With regular testing and following suggestions, Hawrelak’s criteria out of range items went from 9 , to 7, to 4. Suggestions appear to work (slowly). This is a follow up of prior posts, the bottom line is that with
- Jan 25,2022 A review of a ME/CFS Microbiome
- Jul 16,2022 Comparing 4 ME/CFS Samples with New Tool
I am going to start with the same comparison as I did in the prior post above, and then move on to do an analysis using the latest tools available.
Why Follow Up Posts are important
The first item is simple, does the model and suggestion appear to work. Everything is theoretically computed, not based on clinical practice or clinical studies. The second item is that these posts encourages people to try suggestions, or to do “self-serve” with the site.
Foreword – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that appears to have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
Comparisons between Samples
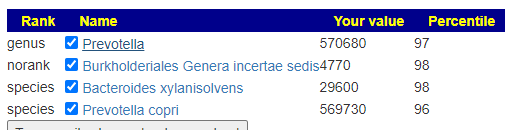
We have the latest test processed through both Ombre and Biomesight. This analysis will use Ombre because that is what was used in prior; latest one will use Biomesight so we can use the new special studies for suggestions
The high lights are:
- Sample quality is better than the prior samples, we see more bacteria reported
- Ombre is reporting more (as we saw in a prior post)
- Improvement in the critical bacteria identified by Dr. Jason Hawrelak, we are down to just 4 bacteria outside of range for both (from prior 7 and 9)
- Similar with Medivere, MyBioma,Nirvana/CosmosId, and XenoGene ranges
- On the opposite side, we have more outside of Box-Plot-Whiskers, Lab Range (+/- 1.96SD) and Kaltoft-Møldrup – this is not unexpected because we have a lot more bacteria. The criteria improved are the criteria with a fix set of bacteria that are usually there in most samples.
- The number of extreme enzymes levels (using Ombre) have been significantly reduced. Compounds have no clear shift
| Measure | 8/22/2022 BIOMESIGHT | 8/22/2022 OMBRE | 6/15/2022 | 5/16/2022 | 3/15/2022 | 11/21/2021 |
| Lab Read Quality | 5 | 5 | 4.8 | 4.8 | 3.6 | 4.2 |
| Bacteria Reported By Lab | 657 | 765 | 515 | 669 | 593 | 473 |
| Bacteria Over 99%ile | 0 | 9 | 0 | 1 | 0 | 1 |
| Bacteria Over 95%ile | 15 | 45 | 4 | 22 | 21 | 9 |
| Bacteria Over 90%ile | 38 | 82 | 22 | 40 | 48 | 21 |
| Bacteria Under 10%ile | 168 | 35 | 43 | 112 | 23 | 87 |
| Bacteria Under 5%ile | 84 | 16 | 18 | 60 | 5 | 46 |
| Bacteria Under 1%ile | 24 | 3 | 0 | 9 | 0 | 2 |
| Lab Read Quality | BiomeSight | Ombre | Ombre | Ombre | Ombre | Ombre |
| Pathogens | 47 | 43 | 37 | 42 | 38 | 33 |
| Outside Range from JasonH | 4 | 4 | 7 | 7 | 9 | 9 |
| Outside Range from Medivere | 15 | 15 | 17 | 17 | 20 | 20 |
| Outside Range from Metagenomics | 8 | 8 | 8 | 8 | 7 | 7 |
| Outside Range from MyBioma | 4 | 4 | 8 | 8 | 10 | 10 |
| Outside Range from Nirvana/CosmosId | 20 | 20 | 23 | 23 | 22 | 22 |
| Outside Range from XenoGene | 4 | 4 | 8 | 8 | 10 | 10 |
| Outside Lab Range (+/- 1.96SD) | 16 | 14 | 2 | 7 | 6 | 2 |
| Outside Box-Plot-Whiskers | 135 | 118 | 42 | 71 | 72 | 25 |
| Outside Kaltoft-Møldrup | 155 | 209 | 113 | 148 | 143 | 91 |
| Condition Est. Over 99%ile | 0 | 0 | 0 | 0 | 0 | 0 |
| Condition Est. Over 95%ile | 0 | 0 | 0 | 0 | 0 | 0 |
| Condition Est. Over 90%ile | 0 | 0 | 0 | 0 | 1 | 0 |
| Enzymes Over 99%ile | 2 | 8 | 91 | 48 | 53 | 5 |
| Enzymes Over 95%ile | 48 | 78 | 599 | 305 | 182 | 147 |
| Enzymes Over 90%ile | 99 | 154 | 719 | 629 | 438 | 458 |
| Enzymes Under 10%ile | 175 | 75 | 70 | 71 | 38 | 169 |
| Enzymes Under 5%ile | 101 | 33 | 19 | 28 | 4 | 78 |
| Enzymes Under 1%ile | 20 | 3 | 2 | 0 | 0 | 0 |
| Compounds Over 99%ile | 31 | 36 | 6 | 93 | 143 | 19 |
| Compounds Over 95%ile | 131 | 265 | 186 | 277 | 190 | 89 |
| Compounds Over 90%ile | 371 | 380 | 303 | 435 | 220 | 118 |
| Compounds Under 10%ile | 212 | 282 | 321 | 528 | 333 | 133 |
| Compounds Under 5%ile | 54 | 186 | 195 | 378 | 310 | 100 |
| Compounds Under 1%ile | 23 | 62 | 0 | 118 | 267 | 42 |
The data suggests further improvement with the latest sample — in terms of numbers, dramatic!
Going Forward
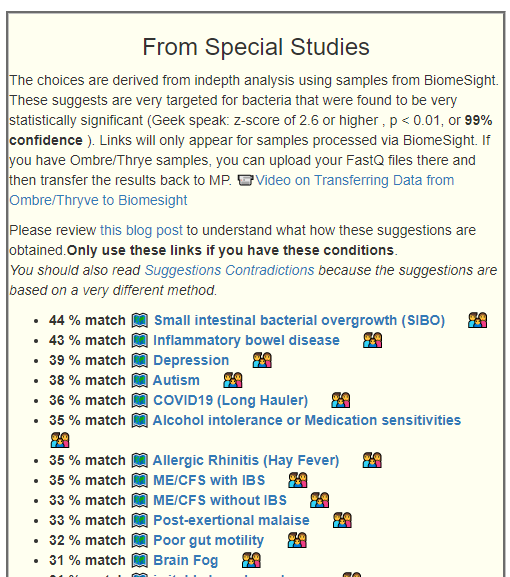
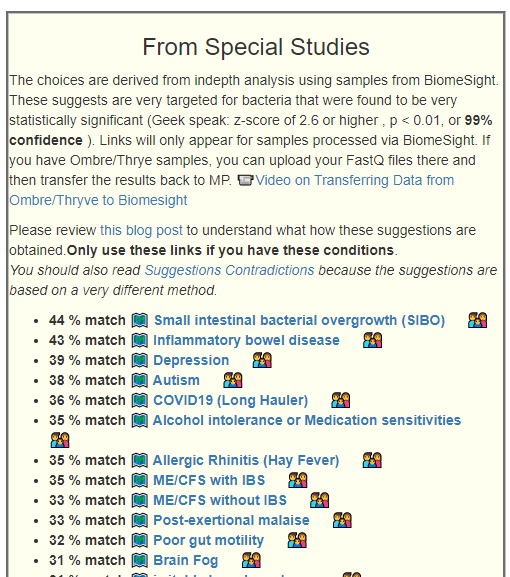
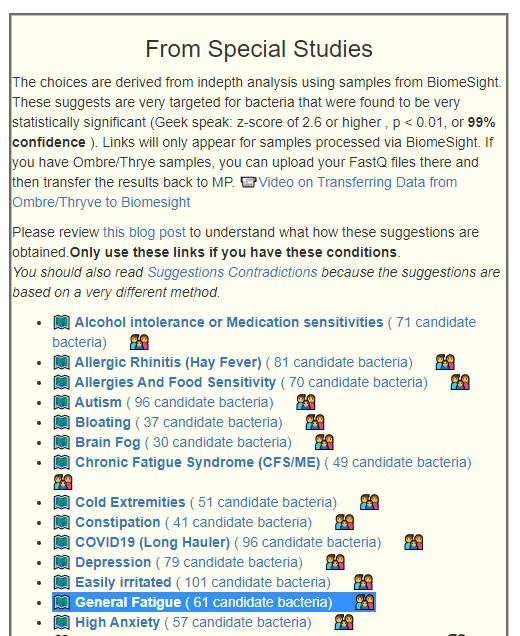
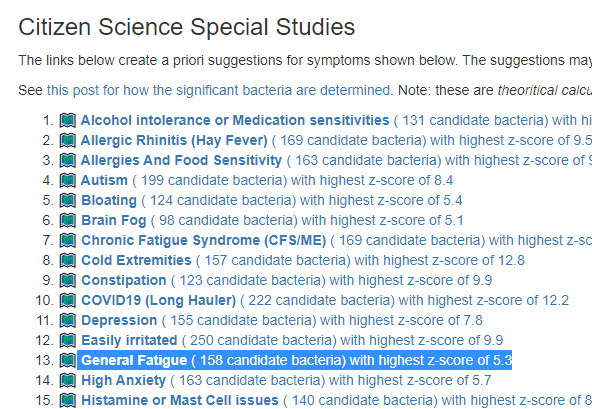
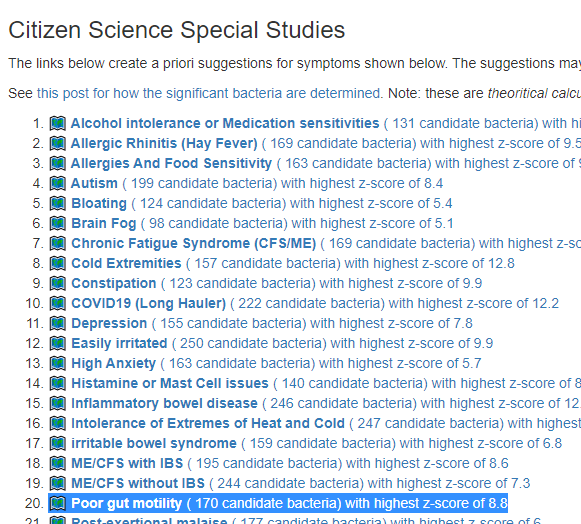
We are going to use the Special Studies to generate the next set of suggestions. Remember that the numbers below are sensitive to the number of bacteria detected (i.e. lab quality). The latest sample had the highest quality which means that percentages may increase due to that alone.
| Percentage Matches | 8/22/2022 | 7/21/2022 | 4/20/2022 | 2/22/2022 | 11/22/2021 | |
| 1 | Alcohol intolerance or Medication sensitivities | 52 | 34 | 36 | 36 | 39 |
| 1 | Allergic Rhinitis (Hay Fever) | 33 | 31 | 35 | 35 | 36 |
| 0 | Allergies And Food Sensitivity | 30 | 32 | 32 | 32 | 34 |
| 0 | Autism | 38 | 28 | 31 | 31 | 44 |
| 1 | Bloating | 24 | 22 | 24 | 24 | 32 |
| 2 | Brain Fog | 28 | 32 | 39 | 39 | 26 |
| 2 | Chronic Fatigue Syndrome (CFS/ME) | 33 | 30 | 28 | 28 | 30 |
| 0 | Cold Extremities | 31 | 36 | 29 | 29 | 31 |
| 0 | Constipation | 17 | 18 | 15 | 15 | 29 |
| 2? | COVID19 (Long Hauler) | 39 | 36 | 31 | 31 | 39 |
| 0 | Depression | 40 | 30 | 33 | 33 | 35 |
| 0 | Easily irritated | 28 | 31 | 24 | 24 | 27 |
| 2 | General Fatigue | 26 | 26 | 28 | 28 | 28 |
| 1 | High Anxiety | 28 | 26 | 25 | 25 | 26 |
| 1 | Histamine or Mast Cell issues | 28 | 24 | 27 | 27 | 32 |
| 0 | Inflammatory bowel disease | 43 | 48 | 28 | 38 | 43 |
| 0 | irritable bowel syndrome | 31 | 30 | 26 | 26 | 36 |
| 1 | Intolerance of Extremes of Heat and Cold | 32 | 30 | 24 | 24 | 36 |
| 0 | ME/CFS with IBS | 31 | 24 | 24 | 24 | 27 |
| 2 | ME/CFS without IBS | 30 | 25 | 23 | 23 | 28 |
| 0 | Poor Gut Motility | 25 | 37 | 31 | 31 | 35 |
| 2 | Post-exertional malaise | 22 | 24 | 23 | 23 | 26 |
| 0 | SIBO | 38 | 36 | 27 | 27 | 34 |
| 0 | Tinnitus (ringing in ear) | 32 | 34 | 24 | 24 | 28 |
| 2 | Unrefreshed sleep | 37 | 27 | 26 | 26 | 29 |
What surprised me, and delighted me, was the relative consistency of the numbers for the same person over time for many symptoms. This time, because of the special studies, we are going to focus on generating suggestions specific to the issues of greatest concerns (2) above.
- Brain Fog
- Chronic Fatigue Syndrome (CFS/ME)
- COVID19 (Long Hauler)
- General Fatigue
- ME/CFS without IBS
- Post-exertional malaise
- Unrefreshed sleep
Having high IBS or IBD values does not equate to ME/CFS with IBS — prior to my latter flares, I saw no gut issues at all.
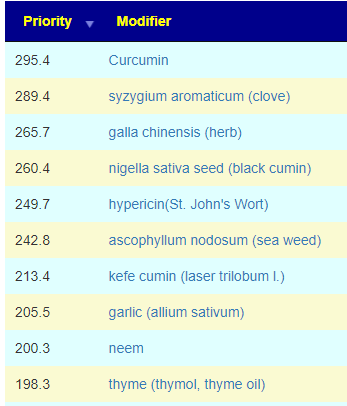
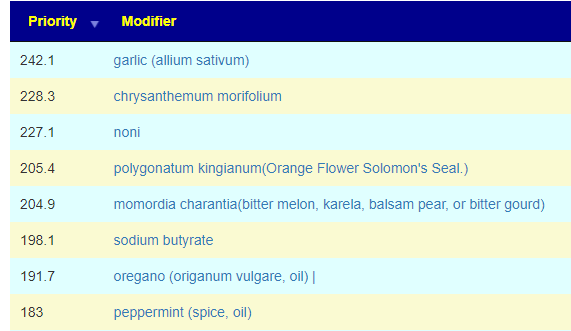
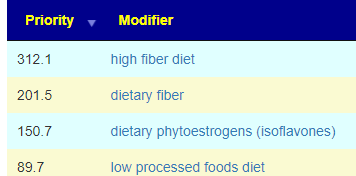
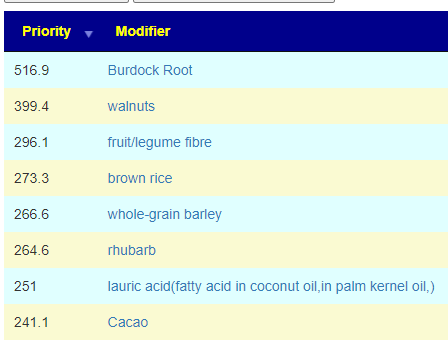
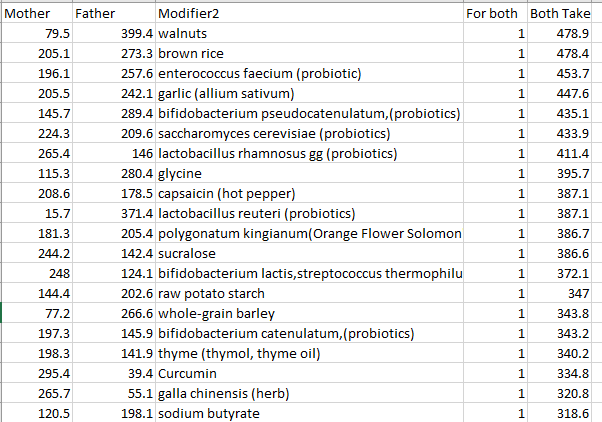
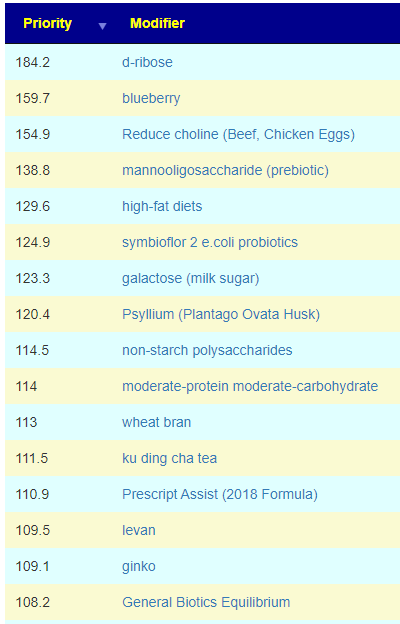
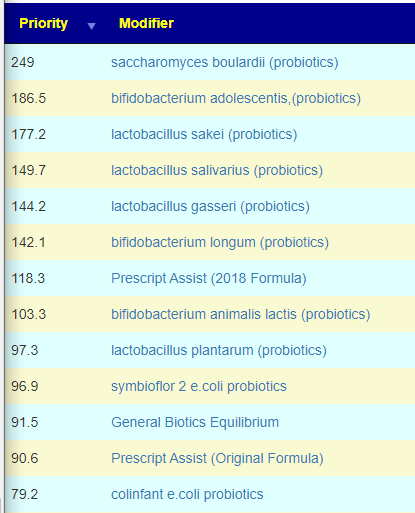
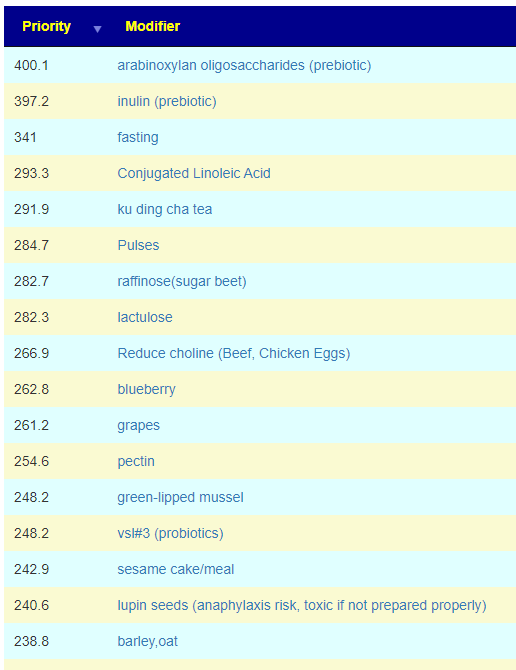
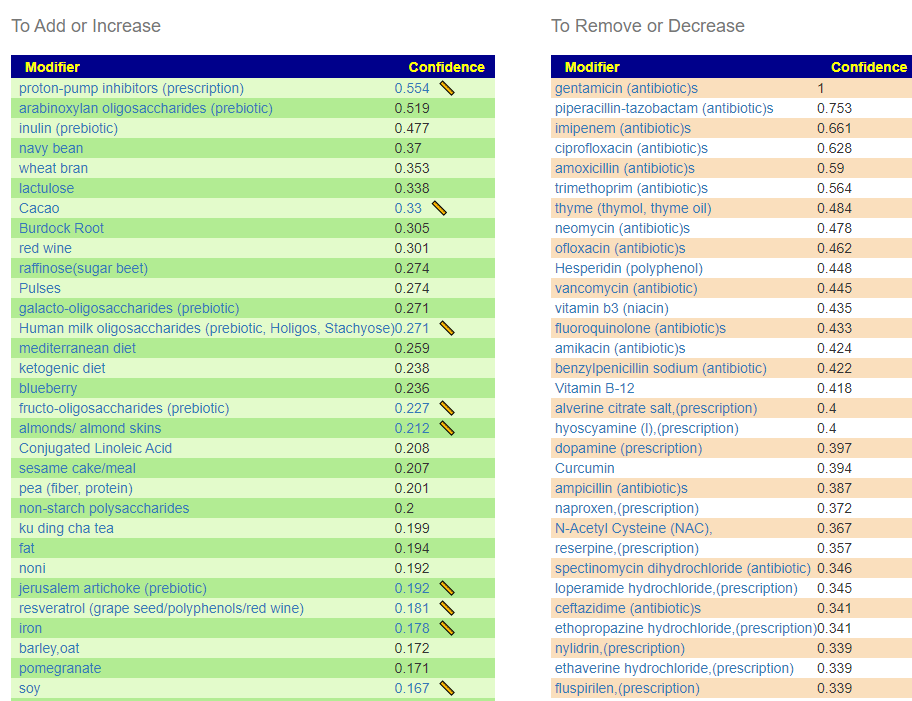
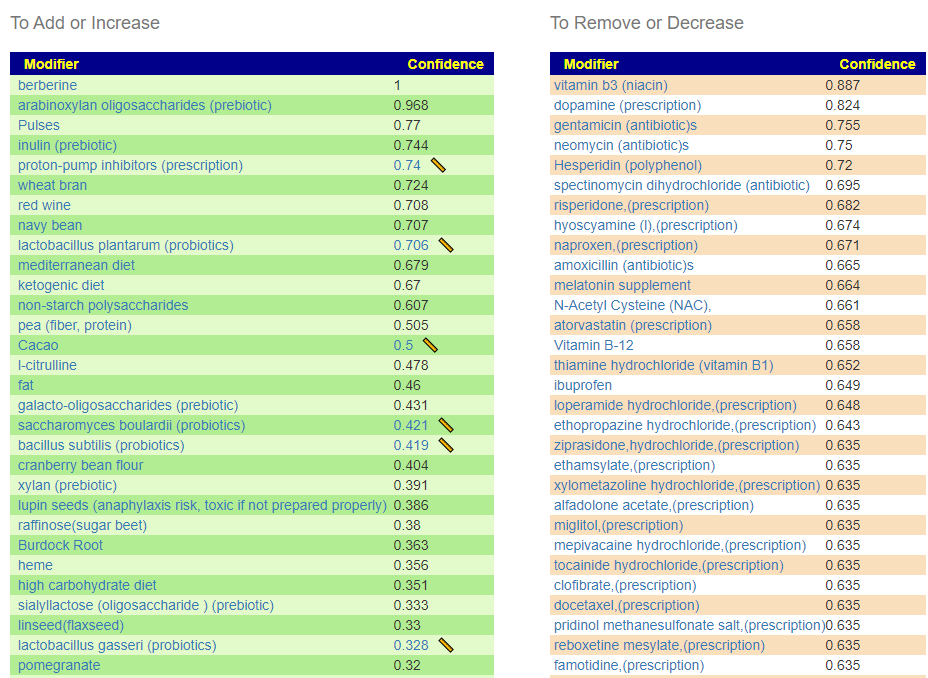
The top Items are similar to each other:
- Pulses (Black Beans,Broad Beans,dry beans, dry broad beans, dry peas, chickpeas, cow peas, pigeon peas, lentils, Bambara beans, vetches, lupins), navy bean, pea (fiber, protein)
- symbioflor 2 e.coli probiotics,colinfant e.coli probiotics and d-ribose (which feeds e.coli)
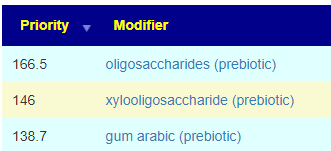
- arabinoxylan oligosaccharides (prebiotic)
- lactulose
- green-lipped mussel
- levan
- fasting
- galacto-oligosaccharides (prebiotic)
- non-starch polysaccharides
- carob
- raffinose(sugar beet)
- wheat bran
- barley,oat
- sesame cake/meal
- Reduce choline (Beef, Chicken Eggs)
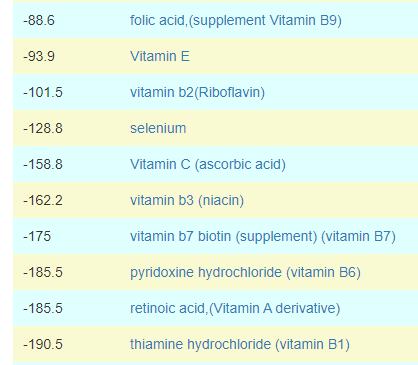
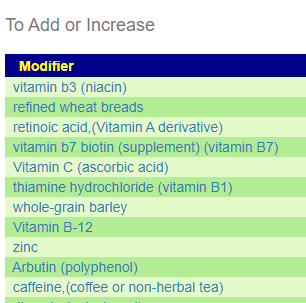
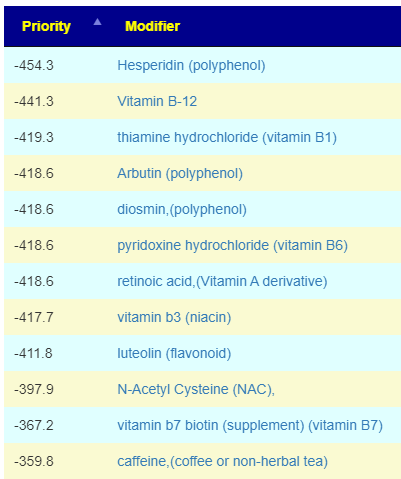
The top of the avoid list are many B-Vitamins. In prior posts, I speculated that the low vitamin B-levels seen in the blood of ME/CFS patients etc is because of greedy gut bacteria that prevents it being absorbed. I just did some literature browsing and this speculation appears to agree with some research.
Now, Wexler et al. show that some gut microbes may be able to pirate vitamin B12 from us as it passes through the digestive tract. Wexler et al. showed that a protein called BtuG on the surface of a type of gut bacteria called Bacteriodes grabs onto vitamin B12 with extraordinary strength. In fact, these bacterial proteins bind to vitamin B12 so strongly that they can even pry it away from our own vitamin B12 collecting protein.
Human gut Bacteroides capture vitamin B12 via cell surface-exposed lipoproteins [2018]
This means that to avoid B-vitamins via food or supplements, despite having low blood level may be a rational approach. Getting Vitamin-B injections bypassing the gut bacteria may be a more effective approach to dealing with low vitamin-B. Choline is connected with B-Vitamins, see The B Vitamins and Choline: Overview and Methods [1998], hence the reduce choline suggestion above.
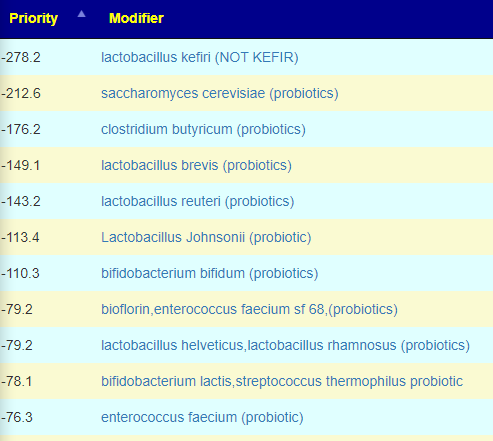
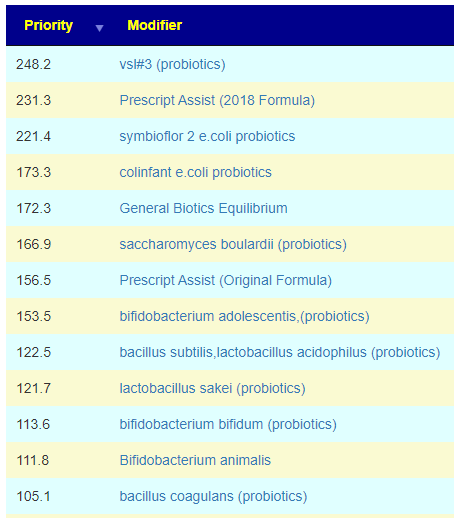
Probiotics
Escherichia coli was the top probiotic on the consensus. Using Ombre reading of the sample and the Kyoto Encyclopedia of Genes and Genomes, Escherichia coli is the top suggestion with items like Bacillus subtilis being 1/3 of contribution. The same results appear with the BiomeSight processing.
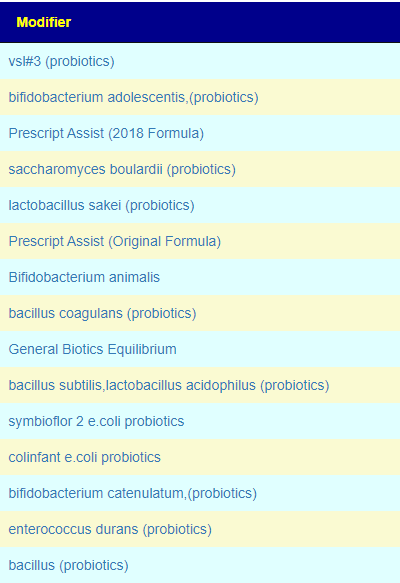
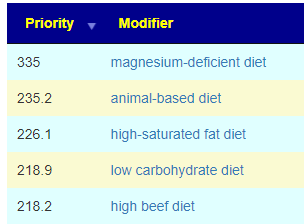
For flavonoids and polyphenols — it seems that supplementing with any should be avoided. The very few with a positive value has ‘equivalents’ being negative values. For amino acids: Conjugated Linoleic Acid, l-citrulline and proline (amino acid) are the top choices. Diet choices are low animal protein (which agrees with avoiding b-vitamins) and high fiber (which agrees with pulses above)
Bottom Line
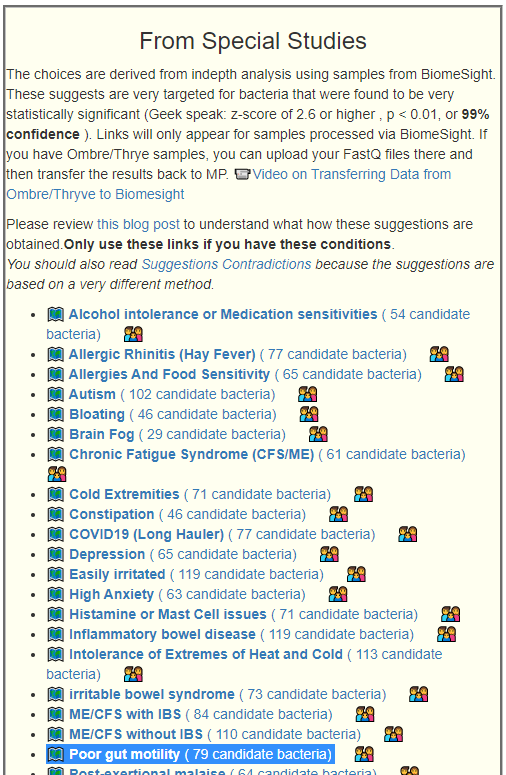
Remember, these are not generic suggestion for anybody with ME/CFS. These are specific to this person’s microbiome. We see that the numbers for his microbiome has improved, but some items are still of concern. Our method of getting suggestions shifted over to using the Special Studies because he had a number of symptoms that were significant which were covered by the special studies, as well as his data being processed thru BiomeSight which we are using for special studies (apples to apples comparisons).
Again, the computations are based on the odds of items helping the microbiome to shift in the desired direction. Odds are just that, some will work, some will not — but ideally more will work than not. For the suggestions, remember ROTATION (Rotation — Essential for Changing the Microbiome), and pick items that work for you and your medical professional. The suggestions can be viewed as a series of dresses on a rack, you do not need to buy all of them to be fashionable. Use the ones that work for you.
Recent Comments