This is the second review I have done since working through the implications of Mathematically Derived Healthy Microbiome. It highlights two very different strategies for improving gut health.
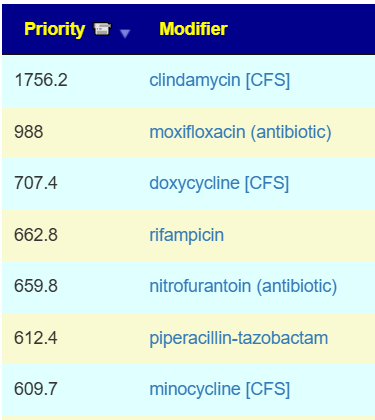
The earlier approach focuses on targeting bacteria that show statistical associations with symptoms. This approach often places many antibiotics near the top of the recommendations. When antibiotics are involved, I tend to favor the Cecile Jadin Protocol for ME/CFS.
The newer approach uses the revised model to target bacteria associated with a healthy, asymptomatic gut. In this approach, antibiotics often appear among the major items to avoid.
Both approaches are based on statistics, but the newer one has a much stronger statistical association.
The earlier approach has a track record of significantly improving the microbiome during the first few cycles. For some people, however, those improvements eventually stall. It also requires a friendly MD to prescribe the antibiotics, which is often a challenge.
If you apply the earlier approach one symptom at a time, the recommendations often contradict each other. “No man may serve two masters” becomes “No recommendations may heal two symptoms.”
The newer approach has no track record yet. It has only recently become available, and it is now being tried by someone whose progress has stalled.
So which one should you use? If you have a friendly MD, I would go with the earlier approach. If you do not, I would go with the newer approach.
Back Story
My symptoms have been somewhat confusing, but for many years ,like over 10 years ago I was constantly bloated with excessive wind/gas but also a lot of belching too. I would eat lots of wheat and sugar and processed foods. 2011 ended up on Proton-pump inhibitors (PPIs) on and off for over 10 years. 2016 appendix burst & got severe peritonitis and ended up very poorly, had 2 weeks of intravenous antibiotics. Slowly recovered.
Years of migraines and brain fog – but yet very active and social.
Then in 2022 I developed throat irritation that was exacerbated (i now believe by certain foods/Ingredients, alcohol, occasional smoking Definately fatty foods but I still cant quite put my finger on what made my throat irritation/ hoarse voice worse). I then developed Biliary Gastritis in October 2024 (Stomach lining erosion) likely from a possible intolerance just like the throat irritation. I became very constipated and still struggle with that.
- Foods that make me worse maybe
- Overly fatty foods
- Possibly milk
- Wheat, bread
- Possibly some fruit
- Big blood sugar spikes off things like carrots and oats, sweet potatoes, very sensitive to carbs and sugar (i wore a glucose monitor out of curiosity) I am not diabetic.
Initial Review
There are two distinct paths, or algorithms, available in Microbiome Prescription.
The prior approach, which I call Traditional, begins with a few straightforward questions:
- Are you prepared to risk a severe Jarisch-Herxheimer reaction? It happens often.
- If you are working, can you afford to miss a few weeks?
- Do you have a friendly MD who is willing to prescribe a single course of each antibiotic listed below and become familiar with Jadin’s protocol?
The newer approach, Healthy Target, was recently added based on an odds-ratio model derived from healthy people. Instead of chasing symptoms, it shifts the goal toward a healthy gut. It does not address individual symptoms directly.
Building Suggestions
Probiotics
We actually have three ways of getting probiotics suggestions:
- Traditional Approach
- Healthy Target using Clinical Studies from PubMed
- Data is very sparse on impacts
- Healthy Target using the “R2 Model” (a statistical model, not clinical studies)
- Data is rich on impacts
We are going to compare only the positive probiotics from the R2 model that are easily available and the top 3 of the other models.
| Bacteria | R2 Model | Healthy x PubMed | Traditional x PubMed |
| Streptococcus thermophilus | 2534 | 4.4 | -179 |
| Enterococcus faecalis (Symbioflor-1) | 1412 | 2.81 | -262 |
| Bifidobacterium infantis | 1123 | -2.77 | -322 |
| Bifidobacterium longum | 762 | 0.74 | -240 |
| Bifidobacterium breve | 389 | -1.2 | -204 |
| Limosilactobacillus fermentum | 47 | 1.31 | 60 |
| Aspergillus oryzae | 30 | -1.34 | -42 |
| pediococcus acidilactici {P acidilactici} | n/a | 7.8 | 75 |
| lactobacillus paragasseri {L. Paragasseri} | n/a | 7.8 | -135 |
| Escherichia coli Nissle 1917 {Mutaflor} | n/a | 7.8 | -12 |
Apart from Lactobacillus fermentum we have disagreement on positive or negative impact. A similar result is often seen when doing symptom by symptom with the traditional approach. We lack sufficient data to have certainty. Being a statistician, I favor the approach with the highest statistical significance — i.e. the novel or Healthy Target approach.
My Current Preference
There is nothing stopping a person trying one approach for 6-12 weeks and then retest; then switch to the other for 6-12 weeks; retest. Make sure that you keep detail notes on responses.
Sample Comparison Tool (example below)
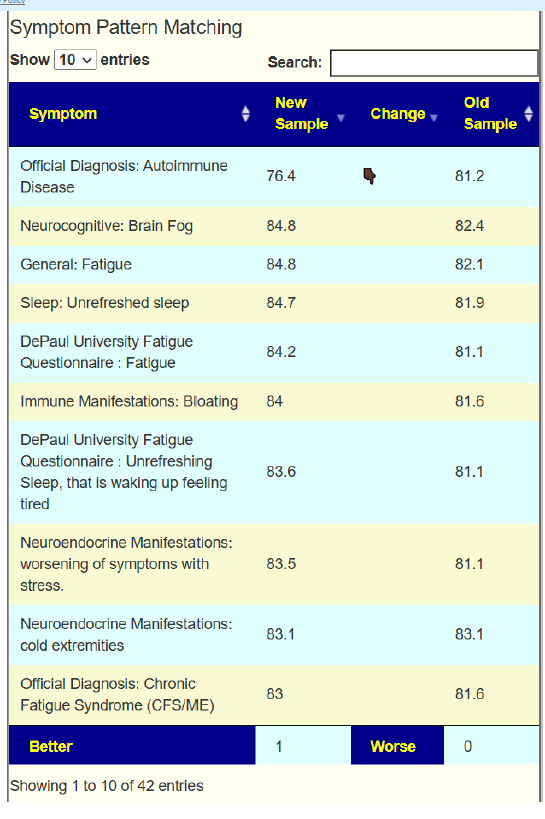
- comparing the Healthy Microbiome Estimate from the two sample
Retrospective: Looking at what they reacted to
| Food | Healthy x PubMed | Traditional x PubMed |
| Overly fatty foods | -1.88 | 262 |
| Possibly milk | – 0.34 | 220 |
| Wheat, bread | -1.36 (refined wheat breads) | -149 (refined wheat breads) |
| Possibly some fruit | 1.73 | -780.1 |
| Range: | -7.82 to 7.82 | -977 to 628 |
| Focus area | -7.82 to – 3.91 3.91 to 7.82 | -977 to -488 314 to 628 |
My impression is that the novel algorithm agrees better with their reactions. This shifts me further towards advocating for the novel algorithm.
Diet Plan
Often people want to simplify suggestions to one specific type of popular diet. This approach often defeat suggestions. Where diet are mentioned, they are secondary or tertiary guidance. Some generic diet studies appears in the suggestions, for example:
- restricted-fiber diet {low fiber diet} at 5.55
- Plant-based diet {Vegetarian diet} 4.57
- low-fat diets 4.37
- low fodmap diet 3.88
- ketogenic diet 3.19
- high-fat diets -1.88
- high-saturated fat diet -2.56
- methionine-choline-deficient diet {methionine-choline deprivation” diet} -2.82
This is intended as supplemental information to refine other suggestions where there is not sufficient information. The diets are what is cited in the literature. Most diets tend to be poorly defined. The classic example is Mediterranean diet. Often the “US Version” fails on the seafood or lamb aspects.
The exact foods vary by region: Greek-style diets may include more yogurt, feta, olives, and seafood, while other Mediterranean areas may use more pasta, beans, lamb, or different local vegetables and herbs. Even the meal pattern can differ, but the overall theme remains plant-forward, minimally processed, and olive-oil based.
Another example is the low-fiber diet. It is usually defined to be under 10 to 15 grams of fiber per day (about 1/2 of the recommended amount of fiber). However, studies show that the US population averages 15-16 grams per day!! so most Americans are already on a low-fiber diet
From the recommendations given I would build a general food diet from:
- 1 cup of blackberries each day, some lingonberry if available at a reasonable price
- Chicken as proteins source, no fish, little meat, no rare beef
- Pumpkin, banana, mushrooms, orka, carrots,
- Figs, banana, Lychee
- Citric juices
- pseudo-cereals {amaranth,quinoa, taro,buckwheat} – for example as a regular morning porridge
Avoid
- Fish
- Dates, Pineapple, nuts
- Celery, Asparagus, mustard greens
- refined wheat breads
The rest are herbs, spices and probiotics. Some avoids that may often be used with foods include:
- Cinnamon, Peppermint, Anise, Clove, Fennel, Sage, Basil, Garlic, Black Pepper, Table Salt
Suggestions are not indented to be dogmatic, rather shift towards one group of foods and seasoning and away from a different group.
Postscript – and Reminder
I am not a licensed medical professional, and the laws where I live prohibit any activity that could be interpreted as practicing medicine or giving personal medical advice. My work is limited to academic and analytical models, and I restrict myself to the language of science and statistics rather than clinical recommendations.
I cannot tell anyone what they should or should not take. Instead, I can present information about items that, based on numerical and statistical analysis, appear to have better odds of improving microbiome-related measures. I am a trained, experienced statistician with appropriate degrees and professional affiliations, and my role is to interpret data—not to treat patients.
All information I provide is for educational and informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Any ideas, rankings, or “suggestions” derived from my analyses must be reviewed and approved by your qualified medical professional before you decide to act on them.
The answers and explanations I provide describe my reasoning and methodology. They are not intended as medical advice for you or for anyone else, and they do not create a doctor–patient or provider–patient relationship. Always consult a knowledgeable licensed healthcare professional before starting, changing, or stopping any treatment, supplement, or health-related regimen.