For some conditions like constipation, if you ask a medical practitioner how to deal with it — the answer you may get may be a simple “Take a good probiotics”. If it is a naturopath, the recommendation will likely be a probiotic from the fridge in the office (likely at a higher price than the same one elsewhere).
What is the BEST one?
My criteria for best is a simple one: what has the highest odds of working given available information. Popularity is not a relevant measure.
A Priori — No microbiome data
Best can be evaluated as the one with the most clinical studies showing benefits. If you search on the US National Library of Medicine you will see around a thousand studies. Many of the studies used strains that are not available in the retail market. This could be a lot of work to get an answer. This link takes you to a search page that lists what is available retail and have studies. The one with the most studies is the best!
There is a gotcha, these are specific for one individual diagnosis — whatever is your hot-button condition.

Microbiome Data is Available
This is not medical condition constrained. Assuming that the microbiome data identifies which bacteria are desired to be raised or lowered, we have several choices:
Published Studies
- Using published studies to engineer the best one.
- Key issue is that there may be no studies finding any probiotic modifies some bacteria that you wish to change.
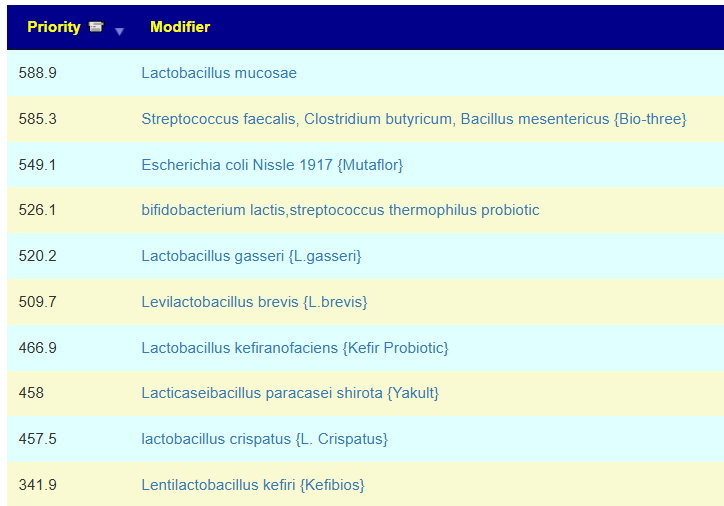
This is the default approach of the expert system on Microbiome Prescription. This produces a list with estimated priority / weights. The one with the highest priority is likely the best.
There is a gotcha — there may be no information on many of the bacteria that you wish to change. You are working in a fog.
Using Metabolite Imbalances
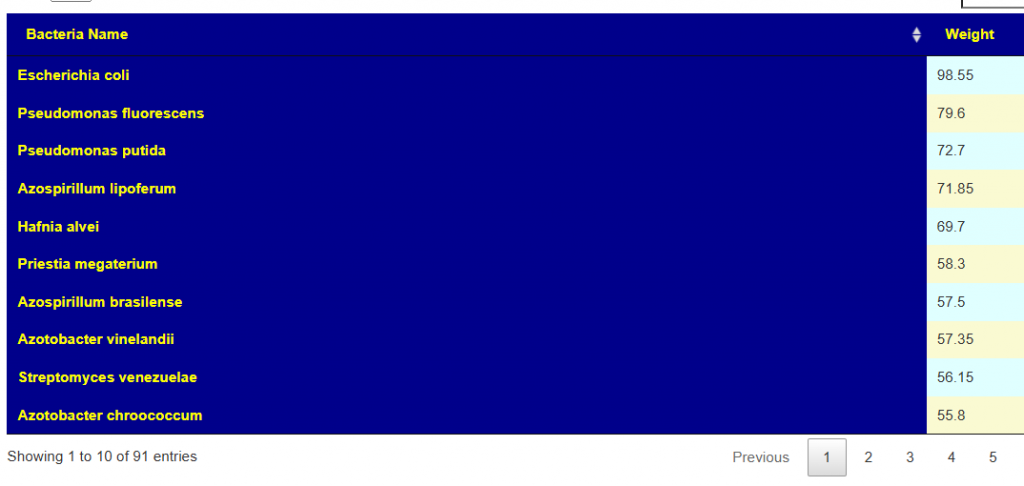
Instead of focusing on individual bacteria, we focus on the chemicals (metabolite) that the bacteria produce or consume. This may be done either from the lab reports or estimating from KEGG: Kyoto Encyclopedia of Genes and Genomes. We focus on too high and too low metabolites and then look at the metabolites produced by each probiotics (by actual measure or by estimates).
We no longer have absence of studies issues. We do have a problem with estimates because we have an assumption that all genes are active — very questionable. We get a list of species that are available (often in mixtures) somewhere in the world.
Using Taxa R2 Associations
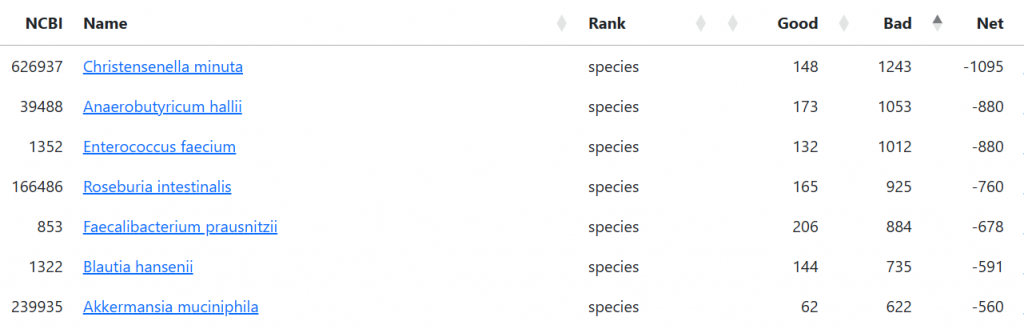
Like Metabolites it is not dependent on the sparse data from studies. We assume that the associations seen in a large collection of shotgun samples from healthy individuals are predictive of the probiotic impact. We are back to dealing with issues on a bacteria by bacteria basis. We have the good impact and the bad impact. We can filter to only good bacteria to be conservative.
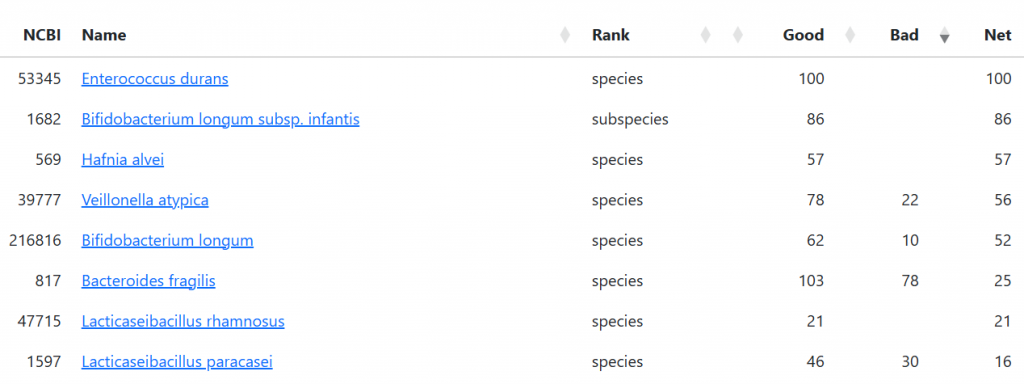
We also can identify probiotics that are likely to have a negative effect. This is important because adverse effect on some bacteria are often omitted from published studies.
Bottom Line
For me, the best approach is to use the R2 suggestions for ranking but require that all of the methods above recommends it. The odds are strongly in favor of it working.
Two Videos discussing the above in more detail.
Recent Comments