I am hoping this will be a model for other Long COVID people to start the recovery process. This person used Biomesight. Those results allow the data from special studies to be used on his microbiome sample.
A word of warning, tests like GI-MAPS will not report on most of the bacteria found to be low in the Special Studies — you need much more detail reports!
Suggested Parallel Reading: CFS Patient after COVID using the Special Studies Results
Foreword – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
Backstory
COVID in February 2021. 37M at the time, athletic/fit. Crossfit x 3 a week, playing football weekly Only mild gastritis prior to COVID. No other health issues. Moderate severity Covid, lots of symptoms.
And then Long COVID and CFS/ME type of symptoms mostly fatigue, PEM and GI problems (pain, food intolerance, bloating..etc) I’d say it’s a moderate/mild case of CFS/ME. But after 18 months still not back to previous levels, can’t walk too long otherwise i crash. I’d say i am around 75%.
High Level Overview
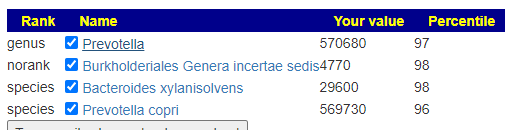
Looking at Health Indication, we find no significant medical conditions flagged (consistent with prior life style). There is one bacteria of potential concern: Prevotella copri, accounting for a whooping 56% of the microbiome! It is interesting that this was also seen in another recent review, see CFS Patient after COVID using the Special Studies Results. In terms of Dr. Jason Hawrelak Recommendations – he’s at the 99.7%ile — extremely healthy!
Using Special Studies
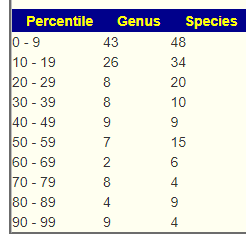
Interpreting the updated table shown below can get a little complicated (i.e. not naively simple) see Special Studies Percentage Matches for details
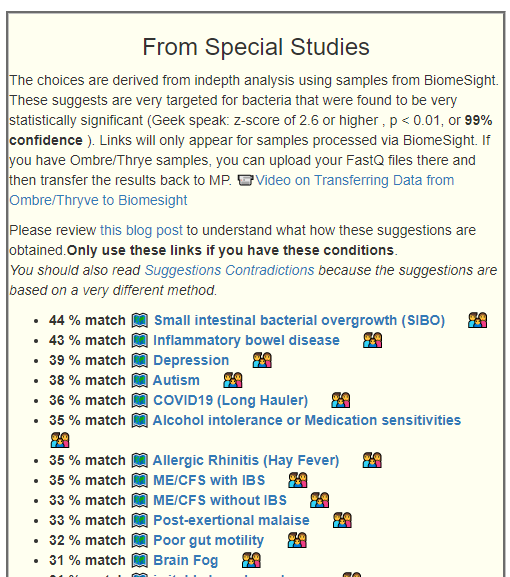
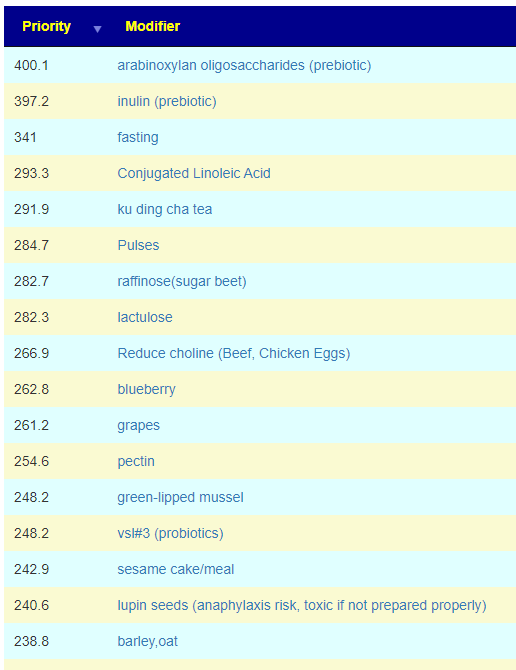
We are going to use the 7 items below – items matching his reported issues. In an independent study that I did, I found that the pattern dims over time as the microbiome evolves. His person is 20 months post-COVID.
- COVID19 (Long Hauler)
- Small intestinal bacterial overgrowth (SIBO)
- ME/CFS with IBS
- Inflammatory bowel disease
- Post-exertional malaise
- General Fatigue
- Bloating
The Prevotella copri concerns me because it’s the mastodon in the room (bigger than an elephant, and a bit hairier!). This specific bacteria is NOT typical for long COVID, but I suspect many will find one or another tyrant to dominate in excess in the face of massive minority representation– hence check for high bacteria counts with high percentile. It was also high in the study cited above, CFS Patient after COVID using the Special Studies Results. I went thru the My Biome View to tag the ones that have a high percentile with with a large count. The purpose is to inhibit these, so they will not inhibit everything else.
The results were almost the opposite of the consensus below for B-Vitamins. It presents a dilemma, a choice that needs to be made. At the moment, I favor the working from the special studies approach (pending feedback from people who tried it). Conceptually, it is a more probable approach — incidentally, it is not the approach usually done (and those approaches, historically, have had very little success to date).
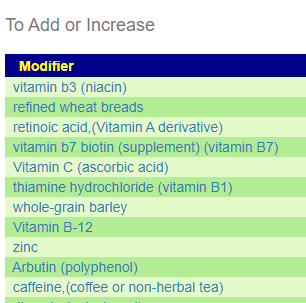
The Consensus
I did not want to toss in any more sets of suggestions. From the start we saw the dominate item in his microbiome was undergrowth of a multitude of bacteria and the domination of one — we have gotten what helped the weak and inhibits the strong.
I found the avoids to be an interesting combination, no red meat and no chicken (matching Reduced choline on the to take) .
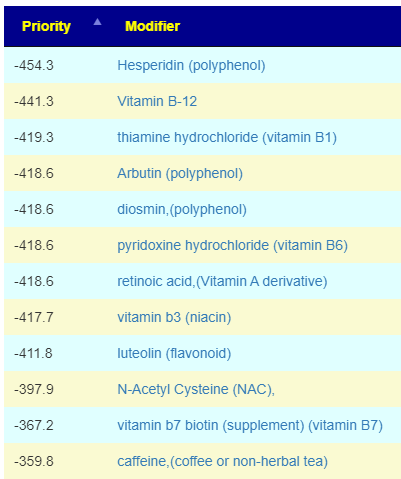
We see that something like a B-Complex should be avoided. I discuss this issue more in the other blog post that I cited above.
Computed Probiotics from KEGG Enzymes
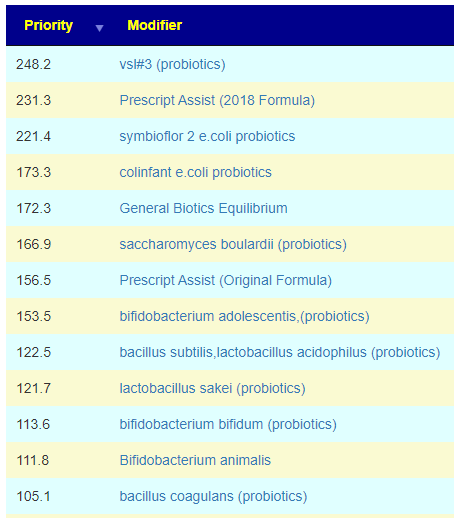
This produced a few items that are reasonably easy to get as single species probiotics. Remember, these are calculated by a totally different mechanism – using the genes of the bacteria in your microbiome and the genes in these bacteria. The top items were:
- Escherichia coli (which is near the top of our to take list)
- Bacillus subtilis (on our to take list) and other similar bacillus species
- Akkermansia muciniphila (which shows up once, with a positive value (74.5) on our consensus)
- Clostridium butyricum (a minor avoid on the consensus with 3 for and 4 against)
- Lactobacillus plantarum (a minor avoid on the consensus with 3 for and 4 against)
My basic take-away are using just 3 probiotics in weekly or fortnight rotations (one at a time)
- Escherichia coli (Mutaflor or Symbioflor-2)
- Bacillus subtilis many sources
- Akkermansia muciniphila (available only in the US unfortunately)
If one of the above cannot be obtained, I would suggest using Clostridium butyricum or Lactobacillus plantarum as the third element in the rotation.
Supplements suggested by KEGG
Although this is using an old algorithm that I have not updated, the list is below.
- alpha-galactosidase (Enzyme) – Percentile: 11
- Amylase (Enzyme) – Percentile: 8 – On Consensus: Take
- beta-alanine – Percentile: 2 – On Consensus: Take
- Glycine – Percentile: 4 – – On Consensus: Minor avoid
- iron – Percentile: 7 – On Consensus: Take
- L-Cysteine – Percentile: 3 – On Consensus: Major avoid
- L-glutamine – Percentile: 14 – On Consensus: Major avoid
- L-Histidine – Percentile: 12 – On Consensus: Take
- L-methionine – Percentile: 10 – On Consensus: Major avoid
- L-Serine – Percentile: 11 – On Consensus: Take
- L-Threonine – Percentile: 16
- magnesium – Percentile: 4 – On Consensus: Take
- NADH – Percentile: 4
- Selenocysteine – Percentile: 4
- zinc – Percentile: 16 – On Consensus: Take
Remember we are dealing with fuzzy data, my usual rule is do positive stuff where there is universal agreement, avoid stuff that are negative or where there are contradictions (I do like playing dice with my health).
Bottom Line
Because of the special studies and this person using the appropriate lab, this was actually a simple analysis to do. The traditional analysis showed “nothing wrong”, a familiar restrain from medical professionals to Long COVID patients. Our special studies and distribution by percentile showed things are wrong. Having 56% of the bacteria being Prevotella copri is saying something is very wrong.
I often try to use analogy of human populations to explain what I see. In this case, we have dozens of small tribes battling each other allowing a dominating force to seize most of the space. There are many historic examples, often under the name of “Divide and Conquer”.
In this example, the high number of low representation bacteria we saw in the overview matched the high number of low number of bacteria we observed in our special studies.
After two months of trying the suggestions, I hope this reader will do a new sample to see how well things shift from these suggestions.
Questions
Q: “Excuse me if I’m missing something but is there any reason why we are focusing on only Commensals, Prevotella, why not on Probiotics at all? I understand it’s way above the range, and it’d like to keep it low ideally, but what about the rest of Microbiome?”
A1: First “the rest of the microbiome” issue – the obvious response is a simple “If it is not broken, don’t fix it”. The above analysis used over 100 different bacteria. Our focus is on the bacteria where there is significant statistically evidence that they are connected to Long COVID. The numbers above are general health. As cited above, with Dr. Jason Hawrelak General Health Recommendations you are better than 99.7% of people. There is a huge variation in recommended ranges coming from labs and specialists — who are you going to rely upon? I am a statistician and I follow the numbers (and the z-scores), in other words, not working off opinion based largely on treating people who do not have Long COVID. I am NOT focusing on commensals, I am focusing on what was shown to be statistically significant.
A2: “why not on Probiotics at all” — Excuse me, I name four key probiotics: Escherichia coli (Mutaflor or Symbioflor-2 are retail products), Bacillus subtilis et al (microbiome labs/ megasporebiotic looks like a good commercial choice), Akkermansia muciniphila (Pendulum) and Clostridium butyricum (miyarisan). You will find alternative brands for some using the probiotic page.
If you mean bifidobacterium and lactobacillus probiotics — they are not indicated in general, in fact, they often appear in the to-avoid list. Example, Long COVID often has brain fog, see this study: Brain fogginess, gas and bloating: a link between SIBO, probiotics and metabolic acidosis [2018] which calls out those two as contributors.
Comment: To answer your question, I’ve had lots of symptoms in the beginning, but for now only mild fatigue and PEM plus gut issues, so I’d say definite ME/CFS with IBS, some Rhinitis, Alcohol intolerance and Long hauling.
Recent Comments