a naturally occurring protein that competes with IL-1 for binding to the IL-1 receptor. It acts as a potent inhibitor of IL-1 signaling and can block the activity of both IL-1α and IL-1β. The recombinant form of IL-1RA, anakinra, is approved for the treatment of rheumatoid arthritis and other autoinflammatory conditions.
IL-1β monoclonal antibodies: Monoclonal antibodies that specifically target IL-1β can block its activity and reduce inflammation. Canakinumab (Ilaris) and gevokizumab are two such antibodies that have been approved for the treatment of autoinflammatory syndromes.
Soluble IL-1 receptor type 2 (sIL-1R2): sIL-1R2 is a naturally occurring protein that can bind to IL-1 and prevent it from interacting with the IL-1 receptor. It is not as potent as IL-1RA, but it has been shown to have some inhibitory activity against IL-1.
Small molecule inhibitors: Several small molecule inhibitors of IL-1 signaling have been developed, such as an orally available selective inhibitor of the NLRP3 inflammasome MCC950. These inhibitors act at various points in the IL-1 signaling pathway and can block IL-1 activity.
Overall, IL-1RA and IL-1β monoclonal antibodies are the most potent and clinically effective ways to block IL-1. However, the choice of treatment would depend on the specific disease or condition being targeted, as well as the patient’s individual needs and circumstances.
So with that, let’s see if we can find supplements that will increase IL-1Ra (Interleukin-1 receptor antagonist) or help the body generate it – to thereby reduce inflammation and support healthy blood production.
Adiponectin induces the anti-inflammatory cytokines IL-10 and IL-1RA in human leukocytes, per here. So perhaps there is a way to get that. Throwing that into Amazon (here), apigenin comes up. So let’s see what ChatGPT has to say about their relationship:
Apigenin and adiponectin are two biologically active compounds that have been studied for their potential health benefits.
Apigenin is a type of flavonoid that is found in a variety of plant-based foods, including fruits, vegetables, and herbs. It has been shown to have anti-inflammatory, antioxidant, and anti-cancer properties.
Adiponectin is a hormone produced by fat cells (adipocytes) that is involved in regulating glucose metabolism and fatty acid oxidation. Adiponectin levels in the blood are inversely related to body fat levels and have been shown to be decreased in obesity and type 2 diabetes.
Studies have suggested that apigenin may have an impact on adiponectin levels in the body. In animal studies, apigenin has been shown to increase adiponectin levels and improve glucose metabolism. However, more research is needed to confirm these findings in humans and to understand the mechanisms by which apigenin may affect adiponectin.
It’s important to note that while apigenin and adiponectin have been shown to have potential health benefits, they should not be used as a substitute for medical treatment. If you have any concerns about your health or nutrition, you should speak with a doctor.
And then to vet if it is pro- or anti- coagulant, ChatGPT was used, and answer marked in the cross-check list here.
Apigenin is a naturally occurring flavonoid that is found in a variety of plant-based foods and has been suggested to have anti-inflammatory and anti-cancer properties. There is limited research on the effects of apigenin supplementation on blood clotting.
In general, blood clotting is a complex process that is regulated by many factors, including the balance between pro-clotting and anti-clotting factors. While some studies have suggested that apigenin may have an anti-clotting effect, other studies have shown no significant effect on blood clotting.
More research is needed to fully understand the effects of apigenin on blood clotting and to determine safe and effective doses for supplementation.
Interestingly, you can buy IL-1Ra here for research purposes. It is very likely the active component of Kineret/Anakinra.
Daily intake of fish or omega-3 increased adiponectin by a whopping 14-60%. Here. And other supplements like the ones here all seem to increase adiponectin. Which fits. Including Chamomile tea, which is a potent source of apigenin per here.
Now CBD has also shown positive results in this condition, so let’s ask ChatGPT about it:
There is limited research on the relationship between CBD and adiponectin, but some studies have suggested that CBD may have an impact on adiponectin levels. In animal studies, CBD has been shown to increase adiponectin levels and improve glucose metabolism. However, more research is needed to confirm these findings in humans and to understand the mechanisms by which CBD may affect adiponectin.
Interestingly, in normal/healthy adults, the #1 source of IL-1Ra is e-coli, and Kineret/Anakrina is produced by e-coli (see here WRT their note about e-Coli allergy “Proteins made from bacteria called E. coli. Ask your healthcare provider if you are not sure”), and in ME/CFS patients e-Coli in the gut is severely low (see here). So this all fits.
Additionally, there are other IL-1B blockers, per here:
Interleukin (IL) 1 is a highly potent proinflammatory mediator that is important in immune defense and in immune-mediated disease.
Three pharmacologic inhibitors (sometimes termed blockers) of IL-1 are commercially available:
And blocking IL-1Beta reverses immunosuppression in mouse models, here.
C. Treating the Excess Micro Coagulation:
Prescription/Drugs:
The following are now commonly-used treatments for long-COVID, with some notes sprinkled in form my own research as to effectiveness and experience.
One of the following approaches:
Heparin (taken as Lovenox)
Low Molecular Weight Heparin (LMWH) is Lovenox. See the sentence from there:
“If insurance will pay for LMWH (Lovenox), use 30 mg. in AM”. That’s for slender patients like me. From here. And it is recommended to be taken sublingually, here.
Sublingual is preferred, as injections may trigger the over-active (IL-1Beta) inflammation mechanism, somewhat nullifying the impact of the anticoagulant. (And I’ve confirmed this on myself – I bloat up and turn red immediately after the shot, ears, neck, face, feet, and stomach.)
Sublingual is however not common and untested effectiveness, e.g. here. “Nevertheless, it is noteworthy that, although promising, the sublingual route of heparin administration has not been extensively investigated for LMWH.” Dr. Berg however highly recommends sublingual, here.
“Apixaban is an oral anticoagulant medication that works by selectively inhibiting Factor Xa, which is a key component in the coagulation cascade. Specifically, apixaban binds to both the free and the clot-bound Factor Xa, inhibiting its ability to activate thrombin, which is the enzyme that promotes the conversion of fibrinogen to fibrin, leading to blood clot formation. By inhibiting Factor Xa, apixaban reduces the risk of blood clots in conditions such as deep vein thrombosis (DVT), pulmonary embolism (PE), and stroke in patients with atrial fibrillation.” from ChatGPT
Clopidogrel (Plavix) 75mg once a day,
“Clopidogrel is an oral antiplatelet medication that works by selectively inhibiting the adenosine diphosphate (ADP) receptor on platelets, which inhibits platelet activation and aggregation. Clopidogrel does not directly act on clotting factors but rather affects platelet function and prevents the formation of blood clots in arteries. Platelets are small, disk-shaped blood cells that play an important role in the formation of blood clots. When an injury occurs, platelets are activated and begin to stick together, forming a plug that stops the bleeding. However, in some cases, platelets can become overactive and form clots inside blood vessels, which can cause serious health problems such as heart attacks and strokes. Clopidogrel inhibits the activation of platelets by blocking the ADP receptor, which is necessary for platelet activation and aggregation. By reducing platelet activation and aggregation, clopidogrel reduces the risk of blood clots in conditions such as acute coronary syndrome, myocardial infarction, and stroke.” from ChatGPT.
Baby Aspirin 75mg once a day, with fish oil and/or SPMs
“Aspirin, including baby aspirin (low-dose aspirin), is a nonsteroidal anti-inflammatory drug (NSAID) that works by blocking the activity of an enzyme called cyclooxygenase (COX). This enzyme is involved in the production of prostaglandins, which are molecules that cause inflammation, pain, and fever. Mast cells are a type of immune cell that play a role in the body’s response to allergens and other irritants. When mast cells are activated, they release a variety of chemicals, including histamine, which can cause inflammation, itching, and other allergic symptoms. There is some evidence to suggest that aspirin may have an impact on mast cells. In particular, aspirin has been shown to inhibit the release of histamine from mast cells in vitro (in a laboratory setting). This effect may be due to aspirin’s ability to block the activity of COX, which is involved in the production of a type of prostaglandin (PGD2) that stimulates mast cell activation and histamine release.” ChatGPT.
Baby aspirin has multi-fold benefits, as in addition to being an anticoagulant, it helps in the promotion of Resolvins, and long-lasting resolvens from here (payed service)
Aspirin is a COX1 inhibitor at lower levels, and at higher levels, it also changes the enzyme function of COX-2 via acetylation.[ref]
Aspirin is unique among NSAIDs in that it acetylates COX2, which then triggers the formation of ‘aspirin-triggered specialized pro-resolving mediators‘ or AT-SPMs. These aspirin-triggered SPMs include AT-lipoxin A4, AT-resolvin D1, and AT-resolvin D3.[ref][ref]
Aspirin-triggered SPMs are unique in that they have a prolonged half-life and act to resolve inflammation for longer.[ref] It is likely why only aspirin, and not other NSAIDs, helps to prevent heart disease and reduces the risk of colon cancer (for some people).
Atorvastatin here to reduce LDL-C which is often too high for fibrinolysis to take hold, as lipid metabolism is disturbed in ME/CFS (see here). (Bromelain also helps, see below.)
Rivaroxaban is an anti-clotting drug being investigated as a possible treatment for Long COVID patients with microclots.[1], here
Looks very effective, but likely not available until 2024, per here
Need to see if there are other sources for it.
Supplements:
Piracetam
Dr. Teitelbaum recommends Piracetam- 1200mg twice a day for 2 weeks, then 2400mg twice a day for 2 weeks, then adjust to optimum dose (up to 4800mg a day). He recommends that it be taken with Hydergine.
In healthy volunteers, piracetam mediated a direct stimulant effect on prostacycline synthesis and reduced the plasma levels of fibrinogen and von Willebrand’s factors (VIII: C; VIII R: AG; VIII R: vW) by 30 to 40%, from here, and more details in this doc, here.
If you get a headache from it, you need more Choline, per here.
8 g piracetam daily in 3 divided doses at 8-hourly intervals, here.
Extremely effective for reducing brain-fog and feeling yourself again, more on why here.
Serrapetase
20,000 SPU to 120,000 SPU total daily dose, with smaller doses at more frequent intervals preferred (i.e., 40,000 SPU three times daily on empty stomach). Enteric coating may improve efficacy. Anecdotally, some are taking much higher doses, but this hasn’t been studied. Here.
240,000 SPU’s x 4/day
Nattokinase
Start at a subtherapeutic dose to assess tolerability (i.e. 2,000 FU once daily on empty stomach). Some may experience a Herxheimer reaction so it’s best to start slowly.
Titrate up dose as tolerated to appropriate dose based on medical history & other medications.
Anti-fibrin and platelet effects per here: “reducing intravascular fibrin and platelet deposition, which in turn reduces downstream microvascular thrombosis and improves cerebral vascular patency.”
“Rutin proved to be the most potently anti-thrombotic compound that we ever tested in this model,” says Flaumenhaft. Of particular note, rutin was shown to inhibit both platelet accumulation and fibrin generation during thrombus formation.”
“In peripheral artery disease, a 4.4g supplement of DHA/EPA for 3 months increased resolvin E3.” source here and see SPMs below for additional benefits
Hesperidin, helps with blood vessel conditions here
“Probiotics. Certain probiotic bacteria, especially the Lactobacillus reuteri NCIMB 30242 strain, have been found to improve markers of thrombosis risk.” here
Hydrogenated water, here, and see how it helps on cerebral ischemia, here, and here
“Inhaled hydrogen gas (H2) has been shown to have significant protective effects on ischemic organs. Clinical trials abroad have shown promise that treatment of patients suffering from stroke, cardiac arrest, or heart attacks may benefit from inhaling hydrogen gas during the early recovery period.” here
Great article on what helps to prevent blood clots, here.
D. Treating Suppressed Immune System: (ones in bold are under consideration)
When the clots and MCAS are treated, blood flow to the gut will improve and the immune system will start to improve on its own (note that a big portion of our immune system comes from our gut, here). Sleep will also improve, which will help the immune system as well. For example, treating the clots and MCAS alone, my oral thrush completely went away.
But nonetheless the immune system will need help along the way, in the form of direct support and correcting gut dysbiosis.
Immune Support
IV IG (here) (I had this and it temporarily helped me)
Shown to reduce T-cell over-activity.
Hyperbaric chambers (also helps with reperfusion injury from the system low oxygenation).
Correcting Gut Dysbiosis
As the condition worsens, the body becomes progressively more intolerant to foods containing histamine and any foods that naturally cause a healthy body to inflame (carbs, sugars, etc.). Details on the biomarkers for histamine intolerance are here. And an excellent view on the difference between the flora of sufferers of this disease and healthy controls is here (tbiomedcentral).
Unfortunately, many (author included) unknowingly make their condition worse by taking standard probiotics which are otherwise helpful for those in good health.
The `why` of this is multifold:
Many probiotics either directly or indirectly produce histamine in the gut and or contribute to SIBO/SIFO (small intestinal overgrowth of bacteria and/or fungus).
Many ME/CFS patients suffer from SIBO (Small Intestine Bacterial Overgrowth) and Candida overgrowth of the small intestine
And many probiotics simply make these conditions worse.
And often the typical advice for improving gut health (adding fiber) will make the SIBO worse – which further triggers both clotting and MCAS
Antibiotics, often prescribed to treat gut dysbiosis, are a trigger for inflammation and coagulation (e.g. here).
But interestingly, some are actually anti-coagulants, so ME/CFS symptoms can sometimes improve temporarily on antibiotics, depending on which are used and the nature of the antibiotic, only to get much worse after the course of antibiotics is done.
H2 blockers, while reducing histamine inflammation and having the potential to help, often can CAUSE SIBO because they reduce stomach acid, which is one of the ways the body prevents bacteria from over-growing the small intestine.
So then the end goal if you are on H2-blockers is to figure out how to get off of them without a relapse.
Spore-based probiotics, Transfer factor, Lactoferrin, and/or ImmunoSEB (more below) and natural anti-inflammatories (above) may be helpful here.
Lack of understanding on what is inflammatory or anti-inflammatory based on your genetics and the status of your current intestinal flora. These can be understood, and interpreted with the following two resources.
Genetic Lifehacks, here – for knowing your genetic propensity for inflammation and recommendations for how to reduce it.
Inflammation is the #1 cause of gut dysbiosis, so this information is extremely helpful.
Microbiome Prescription, here – for knowing the current state of your gut biome (intestinal flora), and recommendations based on literature review on what probiotics to take to rebalance it.
For example, this author’s worst-offender bacteria is here. Below is an example, where the author has at least 50-fold the presence of this harmful bacteria compared to a healthy individual:
“Corynebacterium, 51x normal. A genus of bacteria characteristically cells are rods with filaments attached and produce filamentous microcolonies; facultative anaerobes; carbohydrates are fermented. The genus has only one type species i.e. Corynebacterium matruchotii. Causative agent of diptheria which affects the nasopharyngeal passageways and in suseptible individuals can produce a toxin which inhibits protein synthesis in the host.
Note that as usual, the whole picture needs to be looked at when following your genetics and the state of your current intestinal flora. For example, cross-checking what Microbiome Prescription recommends against the recommendations (and contra-indications) from Genetic Lifehacks is recommended – as well as cross-checking against the 5 core pillars of treatment, as done for this author’s recovery, here.
Note that many “How I treated SIBO” articles online actively made my condition worse, as they included materials which induce an inflammatory response.
Such treatments, in others, is fine – and that’s why these treatments are so successful for patients who are not genetically prone to this disorder – but often materially make Long-COVID and ME/CFS sufferers worse.
It was only after taking the whole picture into account (e.g. not using any SIBO-killing techniques that CAUSE inflammation) did treating SIBO start to work and improve my condition.
With all that said, below are probiotics and supplements that seem to be well-tolerated and in fact help fight SIBO/SIFO in patients with ME/CFS and Long-COVID, which have been used without knowing (a) your genetics or (b) your current gut biome state. (Knowing your genetics and current biome state will accelerate the recovery and reduce the risk of making yourself worse with treatment.)
Probiotics
Spore-based Probiotics
Helps clear small intestine of pathogens
Spurs growth of useful bacteria.
Combining many different forms of the same spore bacteria appears to be beneficial, and from recovered ME/CFS patients, this has proven anecdotally helpful (.e.g reviewing the regime of MoreThereThanHere, here, which combines many different strains of coagulans, subtilis, and clausii) and a clinical trial linked herein, direct link here, where 4 different strains of Bacillus clausii were used.
The major strains that have been found to help are:
Bacillus coagulans
Bacillus subtilis
Promotes fibrinolysis and reduces clotting per NIH and via the DFE produced by subtilis shown in BioMed
“Soil-based probiotics benefits have been investigated in the treatment of small intestinal bacterial overgrowth (SIBO) in patients with IBS. In particular, one probiotic containing all four strains of Bacillus clausii was shown to help control SIBO in a small study with 60 people.” here
Examples products that include these strains, and many who have recovered from ME/CFS or Long-COVID have used these with success, e.g. here and here:
Deep Immune probiotic has viruses (bacteriophages) that infect bad bacteria, more info here.
Bacteriophages
LH01 – Myoviridae
LL5 – Siphoviridae
T4D – Myoviridae
LL12 – Myoviridae
Spore Probiotics:
DE111 Bacillus subtilis
Bacillus coagulans
Lactobacillus acidophilus
Bifidobacterium lactis
Maltodextrin
ProbioSEB CSC3
Bacillus coagulans LBSC (DSM 17654)
Bacillus subtilis PLSSC (ATCC SD 7280)
Bacillus clausii 088AE (MCC 0538)
Designs for Health ProbioSpore (one of MoreThereThanHere’s probiotics)
Bacillus coagulans (Lactospore)
Bacillus subtilis (DE11)
Bacillus coagulans (SNZ1969)
Bacillus coagulans (Lacris-15)
Bacillus clausii (CSI-08)
OrthoSpore IG:
Immonulin 1g
IgG 480mg
Bacillus coagulans (SNZ1969)
Bacillus subtilis (HS43)
Bacillus clausii (B106)
SOLARAY Bacillus Coagulans Probiotic (ordered here, from here)
Swanson Lactobacillus Rhamnosus (ordered here, from here)
Lactobacillus Rhamnosus (unspecified strain)
Particular interest in Lactobacillus rhamnosus GG (LGG) here
Reuteri
NCIMB 30242 strain, have been found to improve markers of thrombosis risk.” here
“In this study, 56% of the children taking PPI’s developed SIBO, while only 6% of those taking PPI’s along with this particular strain of Lactobacillus reuteri developed SIBO.” per here
BioGaia Protectis Immune Active Probiotic (ordered here)
Lactobacillus reuteri DSM17938
Warning this product has additives that may nullify or make a net-negative depending on the severity of your symptoms.
So you may need to do other reuteri strains first, improve, then can use this.
More research and extensive notes on each of these (and other supplements) is in the supplement cross-check document here
Make sure to read the comments, as they contain additional information on the supplement.
For example of why cross-check is needed, take for example if you are using Heparin (Lovenox, Low Molecular Weight Heparin, enoxaparin sodium) as a blood thinner/anti-coagulant. If that’s the case, do not take Lactobacillus Rhamnosus and many other Lactobacillus probiotics as they nullify the anticoagulant effect of Heparin (Lovenox), per NIH, and discovered via here.
Heparin was degraded by:
Enterococcus faecalis,
Lactobacillus animalis,
Lactobacillus casei,
Lactobacillus casei subsp. casei,
Lactobacillus casei subsp. rhamnosus,
Lactobacillus pantheris,
Lactobacillus paracasei subsp. paracasei and
Lactobacillus rhamnosus.
Heparin was not functionally degraded by:
Lactobacillus acidophilus
Lactobacillus aviarius subsp. Aviarius
Lactobacillus brevis
Lactobacillus parabuchneri
Lactobacillus paracasei subsp. Torelans
Lactobacillus reuteri
Lactobacillus saerimneri
Bifidobacterium bifidum.
This yogurt is highly recommended (by the probiotic advisor, here) for constipation-dominant IBS.
Helps reduce immune system inflammatory response to infections (NIH)
Zinc-L-Carnosine and Carnosine
Zinc promotes gut health and overall healing, and tighter intestinal barrier.
Anti-glycationand prevents build of AGEs (Advanced Glycation End products)
“Carnosine has been shown to prevent AGE formations through reduction of blood glucose, prevention of early glycation, and even reversing previously formed AGEs.” (NIH)
“We found that carnosine supplementation in 3xTg-AD mice promotes a strong reduction in the hippocampal intraneuronal accumulation of Aβ and completely rescues AD and aging-related mitochondrial dysfunctions.” (NIH)
“That’s removal of brain amyloid beta plaques tied to dementia!” here
Prevents/reverses age-related brain mitochondrial oxidation per NIH
Carnosine is a dipeptide of β-alanine and L-histidine.
The body consumes histidine to make histamine (and make a histamine storm), and it is the author’s guess that muscles (including gut muscles, brain, nerves, etc. end up low in histidine as a result
And histidine is used in growth, repair of damaged tissues, and making blood cells. It helps protect nerve cells. per Rochester
So it is the author’s view/guess that supplementing with Carnosine should help restore histidine in the body (and in the gut), which fits with many NIH findings, as above.
ImmunoSEB (also helps digest blood clots)
Serratiopeptidase,
Bromelain,
Amylase,
Lysozyme,
Peptidase,
Catalase,
Papain,
Glucoamylase
Lactoferrin
Note that depending on your sensitivity to Lactose, you may need to delay taking this until you have recovered enough to handle Lactose
Broccoli extract
Histamine release is controlled via cAMP, which regulates pro- and anti-inflammatory activities: drugs that elevate intracellular cAMP levels reduce the production of pro-inflammatory mediators and increase the production of anti-inflammatory factors in numerous immune cells. NIH
And broccoli and other cruciferous vegetables have been shown to increase levels of cyclic AMP (cAMP) in the body. This is due to the presence of compounds known as glucosinolates, which are abundant in cruciferous vegetables like broccoli, cauliflower, and kale.
So by increasing cAMP, Broccoli is potently anti-inflammatory.
Cauliflower extract
Artichoke extract
Triphala
Staple in traditional Ayurvedic medicine for 1,000+ years to support immune system
Anti-inflammatory, and does not seem to excite T-cells, per ChatGPT:
Triphala is a combination of three fruits – Amla (Emblica officinalis), Haritaki (Terminalia chebula), and Bibhitaki (Terminalia belerica) – that has been used in Ayurvedic medicine for thousands of years. It has been studied for its potential benefits for digestive health, immune function, and other physiological processes.
While there is limited research on the specific effects of triphala on T-cells, some studies suggest that it may have immune-modulating effects. Triphala has been shown to have potential benefits for reducing inflammation and oxidative stress in the body, which can help to support immune function. It may also have potential benefits for promoting the growth of beneficial gut bacteria, which can help to improve overall health and immune function.
In addition, some studies have suggested that individual components of triphala, such as Amla, Haritaki, and Bibhitaki, may have potential immune-modulating effects. For example, Amla has been shown to have potential anti-inflammatory and antioxidant effects, while Haritaki has been studied for its potential benefits for immune function and anti-inflammatory effects.
Overall, while more research is needed to fully understand the potential impact of triphala on T-cells and immune function, some studies suggest that it may have immune-modulating and anti-inflammatory effects. However, it is important to discuss the use of triphala with a healthcare provider, particularly if you have a history of medical conditions or are taking medications.
Berberine, per ChatGPT, here
Berberine is a natural compound that is extracted from various plants, including the Berberis shrub and goldenseal. It has been used in traditional medicine for thousands of years, and recent research has shown that it has a number of potential health benefits.
Some of the ways in which berberine may impact the body include:
Regulating blood sugar: Berberine has been shown to help lower blood sugar levels by increasing insulin sensitivity and reducing glucose production in the liver. This makes it a potential treatment for conditions such as type 2 diabetes.
Lowering cholesterol: Berberine may also help to lower cholesterol levels by reducing the production of cholesterol in the liver and increasing the excretion of cholesterol in the bile.
Supporting gut health: Berberine has been shown to have antimicrobial properties, which may help to kill harmful bacteria and other pathogens in the gut. It may also help to reduce inflammation in the gut and improve gut barrier function.
Anti-inflammatory effects: Berberine has been shown to have anti-inflammatory effects, which may make it a potential treatment for conditions such as rheumatoid arthritis and inflammatory bowel disease.
Supporting cardiovascular health: Berberine may help to improve cardiovascular health by reducing inflammation, improving cholesterol levels, and reducing the risk of blood clots.
Overall, berberine appears to have a wide range of potential health benefits.
3 capsules twice a day empty stomach for 6 months 4.
Toxaprevent 1 sachet 1 hour before lunch for 2 months
Acetyl-L-Carnitine (here) to help body product Acetylcholine for proper nerve function (here: https://bioelecmed.biomedcentral.com/counter/pdf/10.1186/s42234-023-00104-7.pdf?pdf=button%20sticky)
Results in bowel movement ~1.5 hours after taking
Take first thing in morning
Note that if your condition is severe, you may need to wait to progress before you can take this, as your intestinal muscles may have too much inflammation and too many clots, resulting in pain/damage when using this. So the inflammation and clotting may need to be treated before starting this.
Things to avoid (if senescent T-cell problem, as is my case, not viral reactivation issue):
AHCC
Increases T-cell activity by stimulating IL-1B, per NIH
Used in Japan for treatment of over 600 diseases, per here, and here, and improves parasympathetic tone per here. Eliminated persistent HPV, here at 3g/day. Full guide on it here.
And it is recommended for ME/CFS, MCAS, and COVID post-sequelae, here, but not understood as to why it’s effective.
Helps body deal with physical/disease stress in more productive way.
From ChatGPT, it is also good at suppressing one of the root problems of the disorder, the very potent, and very over-active Inflammatory Interleukin Cytokine IL-1Beta:
“AHCC (Active Hexose Correlated Compound) is a natural extract derived from the mycelium of shiitake mushrooms, which has been suggested to have immunomodulatory effects.
IL-1B is a pro-inflammatory cytokine that plays a role in the body’s immune response, particularly in the regulation of inflammation. Elevated levels of IL-1B are associated with several inflammatory diseases.
Several studies have investigated the potential impact of AHCC on IL-1B levels. One study published in the Journal of Experimental Therapeutics and Oncology in 2011 found that AHCC decreased the production of IL-1B in human immune cells called macrophages, which are known to produce high levels of this cytokine in response to inflammatory stimuli.
Another study published in the Journal of Nutrition and Cancer in 2018 examined the effect of AHCC on colon inflammation in mice. The study found that AHCC supplementation decreased the expression of several inflammatory cytokines, including IL-1B.
And fortunately, according to ChatGPT, it does not seem to cause clotting, and in fact in-vitro it helps to prevent blood clots and particularly useful is improving the lipid profiles, which are found to be off in ME/CFS patients (TO-DO, find the NIH that shows this).
One study published in the Journal of Experimental Therapeutics and Oncology in 2011 found that AHCC reduced platelet aggregation in vitro, which is a key step in the formation of blood clots. However, it is important to note that this was an in vitro study, which means that the effect was observed in a laboratory setting and may not necessarily translate to the human body.
There is currently no direct evidence that AHCC can prevent or treat blood clots in humans. However, some studies have suggested that AHCC may have cardiovascular benefits, such as reducing blood pressure and improving lipid profiles, which may indirectly affect the risk of blood clots.
And from NIH, here, the research agrees that AHCC helps to make T-cells more effective. Which in concert with reduced inflammation, should help the immune system eliminate pathogens more effectively, thereby having a net result of decreased inflammation.
E. Healing the Vasculature:
Will occur naturally and slowly over time as the Endothelium heals once the inflammation (histamine and cytokine storm) episodes stop. But it is best to start treating it in parallel in ways that improve the quality of the vasculature overall, as this can also help reduce platelet aggregation and feedback to preventing histamine and cytokine storms.
The key to healing Endothelial is increasing nitric oxide in the blood (e.g NIH)
Reduces oxidative stress on endothelium and promotes NO synthase in vitro and in vivo, NIH
Also increases mitochondrial function and mitophagy (kill off of old/broken mitochondria) because of the Urolithin A (UA) produced by gut microflora from foods rich in ellagitannins (e.g. walnuts and pomegranate), per Cell here and here, and found/quoted from here.
Pomegranate itself is considered not SIBO/SIFO-safe (per this guide) but the extract is considered SIBO and SIFO, per NIH.
GrapeSeed Extract
L-Arginine
Rutinoside (CARDIOART)
Swanson Endopro Endothelial Support Formula 500 Milligrams,here
Vitamin E
Vitamin C
Aspirin
Aspirin was found to acetylate lysine of eNOS, which evokes activation of its enzymatic activity, i.e. NO synthesis, release and bioavailability of NO not only in endothelial cells, but also in platelets. Per NIH
Beetroot juice (if you can handle the sugar content)
Dark Chocolate (if you can handle the sugar content)
Niacin to flush out capillaries (not niacinamide) 2x per day at 400mg each
This is the LAST STEP and to be used prophylactically when nearly 100% recovered.
Start slow and only after materially improved.
Advice on (Self) Treatment
The hard part about treating all of these is that some things used to treat one of the issues will actually trigger even more severe coagulation (e.g. Stinging Nettles which have high Vitamin K, which strongly contributes to the body’s clotting, here).
Given this, whenever adding a food, supplement or drug, check for the following:
Does it trigger coagulation?
Does it trigger MCAS?
Do a Google search at least and if possible seek expert consultation. And prioritize based on coagulation being the most important to not trigger, followed by MCAS. As the suppressed immune system, poor blood quality, and capillary performance will all naturally improve by treating the excess fibrin coagulation (most important) and the inflammation/MCAS.
So it is paramount to prioritize not triggering the coagulation first and foremost, and inflammation secondarily.
And in terms of adding in foods/supplements/drugs – try to do so slowly and observe the impact. Taking 1-3 days per addition (or removal) to observe how your body responds.
Overall, it’s VERY easy to make things worse. And even more difficult to make things better. So check, and double-check what negative impacts a food, supplement, or drug may have before initiating.
To help with that, here is a WIP sheet that cross-checks supplements/drugs against the main issues with this condition.
And additionally, you need to make sure any supplement you add does not interfere with any medication you are taking, and a great resource for that is https://supp.ai/.
And if you need a consult on if something is a good idea or not, ask ChatGPT, here. It can give answers in 15 seconds that would take me weeks of research to find.
And overall, the supplement that is likely the best to start first is Piracetam, as it shows the strongest response to reducing and/or eliminating brainfog. And eliminating brainfog will allow making better decisions – which will likely improve your recovery.
Associated Unsolved Diseases
Very likely this is the cause or major contributor to:
Note the most/all schizophrenics are addicted to smoking (e.g. here), which is nicotine, and helps to calm them via vagus nerve stimulation, see here.
A better/safer prescription (as nicotine is an “inflammation trap”, see here) is Acetyl-L-Carnitine to help those afflicted to replenish lacking acetylcholine (per here).
Bipolar Disorder (when the clots/inflammation comes in waves – clears and clots)
Autism Spectrum (when the microclotting is triggered at a young age)
Dyslexia (40% of entrepreneurs were found to show signs of dyslexia, here)
And dyslexia is one of the most easily measurable disorders.
Synesthesia (I’ve had this my whole life)
Again, the organs impacted first seem to depend on the capillary nature of each individual, i.e. the physical structure of the capillary per organ/etc. For example in Fibromyalgia, the skeletal muscles seem to be the hardest impacted.
But in many very often the brain and vagus nerve are among the first-impacted organs. With “floating anxiety” being an early mental symptom. And this floating anxiety diverges in people, depending on how bad it is. In some (like me), it makes them want (correction, need) to be the best in the world at something.
So in other words, the genetic propensity for this disease is a blessing and a course. Some of the most driven people in the world are disproportionately more likely to get the disorder, or mysteriously die (without the world knowing that it’s this disorder that killed them). Examples include one of the world’s top surfers, here, more here. Top athletes like here. And Forbes 30 under 30, here. Bruce Willis, here. And even my old boss, Robert Pera, who was the youngest billionaires in the world at one point, developed POTS after mono in high school (covered here as a heart condition, relayed to me personally, here).
I’m an entrepreneur, and always wanted to be the best in the world, or one of the top CEOs in the world. My good friend, who now has chronic Lyme, is one of the best entrepreneurs I know. And interestingly, even Justin Bieber developed chronic Lyme after the pandemic, here.
Robin Williams was driven to be the funniest man alive, and died of suicide from the pain/torture in his head (which many with ME/CFS can relate to), here. And this fits with as we age, the capability to fight (brain) inflammation subsides. And this results in a tipping from extreme drive (productive) to mental disorders which are self-harm inducing (counter-productive). You can see this happening live to Jim Carrey, as many have observed, here. Jonah Hill taking a break from promoting films post-COVID, here. And now even professional hockey players, here
And just like Dyslexics make up some 40%+ of entrepreneurs (here), they also make up a severely disproportionate proportion of the inmate population (e.g. here). And this reflects the “tipping point” hypothesis.
Excess Mortality After COVID-19 Pandemic (WIP)
Unexplained excess mortality from the following is being observed across the US:
Disc atrophy (visible in MRI, confirmed in the author, and all his relatives)
Buzzing feeling in chest
Chest tightness
My Personal Story (WIP)
Why am I Sharing This?:
I’ve dedicated my life to trying to have a material impact on the world in a positive way, primarily using engineering as the mechanism.
In getting the very severe version of Long-COVID, I have found my life’s work, which I consider a blessing on me and my family.
I’m the founder of Luxonis, which enables this sort of stuff, among many life-saving applications. And the former lead of UniFi. Here’s me back in the good days. I’ve lead (and continue to lead) a blessed life. My goal is, and always has been, to give more than I take. Which is the core of the reason for using my (little) energy to write up this Reddit post and the documentation below.
And despite the severity of this illness, and the probability of this disease permanently disabling (or, less likely, killing) me, I still consider myself to be living a blessed life – as my children were also afflicted and the research and treatment below recovered them – which is all I needed/wanted. And that is why…
I consider this this my life’s work.
My Long-COVID story:
I’ve been on a downward spiral now for quite a long time (since June 2021). And ended up unable to walk and at one point, control (or feel) my right leg and both arms below the shoulder. I looked nearly identical to, and had the same state of existence as this guy, with the TPN feeding port to my heart (still in me, here) and all and being given liquids via IV because I couldn’t even drink water. Hospitalized, foley-cathetered, no bowel movements for 20+ days.
I left the hospital for 2 reasons:
To spend some last good days with my wife (in case my research was wrong). I ate a cheeseburger from In-And-Out Burger (and nearly died), rode in a Tesla (here), sat on the roof to enjoy sunsets (here). And generally just did a last-hoorah.
To enable myself to self-treat (which I started immediately upon leaving). The doctors were not allowed (by law) to prescribe what I needed (as it was off-label), and by the nature/constraints of TPN osmolality were feeding me with nearly 80% sugar through TPN (Total Parenteral Nutrition, here), which according to my research (and the impact I saw/felt my body) is HORRIBLE for this condition.
Upon leaving the hospital, I initiated self-treatment and started to recover. I can walk again. Make jokes, and write all this up. Every once a while I even dance a little. And most importantly I can eat at or above my calories each day. And I went from almost no deep sleep at all (monitored by Apple Watch 8) to 1 hour and 42 minutes as of last night.
And with this self-treatment, my mental clarity continues to improve, and my research continues. The in-progress results of my research are below. I still have no idea what the future holds though… as there still could be (very likely are) holes in my research that are actively hurting me or preventing me from recovering as a fast as I could.
TLDR of Research:
It’s a result of a genetic propensity for inflammation, fibrin micro emboli, and poor blood production that’s triggered by COVID (and other spike-protein viruses), other environmental factors, and stress that results in inflammation and tons of tiny blood clots which together reduce microcirculation and oxygen perfusion body-wide which then results in rampant infections, further feeding the disorder, and if severe, and often ends up with full-blown MCAS and POTS.
Treatment requires treating multiple things in parallel in a monitored and carefully-measured manner.
Full Amalgamation of Research:
In this doc are a bagillion NIH references, along with summaries from doctors and practitioners in treating this disorder. Largely Dr. Berg from the ’90s, Dr. Tietelbaum (who didn’t fully get it) and other researchers in Germany, South Africa, and now a startup in California (RTHM).
My daily food and supplementation schedulehere, which brought me back from being this guy (I still have the TPN port in)
My cross-check listhere, to make sure a supplement that makes one thing better (e.g. MCAS) doesn’t make another thing worse (e.g. poor blood quality), and supplements I’m still checking are here.
My food and experience loghere. Most of my meals are/were in Cronometer (highly recommend) but there’s no way to make it public (see here). So I moved to the food/supplementation schedule above.
To give you a visual, here I am June 5th, 2021, coming back from doing a run and HIIT, just 7 days prior to the trauma to my gut that kicked off this long and terribly-confusing downward spiral and ~1.5 years after my COVID-19 infection.
(The award is for Luxonis, from the Embedded Vision Alliance.)
Progression of Symptoms and Treatment to Date
My family seems to have a very strong genetic propensity for ME/CFS. For literally every one of us, we got severely ill after getting mono.
Most in my family (and I’m talking dozens) never recovered and have to be taken care of by their parents.
And many went on to develop mental illnesses.
my brother – Paranoid Schizophrenia,
my cousins, bipolar disorder,
and many tried to commit suicide multiple times (over 20).
I was sick after getting diagnosed with Mono in October 2008 through mid 2011.
During this time, I went from being sharp, driven, and first in my class, to having crazy brainfog and severely low energy and drive.
Towards late 2010, I started developing what I considered to be pre-Schizophrenia.
And this followed the exact trend as my brother:
Sharp, mono, 2-3 years of dumb, then starting to go crazy (and would tell you that – which is pre-Schizophrenia), and then went full-blown Schizophrienic around 3-4 years after mono.
I started researching on how to prevent pre-schizophrenia from developing into full schizophrenia, and around late 2010 I found a German study that showed that high-dose fish oil (6 grams of Omega 3s) would make pre-schizophrenics go back to normal function, and placebo’ed participants developed full schizophrenia. It was double-blind with 80 participants split 40/40. And all 40 with fish oil went back to normal.
I started taking high dose fish oil immediately, and after 6 months my life completely changed. So by mid 2011:
I was high energy.
I had joined many soccer teams.
And I met my lovely wife about a year after that.
And my boss told me “I don’t know what happened, but I swear over the last 6 months you’ve gotten smarter every day”
I then eventually went on to lead UniFi (2015) and then start my own company (Luxonis) in 2017
I wouldn’t realize (or even learn the term ME/CFS) until late 2022, I had just accepted that lower quality of life as “normal” and was amazed at how much energy everyone had… and how little sleep they needed (I needed 11+ hours through those ~3 years).
COVID-19 January 11th 2020 while in Taipei meeting engineer from Wuhan
Recovered, no lingering symptoms
Moderna Vaccine as soon as I could get it
First dose MODERNA COVID-19 VACCINE April 8th, 2021
Lot 019B21A
Qty: 0.5mL
NDC: 80777-0273-99
Loc: 620-045
Second dose MODERNA COVID-19 VACCINE May 6th, 2021
Lot: 023C21A
Qty: 0.5mL
NDC: 80777-0273-99
Loc: 620-045
May 6th after vaccine and following weeks very tired and under the weather for 1+ week after each vaccine.
Noticed a variety of symptoms that lingered after the second dose:
That I peed all the time after the second vaccine dose and had to drink tons of water.
It was harder to start peeing (would wait a while)
And would “flush” with any amount of stress. (My whole body would get hot, especially my face.)
Coworkers noticed me taking my jacket off all the time during any time of stress (e.g. a customer asking a tough question) and then putting it back on right after.
Noticed more sensitivity to heat and cold, needed narrow range
Had to pee super badly on road trip on June 12th 2021
Had kids with us and it was hard to stop (mountains, winding roads). And at this point I’m having to pee every ~45 minutes, and chug water to stay hydrated.
By the time we did stop, I had an EVEN HARDER time initiating the stream
After I did pee, I had severe pain in lower right quadrant, which turned out to be small intestine leading to ileocecal valve (but not the valve itself – it never hurt).
June 13th, 2021
Went from having a regular 3 large poops a day (6’5” tall, 220lbs, big guy) on June 11th to 1 small poop that was smaller than my 2-year-old’s on June 13th.
Booked doctor’s appointment right away as I felt HORRIBLE.
Had to pee ALL THE TIME now, and had even harder time initiating it.
June 25th 2021 PCP does blood work, says I’m fine.
So I was ME/CFS free from mid ~2011 to mid 2021, when gut trauma, after exposure to the O.G. COVID triggered me back into it.
Lost 26lbs between June 12th 2021 and November.
Kept visiting specialists telling them I felt horrible.
All say I’m fine and send me away.
So I convinced myself I _was_ fine and went about life with it being super-hard and poor sleep.
December 13th, 2021
Moderna COVID-19 VACCINE BOOSTER
Lot: 045J21A
K545
Costco 629
December 23rd, 2021
Catch what seems like a cold, turns out to be COVID. Quarantine.
Start to feel better, but still have to pee all the time. Continuing to lose weight.
Have “food poisoning” January 8th 2022.
After which I’m constantly fatigued. Can’t keep up with kids.
Falling asleep randomly after work.
Bad brain fog starts.
“Walking headaches” where each step my head would hurt, and feel full.
Slight pain in same lower right quadrant small intestinal area that had trauma.
Intermittent very-bad sleep disturbances start.
Another “food poisoning” and RSV infection February 7th 2022.
After which I couldn’t poop for days.
Stringy, force-out poops thinner than a pencil.
Ended up with distended abdomen and finally losing consciousness twice getting out of bed on February 14th and in ER.
Doctors perplexed, no idea what’s wrong. Sent me home with Z-pac, Claritin, and Ibuprofen. I felt good-ish for 5 days following.
I felt better for the 5 days on Z-pac (azithromycin), which is likely because it temporarily removed the bad bacteria (e.g. here) in my gut and it is an anticoagulant (NIH)
For both food poisonings, no one else with me got sick, eating the same food. And we were just eating out at restaurants instead of our normal/healthy at-home meals.
Symptoms started rinse-repeat after 5 days. Ended up in ER again about 2 weeks later (end of February). No advice, just sent home.
Health kept trending downward, and we couldn’t figure out how/why.
Saw teams of specialists throughout 2022. Gastro, heart, pulmonary, neurological, neuromuscular, endocrinologist, urologist… you name it, I’ve seen 3x of them at least.
In July 2022 I did a round of HIIT (High Intensity Interval Training) to prepare for soccer season (like I do every year).
One week later I had disturbing fasciculations (video here).
Went to primary care doctor who thought that I had some neurological disease. I concurred.
Had every test done for neurological diseases done. “Not only is this not neurological, neurological isn’t even on the list” the top neurologist in Denver said after poking needles into me and doing nerve conduction, nerve attenuation, nerve dynamic stimuli response, and many other tests.
Spent the next several months going to every type of doctor you can imagine. Gastro, endocrine, urology, pulmonology, cardiology… you name it, I saw 3 of them. And also a bunch of DOs, MDs… everyone you can imagine.
In July the only best-guess was ME/CFS – which came without any advice on how to stop my rapid downward spiral.
I self-treated for a month (using a regime very similar to above, after reading a TON on the internet and many books on it), and regained the capability to bike for 30 minutes, and walk 12 flights of stairs up and 12 flights of stairs down, including going on walks with the family.
I had developed POTS in July as well, and so we booked appointments for being taken care of by a team of POTS doctors. That care started in October and they collectively made me MUCH worse from September until December.
They kept telling me I was recovering.
And I didn’t have the gusto to tell my family that they were making me worse and that my internet research and books I read on ME/CFS was better THAN A TEAM OF DOCTORS.
I just felt crazy saying that.
So from September to December under the care of the POTS team, I lost ~40lbs (at least) and went from 30 minutes of exercise to not being able to being barely able to walk.
By mid-to-late January I could no longer walk, and could barely get out of bed. And I lost the capability to defecate.
By February 1st I lost the capability to control (or feel anything) in my right leg and both arms below the shoulder. And I lost the capability to urinate
I was urinary-catheterized, fed via my heart, and given fluids via an IV as I could no longer drink.
Early February I left the hospital because the prognosis was I had days to live.
I re-started experimental self-treatment based on this research around February 4th.
By February 7th I could walk again.
Around February 9th I felt so good that I used way too much energy and crashed. Walking, talking, touring the outdoors, and even attempting a jog.
And this brings me to today, where I spend my energy researching to try to help others, and if possible, to make me recover. I can walk, make jokes, and hang out with friends at home. But I don’t quite have enough energy (yet) to fully take care of myself.
And now, I spend most of my energy on self-treatment research, and documenting it to help others. Most of which is evaluating the supplements from MoreThereThanHere on Reddit, the research on which is here (make sure to read the comments; there’s much research in them). And my current (and full history) of supplements is here.
And I’m slowly, and very-bumpily, getting better as I try out new supplements to see if my theory on them is right or wrong.
Sometimes I’m right, and I get better.
Sometimes I’m wrong, and get worse.
But overall the slope has been upwards, which is all I can ask for.
And my current effort is figuring out how to rid my gut from the bad bacteria (many of which are horrible for me) from my most recent Ombre report, here, and then using MicrobiomePrescription to figure out which supplements I should or shouldn’t take, and which antibiotics I should or shouldn’t take.
And it is VERY clear from that report that all my bad symptoms come from those bad bacteria.
And this fits with if I just didn’t eat, I’d feel fine. As then I wouldn’t be feeding the bad bacteria.
Treatment on my Kids
My son (4 years old) and daughter (2 years old) both got quite ill when I got quite ill in February, all from RSV, and remained ill up until I started piecing together this research.
Using only very light versions of the treatment above – nearly completely diet only (low/no histamine, low sugar/carbs, basic supplement in the morning with fish oil and other vitamins), both have now fully recovered and are totally different children.
Happy, healthy, and no longer constantly sick/upset and waking up 3-5 times a night.
Prior to this, my son and daughter were both heading in my trajectory (constant, non-stop itchy rashes, flushing, irritation, and constant digestion/eating issues and expressed pain).
My son’s condition had gotten so bad that he was coughing once every 3 seconds all 24/7.
Now they are fully recovered and SO much happier/healthier and both have grown substantially since we figured this out. They’re like completely different children.
Before piecing this together and treating our children, my son and daughter would wake up every morning upset, grumpy, itchy, and with flushed red faces looking tired. And this was after being up 3-4 times a night (where they’d come get us) and likely an unknown-number of additional wakeups (where they wouldn’t come get us).
And now, zero wakeups, and they come into our room cheery, wanting to make jokes/play games, and sleep until 7am instead of 6am. And that’s going to bed at the same time, and with no wakeups. So their quantity and quality of sleep is WAY up.
To-Do
Pull information from cross-check sheet back into the main document.
Spore based products and how much they help, filling out this section with links and explanations.
Make an infographic of how the whole cascade and feedback loops work.
How to stay in remission. Ken’s approach of clearing out toxins:
My usual is 400 mg when I wake up and 400mg at bed time.
Bed time: To improve oxygen delivery and thu sleep quality
Wake Up: to help remove any toxins produced by the immune system (which gears up while you sleep… )
Research more about types of T cells, including CD4+ and Tregs and their role in immune system dysfunction.
Write up this voice conversation on CAR T-Cell Therapy.
The core of the disease is senescent T-cells (aged, broken T-cells) which are telling the body that it’s bleeding out, that it needs to clot, and that it needs to inflame.
Write up the bit about T-cells being senescent and that being core to the overactive cytokine response per this excellent post here and notes below and this article https://pubmed.ncbi.nlm.nih.gov/31830003/
Write up why this causes dysautonomia (vagus nerve is outside of spine, gets hit hard by clotting/inflammation whereas the nerves in the spine are protected by the blood brain barrier)
Similar WRT small fiber neuropathy (which can wax/wane based on inflammation/clotting coming and going).
Write up connection to POTS.
Find sources that showed excess mortality for each
Explain why sugar becomes damaging to tissue in this condition (mitochondria end up being forced into anaerobic)
Retrieve and link sources for many claims
Treating gut dysbiosis section
Make Brain-Fog-Friendly (BFF) version
Integrate these links, which agree/backup the thesis here.
Write up why Blood letting worked on my Dad when caught early: The reason Blood letting worked on my dad was multifold:
1. Let’s clotted blood drain out.
2. Let’s senescent T-cells drain out. The senescent T-cells (old, freaking out) are what cause the inflammation and clotting.
Write up that AHCC (which stimulates T-cells) made me rapidly worse. Has cold and sore throat symptoms all night.
Whereas 1mg Rapamycin, which Dow regulates the impact of T-cells made me feel much better and resulted in demonstrably better sleep.
Research in Progress:
Midodrine – for low blood pressure.
Research motility pro and also the artichoke extracts that MoreThereThanHere is taking, as he’s taking similar, probably to help with motility and gut health, here
Relationship between Lactoferrin and sphingosines
lactoferrin has been found to stimulate the production of ceramide, a type of sphingolipid that plays a critical role in cellular signaling and apoptosis, per ChatGPT.
And I was getting better on OrthoSpore IG back in September and early October.
Pentoxifylline Is An Inexpensive And Widely Available Oral Anti-Tumour Necrosis Factor Agent For Prevention Or Treatment Of Cytokine Storm In COVID-19 COVID-19
Cistanche Tubulosa is a traditional Chinese medicinal plant that has been studied for its potential health benefits, including immune-enhancing effects. While there is limited research on the specific impact of Cistanche tubulosa on T-cells, some studies suggest that it may have a beneficial impact on the immune system as a whole, which may include T-cell function.
For example, a study published in the Journal of Ethnopharmacology in 2010 found that Cistanche tubulosa supplementation in mice led to an increase in the activity of natural killer cells and other immune cells, as well as an improvement in overall immune function. The authors suggest that these effects may be due to the ability of Cistanche tubulosa to enhance the activity of immune cells and reduce oxidative stress.
In addition, a study published in the Journal of Food Science and Technology in 2018 found that a water extract of Cistanche tubulosa led to an increase in the number of white blood cells in mice, which may include T-cells. The authors suggest that these effects may be due to the ability of Cistanche tubulosa to enhance immune function and reduce inflammation.
Overall, while more research is needed to fully understand the specific impact of Cistanche tubulosa on T-cells, some studies suggest that it may have a beneficial impact on the immune system as a whole, which may include T-cell function. It is important to note that Cistanche tubulosa should only be used under the supervision of a healthcare provider, as it may interact with certain medications and may not be appropriate for all individuals.
Enzymatically modified rice bran (EMRB) extract is a dietary supplement that is derived from the outer layer of rice bran. It contains a complex mixture of bioactive compounds, including polysaccharides, proteins, and flavonoids, that have been studied for their potential health benefits.
There is some evidence to suggest that EMRB extract may have an impact on T-cells, which are a type of white blood cell that play a critical role in the immune response.
For example, a study published in the Journal of Nutritional Science and Vitaminology in 2015 found that EMRB extract supplementation in mice led to an increase in the number of T-cells in the spleen, as well as an improvement in the activity of natural killer cells and other immune cells.
In addition, a study published in the Journal of Medicinal Food in 2013 found that EMRB extract supplementation in human subjects led to an increase in the number of T-cells and other immune cells, as well as an improvement in overall immune function.
Overall, while more research is needed to fully understand the potential benefits and risks of EMRB extract supplementation for T-cell function, some studies suggest that EMRB extract may have an impact on T-cells and other immune cells, which may contribute to its potential immune-enhancing effects. It is important to note that EMRB extract should only be used under the supervision of a healthcare provider, as it may interact with certain medications and may not be appropriate for all individuals.
Thymic Protein A (also known as Prothymosin Alpha) is a naturally occurring peptide that is produced in the thymus gland. It has been studied for its potential immune-enhancing effects and has been used to support immune function in individuals with a variety of health conditions.
There is some evidence to suggest that Thymic Protein A may have a beneficial impact on the thymus gland. Thymic Protein A has been shown to promote the development and maturation of T cells, which are produced in the thymus gland. In addition, Thymic Protein A has been shown to stimulate the production of thymic hormones, which are critical for the development and maturation of T cells.
Studies have also suggested that Thymic Protein A may have a protective effect on the thymus gland. For example, a study published in the Journal of Endocrinology in 2007 found that Thymic Protein A administration in mice led to a reduction in the age-related decline in thymus function and an increase in the number of T cells in the thymus gland.
Overall, while more research is needed to fully understand the potential benefits and risks of Thymic Protein A supplementation for thymus function, some studies suggest that Thymic Protein A may have a beneficial impact on the thymus gland by promoting the development and maturation of T cells and protecting the thymus gland from age-related decline. It is important to note that Thymic Protein A should only be used under the supervision of a healthcare provider, as it may interact with certain medications and may not be appropriate for all individuals.
Butyric acid is the energy source which intestinal cells prefer over others, accounting for up to 70% of the energy produced by the cells of the gut, and is critical for both maintaining and rebuilding gut health.
Rapamycin, good article here, and website on it here
From ChatGPT: Rapamycin is a drug that was initially developed as an immunosuppressant, but has since been found to have a variety of other potential health benefits. It works by inhibiting a protein called mTOR, which plays a key role in regulating cell growth and metabolism.
Some of the potential benefits of rapamycin include:
Anti-aging effects: There is growing evidence that rapamycin may have anti-aging effects, possibly due to its ability to improve cellular health and reduce inflammation. Some studies have shown that rapamycin can extend lifespan in animal models, and there is ongoing research into its potential benefits for human longevity.
Cancer treatment: Rapamycin has been used in cancer treatment, as it can inhibit the growth of tumors by blocking mTOR signaling. It has been used to treat several types of cancer, including kidney cancer and certain types of lymphoma.
Neurological conditions: There is some evidence to suggest that rapamycin may have potential benefits for the treatment of neurological conditions, such as Alzheimer’s disease and traumatic brain injury. This may be due to its ability to reduce inflammation and improve cellular health in the brain.
Metabolic disorders: Some studies have suggested that rapamycin may have potential benefits for the treatment of metabolic disorders, such as diabetes and obesity. It may improve insulin sensitivity and reduce inflammation, both of which are important factors in these conditions.
However, it is important to note that rapamycin can have side effects, and its long-term effects on human health are not yet fully understood. It should only be used under the supervision of a healthcare provider, and the potential benefits and risks should be carefully considered.
Metformin with Rapamycin, from ChatGPT: Metformin is a medication that is commonly used to treat type 2 diabetes, a condition in which the body is unable to properly regulate blood sugar levels. It works by reducing the production of glucose in the liver, increasing the sensitivity of cells to insulin, and slowing the absorption of glucose from the intestines.
In addition to its use in diabetes, metformin has been investigated for its potential benefits in a variety of other health conditions, including obesity, polycystic ovary syndrome (PCOS), and cancer. Some of the potential benefits of metformin include:
Weight loss: Metformin may help to promote weight loss in individuals with obesity or insulin resistance. This may be due to its ability to reduce the production of glucose and improve insulin sensitivity.
Improved fertility: Metformin may help to improve fertility in women with PCOS, a condition that can cause irregular periods and difficulty getting pregnant. It may help to regulate ovulation and improve hormone levels.
Reduced cancer risk: Some studies have suggested that metformin may help to reduce the risk of certain types of cancer, including breast, colon, and prostate cancer. This may be due to its ability to reduce insulin levels and inhibit the growth of cancer cells.
Improved cardiovascular health: Metformin may help to reduce the risk of cardiovascular disease in individuals with diabetes, potentially by improving blood sugar control, reducing inflammation, and improving lipid levels.
While metformin is generally considered to be safe and effective, it can have side effects, particularly in individuals with certain medical conditions or who are taking certain medications. It should only be used under the supervision of a healthcare provider, and the potential benefits and risks should be carefully considered.
The new/alternate approach to treating microclots is HELP Apheresis:
https://beatejaeger.com/en/h-e-l-p-apheresis/
It is currently being done in Germany.
“Additionally, H.E.L.P. apheresis potentially removes the SARS-CoV-2 spike protein and microclots present in Long COVID patients (5). “
Supplemental notes
In severe Brain/Spine Injury, lesions can be seen on an MRI, and are considered to be the result of micro-emboli by some researchers, e.g. here.
Ken’s overall approach:
Increasing oxygen flow to the entire body. Typically this means one or more of the following:
Anti-coagulants – best general one is low-dosage heparin (LMWH/Lovenox). It’s cheap and if taken sublingual, no injections are needed. For my Ken’s coagulation mutation, piracetam works as well.
Great resource on low-dose heparin, here. And it is Lovenox, which is taken sublingually. Recommended 30mg in AM for me.
Ken took both Lovenox, Piracetam, and the Fibronolytics in parallel.
Fibrinolytics: Typically bromelain, nattokinease, serrapetase, lumbrokinese. Fibrin deposits can prevent the passage of oxygen to the tissue.
Vascular dilators: My favorite is flushing niacin. I take 400 mg twice a day as a prophylactic. If I get a flush, I know it is warranted. There are others.
Anti-inflammatory: Having blood vessels inflamed restricts oxygen delivery. There are many choices here, likely good to rotate thru several and note any that causes significant improvement.
Hyperbaric Oxygen Chambers: A short term assist but does not address the cause
The human body is fare more complex than a car, but the car analogy is a good starting point. The car is running “rough” – some possible causes:
Fibrinolytics – clogged oil or gas filter
Anti-coagulants – fuel stabilizer, many fuels will become jelly like or deteriorate if left a long time
Vascular dilators – fuel or coolant lines, if pinched, the engine may not work well
Anti-inflammatory – fuel or coolant lines have garbage in them or deteriorating or wrong size
Feedback loop: Engine timing is off. Sparkplugs are firing too late or early
Dashboard Dials: Sending the wrong signals (i.e. fuel gauge is not working), high RPM because you forgot to change gears, etc
Quick Lesson on Coagulation
Often there can be a weakness (DNA/SNP mutation) that makes one part less efficient. Typically, this may not cause any issue –but with the wrong sets of chemical signals, it can either overproduce items “upstream” or inhibit one step.
The diagram shows the cascade, all it takes is one weak link or a different link getting stuck on high.
The biggest challenge is treating all of the factors concurrently. Many MDs will opt for a “let us try just one thing at a time”. You cannot isolate the parts and deal with just one — the signaling chemicals will keep flowing across the entire body. This approach rarely works when there are multiple feedback loops occurring. Personally, I use the flushing niacin as a feedback loop damping mechanism. If I have a cold, flu or other issues, I will add in other stuff to try to keep the loop from getting re-established.
Email from Ken Lassen here:
Try 400 mg of (flushing) niacin – NOT niacinamide (see What Is the Difference Between Niacin & Niacinamide? | livestrong), — why ” Niacinamide, however, does not have the same vasodialating, or blood-vessel widening, effects, that niacin has,” — you are testing if vascular constriction (possibly due to inflammation) is a factor. I would suggest testing every hour or so (I am lazy, my smart watch does it every 10 minutes)…
Assuming no salicylate sensitivity, try a few days taking the maximum dosage specified on the bottle(spread across the day) – you are testing if palette aggregation is a factor
Then try Alpha Lipoic Acid for a week (to give it time to work) (see Alpha Lipoic Acid | CFS Remission ). Ideally a low dosage every 2 hours (it has a short half-life)
Raise the question of DNA analysis of the individuals. I suspect some SNP may be in common with subgroups
Special note on Piracetam
Nothing has helped my mental health more than Piracetam. It’s absolutely incredible. The `why` is that it’s neuroprotective in the face of ischemia. So in other words, it allows your brain to still work properly even in the low-oxygen environment caused by the micro-clots and the (histamine) inflammation.
In healthy volunteers, piracetam mediated a direct stimulant effect on prostacycline synthesis and reduced the plasma levels of fibrinogen and von Willebrand’s factors (VIII: C; VIII R: AG; VIII R: vW) by 30 to 40%, from here
Prostacyclin is a prostaglandin member of the eicosanoid family of lipid molecules. It inhibits platelet activation and is also an effective vasodilator.
Fibrinogen seems to be the main cause of the microclots. So this is why piracetam is so recommended. And it dilates the blood vessels, which is needed in these conditions. (My blood vessels have gotten progressively tinier as I’ve gotten worse.)
And the von Willebrand’s factors are below. Note that it gets A LOT of them.
Piracetam is used to treat vaso-occlusive crisis, which occurs when the microcirculation is obstructed by sickled RBCs, causing ischemic injury to the organ supplied and resultant pain.
Used to treat adult patients suffering from myoclonus of cortical origin, irrespective of aetiology, and should be used in combination with other anti-myoclonic therapies 5.
Piracetam mediate neuroprotective effects against hypoxia-induced damage, intoxication, and electroconvulsive therapy 5.
Vascular effects:
Piracetam is shown to increase the deformability of erythrocytes, reduce platelet aggregation in a dose-dependent manner, reduce the adhesion of erythrocytes to vascular endothelium and capillary vasospasm. In healthy volunteers, piracetam mediated a direct stimulant effect on prostacycline synthesis and reduced the plasma levels of fibrinogen and von Willebrand’s factors (VIII: C; VIII R: AG; VIII R: vW) by 30 to 40% 5. Potentiated microcirculation is thought to arise from a combination of effects on erythrocytes, blood vessels and blood coagulation 1.
And more from ChatGPT on Piracetam:
“Piracetam is a nootropic drug that is used to improve cognitive function and memory. It was first developed in the 1960s and is still widely used today.
Piracetam is believed to work by enhancing the function of the neurotransmitter acetylcholine, which is important for learning, memory, and other cognitive functions. It also increases blood flow and oxygen consumption in the brain, which may further enhance cognitive function.
Piracetam is used to treat a range of conditions, including dementia, Alzheimer’s disease, and other age-related cognitive decline. It is also sometimes used to improve memory and concentration in healthy individuals, although its effects in this population are not well established.
Piracetam is generally well-tolerated and has few side effects. Common side effects may include nervousness, insomnia, and gastrointestinal symptoms such as nausea and diarrhea. Rarely, it can cause more serious side effects such as headaches, dizziness, and skin rash. It is important to talk to a healthcare professional before taking piracetam to determine if it is an appropriate treatment option. It may interact with other medications or health conditions.“
Month-long update from Hannal on the supplements above:
It's important to know that even though these are supplements, they come with nontrivial risks – it's important to find an up-to-date doctor to try these under!
A subset of 24 patients was treated with one month of dual antiplatelet therapy (DAPT) (Clopidogrel 75mg/Aspirin 75mg) once a day, as well as a direct oral anticoagulant (DOAC) (Apixiban) 5 mg twice a day. A proton pump inhibitor (PPI) pantoprazole40 mg/day was also prescribed for gastric protection.
Cyprus pre-treatment:
1. Rupatadine 10mg once a day or Fexofenadine 180mg twice a day. Trade names: Rupafin, Urtimed, Rupall
2. Famotidine 40mg twice a day
3. Toxaprevent 3 capsules twice a day empty stomach for 6 months
4. Toxaprevent 1 sachet 1 hour before lunch for 2 months
Dear Dr Gilles,
It was a pleasure talking to you yesterday.
I have presented your nephews case you described so well to our doctors.
So before travelling to get Help Apheresis treatments, this is what our initial treatment recommendation looks like:
MCAS (mast cell activation syndrome) and depression/anxiety symptoms as part of Long Covid:
As discussed, my mother was on the same regime and has now almost fully recovered with that and 4 Help Apheresis treatments (symptom free and at 70-80% of her energy level).
For more information on the Help Apheresis for Long Covid, please register for free on https://lca-med.org (a community project we support – a resource for GPs/doctors on Help Apheresis for Long Covid).
Glycation is a spontaneous non-enzymatic reaction of free reducing sugars with free amino groups of proteins, DNA, and lipids that forms Amadori products. The Amadori products undergo a variety of irreversible dehydration and rearrangement reactions that lead to the formation of advanced glycation end products (AGEs). Glycation is a process which is caused by the presence of exc ess glucose in skin fibers. This excess triggers an internal reaction in which sugar molecules adhere to the collagen and elastin proteins, which normally help keep skin firm and supple. It is a normally occurring in aging.
Neurotrophic
Neurotrophic factors (NTFs) are a family of biomolecules – nearly all of which are peptides or small proteins – that support the growth, survival, and differentiation of both developing and mature neurons. Wikipedia
Autophagy
A process by which a cell breaks down and destroys old, damaged, or abnormal proteins and other substances in its cytoplasm (the fluid inside a cell). The breakdown products are then recycled for important cell functions, especially during periods of stress or starvation. NIH
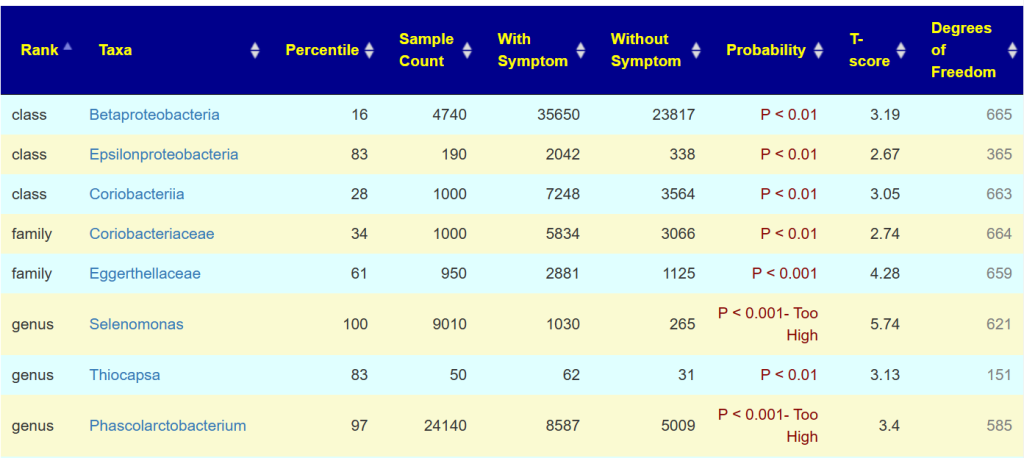
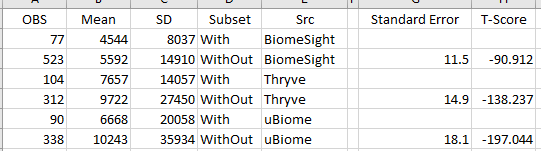


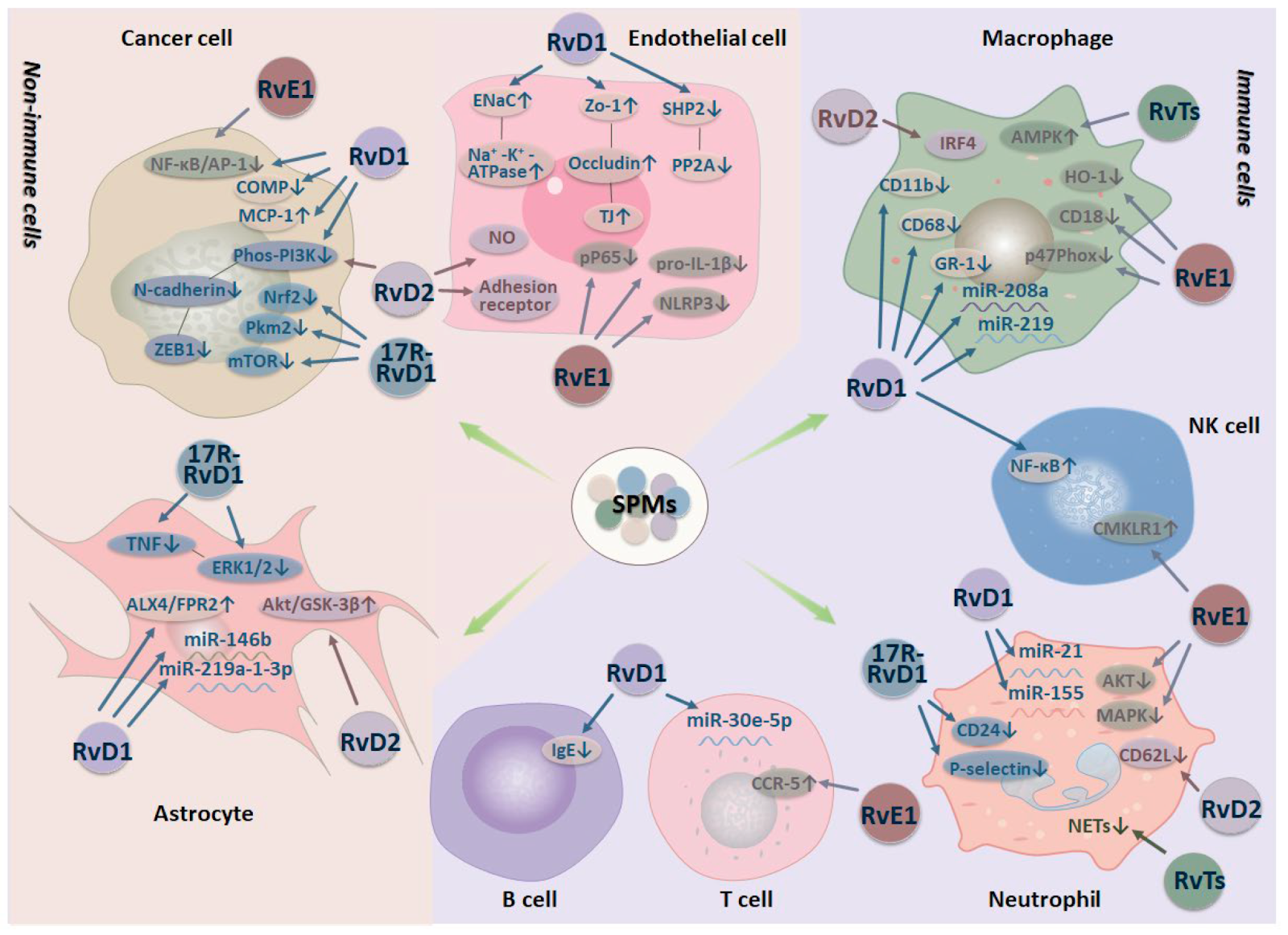


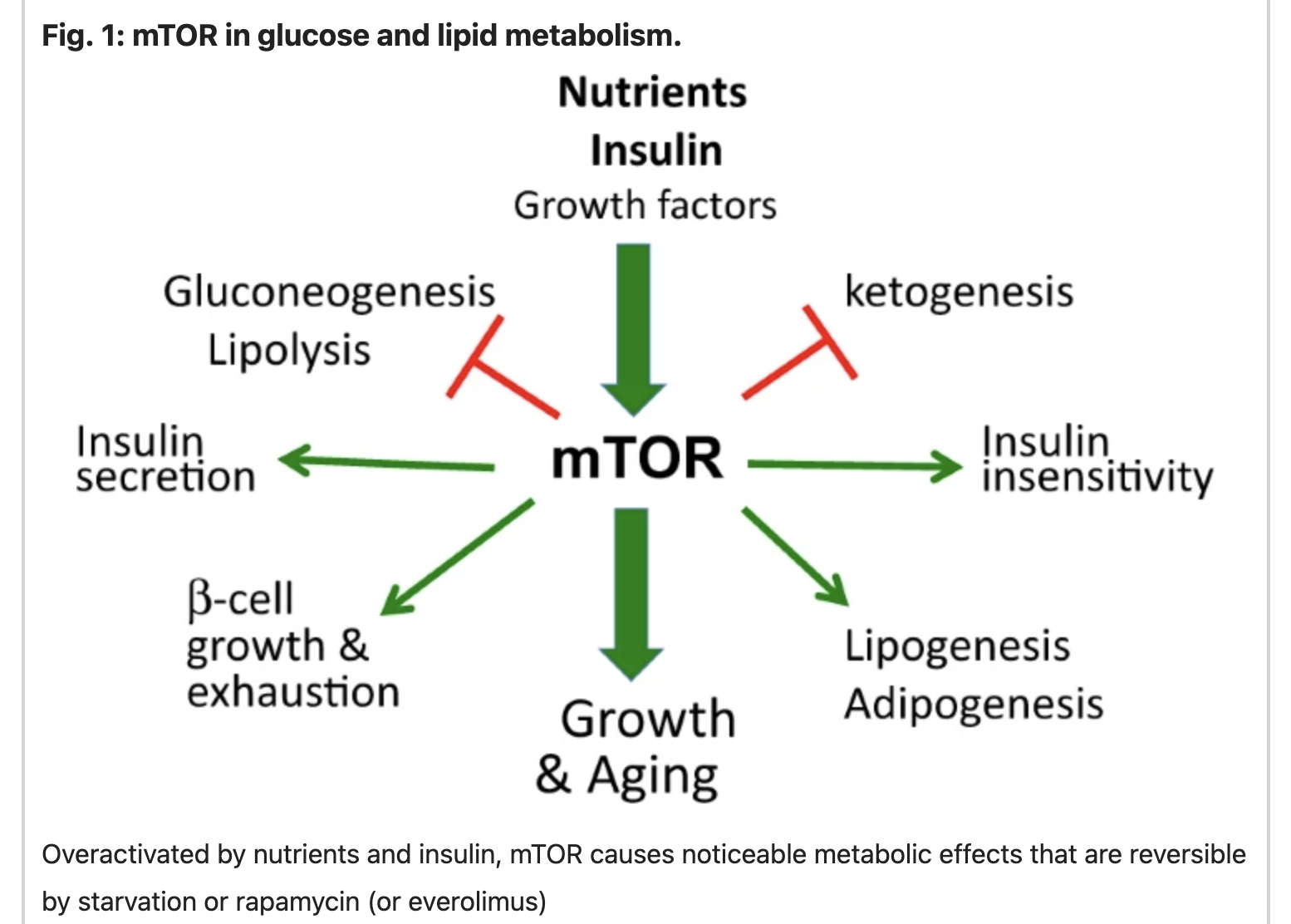
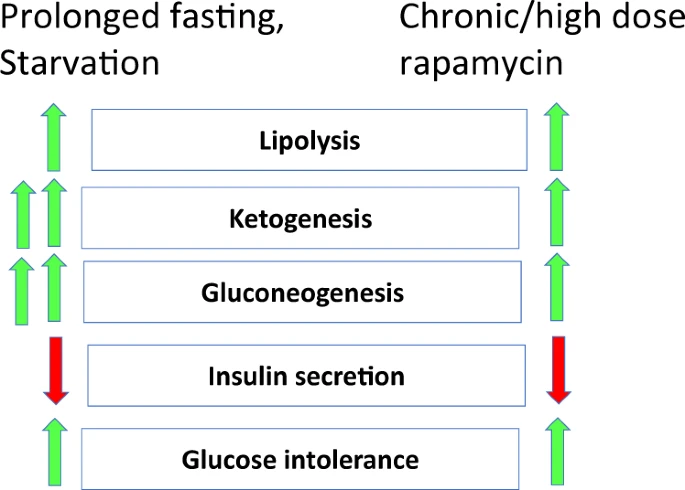

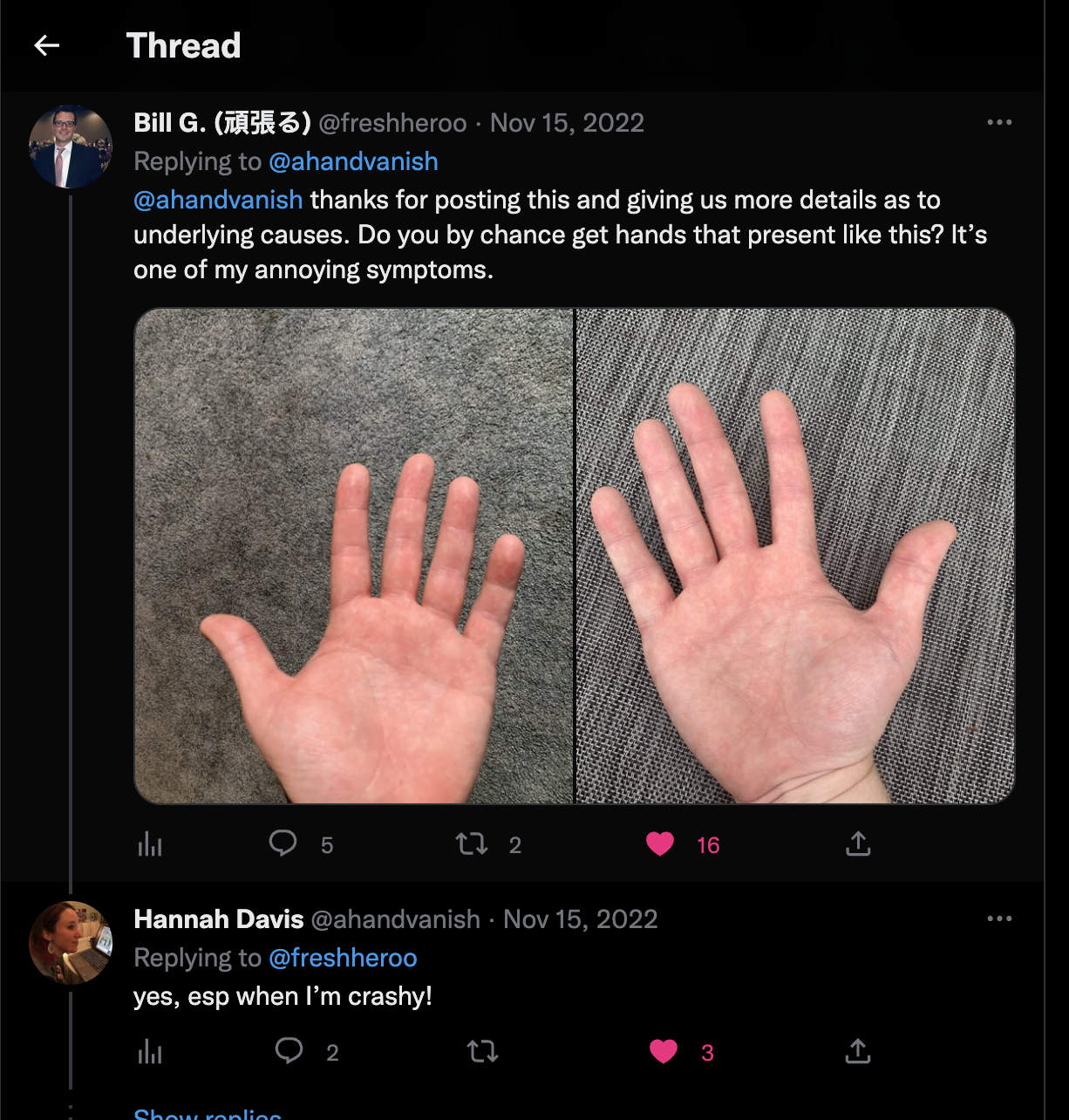
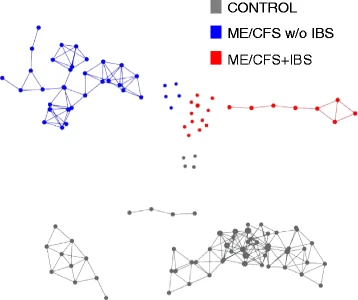{kind=link}
Recent Comments